Peptide-drug Conjugate Information
General Information of This Peptide-drug Conjugate (PDC)
| PDC ID |
PDC_00239
|
|||||
|---|---|---|---|---|---|---|
| PDC Name |
Melflufen
|
|||||
| PDC Status |
Approved
|
|||||
| Indication |
In total 5 Indication(s)
|
|||||
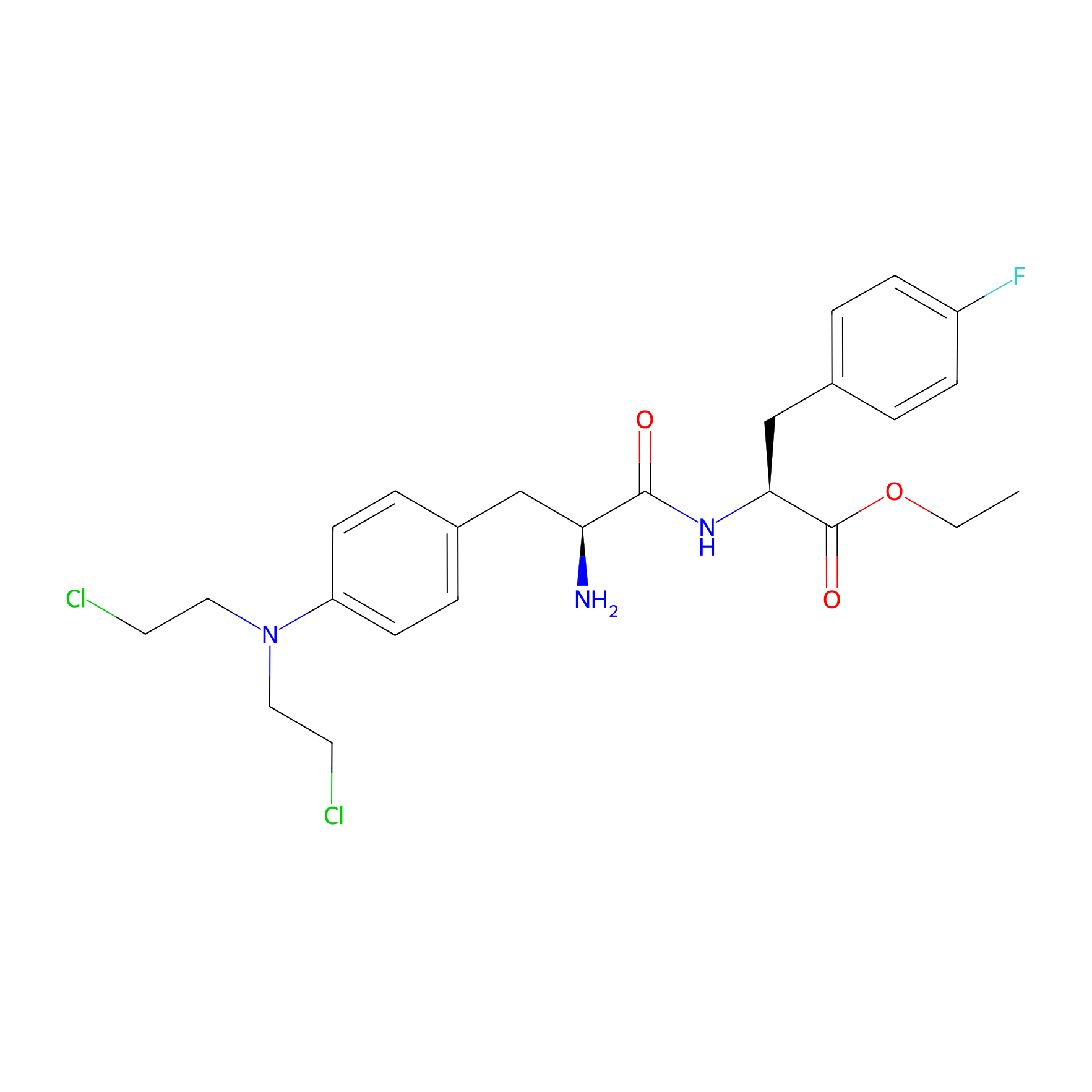
| Structure |
|
|||||
| Peptide Name |
p-Fluorophenylalanine
|
Peptide Info | ||||
| Receptor Name |
Aminopeptidases
|
Receptor Info | ||||
| Drug Name |
Melphalan
|
Drug Info | ||||
| Therapeutic Target |
Human Deoxyribonucleic acid (hDNA)
|
Target Info | ||||
| Linker Name |
Acetic acid
|
Linker Info | ||||
| Peptide Modified Type |
The modification of binding with chemical macromolecules
|
|||||
| Modified Segment |
F
|
|||||
| Formula |
C24H30Cl2FN3O3
|
|||||
| #Ro5 Violations (Lipinski): 1 | Molecular Weight | 498.426 | ||||
| Lipid-water partition coefficient (xlogp) | 3.2701 | |||||
| Hydrogen Bond Donor Count (hbonddonor) | 2 | |||||
| Hydrogen Bond Acceptor Count (hbondacc) | 5 | |||||
| Rotatable Bond Count (rotbonds) | 13 | |||||
Full List of Activity Data of This Peptide-drug Conjugate
Identified from the Human Clinical Data
| Experiment 1 Reporting the Activity Data of This PDC | [1] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Adverse event rate |
97.00%
|
|||
| Patients Enrolled |
Patients with multi-refractory multiple myeloma.
|
||||
| Administration Time | 14.3 week (median) | ||||
| Administration Dosage | 40 mg with dexamethasone (40 mg) | ||||
| MOA of PDC |
Melflufen is highly lipophilic, which promotes its rapid uptake by cells. Once within the cell, melflufen releases its hydrophilic alkylator payloads via the hydrolytic activity of intracellular peptidases (e.g., aminopeptidases). Aminopeptidases are Zn2+-dependent metalloproteinases that remove amino acids at the N-terminal position from oligopeptides and have been associated with multiple tumorigenic processes such as proliferation, apoptosis, differentiation, angiogenesis, and motility. The dependence of melflufen on aminopeptidases was initially demonstrated by the reduced cytotoxic activity of melflufen-but not the alkylator melphalan-when cells were pretreated with bestatin, an antibiotic that is a potent aminopeptidase inhibitor. In addition, structure analogs designed to resist peptide hydrolysis (N-methyl derivative and derivative with D-amino acid) were shown to be almost 100-fold less potent than melflufen. Subsequent in vitro studies demonstrated that hydrolytic cleavage of melflufen by aminopeptidases releases alkylator payloads, including melphalan. In vitro, the activity of melflufen is multi-pronged, including induction of DNA damage, induction of apoptosis, inhibition of VEGF-dependent cell migration, and inhibition of tumor-associated angiogenesis, which have been further reviewed elsewhere. Downregulation of aminopeptidases resulted in reduced melflufen-mediated cytotoxic activity and apoptotic signaling in cultured cells.
Click to Show/Hide
|
||||
| Experiment 2 Reporting the Activity Data of This PDC | [1] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Adverse event rate |
97.00%
|
|||
| MOA of PDC |
Melflufen is highly lipophilic, which promotes its rapid uptake by cells. Once within the cell, melflufen releases its hydrophilic alkylator payloads via the hydrolytic activity of intracellular peptidases (e.g., aminopeptidases). Aminopeptidases are Zn2+-dependent metalloproteinases that remove amino acids at the N-terminal position from oligopeptides and have been associated with multiple tumorigenic processes such as proliferation, apoptosis, differentiation, angiogenesis, and motility. The dependence of melflufen on aminopeptidases was initially demonstrated by the reduced cytotoxic activity of melflufen-but not the alkylator melphalan-when cells were pretreated with bestatin, an antibiotic that is a potent aminopeptidase inhibitor. In addition, structure analogs designed to resist peptide hydrolysis (N-methyl derivative and derivative with D-amino acid) were shown to be almost 100-fold less potent than melflufen. Subsequent in vitro studies demonstrated that hydrolytic cleavage of melflufen by aminopeptidases releases alkylator payloads, including melphalan. In vitro, the activity of melflufen is multi-pronged, including induction of DNA damage, induction of apoptosis, inhibition of VEGF-dependent cell migration, and inhibition of tumor-associated angiogenesis, which have been further reviewed elsewhere. Downregulation of aminopeptidases resulted in reduced melflufen-mediated cytotoxic activity and apoptotic signaling in cultured cells.
Click to Show/Hide
|
||||
| Description |
Overall, 97% of patients experienced any-grade AEs and 85% of patients experienced Grades 3/4 AEs.
|
||||
| In Vivo Model | 75 patients with multiple myeloma. | ||||
| Experiment 3 Reporting the Activity Data of This PDC | [1] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Adverse event rate |
100.00%
|
|||
| Patients Enrolled |
Patients with multi-refractory multiple myeloma.
|
||||
| Administration Time | 28-day cycle | ||||
| Administration Dosage | 40 mg with dexamethasone (40 mg) | ||||
| MOA of PDC |
Melflufen is highly lipophilic, which promotes its rapid uptake by cells. Once within the cell, melflufen releases its hydrophilic alkylator payloads via the hydrolytic activity of intracellular peptidases (e.g., aminopeptidases). Aminopeptidases are Zn2+-dependent metalloproteinases that remove amino acids at the N-terminal position from oligopeptides and have been associated with multiple tumorigenic processes such as proliferation, apoptosis, differentiation, angiogenesis, and motility. The dependence of melflufen on aminopeptidases was initially demonstrated by the reduced cytotoxic activity of melflufen-but not the alkylator melphalan-when cells were pretreated with bestatin, an antibiotic that is a potent aminopeptidase inhibitor. In addition, structure analogs designed to resist peptide hydrolysis (N-methyl derivative and derivative with D-amino acid) were shown to be almost 100-fold less potent than melflufen. Subsequent in vitro studies demonstrated that hydrolytic cleavage of melflufen by aminopeptidases releases alkylator payloads, including melphalan. In vitro, the activity of melflufen is multi-pronged, including induction of DNA damage, induction of apoptosis, inhibition of VEGF-dependent cell migration, and inhibition of tumor-associated angiogenesis, which have been further reviewed elsewhere. Downregulation of aminopeptidases resulted in reduced melflufen-mediated cytotoxic activity and apoptotic signaling in cultured cells.
Click to Show/Hide
|
||||
| Experiment 4 Reporting the Activity Data of This PDC | [2] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Anemia |
9%
|
|||
| MOA of PDC |
Melphalan flufenamide (melflufen), a first-in-class alkylating peptide-drug conjugate, plus dexamethasone was approved in Europe for use in patients with triple-class refractory relapsed/refractory multiple myeloma (RRMM) with 3 prior lines of therapy and without prior autologous stem cell transplantation (ASCT) or with a time to progression >36 months after prior ASCT. The randomized LIGHTHOUSE study (NCT04649060) assessed melflufen plus daratumumab and dexamethasone (melflufen group) versus daratumumab in patients with RRMM with disease refractory to an immunomodulatory agent and a proteasome inhibitor or who had received 3 prior lines of therapy including an immunomodulatory agent and a proteasome inhibitor. A partial clinical hold issued by the US Food and Drug Administration for all melflufen studies led to financial constraints and premature study closure on February 23rd 2022 (data cut-off date). In total, 54 of 240 planned patients were randomized (melflufen group, N=27; daratumumab group, N=27). Median progression-free survival (PFS) was not reached in the melflufen group versus 4.9 months in the daratumumab group (Hazard Ratio: 0.18 [95% Confidence Interval, 0.05-0.65]; P=0.0032) at a median follow-up time of 7.1 and 6.6 months, respectively. Overall response rate (ORR) was 59% in the melflufen group versus 30% in the daratumumab group (P=0.0300). The most common grade 3 treatment-emergent adverse events in the melflufen group versus daratumumab group were neutropenia (50% vs. 12%), thrombocytopenia (50% vs. 8%), and anemia (32% vs. 19%). Melflufen plus daratumumab and dexamethasone demonstrated superior PFS and ORR versus daratumumab in RRMM and a safety profile comparable to previously published melflufen studies.
Click to Show/Hide
|
||||
| Description |
The safety population included patients who received ≥1 dose of melflufen, daratumumab, or dexamethasone (melflufen group) and 26 patients who received daratumumab monotherapy. In the safety population, ≥1 TEAE was reported in 21 patients (96%) with melflufen, daratumumab, and dexamethasone and 22 patients (85%) with daratumumab. Overall, grade ≥3 TEAE occurred in 18 patients (82%) with melflufen, daratumumab, and dexamethasone and 14 patients (54%) with daratumumab. The most common hematologic grade ≥3 TEAE were neutropenia (melflufen group, 11 patients [50%]; daratumumab group, 3 patients [12%]), thrombocytopenia (melflufen group, 11 patients [50%]; daratumumab group, 2 patients [8%]), and anemia (melflufen group, 7 patients [32%]; daratumumab group, 5 patients [19%]). The most common non-hematologic grade ≥3 TEAE were pneumonia (melflufen group, 2 patients [9%]; daratumumab group, 2 patients [8%]) and femur fracture (melflufen group, 0 patients [0%]; daratumumab group, 2 patients [8%]); of these, 1 event (5%) of pneumonia in the melflufen group and 1 event (4%) of femur fracture in the daratumumab group were considered treatment-related TEAE by the investigator. Serious AE occurred in 6 patients (27%) with melflufen, daratumumab, and dexamethasone, and 12 patients (46%) with daratumumab. The most common serious AE (occurring in ≥4 patients overall) were anemia (melflufen group, 2 patients [9%]; daratumumab group, 3 patients [12%]) and pneumonia (melflufen group, 2 patients [9%]; daratumumab group, 2 patients [8%]). TEAE leading to treatment discontinuation occurred in 2 patients (9%) in the melflufen group (neutropenia and thrombocytopenia, N=1 each) and 4 patients (15%) in the daratumumab group (anemia, disease progression, hypercalcemia, and renal failure, N=1 each). Overall, 5 patients died on study before the crossover: 2 patients who received melflufen, daratumumab, and dexamethasone (1 due to disease progression and 1 due to unknown reasons, both >30 days after the last dose of study treatment) and 3 patients who received daratumumab (1 due to disease progression and 1 due to unknown reasons, both ≤30 days after the last dose of study treatment and 1 due to an AE [COVID-19 pneumonia], >30 days after the last dose of study treatment). In addition, one patient who crossed over to receive melflufen, daratumumab, and dexamethasone after progression on daratumumab died.
Click to Show/Hide
|
||||
| In Vivo Model | 22 relapsed/refractory multiple myeloma. | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT04649060 | Clinical Status | Phase 3 | ||
| Clinical Description | This was a randomized, controlled, open-label, Phase 3 multicenter study which enrolled patients with Relapsed-Refractory Multiple Myeloma (RRMM) who were either double refractory to an Immunomodulatory Drug (IMiD) and a Proteasome Inhibitor (PI) (regardless of the number of prior lines of therapy), or had received at least 3 prior lines of therapy including an IMiD and a PI. Patients received treatment with melflufen+dexamethasone+daratumumab or daratumumab until documented progressive disease, unacceptable toxicity, or patient/treating physician decision. Patients in the daratumumab treatment arm had the option to receive treatment with melflufen+dexamethasone+daratumumab after confirmed progressive disease. | ||||
| Experiment 5 Reporting the Activity Data of This PDC | [2] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Anemia |
32%
|
|||
| MOA of PDC |
Melphalan flufenamide (melflufen), a first-in-class alkylating peptide-drug conjugate, plus dexamethasone was approved in Europe for use in patients with triple-class refractory relapsed/refractory multiple myeloma (RRMM) with 3 prior lines of therapy and without prior autologous stem cell transplantation (ASCT) or with a time to progression >36 months after prior ASCT. The randomized LIGHTHOUSE study (NCT04649060) assessed melflufen plus daratumumab and dexamethasone (melflufen group) versus daratumumab in patients with RRMM with disease refractory to an immunomodulatory agent and a proteasome inhibitor or who had received 3 prior lines of therapy including an immunomodulatory agent and a proteasome inhibitor. A partial clinical hold issued by the US Food and Drug Administration for all melflufen studies led to financial constraints and premature study closure on February 23rd 2022 (data cut-off date). In total, 54 of 240 planned patients were randomized (melflufen group, N=27; daratumumab group, N=27). Median progression-free survival (PFS) was not reached in the melflufen group versus 4.9 months in the daratumumab group (Hazard Ratio: 0.18 [95% Confidence Interval, 0.05-0.65]; P=0.0032) at a median follow-up time of 7.1 and 6.6 months, respectively. Overall response rate (ORR) was 59% in the melflufen group versus 30% in the daratumumab group (P=0.0300). The most common grade 3 treatment-emergent adverse events in the melflufen group versus daratumumab group were neutropenia (50% vs. 12%), thrombocytopenia (50% vs. 8%), and anemia (32% vs. 19%). Melflufen plus daratumumab and dexamethasone demonstrated superior PFS and ORR versus daratumumab in RRMM and a safety profile comparable to previously published melflufen studies.
Click to Show/Hide
|
||||
| Description |
The safety population included patients who received ≥1 dose of melflufen, daratumumab, or dexamethasone (melflufen group) and 26 patients who received daratumumab monotherapy. In the safety population, ≥1 TEAE was reported in 21 patients (96%) with melflufen, daratumumab, and dexamethasone and 22 patients (85%) with daratumumab. Overall, grade ≥3 TEAE occurred in 18 patients (82%) with melflufen, daratumumab, and dexamethasone and 14 patients (54%) with daratumumab. The most common hematologic grade ≥3 TEAE were neutropenia (melflufen group, 11 patients [50%]; daratumumab group, 3 patients [12%]), thrombocytopenia (melflufen group, 11 patients [50%]; daratumumab group, 2 patients [8%]), and anemia (melflufen group, 7 patients [32%]; daratumumab group, 5 patients [19%]). The most common non-hematologic grade ≥3 TEAE were pneumonia (melflufen group, 2 patients [9%]; daratumumab group, 2 patients [8%]) and femur fracture (melflufen group, 0 patients [0%]; daratumumab group, 2 patients [8%]); of these, 1 event (5%) of pneumonia in the melflufen group and 1 event (4%) of femur fracture in the daratumumab group were considered treatment-related TEAE by the investigator. Serious AE occurred in 6 patients (27%) with melflufen, daratumumab, and dexamethasone, and 12 patients (46%) with daratumumab. The most common serious AE (occurring in ≥4 patients overall) were anemia (melflufen group, 2 patients [9%]; daratumumab group, 3 patients [12%]) and pneumonia (melflufen group, 2 patients [9%]; daratumumab group, 2 patients [8%]). TEAE leading to treatment discontinuation occurred in 2 patients (9%) in the melflufen group (neutropenia and thrombocytopenia, N=1 each) and 4 patients (15%) in the daratumumab group (anemia, disease progression, hypercalcemia, and renal failure, N=1 each). Overall, 5 patients died on study before the crossover: 2 patients who received melflufen, daratumumab, and dexamethasone (1 due to disease progression and 1 due to unknown reasons, both >30 days after the last dose of study treatment) and 3 patients who received daratumumab (1 due to disease progression and 1 due to unknown reasons, both ≤30 days after the last dose of study treatment and 1 due to an AE [COVID-19 pneumonia], >30 days after the last dose of study treatment). In addition, one patient who crossed over to receive melflufen, daratumumab, and dexamethasone after progression on daratumumab died.
Click to Show/Hide
|
||||
| In Vivo Model | 22 relapsed/refractory multiple myeloma. | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT04649060 | Clinical Status | Phase 3 | ||
| Clinical Description | This was a randomized, controlled, open-label, Phase 3 multicenter study which enrolled patients with Relapsed-Refractory Multiple Myeloma (RRMM) who were either double refractory to an Immunomodulatory Drug (IMiD) and a Proteasome Inhibitor (PI) (regardless of the number of prior lines of therapy), or had received at least 3 prior lines of therapy including an IMiD and a PI. Patients received treatment with melflufen+dexamethasone+daratumumab or daratumumab until documented progressive disease, unacceptable toxicity, or patient/treating physician decision. Patients in the daratumumab treatment arm had the option to receive treatment with melflufen+dexamethasone+daratumumab after confirmed progressive disease. | ||||
| Experiment 6 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Anemia |
64.30%
|
|||
| Patients Enrolled |
14 patients with relapsed refractory multiple myeloma.
|
||||
| Administration Time | 28-day cycle | ||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (melflufen) is a first-in-class peptide-drug conjugate that utilizes increased peptidase expression to selectively release potent alkylating agents inside tumor cells. Melflufen is hydrolyzed by peptidases and esterases to melphalan either directly or through an intermediate metabolite, desethyl-melflufen. The high lipophilicity of melflufen facilitates passive diffusion across cell membranes. The activity and tolerability of melflufen in relapsed/refractory multiple myeloma (RRMM) were demonstrated in the O-12-M1 (NCT01897714), OCEAN (NCT03151811), and HORIZON (NCT02963493) trials.
Click to Show/Hide
|
||||
| Description |
Overall, at least one TEAE was reported in 13 (92.9%) and 13 (100.0%) patients in Arms A and B, respectively (Table 3). During cycle 1, 9 patients (64.3%) and 12 patients (92.3%), respectively, had at least one TEAE. Cumulatively, grade 3 or 4 AEs occurred in 12 (85.7%) and 12 (92.3%) patients, respectively, and serious AEs were reported in 5 (35.7%) and 9 (69.2%) patients, respectively. The most common any-grade AEs in Arms A and B, respectively, were thrombocytopenia (10 [71.4%]; 10 [76.9%]), neutropenia (9 [64.3%]; 9 [69.2%]), and anemia (9 [64.3%]; 7 [53.8%]). No phlebitis or local-infusion-related reactions were reported based on pre- and post-infusion inspection of the IV site, and there were no extravasations observed in Arm A or B. Similarly, VIP scores collected on Day 1 post-infusion and on Day 8 indicated that patients had healthy IV sites (VIP score of 0) with no signs of phlebitis following PVC administration of melflufen. The most common non-hematological AE was positive SARS-CoV-2 test (Arm A: 2 [14.3%]; Arm B: 4 [30.8%]). Pneumonia was the most common serious AE (Arm A: 2 [14.3%]; Arm B: 2 [15.4%]). The most common AE considered related to melflufen and/or dexamethasone by investigators was thrombocytopenia (Arm A: 10 [71.4%]; Arm B: 10 [76.9%]). AEs led to treatment discontinuation in 3 (21.4%) and 6 (46.2%) patients in Arms A and B, respectively.
Click to Show/Hide
|
||||
| Half life period | 75.6 h | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT04412707 | Clinical Status | Phase 2 | ||
| Clinical Description | This is a randomized, two-period, cross-over Phase 2 study, comparing PK, and assessing safety and tolerability and efficacy of peripheral and central intravenous administration of melflufen in patients with RRMM. It is an international study, enrolling patients in US and Europe. The study will enroll patients following at least 2 lines of prior therapy. | ||||
| Experiment 7 Reporting the Activity Data of This PDC | [4] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Anemia |
43.00%
|
|||
| Patients Enrolled |
157 patients with multiple myeloma.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melflufen is a first-in-class peptide-drug conjugate, targeting aminopeptidase which has an increased expression in fast-growing and aggressive malignancies. The lipophilicity of melflufen allows for passive diffusion, selectively targeting myeloma cells. Once inside the cell, melflufen is hydrolyzed to active alkylating metabolites melphalan and desethyl-melflufen. Melflufen and the active metabolites trigger irreversible DNA damage, inhibit proliferation, induces apoptosis, and express antiangiogenic effects. In addition, melflufen demonstrated activity in myeloma cells with documented impaired or absent Tp53 expression and documented resistance to bortezomib, dexamethasone, and melphalan.
Click to Show/Hide
|
||||
| Description |
Based on the safety data collected during the HORIZON trial, treatment emergent adverse events occurred in 100% of patients including 100 patients (64%) having at least 1 CTCAE grade 4 adverse effect. Hematologic grade 3 or 4 adverse effects including thrombocytopenia (76%), neutropenia (79%), anemia (43%), and infections (11%) were the most commonly reported. Other adverse effects, such as fatigue (55%), nausea (32%), diarrhea (27%), and decreased appetite (14%), were similar to other alkylating agents. Pyrexia (24%), including febrile neutropenia (5%), and respiratory tract infections (24%) were contributed to hematologic toxicities.
Click to Show/Hide
|
||||
| Experiment 8 Reporting the Activity Data of This PDC | [1] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Anemia |
64.00%
|
|||
| Patients Enrolled |
Patients with multi-refractory multiple myeloma.
|
||||
| MOA of PDC |
Melflufen is highly lipophilic, which promotes its rapid uptake by cells. Once within the cell, melflufen releases its hydrophilic alkylator payloads via the hydrolytic activity of intracellular peptidases (e.g., aminopeptidases). Aminopeptidases are Zn2+-dependent metalloproteinases that remove amino acids at the N-terminal position from oligopeptides and have been associated with multiple tumorigenic processes such as proliferation, apoptosis, differentiation, angiogenesis, and motility. The dependence of melflufen on aminopeptidases was initially demonstrated by the reduced cytotoxic activity of melflufen-but not the alkylator melphalan-when cells were pretreated with bestatin, an antibiotic that is a potent aminopeptidase inhibitor. In addition, structure analogs designed to resist peptide hydrolysis (N-methyl derivative and derivative with D-amino acid) were shown to be almost 100-fold less potent than melflufen. Subsequent in vitro studies demonstrated that hydrolytic cleavage of melflufen by aminopeptidases releases alkylator payloads, including melphalan. In vitro, the activity of melflufen is multi-pronged, including induction of DNA damage, induction of apoptosis, inhibition of VEGF-dependent cell migration, and inhibition of tumor-associated angiogenesis, which have been further reviewed elsewhere. Downregulation of aminopeptidases resulted in reduced melflufen-mediated cytotoxic activity and apoptotic signaling in cultured cells.
Click to Show/Hide
|
||||
| Description |
Melflufen plus dexamethasone was generally manageable in this heavily pretreated patient population [51]. All patients experienced ≥1 AE, most commonly hematologic AEs including thrombocytopenia (73%), neutropenia (69%), and anemia (64%). The most common non-hematologic AEs included pyrexia (40%), asthenia (31%), fatigue (29%), nausea (27%), and diarrhea (24%).
Click to Show/Hide
|
||||
| Experiment 9 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Arthralgia |
7.10%
|
|||
| Patients Enrolled |
14 patients with relapsed refractory multiple myeloma.
|
||||
| Administration Time | 28-day cycle | ||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (melflufen) is a first-in-class peptide-drug conjugate that utilizes increased peptidase expression to selectively release potent alkylating agents inside tumor cells. Melflufen is hydrolyzed by peptidases and esterases to melphalan either directly or through an intermediate metabolite, desethyl-melflufen. The high lipophilicity of melflufen facilitates passive diffusion across cell membranes. The activity and tolerability of melflufen in relapsed/refractory multiple myeloma (RRMM) were demonstrated in the O-12-M1 (NCT01897714), OCEAN (NCT03151811), and HORIZON (NCT02963493) trials.
Click to Show/Hide
|
||||
| Description |
Overall, at least one TEAE was reported in 13 (92.9%) and 13 (100.0%) patients in Arms A and B, respectively (Table 3). During cycle 1, 9 patients (64.3%) and 12 patients (92.3%), respectively, had at least one TEAE. Cumulatively, grade 3 or 4 AEs occurred in 12 (85.7%) and 12 (92.3%) patients, respectively, and serious AEs were reported in 5 (35.7%) and 9 (69.2%) patients, respectively. The most common any-grade AEs in Arms A and B, respectively, were thrombocytopenia (10 [71.4%]; 10 [76.9%]), neutropenia (9 [64.3%]; 9 [69.2%]), and anemia (9 [64.3%]; 7 [53.8%]). No phlebitis or local-infusion-related reactions were reported based on pre- and post-infusion inspection of the IV site, and there were no extravasations observed in Arm A or B. Similarly, VIP scores collected on Day 1 post-infusion and on Day 8 indicated that patients had healthy IV sites (VIP score of 0) with no signs of phlebitis following PVC administration of melflufen. The most common non-hematological AE was positive SARS-CoV-2 test (Arm A: 2 [14.3%]; Arm B: 4 [30.8%]). Pneumonia was the most common serious AE (Arm A: 2 [14.3%]; Arm B: 2 [15.4%]). The most common AE considered related to melflufen and/or dexamethasone by investigators was thrombocytopenia (Arm A: 10 [71.4%]; Arm B: 10 [76.9%]). AEs led to treatment discontinuation in 3 (21.4%) and 6 (46.2%) patients in Arms A and B, respectively.
Click to Show/Hide
|
||||
| Half life period | 75.6 h | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT04412707 | Clinical Status | Phase 2 | ||
| Clinical Description | This is a randomized, two-period, cross-over Phase 2 study, comparing PK, and assessing safety and tolerability and efficacy of peripheral and central intravenous administration of melflufen in patients with RRMM. It is an international study, enrolling patients in US and Europe. The study will enroll patients following at least 2 lines of prior therapy. | ||||
| Experiment 10 Reporting the Activity Data of This PDC | [1] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Asthenia |
31.00%
|
|||
| Patients Enrolled |
Patients with multi-refractory multiple myeloma.
|
||||
| MOA of PDC |
Melflufen is highly lipophilic, which promotes its rapid uptake by cells. Once within the cell, melflufen releases its hydrophilic alkylator payloads via the hydrolytic activity of intracellular peptidases (e.g., aminopeptidases). Aminopeptidases are Zn2+-dependent metalloproteinases that remove amino acids at the N-terminal position from oligopeptides and have been associated with multiple tumorigenic processes such as proliferation, apoptosis, differentiation, angiogenesis, and motility. The dependence of melflufen on aminopeptidases was initially demonstrated by the reduced cytotoxic activity of melflufen-but not the alkylator melphalan-when cells were pretreated with bestatin, an antibiotic that is a potent aminopeptidase inhibitor. In addition, structure analogs designed to resist peptide hydrolysis (N-methyl derivative and derivative with D-amino acid) were shown to be almost 100-fold less potent than melflufen. Subsequent in vitro studies demonstrated that hydrolytic cleavage of melflufen by aminopeptidases releases alkylator payloads, including melphalan. In vitro, the activity of melflufen is multi-pronged, including induction of DNA damage, induction of apoptosis, inhibition of VEGF-dependent cell migration, and inhibition of tumor-associated angiogenesis, which have been further reviewed elsewhere. Downregulation of aminopeptidases resulted in reduced melflufen-mediated cytotoxic activity and apoptotic signaling in cultured cells.
Click to Show/Hide
|
||||
| Description |
Melflufen plus dexamethasone was generally manageable in this heavily pretreated patient population [51]. All patients experienced ≥1 AE, most commonly hematologic AEs including thrombocytopenia (73%), neutropenia (69%), and anemia (64%). The most common non-hematologic AEs included pyrexia (40%), asthenia (31%), fatigue (29%), nausea (27%), and diarrhea (24%).
Click to Show/Hide
|
||||
| Experiment 11 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Back pain |
14.30%
|
|||
| Patients Enrolled |
14 patients with relapsed refractory multiple myeloma.
|
||||
| Administration Time | 28-day cycle | ||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (melflufen) is a first-in-class peptide-drug conjugate that utilizes increased peptidase expression to selectively release potent alkylating agents inside tumor cells. Melflufen is hydrolyzed by peptidases and esterases to melphalan either directly or through an intermediate metabolite, desethyl-melflufen. The high lipophilicity of melflufen facilitates passive diffusion across cell membranes. The activity and tolerability of melflufen in relapsed/refractory multiple myeloma (RRMM) were demonstrated in the O-12-M1 (NCT01897714), OCEAN (NCT03151811), and HORIZON (NCT02963493) trials.
Click to Show/Hide
|
||||
| Description |
Overall, at least one TEAE was reported in 13 (92.9%) and 13 (100.0%) patients in Arms A and B, respectively (Table 3). During cycle 1, 9 patients (64.3%) and 12 patients (92.3%), respectively, had at least one TEAE. Cumulatively, grade 3 or 4 AEs occurred in 12 (85.7%) and 12 (92.3%) patients, respectively, and serious AEs were reported in 5 (35.7%) and 9 (69.2%) patients, respectively. The most common any-grade AEs in Arms A and B, respectively, were thrombocytopenia (10 [71.4%]; 10 [76.9%]), neutropenia (9 [64.3%]; 9 [69.2%]), and anemia (9 [64.3%]; 7 [53.8%]). No phlebitis or local-infusion-related reactions were reported based on pre- and post-infusion inspection of the IV site, and there were no extravasations observed in Arm A or B. Similarly, VIP scores collected on Day 1 post-infusion and on Day 8 indicated that patients had healthy IV sites (VIP score of 0) with no signs of phlebitis following PVC administration of melflufen. The most common non-hematological AE was positive SARS-CoV-2 test (Arm A: 2 [14.3%]; Arm B: 4 [30.8%]). Pneumonia was the most common serious AE (Arm A: 2 [14.3%]; Arm B: 2 [15.4%]). The most common AE considered related to melflufen and/or dexamethasone by investigators was thrombocytopenia (Arm A: 10 [71.4%]; Arm B: 10 [76.9%]). AEs led to treatment discontinuation in 3 (21.4%) and 6 (46.2%) patients in Arms A and B, respectively.
Click to Show/Hide
|
||||
| Half life period | 75.6 h | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT04412707 | Clinical Status | Phase 2 | ||
| Clinical Description | This is a randomized, two-period, cross-over Phase 2 study, comparing PK, and assessing safety and tolerability and efficacy of peripheral and central intravenous administration of melflufen in patients with RRMM. It is an international study, enrolling patients in US and Europe. The study will enroll patients following at least 2 lines of prior therapy. | ||||
| Experiment 12 Reporting the Activity Data of This PDC | [2] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Best confirmed response |
4%
|
|||
| MOA of PDC |
Melphalan flufenamide (melflufen), a first-in-class alkylating peptide-drug conjugate, plus dexamethasone was approved in Europe for use in patients with triple-class refractory relapsed/refractory multiple myeloma (RRMM) with 3 prior lines of therapy and without prior autologous stem cell transplantation (ASCT) or with a time to progression >36 months after prior ASCT. The randomized LIGHTHOUSE study (NCT04649060) assessed melflufen plus daratumumab and dexamethasone (melflufen group) versus daratumumab in patients with RRMM with disease refractory to an immunomodulatory agent and a proteasome inhibitor or who had received 3 prior lines of therapy including an immunomodulatory agent and a proteasome inhibitor. A partial clinical hold issued by the US Food and Drug Administration for all melflufen studies led to financial constraints and premature study closure on February 23rd 2022 (data cut-off date). In total, 54 of 240 planned patients were randomized (melflufen group, N=27; daratumumab group, N=27). Median progression-free survival (PFS) was not reached in the melflufen group versus 4.9 months in the daratumumab group (Hazard Ratio: 0.18 [95% Confidence Interval, 0.05-0.65]; P=0.0032) at a median follow-up time of 7.1 and 6.6 months, respectively. Overall response rate (ORR) was 59% in the melflufen group versus 30% in the daratumumab group (P=0.0300). The most common grade 3 treatment-emergent adverse events in the melflufen group versus daratumumab group were neutropenia (50% vs. 12%), thrombocytopenia (50% vs. 8%), and anemia (32% vs. 19%). Melflufen plus daratumumab and dexamethasone demonstrated superior PFS and ORR versus daratumumab in RRMM and a safety profile comparable to previously published melflufen studies.
Click to Show/Hide
|
||||
| Description |
In the ITT population, with a median follow-up of 7.1 months in the melflufen group, the median PFS was not reached (NR) and with a median follow-up of 6.6 months in the daratumumab group, the median PFS was 4.9 months (95% CI: 3.4-NR; HR: 0.18 [95% CI: 0.05-0.65]; log-rankP=0.0032). OS was immature, with 2 events (7%) in the melflufen group and 4 events (15%) in the daratumumab group (HR: 0.47 [95% CI: 0.09-2.57]; log-rankP=0.3721) at a median follow-up of 7.6 months and 6.6 months, respectively. The ORR was 59% (95% CI: 39-78) in the melflufen group and 30% (95% CI: 14-50) in the daratumumab group (P=0.0300). More patients in the melflufen group had a complete response (CR; 1 patient [4%]vs. 0 patients [0%]) and very good partial response (VGPR; 4 patients [15%]vs. 3 patients [11%]) compared with the daratumumab group.
Click to Show/Hide
|
||||
| In Vivo Model | 27 Intent-to-treat (ITT) population. | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT04649060 | Clinical Status | Phase 3 | ||
| Clinical Description | This was a randomized, controlled, open-label, Phase 3 multicenter study which enrolled patients with Relapsed-Refractory Multiple Myeloma (RRMM) who were either double refractory to an Immunomodulatory Drug (IMiD) and a Proteasome Inhibitor (PI) (regardless of the number of prior lines of therapy), or had received at least 3 prior lines of therapy including an IMiD and a PI. Patients received treatment with melflufen+dexamethasone+daratumumab or daratumumab until documented progressive disease, unacceptable toxicity, or patient/treating physician decision. Patients in the daratumumab treatment arm had the option to receive treatment with melflufen+dexamethasone+daratumumab after confirmed progressive disease. | ||||
| Experiment 13 Reporting the Activity Data of This PDC | [2] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Best confirmed response |
7%
|
|||
| Patients Enrolled |
14 patients no prior ASCT or TTP >36 months after ASCT.
|
||||
| MOA of PDC |
Melphalan flufenamide (melflufen), a first-in-class alkylating peptide-drug conjugate, plus dexamethasone was approved in Europe for use in patients with triple-class refractory relapsed/refractory multiple myeloma (RRMM) with 3 prior lines of therapy and without prior autologous stem cell transplantation (ASCT) or with a time to progression >36 months after prior ASCT. The randomized LIGHTHOUSE study (NCT04649060) assessed melflufen plus daratumumab and dexamethasone (melflufen group) versus daratumumab in patients with RRMM with disease refractory to an immunomodulatory agent and a proteasome inhibitor or who had received 3 prior lines of therapy including an immunomodulatory agent and a proteasome inhibitor. A partial clinical hold issued by the US Food and Drug Administration for all melflufen studies led to financial constraints and premature study closure on February 23rd 2022 (data cut-off date). In total, 54 of 240 planned patients were randomized (melflufen group, N=27; daratumumab group, N=27). Median progression-free survival (PFS) was not reached in the melflufen group versus 4.9 months in the daratumumab group (Hazard Ratio: 0.18 [95% Confidence Interval, 0.05-0.65]; P=0.0032) at a median follow-up time of 7.1 and 6.6 months, respectively. Overall response rate (ORR) was 59% in the melflufen group versus 30% in the daratumumab group (P=0.0300). The most common grade 3 treatment-emergent adverse events in the melflufen group versus daratumumab group were neutropenia (50% vs. 12%), thrombocytopenia (50% vs. 8%), and anemia (32% vs. 19%). Melflufen plus daratumumab and dexamethasone demonstrated superior PFS and ORR versus daratumumab in RRMM and a safety profile comparable to previously published melflufen studies.
Click to Show/Hide
|
||||
| Description |
Efficacy endpoints were more pronounced in favor of the melflufen group compared with the daratumumab group among patients with no prior ASCT or TTP >36 months after a prior ASCT (melflufen group, N=14; daratumumab group, N=15). Median PFS was NR in the melflufen group and 3.9 months (95% CI: 1.4-4.9) in the daratumumab group (HR, 0.06 [95% CI: 0.01-0.49]; log-rank P=0.0005). Fewer OS events were reported in the melflufen group (1 event [7%] vs. 4 events [27%] in the daratumumab group; log-rank P=0.0369). The ORR was 64% (95% CI: 35-87) in the melflufen group and 13% (95% CI: 2-41) in the daratumumab group (P=0.0055). More patients in the melflufen group had a CR (1 patient [7%] vs. 0 patients [0%]) or VGPR (2 patients [14%] vs. 1 patient [7%]) compared with the daratumumab group.
Click to Show/Hide
|
||||
| Related Clinical Trial | |||||
| NCT Number | NCT04649060 | Clinical Status | Phase 3 | ||
| Clinical Description | This was a randomized, controlled, open-label, Phase 3 multicenter study which enrolled patients with Relapsed-Refractory Multiple Myeloma (RRMM) who were either double refractory to an Immunomodulatory Drug (IMiD) and a Proteasome Inhibitor (PI) (regardless of the number of prior lines of therapy), or had received at least 3 prior lines of therapy including an IMiD and a PI. Patients received treatment with melflufen+dexamethasone+daratumumab or daratumumab until documented progressive disease, unacceptable toxicity, or patient/treating physician decision. Patients in the daratumumab treatment arm had the option to receive treatment with melflufen+dexamethasone+daratumumab after confirmed progressive disease. | ||||
| Experiment 14 Reporting the Activity Data of This PDC | [5] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Bleeding |
100%
|
|||
| Patients Enrolled |
153 patients refractory to prior alkylators (melflufen, n=78; pomalidomide, n=75).
|
||||
| MOA of PDC |
Melphalan flufenamide (melflufen), a first-in-class alkylating peptide-drug conjugate, plus dexamethasone demonstrated superior progression-free survival (PFS), but not overall survival (OS), versus pomalidomide plus dexamethasone in relapsed/refractory multiple myeloma in the OCEAN study. Time to progression (TTP) <36 months after a prior autologous stem cell transplantation (ASCT) was a negative prognostic factor for OS with melflufen. This post hoc exploratory analysis evaluated patients refractory to prior alkylators (e.g., cyclophosphamide and melphalan) in OCEAN. In 153 patients refractory to prior alkylators (melflufen, n = 78; pomalidomide, n = 75), the melflufen and pomalidomide arms had similar median PFS (5.6 months [95% CI, 4.2-8.3] vs. 4.7 months [95% CI, 3.1-7.3]; hazard ratio [HR], 0.92 [95% CI, 0.63-1.33]) and OS (23.4 months [95% CI, 14.4-31.7] vs. 20.0 months [95% CI, 12.0-28.7]; HR, 0.92 [95% CI, 0.62-1.38]). Among alkylator-refractory patients with a TTP 36 months after a prior ASCT or no prior ASCT (melflufen, n = 54; pomalidomide, n = 53), the observed median PFS and OS were longer in the melflufen arm than the pomalidomide arm. The safety profile of melflufen was consistent with previous reports. These results suggest that melflufen is safe and effective in patients with alkylator-refractory disease, suggesting differentiated activity from other alkylators.
Click to Show/Hide
|
||||
| Description |
Overall, the safety profile of melflufen plus dexamethasone in the alkylator-refractory group was consistent between treatment arms (Table 2). In the melflufen and pomalidomide arms, respectively, the frequency of treatment-emergent adverse events (TEAEs; 99% vs. 97%), Grade 3 or 4 TEAEs (85% vs. 82%), serious TEAEs (49% vs. 53%), and fatal TEAEs (19% vs. 16%) were similar (Table 2). However, melflufen compared with pomalidomide saw more dose modifications (76% vs. 67%) and dose reductions (47% vs. 14%), comparable dose delays (57% vs. 51%) but less treatment discontinuation (27% vs. 34%). When comparing patients refractory and not refractory to prior alkylators, rates of TEAEs were generally comparable except for slightly lower rates of serious and fatal TEAEs observed in patients not refractory to alkylators. Among Grade 3 or 4 TEAEs of special interest, melflufen saw more thrombocytopenia (73% vs. 14%), neutropenia (65% vs. 55%), and leukopenia or white blood cell decrease (14% vs. 3%), but less infection (15% vs. 26%), than pomalidomide. Notably, melflufen compared with pomalidomide saw a longer median time to dose reduction (106 days [range, 28-443] vs. 47 days [range, 28-225]), Grade 3 or 4 thrombocytopenia (52 days [range, 15-451] vs. 19 days [range, 8-91]), and Grade 3 or 4 neutropenia (36 days [range, 8-561] vs. 22 days [range, 8-470]).
Click to Show/Hide
|
||||
| Experiment 15 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Bone pain |
14.30%
|
|||
| Patients Enrolled |
14 patients with relapsed refractory multiple myeloma.
|
||||
| Administration Time | 28-day cycle | ||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (melflufen) is a first-in-class peptide-drug conjugate that utilizes increased peptidase expression to selectively release potent alkylating agents inside tumor cells. Melflufen is hydrolyzed by peptidases and esterases to melphalan either directly or through an intermediate metabolite, desethyl-melflufen. The high lipophilicity of melflufen facilitates passive diffusion across cell membranes. The activity and tolerability of melflufen in relapsed/refractory multiple myeloma (RRMM) were demonstrated in the O-12-M1 (NCT01897714), OCEAN (NCT03151811), and HORIZON (NCT02963493) trials.
Click to Show/Hide
|
||||
| Description |
Overall, at least one TEAE was reported in 13 (92.9%) and 13 (100.0%) patients in Arms A and B, respectively (Table 3). During cycle 1, 9 patients (64.3%) and 12 patients (92.3%), respectively, had at least one TEAE. Cumulatively, grade 3 or 4 AEs occurred in 12 (85.7%) and 12 (92.3%) patients, respectively, and serious AEs were reported in 5 (35.7%) and 9 (69.2%) patients, respectively. The most common any-grade AEs in Arms A and B, respectively, were thrombocytopenia (10 [71.4%]; 10 [76.9%]), neutropenia (9 [64.3%]; 9 [69.2%]), and anemia (9 [64.3%]; 7 [53.8%]). No phlebitis or local-infusion-related reactions were reported based on pre- and post-infusion inspection of the IV site, and there were no extravasations observed in Arm A or B. Similarly, VIP scores collected on Day 1 post-infusion and on Day 8 indicated that patients had healthy IV sites (VIP score of 0) with no signs of phlebitis following PVC administration of melflufen. The most common non-hematological AE was positive SARS-CoV-2 test (Arm A: 2 [14.3%]; Arm B: 4 [30.8%]). Pneumonia was the most common serious AE (Arm A: 2 [14.3%]; Arm B: 2 [15.4%]). The most common AE considered related to melflufen and/or dexamethasone by investigators was thrombocytopenia (Arm A: 10 [71.4%]; Arm B: 10 [76.9%]). AEs led to treatment discontinuation in 3 (21.4%) and 6 (46.2%) patients in Arms A and B, respectively.
Click to Show/Hide
|
||||
| Half life period | 75.6 h | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT04412707 | Clinical Status | Phase 2 | ||
| Clinical Description | This is a randomized, two-period, cross-over Phase 2 study, comparing PK, and assessing safety and tolerability and efficacy of peripheral and central intravenous administration of melflufen in patients with RRMM. It is an international study, enrolling patients in US and Europe. The study will enroll patients following at least 2 lines of prior therapy. | ||||
| Experiment 16 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | C-reactive protein increase |
14.30%
|
|||
| Patients Enrolled |
14 patients with relapsed refractory multiple myeloma.
|
||||
| Administration Time | 28-day cycle | ||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (melflufen) is a first-in-class peptide-drug conjugate that utilizes increased peptidase expression to selectively release potent alkylating agents inside tumor cells. Melflufen is hydrolyzed by peptidases and esterases to melphalan either directly or through an intermediate metabolite, desethyl-melflufen. The high lipophilicity of melflufen facilitates passive diffusion across cell membranes. The activity and tolerability of melflufen in relapsed/refractory multiple myeloma (RRMM) were demonstrated in the O-12-M1 (NCT01897714), OCEAN (NCT03151811), and HORIZON (NCT02963493) trials.
Click to Show/Hide
|
||||
| Description |
Overall, at least one TEAE was reported in 13 (92.9%) and 13 (100.0%) patients in Arms A and B, respectively (Table 3). During cycle 1, 9 patients (64.3%) and 12 patients (92.3%), respectively, had at least one TEAE. Cumulatively, grade 3 or 4 AEs occurred in 12 (85.7%) and 12 (92.3%) patients, respectively, and serious AEs were reported in 5 (35.7%) and 9 (69.2%) patients, respectively. The most common any-grade AEs in Arms A and B, respectively, were thrombocytopenia (10 [71.4%]; 10 [76.9%]), neutropenia (9 [64.3%]; 9 [69.2%]), and anemia (9 [64.3%]; 7 [53.8%]). No phlebitis or local-infusion-related reactions were reported based on pre- and post-infusion inspection of the IV site, and there were no extravasations observed in Arm A or B. Similarly, VIP scores collected on Day 1 post-infusion and on Day 8 indicated that patients had healthy IV sites (VIP score of 0) with no signs of phlebitis following PVC administration of melflufen. The most common non-hematological AE was positive SARS-CoV-2 test (Arm A: 2 [14.3%]; Arm B: 4 [30.8%]). Pneumonia was the most common serious AE (Arm A: 2 [14.3%]; Arm B: 2 [15.4%]). The most common AE considered related to melflufen and/or dexamethasone by investigators was thrombocytopenia (Arm A: 10 [71.4%]; Arm B: 10 [76.9%]). AEs led to treatment discontinuation in 3 (21.4%) and 6 (46.2%) patients in Arms A and B, respectively.
Click to Show/Hide
|
||||
| Half life period | 75.6 h | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT04412707 | Clinical Status | Phase 2 | ||
| Clinical Description | This is a randomized, two-period, cross-over Phase 2 study, comparing PK, and assessing safety and tolerability and efficacy of peripheral and central intravenous administration of melflufen in patients with RRMM. It is an international study, enrolling patients in US and Europe. The study will enroll patients following at least 2 lines of prior therapy. | ||||
| Experiment 17 Reporting the Activity Data of This PDC | [4] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Clinical benefit rate |
23%
|
|||
| Patients Enrolled |
81 patients with multiple myeloma.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melflufen is a first-in-class peptide-drug conjugate, targeting aminopeptidase which has an increased expression in fast-growing and aggressive malignancies. The lipophilicity of melflufen allows for passive diffusion, selectively targeting myeloma cells. Once inside the cell, melflufen is hydrolyzed to active alkylating metabolites melphalan and desethyl-melflufen. Melflufen and the active metabolites trigger irreversible DNA damage, inhibit proliferation, induces apoptosis, and express antiangiogenic effects. In addition, melflufen demonstrated activity in myeloma cells with documented impaired or absent Tp53 expression and documented resistance to bortezomib, dexamethasone, and melphalan.
Click to Show/Hide
|
||||
| Description |
The phase I arm established 40 mg of melflufen as the maximum tolerated dose in combination with dexamethasone. The phase II arm found an overall response rate (ORR) of 31% (14 patients) and clinical benefit rate, defined as first occurrence of disease response including minimal response or better, of 49% (22 patients) in the melflufen and dexamethasone group compared with an ORR of 8% (1 patient) and clinical benefit rate of 23% (3 patients) in the melflufen group. Based on these findings, melflufen 40 mg plus dexamethasone 40 mg was deemed a feasible treatment regimen for relapsed and refractory multiple myeloma and appropriate to proceed to a larger phase II trial.
Click to Show/Hide
|
||||
| Experiment 18 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Clinical benefit rate |
47%
|
|||
| Patients Enrolled |
246 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 19 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Clinical benefit rate |
50%
|
|||
| Patients Enrolled |
246 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 20 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Clinical benefit rate (CBR) |
57.10%
|
|||
| Patients Enrolled |
14 patients with relapsed refractory multiple myeloma.
|
||||
| Administration Time | 28-day cycle | ||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (melflufen) is a first-in-class peptide-drug conjugate that utilizes increased peptidase expression to selectively release potent alkylating agents inside tumor cells. Melflufen is hydrolyzed by peptidases and esterases to melphalan either directly or through an intermediate metabolite, desethyl-melflufen. The high lipophilicity of melflufen facilitates passive diffusion across cell membranes. The activity and tolerability of melflufen in relapsed/refractory multiple myeloma (RRMM) were demonstrated in the O-12-M1 (NCT01897714), OCEAN (NCT03151811), and HORIZON (NCT02963493) trials.
Click to Show/Hide
|
||||
| Description |
In Arm A, 4 of the 14 patients achieved an overall response (ORR 28.6% [95% CI: 8.4-58.1]) including 1 patient with CR, and the CBR was 57.1% (95% CI: 28.9-82.3). In Arm B, 1 of the 13 patients achieved an overall response (ORR 7.7% [95% CI: 0.2-36.0]), consisting of a PR, and the CBR was 15.4% (95% CI: 1.9-45.4). In the overall study population, 5 patients had an overall response (ORR 18.5% [95% CI: 6.3-38.1]). DOR data were insufficient to evaluate due to early termination of the study, the low number of patient events (1 in Arm A, 0 in Arm B), and the limited number of responses. Based on the 5 patients who had a response of PR or better at study termination (4 in Arm A, 1 in Arm B), the median TTR was 2.4 months in Arm A, 5.1 months in Arm B, and 2.6 months overall. Based on the 8 and 5 progression events in Arm A and Arm B, respectively, the median TTP was 5.8 months and 4.8 months, respectively, with a median TTP of 5.8 months in the overall population. The median PFS was 5.2 months (95% CI: 2.7 to not evaluable) and 2.9 months (95% CI: 1.5-4.6) in Arms A and B, respectively. For the overall study population, median PFS was 3.7 months (95% CI: 2.7-5.8).
Click to Show/Hide
|
||||
| Half life period | 75.6 h | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT04412707 | Clinical Status | Phase 2 | ||
| Clinical Description | This is a randomized, two-period, cross-over Phase 2 study, comparing PK, and assessing safety and tolerability and efficacy of peripheral and central intravenous administration of melflufen in patients with RRMM. It is an international study, enrolling patients in US and Europe. The study will enroll patients following at least 2 lines of prior therapy. | ||||
| Experiment 21 Reporting the Activity Data of This PDC | [7] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Clinical benefit response rate (CBRR) |
23%
|
|||
| Administration Time | Iv infusion of 40 mg melflufen on day 1 of each 28-day treatment cycle | ||||
| Administration Dosage | Melflufen 40 mg (Single Agent) | ||||
| MOA of PDC |
The antineoplastic activity of melflufen is dependent upon the expression of aminopeptidases, like APN (also known as CD18), which cleave melflufen into melphalan and p-Fluorophenylalanine. Following aminopeptidase-dependent cleavage, the hydrophilic alkylating metabolite melphalan accumulates in myeloma cells. This enrichment of the cytotoxic payload has a substantial impact on the antimyeloma activity of melflufen.
Click to Show/Hide
|
||||
| Description |
In the phase 2 single-agent cohort, the overall response rate was 8% (one of 13 patients; 02-360) and the clinical benefit rate was 23% (three of 13; 5-54).
|
||||
| In Vivo Model | Aged 18 years or older, had relapsed and refractory multiple myeloma, had received two or more previous lines of therapy (including lenalidomide and bortezomib). | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT01897714 | Clinical Status | Phase 1/2 | ||
| Clinical Description | The study will explore escalating doses of melflufen in combination with dexamethasone in small groups of patients to find the maximum tolerated dose of melflufen. That dose will then be used to determine the efficacy and safety profile of melflufen in combination with dexamethasone in a larger group of patients. | ||||
| Experiment 22 Reporting the Activity Data of This PDC | [7] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Clinical benefit response rate (CBRR) |
49%
|
|||
| Administration Time | Iv infusion of 40 mg melflufen on day 1 of each 21-day or 28-day treatment cycles, in combination with 40 mg dexamet hasone (oral or iv) on days 1, 8 and 15 of each 21-day treatment cycles. for any patients on the 28-day treatment sc hedule, an additional dose of 40 mg dexamet hasone was administered on day 22 of each treatment cycle | ||||
| Administration Dosage | Melflufen 40 mg + Dexamethasone | ||||
| MOA of PDC |
The antineoplastic activity of melflufen is dependent upon the expression of aminopeptidases, like APN (also known as CD18), which cleave melflufen into melphalan and p-Fluorophenylalanine. Following aminopeptidase-dependent cleavage, the hydrophilic alkylating metabolite melphalan accumulates in myeloma cells. This enrichment of the cytotoxic payload has a substantial impact on the antimyeloma activity of melflufen.
Click to Show/Hide
|
||||
| Description |
In phase 2, patients treated with combination therapy achieved an overall response rate of 31% (14 of 45 patients; 95% CI 18-47) and clinical benefit rate of 49% (22 of 45; 34-64)
|
||||
| In Vivo Model | Aged 18 years or older, had relapsed and refractory multiple myeloma, had received two or more previous lines of therapy (including lenalidomide and bortezomib). | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT01897714 | Clinical Status | Phase 1/2 | ||
| Clinical Description | The study will explore escalating doses of melflufen in combination with dexamethasone in small groups of patients to find the maximum tolerated dose of melflufen. That dose will then be used to determine the efficacy and safety profile of melflufen in combination with dexamethasone in a larger group of patients. | ||||
| Experiment 23 Reporting the Activity Data of This PDC | [2] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Complete response (CR) |
14%
|
|||
| Patients Enrolled |
14 patients no prior ASCT or TTP >36 months after ASCT.
|
||||
| MOA of PDC |
Melphalan flufenamide (melflufen), a first-in-class alkylating peptide-drug conjugate, plus dexamethasone was approved in Europe for use in patients with triple-class refractory relapsed/refractory multiple myeloma (RRMM) with 3 prior lines of therapy and without prior autologous stem cell transplantation (ASCT) or with a time to progression >36 months after prior ASCT. The randomized LIGHTHOUSE study (NCT04649060) assessed melflufen plus daratumumab and dexamethasone (melflufen group) versus daratumumab in patients with RRMM with disease refractory to an immunomodulatory agent and a proteasome inhibitor or who had received 3 prior lines of therapy including an immunomodulatory agent and a proteasome inhibitor. A partial clinical hold issued by the US Food and Drug Administration for all melflufen studies led to financial constraints and premature study closure on February 23rd 2022 (data cut-off date). In total, 54 of 240 planned patients were randomized (melflufen group, N=27; daratumumab group, N=27). Median progression-free survival (PFS) was not reached in the melflufen group versus 4.9 months in the daratumumab group (Hazard Ratio: 0.18 [95% Confidence Interval, 0.05-0.65]; P=0.0032) at a median follow-up time of 7.1 and 6.6 months, respectively. Overall response rate (ORR) was 59% in the melflufen group versus 30% in the daratumumab group (P=0.0300). The most common grade 3 treatment-emergent adverse events in the melflufen group versus daratumumab group were neutropenia (50% vs. 12%), thrombocytopenia (50% vs. 8%), and anemia (32% vs. 19%). Melflufen plus daratumumab and dexamethasone demonstrated superior PFS and ORR versus daratumumab in RRMM and a safety profile comparable to previously published melflufen studies.
Click to Show/Hide
|
||||
| Description |
Efficacy endpoints were more pronounced in favor of the melflufen group compared with the daratumumab group among patients with no prior ASCT or TTP >36 months after a prior ASCT (melflufen group, N=14; daratumumab group, N=15). Median PFS was NR in the melflufen group and 3.9 months (95% CI: 1.4-4.9) in the daratumumab group (HR, 0.06 [95% CI: 0.01-0.49]; log-rank P=0.0005). Fewer OS events were reported in the melflufen group (1 event [7%] vs. 4 events [27%] in the daratumumab group; log-rank P=0.0369). The ORR was 64% (95% CI: 35-87) in the melflufen group and 13% (95% CI: 2-41) in the daratumumab group (P=0.0055). More patients in the melflufen group had a CR (1 patient [7%] vs. 0 patients [0%]) or VGPR (2 patients [14%] vs. 1 patient [7%]) compared with the daratumumab group.
Click to Show/Hide
|
||||
| Related Clinical Trial | |||||
| NCT Number | NCT04649060 | Clinical Status | Phase 3 | ||
| Clinical Description | This was a randomized, controlled, open-label, Phase 3 multicenter study which enrolled patients with Relapsed-Refractory Multiple Myeloma (RRMM) who were either double refractory to an Immunomodulatory Drug (IMiD) and a Proteasome Inhibitor (PI) (regardless of the number of prior lines of therapy), or had received at least 3 prior lines of therapy including an IMiD and a PI. Patients received treatment with melflufen+dexamethasone+daratumumab or daratumumab until documented progressive disease, unacceptable toxicity, or patient/treating physician decision. Patients in the daratumumab treatment arm had the option to receive treatment with melflufen+dexamethasone+daratumumab after confirmed progressive disease. | ||||
| Experiment 24 Reporting the Activity Data of This PDC | [2] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Complete response (CR) |
15%
|
|||
| MOA of PDC |
Melphalan flufenamide (melflufen), a first-in-class alkylating peptide-drug conjugate, plus dexamethasone was approved in Europe for use in patients with triple-class refractory relapsed/refractory multiple myeloma (RRMM) with 3 prior lines of therapy and without prior autologous stem cell transplantation (ASCT) or with a time to progression >36 months after prior ASCT. The randomized LIGHTHOUSE study (NCT04649060) assessed melflufen plus daratumumab and dexamethasone (melflufen group) versus daratumumab in patients with RRMM with disease refractory to an immunomodulatory agent and a proteasome inhibitor or who had received 3 prior lines of therapy including an immunomodulatory agent and a proteasome inhibitor. A partial clinical hold issued by the US Food and Drug Administration for all melflufen studies led to financial constraints and premature study closure on February 23rd 2022 (data cut-off date). In total, 54 of 240 planned patients were randomized (melflufen group, N=27; daratumumab group, N=27). Median progression-free survival (PFS) was not reached in the melflufen group versus 4.9 months in the daratumumab group (Hazard Ratio: 0.18 [95% Confidence Interval, 0.05-0.65]; P=0.0032) at a median follow-up time of 7.1 and 6.6 months, respectively. Overall response rate (ORR) was 59% in the melflufen group versus 30% in the daratumumab group (P=0.0300). The most common grade 3 treatment-emergent adverse events in the melflufen group versus daratumumab group were neutropenia (50% vs. 12%), thrombocytopenia (50% vs. 8%), and anemia (32% vs. 19%). Melflufen plus daratumumab and dexamethasone demonstrated superior PFS and ORR versus daratumumab in RRMM and a safety profile comparable to previously published melflufen studies.
Click to Show/Hide
|
||||
| Description |
In the ITT population, with a median follow-up of 7.1 months in the melflufen group, the median PFS was not reached (NR) and with a median follow-up of 6.6 months in the daratumumab group, the median PFS was 4.9 months (95% CI: 3.4-NR; HR: 0.18 [95% CI: 0.05-0.65]; log-rankP=0.0032). OS was immature, with 2 events (7%) in the melflufen group and 4 events (15%) in the daratumumab group (HR: 0.47 [95% CI: 0.09-2.57]; log-rankP=0.3721) at a median follow-up of 7.6 months and 6.6 months, respectively. The ORR was 59% (95% CI: 39-78) in the melflufen group and 30% (95% CI: 14-50) in the daratumumab group (P=0.0300). More patients in the melflufen group had a complete response (CR; 1 patient [4%]vs. 0 patients [0%]) and very good partial response (VGPR; 4 patients [15%]vs. 3 patients [11%]) compared with the daratumumab group.
Click to Show/Hide
|
||||
| In Vivo Model | 27 Intent-to-treat (ITT) population. | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT04649060 | Clinical Status | Phase 3 | ||
| Clinical Description | This was a randomized, controlled, open-label, Phase 3 multicenter study which enrolled patients with Relapsed-Refractory Multiple Myeloma (RRMM) who were either double refractory to an Immunomodulatory Drug (IMiD) and a Proteasome Inhibitor (PI) (regardless of the number of prior lines of therapy), or had received at least 3 prior lines of therapy including an IMiD and a PI. Patients received treatment with melflufen+dexamethasone+daratumumab or daratumumab until documented progressive disease, unacceptable toxicity, or patient/treating physician decision. Patients in the daratumumab treatment arm had the option to receive treatment with melflufen+dexamethasone+daratumumab after confirmed progressive disease. | ||||
| Experiment 25 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Complete response (CR) |
7.10%
|
|||
| Patients Enrolled |
14 patients with relapsed refractory multiple myeloma.
|
||||
| Administration Time | 28-day cycle | ||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (melflufen) is a first-in-class peptide-drug conjugate that utilizes increased peptidase expression to selectively release potent alkylating agents inside tumor cells. Melflufen is hydrolyzed by peptidases and esterases to melphalan either directly or through an intermediate metabolite, desethyl-melflufen. The high lipophilicity of melflufen facilitates passive diffusion across cell membranes. The activity and tolerability of melflufen in relapsed/refractory multiple myeloma (RRMM) were demonstrated in the O-12-M1 (NCT01897714), OCEAN (NCT03151811), and HORIZON (NCT02963493) trials.
Click to Show/Hide
|
||||
| Description |
In Arm A, 4 of the 14 patients achieved an overall response (ORR 28.6% [95% CI: 8.4-58.1]) including 1 patient with CR, and the CBR was 57.1% (95% CI: 28.9-82.3). In Arm B, 1 of the 13 patients achieved an overall response (ORR 7.7% [95% CI: 0.2-36.0]), consisting of a PR, and the CBR was 15.4% (95% CI: 1.9-45.4). In the overall study population, 5 patients had an overall response (ORR 18.5% [95% CI: 6.3-38.1]). DOR data were insufficient to evaluate due to early termination of the study, the low number of patient events (1 in Arm A, 0 in Arm B), and the limited number of responses. Based on the 5 patients who had a response of PR or better at study termination (4 in Arm A, 1 in Arm B), the median TTR was 2.4 months in Arm A, 5.1 months in Arm B, and 2.6 months overall. Based on the 8 and 5 progression events in Arm A and Arm B, respectively, the median TTP was 5.8 months and 4.8 months, respectively, with a median TTP of 5.8 months in the overall population. The median PFS was 5.2 months (95% CI: 2.7 to not evaluable) and 2.9 months (95% CI: 1.5-4.6) in Arms A and B, respectively. For the overall study population, median PFS was 3.7 months (95% CI: 2.7-5.8).
Click to Show/Hide
|
||||
| Half life period | 75.6 h | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT04412707 | Clinical Status | Phase 2 | ||
| Clinical Description | This is a randomized, two-period, cross-over Phase 2 study, comparing PK, and assessing safety and tolerability and efficacy of peripheral and central intravenous administration of melflufen in patients with RRMM. It is an international study, enrolling patients in US and Europe. The study will enroll patients following at least 2 lines of prior therapy. | ||||
| Experiment 26 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Complete response (CR) |
0%
|
|||
| Patients Enrolled |
246 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 27 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Complete response (CR) |
1%
|
|||
| Patients Enrolled |
246 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 28 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Complete response (CR) |
2%
|
|||
| Patients Enrolled |
246 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 29 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Complete response (CR) |
3%
|
|||
| Patients Enrolled |
246 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 30 Reporting the Activity Data of This PDC | [4] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Decreased appetite |
14%
|
|||
| Patients Enrolled |
157 patients with multiple myeloma.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melflufen is a first-in-class peptide-drug conjugate, targeting aminopeptidase which has an increased expression in fast-growing and aggressive malignancies. The lipophilicity of melflufen allows for passive diffusion, selectively targeting myeloma cells. Once inside the cell, melflufen is hydrolyzed to active alkylating metabolites melphalan and desethyl-melflufen. Melflufen and the active metabolites trigger irreversible DNA damage, inhibit proliferation, induces apoptosis, and express antiangiogenic effects. In addition, melflufen demonstrated activity in myeloma cells with documented impaired or absent Tp53 expression and documented resistance to bortezomib, dexamethasone, and melphalan.
Click to Show/Hide
|
||||
| Description |
Based on the safety data collected during the HORIZON trial, treatment emergent adverse events occurred in 100% of patients including 100 patients (64%) having at least 1 CTCAE grade 4 adverse effect. Hematologic grade 3 or 4 adverse effects including thrombocytopenia (76%), neutropenia (79%), anemia (43%), and infections (11%) were the most commonly reported. Other adverse effects, such as fatigue (55%), nausea (32%), diarrhea (27%), and decreased appetite (14%), were similar to other alkylating agents. Pyrexia (24%), including febrile neutropenia (5%), and respiratory tract infections (24%) were contributed to hematologic toxicities.
Click to Show/Hide
|
||||
| Experiment 31 Reporting the Activity Data of This PDC | [4] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Diarrhea |
27%
|
|||
| Patients Enrolled |
157 patients with multiple myeloma.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melflufen is a first-in-class peptide-drug conjugate, targeting aminopeptidase which has an increased expression in fast-growing and aggressive malignancies. The lipophilicity of melflufen allows for passive diffusion, selectively targeting myeloma cells. Once inside the cell, melflufen is hydrolyzed to active alkylating metabolites melphalan and desethyl-melflufen. Melflufen and the active metabolites trigger irreversible DNA damage, inhibit proliferation, induces apoptosis, and express antiangiogenic effects. In addition, melflufen demonstrated activity in myeloma cells with documented impaired or absent Tp53 expression and documented resistance to bortezomib, dexamethasone, and melphalan.
Click to Show/Hide
|
||||
| Description |
Based on the safety data collected during the HORIZON trial, treatment emergent adverse events occurred in 100% of patients including 100 patients (64%) having at least 1 CTCAE grade 4 adverse effect. Hematologic grade 3 or 4 adverse effects including thrombocytopenia (76%), neutropenia (79%), anemia (43%), and infections (11%) were the most commonly reported. Other adverse effects, such as fatigue (55%), nausea (32%), diarrhea (27%), and decreased appetite (14%), were similar to other alkylating agents. Pyrexia (24%), including febrile neutropenia (5%), and respiratory tract infections (24%) were contributed to hematologic toxicities.
Click to Show/Hide
|
||||
| Experiment 32 Reporting the Activity Data of This PDC | [1] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Diarrhea |
24.00%
|
|||
| Patients Enrolled |
Patients with multi-refractory multiple myeloma.
|
||||
| MOA of PDC |
Melflufen is highly lipophilic, which promotes its rapid uptake by cells. Once within the cell, melflufen releases its hydrophilic alkylator payloads via the hydrolytic activity of intracellular peptidases (e.g., aminopeptidases). Aminopeptidases are Zn2+-dependent metalloproteinases that remove amino acids at the N-terminal position from oligopeptides and have been associated with multiple tumorigenic processes such as proliferation, apoptosis, differentiation, angiogenesis, and motility. The dependence of melflufen on aminopeptidases was initially demonstrated by the reduced cytotoxic activity of melflufen-but not the alkylator melphalan-when cells were pretreated with bestatin, an antibiotic that is a potent aminopeptidase inhibitor. In addition, structure analogs designed to resist peptide hydrolysis (N-methyl derivative and derivative with D-amino acid) were shown to be almost 100-fold less potent than melflufen. Subsequent in vitro studies demonstrated that hydrolytic cleavage of melflufen by aminopeptidases releases alkylator payloads, including melphalan. In vitro, the activity of melflufen is multi-pronged, including induction of DNA damage, induction of apoptosis, inhibition of VEGF-dependent cell migration, and inhibition of tumor-associated angiogenesis, which have been further reviewed elsewhere. Downregulation of aminopeptidases resulted in reduced melflufen-mediated cytotoxic activity and apoptotic signaling in cultured cells.
Click to Show/Hide
|
||||
| Description |
Melflufen plus dexamethasone was generally manageable in this heavily pretreated patient population [51]. All patients experienced ≥1 AE, most commonly hematologic AEs including thrombocytopenia (73%), neutropenia (69%), and anemia (64%). The most common non-hematologic AEs included pyrexia (40%), asthenia (31%), fatigue (29%), nausea (27%), and diarrhea (24%).
Click to Show/Hide
|
||||
| Experiment 33 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Fatigue |
7.10%
|
|||
| Patients Enrolled |
14 patients with relapsed refractory multiple myeloma.
|
||||
| Administration Time | 28-day cycle | ||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (melflufen) is a first-in-class peptide-drug conjugate that utilizes increased peptidase expression to selectively release potent alkylating agents inside tumor cells. Melflufen is hydrolyzed by peptidases and esterases to melphalan either directly or through an intermediate metabolite, desethyl-melflufen. The high lipophilicity of melflufen facilitates passive diffusion across cell membranes. The activity and tolerability of melflufen in relapsed/refractory multiple myeloma (RRMM) were demonstrated in the O-12-M1 (NCT01897714), OCEAN (NCT03151811), and HORIZON (NCT02963493) trials.
Click to Show/Hide
|
||||
| Description |
Overall, at least one TEAE was reported in 13 (92.9%) and 13 (100.0%) patients in Arms A and B, respectively (Table 3). During cycle 1, 9 patients (64.3%) and 12 patients (92.3%), respectively, had at least one TEAE. Cumulatively, grade 3 or 4 AEs occurred in 12 (85.7%) and 12 (92.3%) patients, respectively, and serious AEs were reported in 5 (35.7%) and 9 (69.2%) patients, respectively. The most common any-grade AEs in Arms A and B, respectively, were thrombocytopenia (10 [71.4%]; 10 [76.9%]), neutropenia (9 [64.3%]; 9 [69.2%]), and anemia (9 [64.3%]; 7 [53.8%]). No phlebitis or local-infusion-related reactions were reported based on pre- and post-infusion inspection of the IV site, and there were no extravasations observed in Arm A or B. Similarly, VIP scores collected on Day 1 post-infusion and on Day 8 indicated that patients had healthy IV sites (VIP score of 0) with no signs of phlebitis following PVC administration of melflufen. The most common non-hematological AE was positive SARS-CoV-2 test (Arm A: 2 [14.3%]; Arm B: 4 [30.8%]). Pneumonia was the most common serious AE (Arm A: 2 [14.3%]; Arm B: 2 [15.4%]). The most common AE considered related to melflufen and/or dexamethasone by investigators was thrombocytopenia (Arm A: 10 [71.4%]; Arm B: 10 [76.9%]). AEs led to treatment discontinuation in 3 (21.4%) and 6 (46.2%) patients in Arms A and B, respectively.
Click to Show/Hide
|
||||
| Half life period | 75.6 h | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT04412707 | Clinical Status | Phase 2 | ||
| Clinical Description | This is a randomized, two-period, cross-over Phase 2 study, comparing PK, and assessing safety and tolerability and efficacy of peripheral and central intravenous administration of melflufen in patients with RRMM. It is an international study, enrolling patients in US and Europe. The study will enroll patients following at least 2 lines of prior therapy. | ||||
| Experiment 34 Reporting the Activity Data of This PDC | [4] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Fatigue |
55%
|
|||
| Patients Enrolled |
157 patients with multiple myeloma.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melflufen is a first-in-class peptide-drug conjugate, targeting aminopeptidase which has an increased expression in fast-growing and aggressive malignancies. The lipophilicity of melflufen allows for passive diffusion, selectively targeting myeloma cells. Once inside the cell, melflufen is hydrolyzed to active alkylating metabolites melphalan and desethyl-melflufen. Melflufen and the active metabolites trigger irreversible DNA damage, inhibit proliferation, induces apoptosis, and express antiangiogenic effects. In addition, melflufen demonstrated activity in myeloma cells with documented impaired or absent Tp53 expression and documented resistance to bortezomib, dexamethasone, and melphalan.
Click to Show/Hide
|
||||
| Description |
Based on the safety data collected during the HORIZON trial, treatment emergent adverse events occurred in 100% of patients including 100 patients (64%) having at least 1 CTCAE grade 4 adverse effect. Hematologic grade 3 or 4 adverse effects including thrombocytopenia (76%), neutropenia (79%), anemia (43%), and infections (11%) were the most commonly reported. Other adverse effects, such as fatigue (55%), nausea (32%), diarrhea (27%), and decreased appetite (14%), were similar to other alkylating agents. Pyrexia (24%), including febrile neutropenia (5%), and respiratory tract infections (24%) were contributed to hematologic toxicities.
Click to Show/Hide
|
||||
| Experiment 35 Reporting the Activity Data of This PDC | [1] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Fatigue |
29%
|
|||
| Patients Enrolled |
Patients with multi-refractory multiple myeloma.
|
||||
| MOA of PDC |
Melflufen is highly lipophilic, which promotes its rapid uptake by cells. Once within the cell, melflufen releases its hydrophilic alkylator payloads via the hydrolytic activity of intracellular peptidases (e.g., aminopeptidases). Aminopeptidases are Zn2+-dependent metalloproteinases that remove amino acids at the N-terminal position from oligopeptides and have been associated with multiple tumorigenic processes such as proliferation, apoptosis, differentiation, angiogenesis, and motility. The dependence of melflufen on aminopeptidases was initially demonstrated by the reduced cytotoxic activity of melflufen-but not the alkylator melphalan-when cells were pretreated with bestatin, an antibiotic that is a potent aminopeptidase inhibitor. In addition, structure analogs designed to resist peptide hydrolysis (N-methyl derivative and derivative with D-amino acid) were shown to be almost 100-fold less potent than melflufen. Subsequent in vitro studies demonstrated that hydrolytic cleavage of melflufen by aminopeptidases releases alkylator payloads, including melphalan. In vitro, the activity of melflufen is multi-pronged, including induction of DNA damage, induction of apoptosis, inhibition of VEGF-dependent cell migration, and inhibition of tumor-associated angiogenesis, which have been further reviewed elsewhere. Downregulation of aminopeptidases resulted in reduced melflufen-mediated cytotoxic activity and apoptotic signaling in cultured cells.
Click to Show/Hide
|
||||
| Description |
Melflufen plus dexamethasone was generally manageable in this heavily pretreated patient population [51]. All patients experienced ≥1 AE, most commonly hematologic AEs including thrombocytopenia (73%), neutropenia (69%), and anemia (64%). The most common non-hematologic AEs included pyrexia (40%), asthenia (31%), fatigue (29%), nausea (27%), and diarrhea (24%).
Click to Show/Hide
|
||||
| Experiment 36 Reporting the Activity Data of This PDC | [1] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade ≥3 adverse event |
82%
|
|||
| Patients Enrolled |
Patients with multi-refractory multiple myeloma.
|
||||
| MOA of PDC |
Melflufen is highly lipophilic, which promotes its rapid uptake by cells. Once within the cell, melflufen releases its hydrophilic alkylator payloads via the hydrolytic activity of intracellular peptidases (e.g., aminopeptidases). Aminopeptidases are Zn2+-dependent metalloproteinases that remove amino acids at the N-terminal position from oligopeptides and have been associated with multiple tumorigenic processes such as proliferation, apoptosis, differentiation, angiogenesis, and motility. The dependence of melflufen on aminopeptidases was initially demonstrated by the reduced cytotoxic activity of melflufen-but not the alkylator melphalan-when cells were pretreated with bestatin, an antibiotic that is a potent aminopeptidase inhibitor. In addition, structure analogs designed to resist peptide hydrolysis (N-methyl derivative and derivative with D-amino acid) were shown to be almost 100-fold less potent than melflufen. Subsequent in vitro studies demonstrated that hydrolytic cleavage of melflufen by aminopeptidases releases alkylator payloads, including melphalan. In vitro, the activity of melflufen is multi-pronged, including induction of DNA damage, induction of apoptosis, inhibition of VEGF-dependent cell migration, and inhibition of tumor-associated angiogenesis, which have been further reviewed elsewhere. Downregulation of aminopeptidases resulted in reduced melflufen-mediated cytotoxic activity and apoptotic signaling in cultured cells.
Click to Show/Hide
|
||||
| Description |
Melflufen-related Grade ≥3 AEs occurred in 82% of patients.
|
||||
| Experiment 37 Reporting the Activity Data of This PDC | [1] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade ≥3 treatment-emergent adverse event |
82%
|
|||
| Patients Enrolled |
Patients with multi-refractory multiple myeloma.
|
||||
| Administration Time | 28-day cycle | ||||
| Administration Dosage | 40 mg with dexamethasone (40 mg) | ||||
| MOA of PDC |
Melflufen is highly lipophilic, which promotes its rapid uptake by cells. Once within the cell, melflufen releases its hydrophilic alkylator payloads via the hydrolytic activity of intracellular peptidases (e.g., aminopeptidases). Aminopeptidases are Zn2+-dependent metalloproteinases that remove amino acids at the N-terminal position from oligopeptides and have been associated with multiple tumorigenic processes such as proliferation, apoptosis, differentiation, angiogenesis, and motility. The dependence of melflufen on aminopeptidases was initially demonstrated by the reduced cytotoxic activity of melflufen-but not the alkylator melphalan-when cells were pretreated with bestatin, an antibiotic that is a potent aminopeptidase inhibitor. In addition, structure analogs designed to resist peptide hydrolysis (N-methyl derivative and derivative with D-amino acid) were shown to be almost 100-fold less potent than melflufen. Subsequent in vitro studies demonstrated that hydrolytic cleavage of melflufen by aminopeptidases releases alkylator payloads, including melphalan. In vitro, the activity of melflufen is multi-pronged, including induction of DNA damage, induction of apoptosis, inhibition of VEGF-dependent cell migration, and inhibition of tumor-associated angiogenesis, which have been further reviewed elsewhere. Downregulation of aminopeptidases resulted in reduced melflufen-mediated cytotoxic activity and apoptotic signaling in cultured cells.
Click to Show/Hide
|
||||
| Experiment 38 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 1-2 abdominal mass |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 39 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 1-2 anaemia |
24%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 40 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 1-2 asthenia |
12%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 41 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 1-2 brain oedema |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 42 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 1-2 bronchitis |
4%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 43 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 1-2 cardiac arrest |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 44 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 1-2 cardiac failure acute |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 45 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 1-2 cerebral haemorrhage |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 46 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 1-2 cerebrovascular insufficiency |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 47 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 1-2 constipation |
7%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 48 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 1-2 covid-19 pneumonia |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 49 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 1-2 craniocerebral injury |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 50 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 1-2 death for unknown reason |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 51 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 1-2 diarrhoea |
12%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 52 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 1-2 escherichia sepsis |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 53 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 1-2 fatigue |
14%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 54 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 1-2 general physical health deterioration | < 1% | |||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 55 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 1-2 haematological treatment-emergent adverse event |
8%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 56 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 1-2 leukopenia |
4%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 57 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 1-2 lower respiratory tract infection |
1%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 58 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 1-2 lymphopenia |
1%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 59 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 1-2 multiple organ dysfunction syndrome |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 60 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 1-2 myelodysplastic syndromes | < 1% | |||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 61 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 1-2 nausea |
13%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 62 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 1-2 neutropenia |
6%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 63 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 1-2 neutrophil count decreased |
1%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 64 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 1-2 non-haematological treatment-emergent adverse event |
44%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 65 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 1-2 oesophageal carcinoma |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 66 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 1-2 pancytopenia |
1%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 67 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 1-2 platelet count decreased |
3%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 68 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 1-2 pleural effusion | < 1% | |||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 69 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 1-2 pneumonia |
3%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 70 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 1-2 post-procedural complication |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 71 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 1-2 pulmonary embolism |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 72 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 1-2 pulmonary oedema |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 73 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 1-2 pyrexia |
13%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 74 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 1-2 renal failure |
1%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 75 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 1-2 respiratory arrest |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 76 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 1-2 respiratory failure |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 77 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 1-2 sepsis | < 1% | |||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 78 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 1-2 septic shock |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 79 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 1-2 subdural haematoma |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 80 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 1-2 sudden cardiac death |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 81 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 1-2 sudden death |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 82 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 1-2 thrombocytopenia |
7%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 83 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 1-2 upper respiratory tract infection |
11%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 84 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 1-2 urinary tract infection |
4%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 85 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 1-2 white blood cell count decreased |
4%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 86 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 3 abdominal mass |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 87 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 3 anaemia |
40%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 88 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 3 asthenia |
2%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 89 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 3 brain oedema |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 90 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 3 bronchitis |
1%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 91 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 3 cardiac arrest |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 92 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 3 cardiac failure acute |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 93 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 3 cerebral haemorrhage |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 94 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 3 cerebrovascular insufficiency |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 95 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 3 constipation |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 96 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 3 covid-19 pneumonia |
2%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 97 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 3 craniocerebral injury |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 98 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 3 death for unknown reason |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 99 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 3 diarrhoea |
1%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 100 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 3 escherichia sepsis |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 101 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 3 fatigue |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 102 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 3 general physical health deterioration |
1%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 103 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 3 haematological treatment-emergent adverse event |
33%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 104 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 3 leukopenia |
6%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 105 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 3 lower respiratory tract infection |
1%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 106 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 3 lymphopenia |
2%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 107 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 3 multiple organ dysfunction syndrome |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 108 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 3 myelodysplastic syndromes |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 109 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 3 nausea | < 1% | |||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 110 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 3 neutropenia |
28%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 111 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 3 neutrophil count decreased |
8%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 112 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 3 non-haematological treatment-emergent adverse event |
32%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 113 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 3 oesophageal carcinoma |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 114 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 3 pancytopenia | < 1% | |||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 115 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 3 platelet count decreased |
8%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 116 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 3 pleural effusion |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 117 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 3 pneumonia |
4%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 118 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 3 post-procedural complication |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 119 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 3 pulmonary embolism |
1%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 120 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 3 pulmonary oedema |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 121 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 3 pyrexia |
1%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 122 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 3 renal failure |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 123 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 3 respiratory arrest |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 124 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 3 respiratory failure | < 1% | |||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 125 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 3 sepsis | < 1% | |||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 126 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 3 septic shock |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 127 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 3 subdural haematoma |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 128 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 3 sudden cardiac death |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 129 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 3 sudden death |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 130 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 3 thrombocytopenia |
32%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 131 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 3 upper respiratory tract infection |
1%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 132 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 3 urinary tract infection |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 133 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 3 white blood cell count decreased |
3%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 134 Reporting the Activity Data of This PDC | [1] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 3/4 adverse events |
85%
|
|||
| Patients Enrolled |
Patients with multi-refractory multiple myeloma.
|
||||
| Administration Time | 14.3 week (median) | ||||
| Administration Dosage | 40 mg with dexamethasone (40 mg) | ||||
| MOA of PDC |
Melflufen is highly lipophilic, which promotes its rapid uptake by cells. Once within the cell, melflufen releases its hydrophilic alkylator payloads via the hydrolytic activity of intracellular peptidases (e.g., aminopeptidases). Aminopeptidases are Zn2+-dependent metalloproteinases that remove amino acids at the N-terminal position from oligopeptides and have been associated with multiple tumorigenic processes such as proliferation, apoptosis, differentiation, angiogenesis, and motility. The dependence of melflufen on aminopeptidases was initially demonstrated by the reduced cytotoxic activity of melflufen-but not the alkylator melphalan-when cells were pretreated with bestatin, an antibiotic that is a potent aminopeptidase inhibitor. In addition, structure analogs designed to resist peptide hydrolysis (N-methyl derivative and derivative with D-amino acid) were shown to be almost 100-fold less potent than melflufen. Subsequent in vitro studies demonstrated that hydrolytic cleavage of melflufen by aminopeptidases releases alkylator payloads, including melphalan. In vitro, the activity of melflufen is multi-pronged, including induction of DNA damage, induction of apoptosis, inhibition of VEGF-dependent cell migration, and inhibition of tumor-associated angiogenesis, which have been further reviewed elsewhere. Downregulation of aminopeptidases resulted in reduced melflufen-mediated cytotoxic activity and apoptotic signaling in cultured cells.
Click to Show/Hide
|
||||
| Experiment 135 Reporting the Activity Data of This PDC | [1] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 3/4 adverse events |
85%
|
|||
| MOA of PDC |
Melflufen is highly lipophilic, which promotes its rapid uptake by cells. Once within the cell, melflufen releases its hydrophilic alkylator payloads via the hydrolytic activity of intracellular peptidases (e.g., aminopeptidases). Aminopeptidases are Zn2+-dependent metalloproteinases that remove amino acids at the N-terminal position from oligopeptides and have been associated with multiple tumorigenic processes such as proliferation, apoptosis, differentiation, angiogenesis, and motility. The dependence of melflufen on aminopeptidases was initially demonstrated by the reduced cytotoxic activity of melflufen-but not the alkylator melphalan-when cells were pretreated with bestatin, an antibiotic that is a potent aminopeptidase inhibitor. In addition, structure analogs designed to resist peptide hydrolysis (N-methyl derivative and derivative with D-amino acid) were shown to be almost 100-fold less potent than melflufen. Subsequent in vitro studies demonstrated that hydrolytic cleavage of melflufen by aminopeptidases releases alkylator payloads, including melphalan. In vitro, the activity of melflufen is multi-pronged, including induction of DNA damage, induction of apoptosis, inhibition of VEGF-dependent cell migration, and inhibition of tumor-associated angiogenesis, which have been further reviewed elsewhere. Downregulation of aminopeptidases resulted in reduced melflufen-mediated cytotoxic activity and apoptotic signaling in cultured cells.
Click to Show/Hide
|
||||
| Description |
Overall, 97% of patients experienced any-grade AEs and 85% of patients experienced Grades 3/4 AEs.
|
||||
| In Vivo Model | 75 patients with multiple myeloma. | ||||
| Experiment 136 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 4 abdominal mass |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 137 Reporting the Activity Data of This PDC | [4] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 4 adverse effect |
64%
|
|||
| Patients Enrolled |
157 patients with multiple myeloma.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melflufen is a first-in-class peptide-drug conjugate, targeting aminopeptidase which has an increased expression in fast-growing and aggressive malignancies. The lipophilicity of melflufen allows for passive diffusion, selectively targeting myeloma cells. Once inside the cell, melflufen is hydrolyzed to active alkylating metabolites melphalan and desethyl-melflufen. Melflufen and the active metabolites trigger irreversible DNA damage, inhibit proliferation, induces apoptosis, and express antiangiogenic effects. In addition, melflufen demonstrated activity in myeloma cells with documented impaired or absent Tp53 expression and documented resistance to bortezomib, dexamethasone, and melphalan.
Click to Show/Hide
|
||||
| Description |
Based on the safety data collected during the HORIZON trial, treatment emergent adverse events occurred in 100% of patients including 100 patients (64%) having at least 1 CTCAE grade 4 adverse effect. Hematologic grade 3 or 4 adverse effects including thrombocytopenia (76%), neutropenia (79%), anemia (43%), and infections (11%) were the most commonly reported. Other adverse effects, such as fatigue (55%), nausea (32%), diarrhea (27%), and decreased appetite (14%), were similar to other alkylating agents. Pyrexia (24%), including febrile neutropenia (5%), and respiratory tract infections (24%) were contributed to hematologic toxicities.
Click to Show/Hide
|
||||
| Experiment 138 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 4 anaemia |
2%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 139 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 4 asthenia |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 140 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 4 brain oedema |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 141 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 4 bronchitis |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 142 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 4 cardiac arrest |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 143 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 4 cardiac failure acute |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 144 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 4 cerebral haemorrhage |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 145 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 4 cerebrovascular insufficiency |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 146 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 4 constipation |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 147 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 4 covid-19 pneumonia |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 148 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 4 craniocerebral injury |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 149 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 4 death for unknown reason |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 150 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 4 diarrhoea |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 151 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 4 escherichia sepsis | < 1% | |||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 152 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 4 fatigue |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 153 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 4 general physical health deterioration |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 154 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 4 haematological treatment-emergent adverse event |
53%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 155 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 4 leukopenia |
1%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 156 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 4 lower respiratory tract infection |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 157 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 4 lymphopenia |
2%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 158 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 4 multiple organ dysfunction syndrome |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 159 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 4 myelodysplastic syndromes |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 160 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 4 nausea |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 161 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 4 neutropenia |
26%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 162 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 4 neutrophil count decreased |
4%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 163 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 4 non-haematological treatment-emergent adverse event |
2%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 164 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 4 oesophageal carcinoma |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 165 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 4 pancytopenia | < 1% | |||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 166 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 4 platelet count decreased |
7%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 167 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 4 pleural effusion |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 168 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 4 pneumonia |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 169 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 4 post-procedural complication |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 170 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 4 pulmonary embolism |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 171 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 4 pulmonary oedema |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 172 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 4 pyrexia |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 173 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 4 renal failure |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 174 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 4 respiratory arrest |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 175 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 4 respiratory failure | < 1% | |||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 176 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 4 sepsis |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 177 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 4 septic shock |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 178 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 4 subdural haematoma |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 179 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 4 sudden cardiac death |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 180 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 4 sudden death |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 181 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 4 thrombocytopenia |
31%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 182 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 4 upper respiratory tract infection |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 183 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 4 urinary tract infection |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 184 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 4 white blood cell count decreased |
3%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 185 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 5 abdominal mass |
1%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 186 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 5 asthenia | < 1% | |||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 187 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 5 brain oedema | < 1% | |||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 188 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 5 bronchitis |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 189 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 5 cardiac arrest | < 1% | |||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 190 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 5 cardiac failure acute | < 1% | |||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 191 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 5 cerebral haemorrhage | < 1% | |||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 192 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 5 cerebrovascular insufficiency |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 193 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 5 constipation |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 194 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 5 covid-19 pneumonia |
3%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 195 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 5 craniocerebral injury |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 196 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 5 death for unknown reason |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 197 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 5 diarrhoea |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 198 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 5 escherichia sepsis |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 199 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 5 fatigue |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 200 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 5 general physical health deterioration |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 201 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 5 haematological treatment-emergent adverse event |
1%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 202 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 5 lower respiratory tract infection |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 203 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 5 multiple organ dysfunction syndrome |
1%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 204 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 5 myelodysplastic syndromes |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 205 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 5 nausea |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 206 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 5 neutropenia | < 1% | |||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 207 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 5 non-haematological treatment-emergent adverse event |
11%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 208 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 5 oesophageal carcinoma | < 1% | |||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 209 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 5 pancytopenia | < 1% | |||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 210 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 5 pleural effusion |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 211 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 5 pneumonia |
1%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 212 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 5 post-procedural complication | < 1% | |||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 213 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 5 pulmonary embolism | < 1% | |||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 214 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 5 pulmonary oedema | < 1% | |||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 215 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 5 pyrexia |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 216 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 5 renal failure |
1%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 217 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 5 respiratory arrest |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 218 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 5 respiratory failure |
1%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 219 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 5 sepsis |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 220 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 5 septic shock |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 221 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 5 subdural haematoma | < 1% | |||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 222 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 5 sudden cardiac death |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 223 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 5 sudden death |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 224 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 5 upper respiratory tract infection |
0%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 225 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Grade 5 urinary tract infection |
1%
|
|||
| Patients Enrolled |
228 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 226 Reporting the Activity Data of This PDC | [8] | ||||
| Indication | lymphoma | ||||
| Efficacy Data | Half Maximal Inhibitory Concentration (IC50) |
0.078 μM
|
|||
| Description |
The cytotoxicity of melflufen in primary human lymphoma cells, plotted as dose response curves with survival index (SI %) for each concentration tested. Sensitivity towards melflufen varied considerably (>300 fold) and the IC50range from 2.7 nM to 0.55 uM. The efficacy of melflufen corresponded to a 13- to 455-fold potency improvement (p< 0.001) compared to melphalan.
Click to Show/Hide
|
||||
| In Vitro Model | Lymphoma | Primary human lymphoma cell | Homo sapiens | ||
| Experiment 227 Reporting the Activity Data of This PDC | [9] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Hazard ratio |
62%
|
|||
| Patients Enrolled |
37 relapsed/refractory multiple myeloma patients aged 75 years.
|
||||
| MOA of PDC |
In summary, the interpretation of the results from the OCEAN study were impacted by the heterogeneity of the population, with age and previous success of ASCT therapy identified as prognostic factors with study therapies. The safety profile of melflufen and dexamethasone is primarily characterized by hematologic AEs that are clinically manageable. Observed infection rates, which included COVID-19, were generally low. Taken together, these data support the use of melflufen and dexamethasone in patients who have not received a previous ASCT or who underwent a successful ASCT (ie, TTP >36 months post-ASCT). In addition, the favorable efficacy profile and convenience of monthly outpatient infusions, especially for patients without access to other therapeutics such as CAR T-cell therapy or bispecific antibodies, bode well for this combination translating successfully into real-world practice.
Click to Show/Hide
|
||||
| Description |
In this updated survival analysis, median OS (95% CI) was 20.2 months (15.8-24.3) with melflufen and 24.0 months (19.1-28.7) with pomalidomide (HR, 1.14 [95% CI, 0.91-1.43]; P =.24), with a median follow-up time of 31.8 months and 29.8 months, respectively. Because of imbalance in the number of patients who were randomized but not treated, survival was also evaluated in the safety population: median OS (95% CI) was 21.3 months (16.6-24.8) with melflufen and 24.0 months (19.8-28.7) with pomalidomide (HR, 1.12 [95% CI, 0.89-1.42]; P =.33), with the curves overlapping until 10 months after randomization. Sensitivity analyses revealed that the uneven distribution of randomized but not treated patients impacted OS, but not PFS. Although a similar number of patients received subsequent therapy after OCEAN (melflufen group, 169/246 [69%] patients; pomalidomide group, 164/249 [66%] patients), the type of subsequent therapy and timing of subsequent therapy initiation differed between treatment groups.
Click to Show/Hide
|
||||
| Experiment 228 Reporting the Activity Data of This PDC | [9] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Hazard ratio |
103%
|
|||
| Patients Enrolled |
113 relapsed/refractory multiple myeloma patients aged 65-74 years.
|
||||
| MOA of PDC |
In summary, the interpretation of the results from the OCEAN study were impacted by the heterogeneity of the population, with age and previous success of ASCT therapy identified as prognostic factors with study therapies. The safety profile of melflufen and dexamethasone is primarily characterized by hematologic AEs that are clinically manageable. Observed infection rates, which included COVID-19, were generally low. Taken together, these data support the use of melflufen and dexamethasone in patients who have not received a previous ASCT or who underwent a successful ASCT (ie, TTP >36 months post-ASCT). In addition, the favorable efficacy profile and convenience of monthly outpatient infusions, especially for patients without access to other therapeutics such as CAR T-cell therapy or bispecific antibodies, bode well for this combination translating successfully into real-world practice.
Click to Show/Hide
|
||||
| Description |
In this updated survival analysis, median OS (95% CI) was 20.2 months (15.8-24.3) with melflufen and 24.0 months (19.1-28.7) with pomalidomide (HR, 1.14 [95% CI, 0.91-1.43]; P =.24), with a median follow-up time of 31.8 months and 29.8 months, respectively. Because of imbalance in the number of patients who were randomized but not treated, survival was also evaluated in the safety population: median OS (95% CI) was 21.3 months (16.6-24.8) with melflufen and 24.0 months (19.8-28.7) with pomalidomide (HR, 1.12 [95% CI, 0.89-1.42]; P =.33), with the curves overlapping until 10 months after randomization. Sensitivity analyses revealed that the uneven distribution of randomized but not treated patients impacted OS, but not PFS. Although a similar number of patients received subsequent therapy after OCEAN (melflufen group, 169/246 [69%] patients; pomalidomide group, 164/249 [66%] patients), the type of subsequent therapy and timing of subsequent therapy initiation differed between treatment groups.
Click to Show/Hide
|
||||
| Experiment 229 Reporting the Activity Data of This PDC | [9] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Hazard ratio |
168%
|
|||
| Patients Enrolled |
96 relapsed/refractory multiple myeloma patients aged <65 years.
|
||||
| MOA of PDC |
In summary, the interpretation of the results from the OCEAN study were impacted by the heterogeneity of the population, with age and previous success of ASCT therapy identified as prognostic factors with study therapies. The safety profile of melflufen and dexamethasone is primarily characterized by hematologic AEs that are clinically manageable. Observed infection rates, which included COVID-19, were generally low. Taken together, these data support the use of melflufen and dexamethasone in patients who have not received a previous ASCT or who underwent a successful ASCT (ie, TTP >36 months post-ASCT). In addition, the favorable efficacy profile and convenience of monthly outpatient infusions, especially for patients without access to other therapeutics such as CAR T-cell therapy or bispecific antibodies, bode well for this combination translating successfully into real-world practice.
Click to Show/Hide
|
||||
| Description |
In this updated survival analysis, median OS (95% CI) was 20.2 months (15.8-24.3) with melflufen and 24.0 months (19.1-28.7) with pomalidomide (HR, 1.14 [95% CI, 0.91-1.43]; P =.24), with a median follow-up time of 31.8 months and 29.8 months, respectively. Because of imbalance in the number of patients who were randomized but not treated, survival was also evaluated in the safety population: median OS (95% CI) was 21.3 months (16.6-24.8) with melflufen and 24.0 months (19.8-28.7) with pomalidomide (HR, 1.12 [95% CI, 0.89-1.42]; P =.33), with the curves overlapping until 10 months after randomization. Sensitivity analyses revealed that the uneven distribution of randomized but not treated patients impacted OS, but not PFS. Although a similar number of patients received subsequent therapy after OCEAN (melflufen group, 169/246 [69%] patients; pomalidomide group, 164/249 [66%] patients), the type of subsequent therapy and timing of subsequent therapy initiation differed between treatment groups.
Click to Show/Hide
|
||||
| Experiment 230 Reporting the Activity Data of This PDC | [9] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Hemorrhage |
1%
|
|||
| Patients Enrolled |
101 relapsed/refractory multiple myeloma patients with TTP <36 month Post-ASCTb.
|
||||
| MOA of PDC |
In summary, the interpretation of the results from the OCEAN study were impacted by the heterogeneity of the population, with age and previous success of ASCT therapy identified as prognostic factors with study therapies. The safety profile of melflufen and dexamethasone is primarily characterized by hematologic AEs that are clinically manageable. Observed infection rates, which included COVID-19, were generally low. Taken together, these data support the use of melflufen and dexamethasone in patients who have not received a previous ASCT or who underwent a successful ASCT (ie, TTP >36 months post-ASCT). In addition, the favorable efficacy profile and convenience of monthly outpatient infusions, especially for patients without access to other therapeutics such as CAR T-cell therapy or bispecific antibodies, bode well for this combination translating successfully into real-world practice.
Click to Show/Hide
|
||||
| Description |
Given the prognostic importance of TTP <36 months post-ASCT in OCEAN, we evaluated this prognostic factor in a post hoc analysis from the HORIZON study. Among 110 patients with triple-class refractory disease who had received ≥3 prior lines of therapy, 77 (70%) had received a previous ASCT and 58 (53%) had TTP <36 months post-ASCT (Suppl. Table S3). In patients with a TTP >36 months post-ASCT or no ASCT versus patients with a TTP <36 months post-ASCT, ORR was higher (29% vs 22%; Suppl. Table S4) and median DOR (7.6 months vs 3.9 months) and median PFS (4.2 months vs 3.4 months) were longer. Since pomalidomide and lenalidomide both belong to the immunomodulatory drugs, we analyzed if the duration of previous treatment with lenalidomide could have impacted the results. The median duration of lenalidomide was 14.4 months in patients with ASCT and TTP < 36 months, 38.3 months in patients with ASCT and TTP > 36 months, and 14.6 months in patients with no previous ASCT. However, the median PFS for patients treated with pomalidomide did not differ substantially between these groups of patients. The safety profile of melflufen and dexamethasone was generally consistent between patients with a TTP >36 months post-ASCT or no ASCT and patients with a TTP <36 months post-ASCT. In OCEAN among the melflufen group, the frequency of grade 3/4 TEAEs (88% and 92%), serious TEAEs (44% and 38%), and fatal adverse events (AEs; 11% and 13%) was similar in patients with a TTP >36 months post-ASCT or no ASCT and patients with TTP <36 months. However, patients with a TTP >36 months post-ASCT or no ASCT had lower rates of TEAEs leading to treatment discontinuation (23% and 31%), the longer median duration of study treatment (35.1 weeks vs 15.1 weeks), and longer median time to experiencing grade 3/4 thrombocytopenia (11.2 weeks vs 4.1 weeks) and grade 3/4 neutropenia (4.8 weeks vs 2.1 weeks) than patients with a TTP <36 months post-ASCT. In HORIZON, patients with a TTP >36 months post-ASCT or no ASCT had lower rates of grade 3/4 TEAEs (88% and 98%), but higher rates of serious TEAEs (64% and 53%) and similar rates of TEAEs leading to treatment discontinuation (29% and 33%) than patients with a TTP <36 months post-ASCT.
Click to Show/Hide
|
||||
| Experiment 231 Reporting the Activity Data of This PDC | [9] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Hemorrhage |
3%
|
|||
| Patients Enrolled |
145 patients who has relapsed/refractory multiple myeloma with no previous ASCT or TTP >36 month Post-ASCTa.
|
||||
| MOA of PDC |
In summary, the interpretation of the results from the OCEAN study were impacted by the heterogeneity of the population, with age and previous success of ASCT therapy identified as prognostic factors with study therapies. The safety profile of melflufen and dexamethasone is primarily characterized by hematologic AEs that are clinically manageable. Observed infection rates, which included COVID-19, were generally low. Taken together, these data support the use of melflufen and dexamethasone in patients who have not received a previous ASCT or who underwent a successful ASCT (ie, TTP >36 months post-ASCT). In addition, the favorable efficacy profile and convenience of monthly outpatient infusions, especially for patients without access to other therapeutics such as CAR T-cell therapy or bispecific antibodies, bode well for this combination translating successfully into real-world practice.
Click to Show/Hide
|
||||
| Description |
Given the prognostic importance of TTP <36 months post-ASCT in OCEAN, we evaluated this prognostic factor in a post hoc analysis from the HORIZON study. Among 110 patients with triple-class refractory disease who had received ≥3 prior lines of therapy, 77 (70%) had received a previous ASCT and 58 (53%) had TTP <36 months post-ASCT (Suppl. Table S3). In patients with a TTP >36 months post-ASCT or no ASCT versus patients with a TTP <36 months post-ASCT, ORR was higher (29% vs 22%; Suppl. Table S4) and median DOR (7.6 months vs 3.9 months) and median PFS (4.2 months vs 3.4 months) were longer. Since pomalidomide and lenalidomide both belong to the immunomodulatory drugs, we analyzed if the duration of previous treatment with lenalidomide could have impacted the results. The median duration of lenalidomide was 14.4 months in patients with ASCT and TTP < 36 months, 38.3 months in patients with ASCT and TTP > 36 months, and 14.6 months in patients with no previous ASCT. However, the median PFS for patients treated with pomalidomide did not differ substantially between these groups of patients. The safety profile of melflufen and dexamethasone was generally consistent between patients with a TTP >36 months post-ASCT or no ASCT and patients with a TTP <36 months post-ASCT. In OCEAN among the melflufen group, the frequency of grade 3/4 TEAEs (88% and 92%), serious TEAEs (44% and 38%), and fatal adverse events (AEs; 11% and 13%) was similar in patients with a TTP >36 months post-ASCT or no ASCT and patients with TTP <36 months. However, patients with a TTP >36 months post-ASCT or no ASCT had lower rates of TEAEs leading to treatment discontinuation (23% and 31%), the longer median duration of study treatment (35.1 weeks vs 15.1 weeks), and longer median time to experiencing grade 3/4 thrombocytopenia (11.2 weeks vs 4.1 weeks) and grade 3/4 neutropenia (4.8 weeks vs 2.1 weeks) than patients with a TTP <36 months post-ASCT. In HORIZON, patients with a TTP >36 months post-ASCT or no ASCT had lower rates of grade 3/4 TEAEs (88% and 98%), but higher rates of serious TEAEs (64% and 53%) and similar rates of TEAEs leading to treatment discontinuation (29% and 33%) than patients with a TTP <36 months post-ASCT.
Click to Show/Hide
|
||||
| Experiment 232 Reporting the Activity Data of This PDC | [9] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Infection |
11%
|
|||
| Patients Enrolled |
101 relapsed/refractory multiple myeloma patients with TTP <36 month Post-ASCTb.
|
||||
| MOA of PDC |
In summary, the interpretation of the results from the OCEAN study were impacted by the heterogeneity of the population, with age and previous success of ASCT therapy identified as prognostic factors with study therapies. The safety profile of melflufen and dexamethasone is primarily characterized by hematologic AEs that are clinically manageable. Observed infection rates, which included COVID-19, were generally low. Taken together, these data support the use of melflufen and dexamethasone in patients who have not received a previous ASCT or who underwent a successful ASCT (ie, TTP >36 months post-ASCT). In addition, the favorable efficacy profile and convenience of monthly outpatient infusions, especially for patients without access to other therapeutics such as CAR T-cell therapy or bispecific antibodies, bode well for this combination translating successfully into real-world practice.
Click to Show/Hide
|
||||
| Description |
Given the prognostic importance of TTP <36 months post-ASCT in OCEAN, we evaluated this prognostic factor in a post hoc analysis from the HORIZON study. Among 110 patients with triple-class refractory disease who had received ≥3 prior lines of therapy, 77 (70%) had received a previous ASCT and 58 (53%) had TTP <36 months post-ASCT (Suppl. Table S3). In patients with a TTP >36 months post-ASCT or no ASCT versus patients with a TTP <36 months post-ASCT, ORR was higher (29% vs 22%; Suppl. Table S4) and median DOR (7.6 months vs 3.9 months) and median PFS (4.2 months vs 3.4 months) were longer. Since pomalidomide and lenalidomide both belong to the immunomodulatory drugs, we analyzed if the duration of previous treatment with lenalidomide could have impacted the results. The median duration of lenalidomide was 14.4 months in patients with ASCT and TTP < 36 months, 38.3 months in patients with ASCT and TTP > 36 months, and 14.6 months in patients with no previous ASCT. However, the median PFS for patients treated with pomalidomide did not differ substantially between these groups of patients. The safety profile of melflufen and dexamethasone was generally consistent between patients with a TTP >36 months post-ASCT or no ASCT and patients with a TTP <36 months post-ASCT. In OCEAN among the melflufen group, the frequency of grade 3/4 TEAEs (88% and 92%), serious TEAEs (44% and 38%), and fatal adverse events (AEs; 11% and 13%) was similar in patients with a TTP >36 months post-ASCT or no ASCT and patients with TTP <36 months. However, patients with a TTP >36 months post-ASCT or no ASCT had lower rates of TEAEs leading to treatment discontinuation (23% and 31%), the longer median duration of study treatment (35.1 weeks vs 15.1 weeks), and longer median time to experiencing grade 3/4 thrombocytopenia (11.2 weeks vs 4.1 weeks) and grade 3/4 neutropenia (4.8 weeks vs 2.1 weeks) than patients with a TTP <36 months post-ASCT. In HORIZON, patients with a TTP >36 months post-ASCT or no ASCT had lower rates of grade 3/4 TEAEs (88% and 98%), but higher rates of serious TEAEs (64% and 53%) and similar rates of TEAEs leading to treatment discontinuation (29% and 33%) than patients with a TTP <36 months post-ASCT.
Click to Show/Hide
|
||||
| Experiment 233 Reporting the Activity Data of This PDC | [9] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Infection |
15%
|
|||
| Patients Enrolled |
145 patients who has relapsed/refractory multiple myeloma with no previous ASCT or TTP >36 month Post-ASCTa.
|
||||
| MOA of PDC |
In summary, the interpretation of the results from the OCEAN study were impacted by the heterogeneity of the population, with age and previous success of ASCT therapy identified as prognostic factors with study therapies. The safety profile of melflufen and dexamethasone is primarily characterized by hematologic AEs that are clinically manageable. Observed infection rates, which included COVID-19, were generally low. Taken together, these data support the use of melflufen and dexamethasone in patients who have not received a previous ASCT or who underwent a successful ASCT (ie, TTP >36 months post-ASCT). In addition, the favorable efficacy profile and convenience of monthly outpatient infusions, especially for patients without access to other therapeutics such as CAR T-cell therapy or bispecific antibodies, bode well for this combination translating successfully into real-world practice.
Click to Show/Hide
|
||||
| Description |
Given the prognostic importance of TTP <36 months post-ASCT in OCEAN, we evaluated this prognostic factor in a post hoc analysis from the HORIZON study. Among 110 patients with triple-class refractory disease who had received ≥3 prior lines of therapy, 77 (70%) had received a previous ASCT and 58 (53%) had TTP <36 months post-ASCT (Suppl. Table S3). In patients with a TTP >36 months post-ASCT or no ASCT versus patients with a TTP <36 months post-ASCT, ORR was higher (29% vs 22%; Suppl. Table S4) and median DOR (7.6 months vs 3.9 months) and median PFS (4.2 months vs 3.4 months) were longer. Since pomalidomide and lenalidomide both belong to the immunomodulatory drugs, we analyzed if the duration of previous treatment with lenalidomide could have impacted the results. The median duration of lenalidomide was 14.4 months in patients with ASCT and TTP < 36 months, 38.3 months in patients with ASCT and TTP > 36 months, and 14.6 months in patients with no previous ASCT. However, the median PFS for patients treated with pomalidomide did not differ substantially between these groups of patients. The safety profile of melflufen and dexamethasone was generally consistent between patients with a TTP >36 months post-ASCT or no ASCT and patients with a TTP <36 months post-ASCT. In OCEAN among the melflufen group, the frequency of grade 3/4 TEAEs (88% and 92%), serious TEAEs (44% and 38%), and fatal adverse events (AEs; 11% and 13%) was similar in patients with a TTP >36 months post-ASCT or no ASCT and patients with TTP <36 months. However, patients with a TTP >36 months post-ASCT or no ASCT had lower rates of TEAEs leading to treatment discontinuation (23% and 31%), the longer median duration of study treatment (35.1 weeks vs 15.1 weeks), and longer median time to experiencing grade 3/4 thrombocytopenia (11.2 weeks vs 4.1 weeks) and grade 3/4 neutropenia (4.8 weeks vs 2.1 weeks) than patients with a TTP <36 months post-ASCT. In HORIZON, patients with a TTP >36 months post-ASCT or no ASCT had lower rates of grade 3/4 TEAEs (88% and 98%), but higher rates of serious TEAEs (64% and 53%) and similar rates of TEAEs leading to treatment discontinuation (29% and 33%) than patients with a TTP <36 months post-ASCT.
Click to Show/Hide
|
||||
| Experiment 234 Reporting the Activity Data of This PDC | [4] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Infection rate |
11%
|
|||
| Patients Enrolled |
157 patients with multiple myeloma.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melflufen is a first-in-class peptide-drug conjugate, targeting aminopeptidase which has an increased expression in fast-growing and aggressive malignancies. The lipophilicity of melflufen allows for passive diffusion, selectively targeting myeloma cells. Once inside the cell, melflufen is hydrolyzed to active alkylating metabolites melphalan and desethyl-melflufen. Melflufen and the active metabolites trigger irreversible DNA damage, inhibit proliferation, induces apoptosis, and express antiangiogenic effects. In addition, melflufen demonstrated activity in myeloma cells with documented impaired or absent Tp53 expression and documented resistance to bortezomib, dexamethasone, and melphalan.
Click to Show/Hide
|
||||
| Description |
Based on the safety data collected during the HORIZON trial, treatment emergent adverse events occurred in 100% of patients including 100 patients (64%) having at least 1 CTCAE grade 4 adverse effect. Hematologic grade 3 or 4 adverse effects including thrombocytopenia (76%), neutropenia (79%), anemia (43%), and infections (11%) were the most commonly reported. Other adverse effects, such as fatigue (55%), nausea (32%), diarrhea (27%), and decreased appetite (14%), were similar to other alkylating agents. Pyrexia (24%), including febrile neutropenia (5%), and respiratory tract infections (24%) were contributed to hematologic toxicities.
Click to Show/Hide
|
||||
| Experiment 235 Reporting the Activity Data of This PDC | [5] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Infections |
73.33%
|
|||
| Patients Enrolled |
153 patients refractory to prior alkylators (melflufen, n=78; pomalidomide, n=75).
|
||||
| MOA of PDC |
Melphalan flufenamide (melflufen), a first-in-class alkylating peptide-drug conjugate, plus dexamethasone demonstrated superior progression-free survival (PFS), but not overall survival (OS), versus pomalidomide plus dexamethasone in relapsed/refractory multiple myeloma in the OCEAN study. Time to progression (TTP) <36 months after a prior autologous stem cell transplantation (ASCT) was a negative prognostic factor for OS with melflufen. This post hoc exploratory analysis evaluated patients refractory to prior alkylators (e.g., cyclophosphamide and melphalan) in OCEAN. In 153 patients refractory to prior alkylators (melflufen, n = 78; pomalidomide, n = 75), the melflufen and pomalidomide arms had similar median PFS (5.6 months [95% CI, 4.2-8.3] vs. 4.7 months [95% CI, 3.1-7.3]; hazard ratio [HR], 0.92 [95% CI, 0.63-1.33]) and OS (23.4 months [95% CI, 14.4-31.7] vs. 20.0 months [95% CI, 12.0-28.7]; HR, 0.92 [95% CI, 0.62-1.38]). Among alkylator-refractory patients with a TTP 36 months after a prior ASCT or no prior ASCT (melflufen, n = 54; pomalidomide, n = 53), the observed median PFS and OS were longer in the melflufen arm than the pomalidomide arm. The safety profile of melflufen was consistent with previous reports. These results suggest that melflufen is safe and effective in patients with alkylator-refractory disease, suggesting differentiated activity from other alkylators.
Click to Show/Hide
|
||||
| Description |
Overall, the safety profile of melflufen plus dexamethasone in the alkylator-refractory group was consistent between treatment arms (Table 2). In the melflufen and pomalidomide arms, respectively, the frequency of treatment-emergent adverse events (TEAEs; 99% vs. 97%), Grade 3 or 4 TEAEs (85% vs. 82%), serious TEAEs (49% vs. 53%), and fatal TEAEs (19% vs. 16%) were similar (Table 2). However, melflufen compared with pomalidomide saw more dose modifications (76% vs. 67%) and dose reductions (47% vs. 14%), comparable dose delays (57% vs. 51%) but less treatment discontinuation (27% vs. 34%). When comparing patients refractory and not refractory to prior alkylators, rates of TEAEs were generally comparable except for slightly lower rates of serious and fatal TEAEs observed in patients not refractory to alkylators. Among Grade 3 or 4 TEAEs of special interest, melflufen saw more thrombocytopenia (73% vs. 14%), neutropenia (65% vs. 55%), and leukopenia or white blood cell decrease (14% vs. 3%), but less infection (15% vs. 26%), than pomalidomide. Notably, melflufen compared with pomalidomide saw a longer median time to dose reduction (106 days [range, 28-443] vs. 47 days [range, 28-225]), Grade 3 or 4 thrombocytopenia (52 days [range, 15-451] vs. 19 days [range, 8-91]), and Grade 3 or 4 neutropenia (36 days [range, 8-561] vs. 22 days [range, 8-470]).
Click to Show/Hide
|
||||
| Experiment 236 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Leukopenia |
14.30%
|
|||
| Patients Enrolled |
14 patients with relapsed refractory multiple myeloma.
|
||||
| Administration Time | 28-day cycle | ||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (melflufen) is a first-in-class peptide-drug conjugate that utilizes increased peptidase expression to selectively release potent alkylating agents inside tumor cells. Melflufen is hydrolyzed by peptidases and esterases to melphalan either directly or through an intermediate metabolite, desethyl-melflufen. The high lipophilicity of melflufen facilitates passive diffusion across cell membranes. The activity and tolerability of melflufen in relapsed/refractory multiple myeloma (RRMM) were demonstrated in the O-12-M1 (NCT01897714), OCEAN (NCT03151811), and HORIZON (NCT02963493) trials.
Click to Show/Hide
|
||||
| Description |
Overall, at least one TEAE was reported in 13 (92.9%) and 13 (100.0%) patients in Arms A and B, respectively (Table 3). During cycle 1, 9 patients (64.3%) and 12 patients (92.3%), respectively, had at least one TEAE. Cumulatively, grade 3 or 4 AEs occurred in 12 (85.7%) and 12 (92.3%) patients, respectively, and serious AEs were reported in 5 (35.7%) and 9 (69.2%) patients, respectively. The most common any-grade AEs in Arms A and B, respectively, were thrombocytopenia (10 [71.4%]; 10 [76.9%]), neutropenia (9 [64.3%]; 9 [69.2%]), and anemia (9 [64.3%]; 7 [53.8%]). No phlebitis or local-infusion-related reactions were reported based on pre- and post-infusion inspection of the IV site, and there were no extravasations observed in Arm A or B. Similarly, VIP scores collected on Day 1 post-infusion and on Day 8 indicated that patients had healthy IV sites (VIP score of 0) with no signs of phlebitis following PVC administration of melflufen. The most common non-hematological AE was positive SARS-CoV-2 test (Arm A: 2 [14.3%]; Arm B: 4 [30.8%]). Pneumonia was the most common serious AE (Arm A: 2 [14.3%]; Arm B: 2 [15.4%]). The most common AE considered related to melflufen and/or dexamethasone by investigators was thrombocytopenia (Arm A: 10 [71.4%]; Arm B: 10 [76.9%]). AEs led to treatment discontinuation in 3 (21.4%) and 6 (46.2%) patients in Arms A and B, respectively.
Click to Show/Hide
|
||||
| Half life period | 75.6 h | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT04412707 | Clinical Status | Phase 2 | ||
| Clinical Description | This is a randomized, two-period, cross-over Phase 2 study, comparing PK, and assessing safety and tolerability and efficacy of peripheral and central intravenous administration of melflufen in patients with RRMM. It is an international study, enrolling patients in US and Europe. The study will enroll patients following at least 2 lines of prior therapy. | ||||
| Experiment 237 Reporting the Activity Data of This PDC | [5] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Leukopenia |
71.43%
|
|||
| Patients Enrolled |
153 patients refractory to prior alkylators (melflufen, n=78; pomalidomide, n=75).
|
||||
| MOA of PDC |
Melphalan flufenamide (melflufen), a first-in-class alkylating peptide-drug conjugate, plus dexamethasone demonstrated superior progression-free survival (PFS), but not overall survival (OS), versus pomalidomide plus dexamethasone in relapsed/refractory multiple myeloma in the OCEAN study. Time to progression (TTP) <36 months after a prior autologous stem cell transplantation (ASCT) was a negative prognostic factor for OS with melflufen. This post hoc exploratory analysis evaluated patients refractory to prior alkylators (e.g., cyclophosphamide and melphalan) in OCEAN. In 153 patients refractory to prior alkylators (melflufen, n = 78; pomalidomide, n = 75), the melflufen and pomalidomide arms had similar median PFS (5.6 months [95% CI, 4.2-8.3] vs. 4.7 months [95% CI, 3.1-7.3]; hazard ratio [HR], 0.92 [95% CI, 0.63-1.33]) and OS (23.4 months [95% CI, 14.4-31.7] vs. 20.0 months [95% CI, 12.0-28.7]; HR, 0.92 [95% CI, 0.62-1.38]). Among alkylator-refractory patients with a TTP 36 months after a prior ASCT or no prior ASCT (melflufen, n = 54; pomalidomide, n = 53), the observed median PFS and OS were longer in the melflufen arm than the pomalidomide arm. The safety profile of melflufen was consistent with previous reports. These results suggest that melflufen is safe and effective in patients with alkylator-refractory disease, suggesting differentiated activity from other alkylators.
Click to Show/Hide
|
||||
| Description |
Overall, the safety profile of melflufen plus dexamethasone in the alkylator-refractory group was consistent between treatment arms (Table 2). In the melflufen and pomalidomide arms, respectively, the frequency of treatment-emergent adverse events (TEAEs; 99% vs. 97%), Grade 3 or 4 TEAEs (85% vs. 82%), serious TEAEs (49% vs. 53%), and fatal TEAEs (19% vs. 16%) were similar (Table 2). However, melflufen compared with pomalidomide saw more dose modifications (76% vs. 67%) and dose reductions (47% vs. 14%), comparable dose delays (57% vs. 51%) but less treatment discontinuation (27% vs. 34%). When comparing patients refractory and not refractory to prior alkylators, rates of TEAEs were generally comparable except for slightly lower rates of serious and fatal TEAEs observed in patients not refractory to alkylators. Among Grade 3 or 4 TEAEs of special interest, melflufen saw more thrombocytopenia (73% vs. 14%), neutropenia (65% vs. 55%), and leukopenia or white blood cell decrease (14% vs. 3%), but less infection (15% vs. 26%), than pomalidomide. Notably, melflufen compared with pomalidomide saw a longer median time to dose reduction (106 days [range, 28-443] vs. 47 days [range, 28-225]), Grade 3 or 4 thrombocytopenia (52 days [range, 15-451] vs. 19 days [range, 8-91]), and Grade 3 or 4 neutropenia (36 days [range, 8-561] vs. 22 days [range, 8-470]).
Click to Show/Hide
|
||||
| Experiment 238 Reporting the Activity Data of This PDC | [7] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Maximum tolerated dose |
40 mg
|
|||
| Administration Time | Intravenous (iv) infusion of 15 milligram (mg) melflufen on day 1 of each 21-day treatment cycle, in combination with 40 mg dexamet hasone (oral or iv) on days 1, 8 and 15 of each 21-day treatment cycle | ||||
| Administration Dosage | Melflufen 15 mg + Dexamethasone | ||||
| MOA of PDC |
The antineoplastic activity of melflufen is dependent upon the expression of aminopeptidases, like APN (also known as CD18), which cleave melflufen into melphalan and p-Fluorophenylalanine. Following aminopeptidase-dependent cleavage, the hydrophilic alkylating metabolite melphalan accumulates in myeloma cells. This enrichment of the cytotoxic payload has a substantial impact on the antimyeloma activity of melflufen.
Click to Show/Hide
|
||||
| Description |
In phase 1, the established maximum tolerated dose was 40 mg of melflufen in combination with dexamethasone.
|
||||
| In Vivo Model | Aged 18 years or older, had relapsed and refractory multiple myeloma, had received two or more previous lines of therapy (including lenalidomide and bortezomib). | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT01897714 | Clinical Status | Phase 1/2 | ||
| Clinical Description | The study will explore escalating doses of melflufen in combination with dexamethasone in small groups of patients to find the maximum tolerated dose of melflufen. That dose will then be used to determine the efficacy and safety profile of melflufen in combination with dexamethasone in a larger group of patients. | ||||
| Experiment 239 Reporting the Activity Data of This PDC | [7] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Maximum tolerated dose |
40 mg
|
|||
| Administration Time | Iv infusion of 25 mg melflufen on day 1 of each 21-day treatment cycle, in combination with 40 mg dexamet hasone (oral or iv) on days 1, 8 and 15 of each 21-day treatment cycle | ||||
| Administration Dosage | Melflufen 25 mg + Dexamethasone | ||||
| MOA of PDC |
The antineoplastic activity of melflufen is dependent upon the expression of aminopeptidases, like APN (also known as CD18), which cleave melflufen into melphalan and p-Fluorophenylalanine. Following aminopeptidase-dependent cleavage, the hydrophilic alkylating metabolite melphalan accumulates in myeloma cells. This enrichment of the cytotoxic payload has a substantial impact on the antimyeloma activity of melflufen.
Click to Show/Hide
|
||||
| Description |
In phase 1, the established maximum tolerated dose was 41 mg of melflufen in combination with dexamethasone.
|
||||
| In Vivo Model | Aged 18 years or older, had relapsed and refractory multiple myeloma, had received two or more previous lines of therapy (including lenalidomide and bortezomib). | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT01897714 | Clinical Status | Phase 1/2 | ||
| Clinical Description | The study will explore escalating doses of melflufen in combination with dexamethasone in small groups of patients to find the maximum tolerated dose of melflufen. That dose will then be used to determine the efficacy and safety profile of melflufen in combination with dexamethasone in a larger group of patients. | ||||
| Experiment 240 Reporting the Activity Data of This PDC | [7] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Maximum tolerated dose |
40 mg
|
|||
| Administration Time | Iv infusion of 40 mg melflufen on day 1 of each 21-day treatment cycle, in combination with 40 mg dexamet hasone (oral or iv) on days 1, 8 and 15 of each 21-day treatment cycle | ||||
| Administration Dosage | Melflufen 40 mg + Dexamethasone | ||||
| MOA of PDC |
The antineoplastic activity of melflufen is dependent upon the expression of aminopeptidases, like APN (also known as CD18), which cleave melflufen into melphalan and p-Fluorophenylalanine. Following aminopeptidase-dependent cleavage, the hydrophilic alkylating metabolite melphalan accumulates in myeloma cells. This enrichment of the cytotoxic payload has a substantial impact on the antimyeloma activity of melflufen.
Click to Show/Hide
|
||||
| Description |
In phase 1, the established maximum tolerated dose was 42 mg of melflufen in combination with dexamethasone.
|
||||
| In Vivo Model | Aged 18 years or older, had relapsed and refractory multiple myeloma, had received two or more previous lines of therapy (including lenalidomide and bortezomib). | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT01897714 | Clinical Status | Phase 1/2 | ||
| Clinical Description | The study will explore escalating doses of melflufen in combination with dexamethasone in small groups of patients to find the maximum tolerated dose of melflufen. That dose will then be used to determine the efficacy and safety profile of melflufen in combination with dexamethasone in a larger group of patients. | ||||
| Experiment 241 Reporting the Activity Data of This PDC | [7] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Maximum tolerated dose |
40 mg
|
|||
| Administration Time | Iv infusion of 55 mg melflufen on day 1 of each 21-day treatment cycle, in combination with 40 mg dexamet hasone (oral or iv) on days 1, 8 and 15 of each 21-day treatment cycle | ||||
| Administration Dosage | Melflufen 55 mg + Dexamethasone | ||||
| MOA of PDC |
The antineoplastic activity of melflufen is dependent upon the expression of aminopeptidases, like APN (also known as CD18), which cleave melflufen into melphalan and p-Fluorophenylalanine. Following aminopeptidase-dependent cleavage, the hydrophilic alkylating metabolite melphalan accumulates in myeloma cells. This enrichment of the cytotoxic payload has a substantial impact on the antimyeloma activity of melflufen.
Click to Show/Hide
|
||||
| Description |
In phase 1, the established maximum tolerated dose was 43 mg of melflufen in combination with dexamethasone.
|
||||
| In Vivo Model | Aged 18 years or older, had relapsed and refractory multiple myeloma, had received two or more previous lines of therapy (including lenalidomide and bortezomib). | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT01897714 | Clinical Status | Phase 1/2 | ||
| Clinical Description | The study will explore escalating doses of melflufen in combination with dexamethasone in small groups of patients to find the maximum tolerated dose of melflufen. That dose will then be used to determine the efficacy and safety profile of melflufen in combination with dexamethasone in a larger group of patients. | ||||
| Experiment 242 Reporting the Activity Data of This PDC | [4] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Median duration of response |
4.4 months
|
|||
| Patients Enrolled |
Patients with triple-class refractory disease group multiple myeloma.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melflufen is a first-in-class peptide-drug conjugate, targeting aminopeptidase which has an increased expression in fast-growing and aggressive malignancies. The lipophilicity of melflufen allows for passive diffusion, selectively targeting myeloma cells. Once inside the cell, melflufen is hydrolyzed to active alkylating metabolites melphalan and desethyl-melflufen. Melflufen and the active metabolites trigger irreversible DNA damage, inhibit proliferation, induces apoptosis, and express antiangiogenic effects. In addition, melflufen demonstrated activity in myeloma cells with documented impaired or absent Tp53 expression and documented resistance to bortezomib, dexamethasone, and melphalan.
Click to Show/Hide
|
||||
| Description |
The primary outcome of the study was ORR, defined based on the International Myeloma Working Group (IMWG) uniform response criteria. Investigators included a preplanned subgroup analysis in patients with triple-class refractory disease defined as refractory to at least 1 immunomodulator, 1 proteosome inhibitor, and 1 anti-CD38 antibody. From December 28, 2016, to October 14, 2019, investigators enrolled 157 patients across 17 sites that received at least 1 dose of melflufen. Patient baseline demographics included median age of 65 years old, an average of 5 previous lines of therapy, and 98% of patients were refractory to their previous line of therapy. A total of 131 patients (83%) discontinued treatment due to either disease progression or adverse effects. The median ORR was 29% (22%-37%) for the all treatment group and 26% (18%-35%) in the triple-class refractory disease group. The median duration of at least partial response or better was 5.5 months (3.9-7.6 months) in the all treatment group and 4.4 months (3.4-7.6 months) in the triple-class refractory disease group. Median overall survival (OS) was 11.6 months (9.3-15.4 months) in the all treatment group and 16.5 months (11.5-18.5 months) in the triple-class refractory group.
Click to Show/Hide
|
||||
| Experiment 243 Reporting the Activity Data of This PDC | [4] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Median duration of response |
5.5 months
|
|||
| Patients Enrolled |
157 patients with multiple myeloma.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melflufen is a first-in-class peptide-drug conjugate, targeting aminopeptidase which has an increased expression in fast-growing and aggressive malignancies. The lipophilicity of melflufen allows for passive diffusion, selectively targeting myeloma cells. Once inside the cell, melflufen is hydrolyzed to active alkylating metabolites melphalan and desethyl-melflufen. Melflufen and the active metabolites trigger irreversible DNA damage, inhibit proliferation, induces apoptosis, and express antiangiogenic effects. In addition, melflufen demonstrated activity in myeloma cells with documented impaired or absent Tp53 expression and documented resistance to bortezomib, dexamethasone, and melphalan.
Click to Show/Hide
|
||||
| Description |
The primary outcome of the study was ORR, defined based on the International Myeloma Working Group (IMWG) uniform response criteria. Investigators included a preplanned subgroup analysis in patients with triple-class refractory disease defined as refractory to at least 1 immunomodulator, 1 proteosome inhibitor, and 1 anti-CD38 antibody. From December 28, 2016, to October 14, 2019, investigators enrolled 157 patients across 17 sites that received at least 1 dose of melflufen. Patient baseline demographics included median age of 65 years old, an average of 5 previous lines of therapy, and 98% of patients were refractory to their previous line of therapy. A total of 131 patients (83%) discontinued treatment due to either disease progression or adverse effects. The median ORR was 29% (22%-37%) for the all treatment group and 26% (18%-35%) in the triple-class refractory disease group. The median duration of at least partial response or better was 5.5 months (3.9-7.6 months) in the all treatment group and 4.4 months (3.4-7.6 months) in the triple-class refractory disease group. Median overall survival (OS) was 11.6 months (9.3-15.4 months) in the all treatment group and 16.5 months (11.5-18.5 months) in the triple-class refractory group.
Click to Show/Hide
|
||||
| Experiment 244 Reporting the Activity Data of This PDC | [1] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Median duration of response |
4.4 months
|
|||
| Patients Enrolled |
Patients evaluable for response.
|
||||
| MOA of PDC |
Melflufen is highly lipophilic, which promotes its rapid uptake by cells. Once within the cell, melflufen releases its hydrophilic alkylator payloads via the hydrolytic activity of intracellular peptidases (e.g., aminopeptidases). Aminopeptidases are Zn2+-dependent metalloproteinases that remove amino acids at the N-terminal position from oligopeptides and have been associated with multiple tumorigenic processes such as proliferation, apoptosis, differentiation, angiogenesis, and motility. The dependence of melflufen on aminopeptidases was initially demonstrated by the reduced cytotoxic activity of melflufen-but not the alkylator melphalan-when cells were pretreated with bestatin, an antibiotic that is a potent aminopeptidase inhibitor. In addition, structure analogs designed to resist peptide hydrolysis (N-methyl derivative and derivative with D-amino acid) were shown to be almost 100-fold less potent than melflufen. Subsequent in vitro studies demonstrated that hydrolytic cleavage of melflufen by aminopeptidases releases alkylator payloads, including melphalan. In vitro, the activity of melflufen is multi-pronged, including induction of DNA damage, induction of apoptosis, inhibition of VEGF-dependent cell migration, and inhibition of tumor-associated angiogenesis, which have been further reviewed elsewhere. Downregulation of aminopeptidases resulted in reduced melflufen-mediated cytotoxic activity and apoptotic signaling in cultured cells.
Click to Show/Hide
|
||||
| Description |
Among 125 patients evaluable for response, the ORR (≥PR) was 29%, with 1 patient achieving a stringent complete response (CR) and 10 patients achieving a VGPR. The median duration of response was 4.4 months. The ORR was 21% among 47 patients with high-risk cytogenetics, 24% among 93 patients with triple-class refractory disease, and 24% among 42 patients with extramedullary disease.
Click to Show/Hide
|
||||
| Experiment 245 Reporting the Activity Data of This PDC | [9] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Median duration of treatment |
15.1 weeks
|
|||
| Patients Enrolled |
101 relapsed/refractory multiple myeloma patients with TTP <36 month Post-ASCTb.
|
||||
| MOA of PDC |
In summary, the interpretation of the results from the OCEAN study were impacted by the heterogeneity of the population, with age and previous success of ASCT therapy identified as prognostic factors with study therapies. The safety profile of melflufen and dexamethasone is primarily characterized by hematologic AEs that are clinically manageable. Observed infection rates, which included COVID-19, were generally low. Taken together, these data support the use of melflufen and dexamethasone in patients who have not received a previous ASCT or who underwent a successful ASCT (ie, TTP >36 months post-ASCT). In addition, the favorable efficacy profile and convenience of monthly outpatient infusions, especially for patients without access to other therapeutics such as CAR T-cell therapy or bispecific antibodies, bode well for this combination translating successfully into real-world practice.
Click to Show/Hide
|
||||
| Description |
Given the prognostic importance of TTP <36 months post-ASCT in OCEAN, we evaluated this prognostic factor in a post hoc analysis from the HORIZON study. Among 110 patients with triple-class refractory disease who had received ≥3 prior lines of therapy, 77 (70%) had received a previous ASCT and 58 (53%) had TTP <36 months post-ASCT (Suppl. Table S3). In patients with a TTP >36 months post-ASCT or no ASCT versus patients with a TTP <36 months post-ASCT, ORR was higher (29% vs 22%; Suppl. Table S4) and median DOR (7.6 months vs 3.9 months) and median PFS (4.2 months vs 3.4 months) were longer. Since pomalidomide and lenalidomide both belong to the immunomodulatory drugs, we analyzed if the duration of previous treatment with lenalidomide could have impacted the results. The median duration of lenalidomide was 14.4 months in patients with ASCT and TTP < 36 months, 38.3 months in patients with ASCT and TTP > 36 months, and 14.6 months in patients with no previous ASCT. However, the median PFS for patients treated with pomalidomide did not differ substantially between these groups of patients. The safety profile of melflufen and dexamethasone was generally consistent between patients with a TTP >36 months post-ASCT or no ASCT and patients with a TTP <36 months post-ASCT. In OCEAN among the melflufen group, the frequency of grade 3/4 TEAEs (88% and 92%), serious TEAEs (44% and 38%), and fatal adverse events (AEs; 11% and 13%) was similar in patients with a TTP >36 months post-ASCT or no ASCT and patients with TTP <36 months. However, patients with a TTP >36 months post-ASCT or no ASCT had lower rates of TEAEs leading to treatment discontinuation (23% and 31%), the longer median duration of study treatment (35.1 weeks vs 15.1 weeks), and longer median time to experiencing grade 3/4 thrombocytopenia (11.2 weeks vs 4.1 weeks) and grade 3/4 neutropenia (4.8 weeks vs 2.1 weeks) than patients with a TTP <36 months post-ASCT. In HORIZON, patients with a TTP >36 months post-ASCT or no ASCT had lower rates of grade 3/4 TEAEs (88% and 98%), but higher rates of serious TEAEs (64% and 53%) and similar rates of TEAEs leading to treatment discontinuation (29% and 33%) than patients with a TTP <36 months post-ASCT.
Click to Show/Hide
|
||||
| Experiment 246 Reporting the Activity Data of This PDC | [9] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Median duration of treatment |
35.1 weeks
|
|||
| Patients Enrolled |
145 patients who has relapsed/refractory multiple myeloma with no previous ASCT or TTP >36 month Post-ASCTa.
|
||||
| MOA of PDC |
In summary, the interpretation of the results from the OCEAN study were impacted by the heterogeneity of the population, with age and previous success of ASCT therapy identified as prognostic factors with study therapies. The safety profile of melflufen and dexamethasone is primarily characterized by hematologic AEs that are clinically manageable. Observed infection rates, which included COVID-19, were generally low. Taken together, these data support the use of melflufen and dexamethasone in patients who have not received a previous ASCT or who underwent a successful ASCT (ie, TTP >36 months post-ASCT). In addition, the favorable efficacy profile and convenience of monthly outpatient infusions, especially for patients without access to other therapeutics such as CAR T-cell therapy or bispecific antibodies, bode well for this combination translating successfully into real-world practice.
Click to Show/Hide
|
||||
| Description |
Given the prognostic importance of TTP <36 months post-ASCT in OCEAN, we evaluated this prognostic factor in a post hoc analysis from the HORIZON study. Among 110 patients with triple-class refractory disease who had received ≥3 prior lines of therapy, 77 (70%) had received a previous ASCT and 58 (53%) had TTP <36 months post-ASCT (Suppl. Table S3). In patients with a TTP >36 months post-ASCT or no ASCT versus patients with a TTP <36 months post-ASCT, ORR was higher (29% vs 22%; Suppl. Table S4) and median DOR (7.6 months vs 3.9 months) and median PFS (4.2 months vs 3.4 months) were longer. Since pomalidomide and lenalidomide both belong to the immunomodulatory drugs, we analyzed if the duration of previous treatment with lenalidomide could have impacted the results. The median duration of lenalidomide was 14.4 months in patients with ASCT and TTP < 36 months, 38.3 months in patients with ASCT and TTP > 36 months, and 14.6 months in patients with no previous ASCT. However, the median PFS for patients treated with pomalidomide did not differ substantially between these groups of patients. The safety profile of melflufen and dexamethasone was generally consistent between patients with a TTP >36 months post-ASCT or no ASCT and patients with a TTP <36 months post-ASCT. In OCEAN among the melflufen group, the frequency of grade 3/4 TEAEs (88% and 92%), serious TEAEs (44% and 38%), and fatal adverse events (AEs; 11% and 13%) was similar in patients with a TTP >36 months post-ASCT or no ASCT and patients with TTP <36 months. However, patients with a TTP >36 months post-ASCT or no ASCT had lower rates of TEAEs leading to treatment discontinuation (23% and 31%), the longer median duration of study treatment (35.1 weeks vs 15.1 weeks), and longer median time to experiencing grade 3/4 thrombocytopenia (11.2 weeks vs 4.1 weeks) and grade 3/4 neutropenia (4.8 weeks vs 2.1 weeks) than patients with a TTP <36 months post-ASCT. In HORIZON, patients with a TTP >36 months post-ASCT or no ASCT had lower rates of grade 3/4 TEAEs (88% and 98%), but higher rates of serious TEAEs (64% and 53%) and similar rates of TEAEs leading to treatment discontinuation (29% and 33%) than patients with a TTP <36 months post-ASCT.
Click to Show/Hide
|
||||
| Experiment 247 Reporting the Activity Data of This PDC | [4] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Median overall survival (mOS) |
19.7 months
|
|||
| Patients Enrolled |
Patients with multiple myeloma.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melflufen is a first-in-class peptide-drug conjugate, targeting aminopeptidase which has an increased expression in fast-growing and aggressive malignancies. The lipophilicity of melflufen allows for passive diffusion, selectively targeting myeloma cells. Once inside the cell, melflufen is hydrolyzed to active alkylating metabolites melphalan and desethyl-melflufen. Melflufen and the active metabolites trigger irreversible DNA damage, inhibit proliferation, induces apoptosis, and express antiangiogenic effects. In addition, melflufen demonstrated activity in myeloma cells with documented impaired or absent Tp53 expression and documented resistance to bortezomib, dexamethasone, and melphalan.
Click to Show/Hide
|
||||
| Description |
The FDA announced on July 28, 2021, all ongoing melflufen clinical trials are to suspend enrollment until a complete safety analysis can be performed. This recommendation is based on preliminary OCEAN trial OS data. The hazard ratio for OS was 1.104 (0.846-1.441) when comparing the 2 treatment arms, favoring pomalidomide plus dexamethasone. At a median follow-up of 19.1 months, the median OS for the melflufen arm was 19.7 months (15.1-25.6) compared with 25 months (18.1-31.9) in the pomalidomide arm. At this time, no further recommendations have been made by the FDA concerning the continuation of melflufen clinical trials.
Click to Show/Hide
|
||||
| Experiment 248 Reporting the Activity Data of This PDC | [4] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Median overall survival (mOS) |
11.6 months
|
|||
| Patients Enrolled |
157 patients with multiple myeloma.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melflufen is a first-in-class peptide-drug conjugate, targeting aminopeptidase which has an increased expression in fast-growing and aggressive malignancies. The lipophilicity of melflufen allows for passive diffusion, selectively targeting myeloma cells. Once inside the cell, melflufen is hydrolyzed to active alkylating metabolites melphalan and desethyl-melflufen. Melflufen and the active metabolites trigger irreversible DNA damage, inhibit proliferation, induces apoptosis, and express antiangiogenic effects. In addition, melflufen demonstrated activity in myeloma cells with documented impaired or absent Tp53 expression and documented resistance to bortezomib, dexamethasone, and melphalan.
Click to Show/Hide
|
||||
| Description |
The primary outcome of the study was ORR, defined based on the International Myeloma Working Group (IMWG) uniform response criteria. Investigators included a preplanned subgroup analysis in patients with triple-class refractory disease defined as refractory to at least 1 immunomodulator, 1 proteosome inhibitor, and 1 anti-CD38 antibody. From December 28, 2016, to October 14, 2019, investigators enrolled 157 patients across 17 sites that received at least 1 dose of melflufen. Patient baseline demographics included median age of 65 years old, an average of 5 previous lines of therapy, and 98% of patients were refractory to their previous line of therapy. A total of 131 patients (83%) discontinued treatment due to either disease progression or adverse effects. The median ORR was 29% (22%-37%) for the all treatment group and 26% (18%-35%) in the triple-class refractory disease group. The median duration of at least partial response or better was 5.5 months (3.9-7.6 months) in the all treatment group and 4.4 months (3.4-7.6 months) in the triple-class refractory disease group. Median overall survival (OS) was 11.6 months (9.3-15.4 months) in the all treatment group and 16.5 months (11.5-18.5 months) in the triple-class refractory group.
Click to Show/Hide
|
||||
| Experiment 249 Reporting the Activity Data of This PDC | [4] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Median overall survival (mOS) |
16.5 months
|
|||
| Patients Enrolled |
Patients with triple-class refractory disease group multiple myeloma.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melflufen is a first-in-class peptide-drug conjugate, targeting aminopeptidase which has an increased expression in fast-growing and aggressive malignancies. The lipophilicity of melflufen allows for passive diffusion, selectively targeting myeloma cells. Once inside the cell, melflufen is hydrolyzed to active alkylating metabolites melphalan and desethyl-melflufen. Melflufen and the active metabolites trigger irreversible DNA damage, inhibit proliferation, induces apoptosis, and express antiangiogenic effects. In addition, melflufen demonstrated activity in myeloma cells with documented impaired or absent Tp53 expression and documented resistance to bortezomib, dexamethasone, and melphalan.
Click to Show/Hide
|
||||
| Description |
The primary outcome of the study was ORR, defined based on the International Myeloma Working Group (IMWG) uniform response criteria. Investigators included a preplanned subgroup analysis in patients with triple-class refractory disease defined as refractory to at least 1 immunomodulator, 1 proteosome inhibitor, and 1 anti-CD38 antibody. From December 28, 2016, to October 14, 2019, investigators enrolled 157 patients across 17 sites that received at least 1 dose of melflufen. Patient baseline demographics included median age of 65 years old, an average of 5 previous lines of therapy, and 98% of patients were refractory to their previous line of therapy. A total of 131 patients (83%) discontinued treatment due to either disease progression or adverse effects. The median ORR was 29% (22%-37%) for the all treatment group and 26% (18%-35%) in the triple-class refractory disease group. The median duration of at least partial response or better was 5.5 months (3.9-7.6 months) in the all treatment group and 4.4 months (3.4-7.6 months) in the triple-class refractory disease group. Median overall survival (OS) was 11.6 months (9.3-15.4 months) in the all treatment group and 16.5 months (11.5-18.5 months) in the triple-class refractory group.
Click to Show/Hide
|
||||
| Experiment 250 Reporting the Activity Data of This PDC | [1] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Median overall survival (mOS) |
8.1 months
|
|||
| Patients Enrolled |
Patients with extramedullary disease.
|
||||
| MOA of PDC |
Melflufen is highly lipophilic, which promotes its rapid uptake by cells. Once within the cell, melflufen releases its hydrophilic alkylator payloads via the hydrolytic activity of intracellular peptidases (e.g., aminopeptidases). Aminopeptidases are Zn2+-dependent metalloproteinases that remove amino acids at the N-terminal position from oligopeptides and have been associated with multiple tumorigenic processes such as proliferation, apoptosis, differentiation, angiogenesis, and motility. The dependence of melflufen on aminopeptidases was initially demonstrated by the reduced cytotoxic activity of melflufen-but not the alkylator melphalan-when cells were pretreated with bestatin, an antibiotic that is a potent aminopeptidase inhibitor. In addition, structure analogs designed to resist peptide hydrolysis (N-methyl derivative and derivative with D-amino acid) were shown to be almost 100-fold less potent than melflufen. Subsequent in vitro studies demonstrated that hydrolytic cleavage of melflufen by aminopeptidases releases alkylator payloads, including melphalan. In vitro, the activity of melflufen is multi-pronged, including induction of DNA damage, induction of apoptosis, inhibition of VEGF-dependent cell migration, and inhibition of tumor-associated angiogenesis, which have been further reviewed elsewhere. Downregulation of aminopeptidases resulted in reduced melflufen-mediated cytotoxic activity and apoptotic signaling in cultured cells.
Click to Show/Hide
|
||||
| Description |
The median PFS and OS were 4.2 and 11.6 months for all patients, 4.0 and 11.3 months for patients with triple-class refractory disease, and 3.0 and 8.1 months for patients with extramedullary disease, respectively.
|
||||
| Experiment 251 Reporting the Activity Data of This PDC | [1] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Median overall survival (mOS) |
11.3 months
|
|||
| Patients Enrolled |
Patients with triple-class refractory disease.
|
||||
| MOA of PDC |
Melflufen is highly lipophilic, which promotes its rapid uptake by cells. Once within the cell, melflufen releases its hydrophilic alkylator payloads via the hydrolytic activity of intracellular peptidases (e.g., aminopeptidases). Aminopeptidases are Zn2+-dependent metalloproteinases that remove amino acids at the N-terminal position from oligopeptides and have been associated with multiple tumorigenic processes such as proliferation, apoptosis, differentiation, angiogenesis, and motility. The dependence of melflufen on aminopeptidases was initially demonstrated by the reduced cytotoxic activity of melflufen-but not the alkylator melphalan-when cells were pretreated with bestatin, an antibiotic that is a potent aminopeptidase inhibitor. In addition, structure analogs designed to resist peptide hydrolysis (N-methyl derivative and derivative with D-amino acid) were shown to be almost 100-fold less potent than melflufen. Subsequent in vitro studies demonstrated that hydrolytic cleavage of melflufen by aminopeptidases releases alkylator payloads, including melphalan. In vitro, the activity of melflufen is multi-pronged, including induction of DNA damage, induction of apoptosis, inhibition of VEGF-dependent cell migration, and inhibition of tumor-associated angiogenesis, which have been further reviewed elsewhere. Downregulation of aminopeptidases resulted in reduced melflufen-mediated cytotoxic activity and apoptotic signaling in cultured cells.
Click to Show/Hide
|
||||
| Description |
The median PFS and OS were 4.2 and 11.6 months for all patients, 4.0 and 11.3 months for patients with triple-class refractory disease, and 3.0 and 8.1 months for patients with extramedullary disease, respectively.
|
||||
| Experiment 252 Reporting the Activity Data of This PDC | [1] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Median overall survival (mOS) |
11.6 months
|
|||
| Patients Enrolled |
All patients.
|
||||
| MOA of PDC |
Melflufen is highly lipophilic, which promotes its rapid uptake by cells. Once within the cell, melflufen releases its hydrophilic alkylator payloads via the hydrolytic activity of intracellular peptidases (e.g., aminopeptidases). Aminopeptidases are Zn2+-dependent metalloproteinases that remove amino acids at the N-terminal position from oligopeptides and have been associated with multiple tumorigenic processes such as proliferation, apoptosis, differentiation, angiogenesis, and motility. The dependence of melflufen on aminopeptidases was initially demonstrated by the reduced cytotoxic activity of melflufen-but not the alkylator melphalan-when cells were pretreated with bestatin, an antibiotic that is a potent aminopeptidase inhibitor. In addition, structure analogs designed to resist peptide hydrolysis (N-methyl derivative and derivative with D-amino acid) were shown to be almost 100-fold less potent than melflufen. Subsequent in vitro studies demonstrated that hydrolytic cleavage of melflufen by aminopeptidases releases alkylator payloads, including melphalan. In vitro, the activity of melflufen is multi-pronged, including induction of DNA damage, induction of apoptosis, inhibition of VEGF-dependent cell migration, and inhibition of tumor-associated angiogenesis, which have been further reviewed elsewhere. Downregulation of aminopeptidases resulted in reduced melflufen-mediated cytotoxic activity and apoptotic signaling in cultured cells.
Click to Show/Hide
|
||||
| Description |
The median PFS and OS were 4.2 and 11.6 months for all patients, 4.0 and 11.3 months for patients with triple-class refractory disease, and 3.0 and 8.1 months for patients with extramedullary disease, respectively.
|
||||
| Experiment 253 Reporting the Activity Data of This PDC | [1] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Median overall survival (mOS) |
15.5 months
|
|||
| Patients Enrolled |
Patients with multi-refractory multiple myeloma.
|
||||
| MOA of PDC |
Melflufen is highly lipophilic, which promotes its rapid uptake by cells. Once within the cell, melflufen releases its hydrophilic alkylator payloads via the hydrolytic activity of intracellular peptidases (e.g., aminopeptidases). Aminopeptidases are Zn2+-dependent metalloproteinases that remove amino acids at the N-terminal position from oligopeptides and have been associated with multiple tumorigenic processes such as proliferation, apoptosis, differentiation, angiogenesis, and motility. The dependence of melflufen on aminopeptidases was initially demonstrated by the reduced cytotoxic activity of melflufen-but not the alkylator melphalan-when cells were pretreated with bestatin, an antibiotic that is a potent aminopeptidase inhibitor. In addition, structure analogs designed to resist peptide hydrolysis (N-methyl derivative and derivative with D-amino acid) were shown to be almost 100-fold less potent than melflufen. Subsequent in vitro studies demonstrated that hydrolytic cleavage of melflufen by aminopeptidases releases alkylator payloads, including melphalan. In vitro, the activity of melflufen is multi-pronged, including induction of DNA damage, induction of apoptosis, inhibition of VEGF-dependent cell migration, and inhibition of tumor-associated angiogenesis, which have been further reviewed elsewhere. Downregulation of aminopeptidases resulted in reduced melflufen-mediated cytotoxic activity and apoptotic signaling in cultured cells.
Click to Show/Hide
|
||||
| Description |
Among the 13 patients who received single-agent melflufen, the median number of prior therapies was 5 (range, 4-8), the ORR was 8% (1 PR), median PFS was 4.4 months, and median OS was 15.5 months.
|
||||
| Experiment 254 Reporting the Activity Data of This PDC | [9] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Median overall survival (mOS) |
16.2 months
|
|||
| Patients Enrolled |
96 relapsed/refractory multiple myeloma patients aged <65 years.
|
||||
| MOA of PDC |
In summary, the interpretation of the results from the OCEAN study were impacted by the heterogeneity of the population, with age and previous success of ASCT therapy identified as prognostic factors with study therapies. The safety profile of melflufen and dexamethasone is primarily characterized by hematologic AEs that are clinically manageable. Observed infection rates, which included COVID-19, were generally low. Taken together, these data support the use of melflufen and dexamethasone in patients who have not received a previous ASCT or who underwent a successful ASCT (ie, TTP >36 months post-ASCT). In addition, the favorable efficacy profile and convenience of monthly outpatient infusions, especially for patients without access to other therapeutics such as CAR T-cell therapy or bispecific antibodies, bode well for this combination translating successfully into real-world practice.
Click to Show/Hide
|
||||
| Description |
In this updated survival analysis, median OS (95% CI) was 20.2 months (15.8-24.3) with melflufen and 24.0 months (19.1-28.7) with pomalidomide (HR, 1.14 [95% CI, 0.91-1.43]; P =.24), with a median follow-up time of 31.8 months and 29.8 months, respectively. Because of imbalance in the number of patients who were randomized but not treated, survival was also evaluated in the safety population: median OS (95% CI) was 21.3 months (16.6-24.8) with melflufen and 24.0 months (19.8-28.7) with pomalidomide (HR, 1.12 [95% CI, 0.89-1.42]; P =.33), with the curves overlapping until 10 months after randomization. Sensitivity analyses revealed that the uneven distribution of randomized but not treated patients impacted OS, but not PFS. Although a similar number of patients received subsequent therapy after OCEAN (melflufen group, 169/246 [69%] patients; pomalidomide group, 164/249 [66%] patients), the type of subsequent therapy and timing of subsequent therapy initiation differed between treatment groups.
Click to Show/Hide
|
||||
| Experiment 255 Reporting the Activity Data of This PDC | [9] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Median overall survival (mOS) |
20.5 months
|
|||
| Patients Enrolled |
113 relapsed/refractory multiple myeloma patients aged 65-74 years.
|
||||
| MOA of PDC |
In summary, the interpretation of the results from the OCEAN study were impacted by the heterogeneity of the population, with age and previous success of ASCT therapy identified as prognostic factors with study therapies. The safety profile of melflufen and dexamethasone is primarily characterized by hematologic AEs that are clinically manageable. Observed infection rates, which included COVID-19, were generally low. Taken together, these data support the use of melflufen and dexamethasone in patients who have not received a previous ASCT or who underwent a successful ASCT (ie, TTP >36 months post-ASCT). In addition, the favorable efficacy profile and convenience of monthly outpatient infusions, especially for patients without access to other therapeutics such as CAR T-cell therapy or bispecific antibodies, bode well for this combination translating successfully into real-world practice.
Click to Show/Hide
|
||||
| Description |
In this updated survival analysis, median OS (95% CI) was 20.2 months (15.8-24.3) with melflufen and 24.0 months (19.1-28.7) with pomalidomide (HR, 1.14 [95% CI, 0.91-1.43]; P =.24), with a median follow-up time of 31.8 months and 29.8 months, respectively. Because of imbalance in the number of patients who were randomized but not treated, survival was also evaluated in the safety population: median OS (95% CI) was 21.3 months (16.6-24.8) with melflufen and 24.0 months (19.8-28.7) with pomalidomide (HR, 1.12 [95% CI, 0.89-1.42]; P =.33), with the curves overlapping until 10 months after randomization. Sensitivity analyses revealed that the uneven distribution of randomized but not treated patients impacted OS, but not PFS. Although a similar number of patients received subsequent therapy after OCEAN (melflufen group, 169/246 [69%] patients; pomalidomide group, 164/249 [66%] patients), the type of subsequent therapy and timing of subsequent therapy initiation differed between treatment groups.
Click to Show/Hide
|
||||
| Experiment 256 Reporting the Activity Data of This PDC | [5] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Median overall survival (mOS) |
23.4 months
|
|||
| Patients Enrolled |
153 patients refractory to prior alkylators (melflufen, n=78; pomalidomide, n=75).
|
||||
| MOA of PDC |
Melphalan flufenamide (melflufen), a first-in-class alkylating peptide-drug conjugate, plus dexamethasone demonstrated superior progression-free survival (PFS), but not overall survival (OS), versus pomalidomide plus dexamethasone in relapsed/refractory multiple myeloma in the OCEAN study. Time to progression (TTP) <36 months after a prior autologous stem cell transplantation (ASCT) was a negative prognostic factor for OS with melflufen. This post hoc exploratory analysis evaluated patients refractory to prior alkylators (e.g., cyclophosphamide and melphalan) in OCEAN. In 153 patients refractory to prior alkylators (melflufen, n = 78; pomalidomide, n = 75), the melflufen and pomalidomide arms had similar median PFS (5.6 months [95% CI, 4.2-8.3] vs. 4.7 months [95% CI, 3.1-7.3]; hazard ratio [HR], 0.92 [95% CI, 0.63-1.33]) and OS (23.4 months [95% CI, 14.4-31.7] vs. 20.0 months [95% CI, 12.0-28.7]; HR, 0.92 [95% CI, 0.62-1.38]). Among alkylator-refractory patients with a TTP 36 months after a prior ASCT or no prior ASCT (melflufen, n = 54; pomalidomide, n = 53), the observed median PFS and OS were longer in the melflufen arm than the pomalidomide arm. The safety profile of melflufen was consistent with previous reports. These results suggest that melflufen is safe and effective in patients with alkylator-refractory disease, suggesting differentiated activity from other alkylators.
Click to Show/Hide
|
||||
| Description |
In the overall alkylator-refractory group, the melflufen and pomalidomide arms saw a similar median PFS (5.6 months [95% CI, 4.2-8.3] vs. 4.7 months [95% CI, 3.1-7.3]; HR, 0.92 [95% CI, 0.63-1.33]) and median OS (23.4 months [14.4-31.7] vs. 20.0 months [12.0-28.7]; HR, 0.92 [95% CI, 0.62-1.38]). Corresponding results were observed when evaluating PFS and OS in subgroups by type of prior alkylating agent received. In the melflufen and pomalidomide arms, the ORR was 24.4% and 28.0% in patients refractory to alkylators overall, 22.2% and 25.0% in patients refractory to cyclophosphamide, and 33.3% and 26.1% in patients refractory to melphalan, respectively.
Click to Show/Hide
|
||||
| Experiment 257 Reporting the Activity Data of This PDC | [9] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Median overall survival (mOS) |
26.5 months
|
|||
| Patients Enrolled |
37 relapsed/refractory multiple myeloma patients aged 75 years.
|
||||
| MOA of PDC |
In summary, the interpretation of the results from the OCEAN study were impacted by the heterogeneity of the population, with age and previous success of ASCT therapy identified as prognostic factors with study therapies. The safety profile of melflufen and dexamethasone is primarily characterized by hematologic AEs that are clinically manageable. Observed infection rates, which included COVID-19, were generally low. Taken together, these data support the use of melflufen and dexamethasone in patients who have not received a previous ASCT or who underwent a successful ASCT (ie, TTP >36 months post-ASCT). In addition, the favorable efficacy profile and convenience of monthly outpatient infusions, especially for patients without access to other therapeutics such as CAR T-cell therapy or bispecific antibodies, bode well for this combination translating successfully into real-world practice.
Click to Show/Hide
|
||||
| Description |
In this updated survival analysis, median OS (95% CI) was 20.2 months (15.8-24.3) with melflufen and 24.0 months (19.1-28.7) with pomalidomide (HR, 1.14 [95% CI, 0.91-1.43]; P =.24), with a median follow-up time of 31.8 months and 29.8 months, respectively. Because of imbalance in the number of patients who were randomized but not treated, survival was also evaluated in the safety population: median OS (95% CI) was 21.3 months (16.6-24.8) with melflufen and 24.0 months (19.8-28.7) with pomalidomide (HR, 1.12 [95% CI, 0.89-1.42]; P =.33), with the curves overlapping until 10 months after randomization. Sensitivity analyses revealed that the uneven distribution of randomized but not treated patients impacted OS, but not PFS. Although a similar number of patients received subsequent therapy after OCEAN (melflufen group, 169/246 [69%] patients; pomalidomide group, 164/249 [66%] patients), the type of subsequent therapy and timing of subsequent therapy initiation differed between treatment groups.
Click to Show/Hide
|
||||
| Experiment 258 Reporting the Activity Data of This PDC | [10] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Median progression-free survival (mPFS) |
6.8 months
|
|||
| Administration Time | 15.5 months | ||||
| MOA of PDC |
Melflufen, a highly lipophilic PDC, takes a novel approach by taking advantage of increased aminopeptidase activity to selectively increase the release and concentration of cytotoxic alkylating agents inside of tumor cells. Being highly lipophilic, melflufen does not require active transport, a process that may be defective in cancer cells and contribute to chemoresistance, but instead rapidly enters cells via passive diffusion. The lipophilic nature of melflufen also likely results in its favorable distribution to bone marrow, a fatty tissue, and the physiological component most relevant to MM. Once inside the tumor cells, melflufen is rapidly hydrolyzed by aminopeptidases, enzymes that are found in normal cells but are overexpressed in MM and upon which cancer cells are particularly dependent. This hydrolysis releases potent alkylating agents - most notably melphalan and des-ethyl melflufen - within the cells. Aminopeptidase-driven release of these hydrophilic molecules, which cannot readily diffuse out, thereby results in intracellular trapping. Leveraging high tumor cell aminopeptidase concentrations to rapidly drive intracellular alkylating agent release may provide a safety advantage over alkylators, such as melphalan, which lack such a mechanism for tumor cell targeting, particularly in tumors with an aggressive phenotype.
Click to Show/Hide
|
||||
| Description |
OCEAN randomized patients to 28-day cycles of melflufen 40 mg intravenous on day 1 plus dexamethasone 40 mg oral (days 1, 8, 15, and 22) or pomalidomide 4 mg oral (days 1-21) plus dexamethasone 40 mg oral (days 1, 8, 15, and 22). The primary objective was to compare the PFS of melflufen plus dexamethasone and pomalidomide plus dexamethasone by independent review. Secondary endpoints include comparing ORR, OS, and safety and tolerability. Notably, the OCEAN patient population and study design mirrored those of the MM-003 study to allow for the most robust comparison between melflufen and pomalidomide. Primary results of the OCEAN trial were recently published, with additional survival follow-up ongoing. In total, 495 patients were randomized (246 to the melflufen arm and 249 to the pomalidomide arm). The study met its primary endpoints, with melflufen plus dexamethasone demonstrating a superior PFS to pomalidomide plus dexamethasone (median PFS: 6.8 months vs 4.9 months; hazard ratio [HR], 0.79 [95% CI, 0.64-0.98]; P = 0.03), but OS favored pomalidomide plus dexamethasone (median OS: 19.8 months vs 25.0 months; HR, 1.10 [95% CI, 0.85-1.44]; not significant). However, additional exploratory and post-hoc analyses identified previous ASCT and age as significant prognostic factors, which is not surprising given that transplant eligibility and age are generally correlated. Patients who had not received a previous ASCT (melflufen, n = 121; pomalidomide, n = 129) had better PFS and OS with melflufen plus dexamethasone than with pomalidomide plus dexamethasone (median PFS: 9.3 months vs 4.6 months; HR, 0.59 [95% CI, 0.44-0.79]; P < 0.001; median OS: 21.6 months vs 16.5 months; HR, 0.78 [95% CI, 0.55-1.12]; not significant), while patients who had received previous ASCT (melflufen, n = 125; pomalidomide, n = 120) saw similar PFS between groups but worse OS with melflufen plus dexamethasone than with pomalidomide plus dexamethasone (median PFS: 4.4 months vs 5.2 months; HR, 1.06 [95% CI, 0.79-1.43]; not significant; median OS: 16.7 months vs 31.0 months; HR, 1.61 [95% CI, 1.09-2.40]; P = 0.02). In patients aged ≥75, PFS was more favorable with melflufen (HR, 0.43 [95% CI, 0.24-0.76]; P = 0.003) but in patients aged <65, OS data favored pomalidomide (HR, 1.71 [95% CI, 1.09-2.69]; P = 0.02). Safety was evaluated in patients who received at least one dose of study medication (melflufen, n = 228; pomalidomide, n = 246).
Click to Show/Hide
|
||||
| Related Clinical Trial | |||||
| NCT Number | NCT03151811 | Clinical Status | Phase 3 | ||
| Clinical Description | This was a randomized, controlled, open-label, Phase 3 multicenter study which enrolled patients with RRMM following 2-4 lines of prior therapy and who were refractory to lenalidomide in the last line of therapy as demonstrated by disease progression on or within 60 days of completion of the last dose of lenalidomide. Patients received either melflufen+dex or pomalidomide+dex. | ||||
| Experiment 259 Reporting the Activity Data of This PDC | [10] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Median progression-free survival (mPFS) |
4.2 months
|
|||
| Administration Time | 14 months | ||||
| MOA of PDC |
Melflufen, a highly lipophilic PDC, takes a novel approach by taking advantage of increased aminopeptidase activity to selectively increase the release and concentration of cytotoxic alkylating agents inside of tumor cells. Being highly lipophilic, melflufen does not require active transport, a process that may be defective in cancer cells and contribute to chemoresistance, but instead rapidly enters cells via passive diffusion. The lipophilic nature of melflufen also likely results in its favorable distribution to bone marrow, a fatty tissue, and the physiological component most relevant to MM. Once inside the tumor cells, melflufen is rapidly hydrolyzed by aminopeptidases, enzymes that are found in normal cells but are overexpressed in MM and upon which cancer cells are particularly dependent. This hydrolysis releases potent alkylating agents - most notably melphalan and des-ethyl melflufen - within the cells. Aminopeptidase-driven release of these hydrophilic molecules, which cannot readily diffuse out, thereby results in intracellular trapping. Leveraging high tumor cell aminopeptidase concentrations to rapidly drive intracellular alkylating agent release may provide a safety advantage over alkylators, such as melphalan, which lack such a mechanism for tumor cell targeting, particularly in tumors with an aggressive phenotype.
Click to Show/Hide
|
||||
| Description |
Extensive subgroup analyses have been carried out using O-12-M1 and HORIZON data. In HORIZON, patients with triple-refractory disease and those with disease refractory to anti-CD38 mAbs in the last line had efficacy outcomes similar to those in the overall patient population. Patients with MM refractory to anti-CD38 mAbs in the last line (n = 63) had better response (ORR 35% versus 31%), median PFS (4.6 versus 3.4 months) and OS (15.4 versus 9.3 months) than patients in the MAMMOTH trial treated with conventional chemotherapy (n = 275). Baseline characteristics were similar in these two trials, except that in HORIZON, patients were more heavily pretreated (median 5 versus 4 therapies). Among patients in HORIZON whose disease was alkylator-refractory in any prior line (n = 92), the ORR was 21% and median PFS was 3.8 months. None of the seven patients with melphalan-refractory disease, however, had an objective response by independent review. This contrasts with the 44% ORR observed in nine patients with melphalan-refractory disease in O-12-M1. All seven patients in HORIZON, however, were at least triple-class refractory, and none had achieved a CR in any prior line.
Click to Show/Hide
|
||||
| Related Clinical Trial | |||||
| NCT Number | NCT02963493 | Clinical Status | Phase 2 | ||
| Clinical Description | This study will evaluate melflufen in combination with dexamethasone in adult patients with relapsed or refractory multiple myeloma in whose disease is refractory to pomalidomide and/or an anti-CD38 monoclonal antibody. All patients in the study will be treated with melflufen on Day 1 and dexamethasone on Days 1, 8, 15 and 22 of each 28-day cycle. | ||||
| Experiment 260 Reporting the Activity Data of This PDC | [10] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Median progression-free survival (mPFS) |
5.7 months
|
|||
| Administration Time | 27.9 months | ||||
| MOA of PDC |
Melflufen, a highly lipophilic PDC, takes a novel approach by taking advantage of increased aminopeptidase activity to selectively increase the release and concentration of cytotoxic alkylating agents inside of tumor cells. Being highly lipophilic, melflufen does not require active transport, a process that may be defective in cancer cells and contribute to chemoresistance, but instead rapidly enters cells via passive diffusion. The lipophilic nature of melflufen also likely results in its favorable distribution to bone marrow, a fatty tissue, and the physiological component most relevant to MM. Once inside the tumor cells, melflufen is rapidly hydrolyzed by aminopeptidases, enzymes that are found in normal cells but are overexpressed in MM and upon which cancer cells are particularly dependent. This hydrolysis releases potent alkylating agents - most notably melphalan and des-ethyl melflufen - within the cells. Aminopeptidase-driven release of these hydrophilic molecules, which cannot readily diffuse out, thereby results in intracellular trapping. Leveraging high tumor cell aminopeptidase concentrations to rapidly drive intracellular alkylating agent release may provide a safety advantage over alkylators, such as melphalan, which lack such a mechanism for tumor cell targeting, particularly in tumors with an aggressive phenotype.
Click to Show/Hide
|
||||
| Description |
Forty-five patients received melflufen plus dexamethasone in the phase II portion of the study. The median age was 66 years, 67% were male, the median prior therapies were 4 (range, 3-5), 67% were double refractory (PI and IMiD), 58% had received previous ASCT, 20% had International Staging System (ISS) stage 3 disease, and 44% had high-risk cytogenetics. At a median follow-up time of 27.9 months, the ORR in this cohort was 31% (95% CI: 18-47), including 11% very good partial response (VGPR). No complete responses (CRs) occurred. Interestingly, among patients whose disease was refractory to melphalan in any prior line, the ORR was 44%. The CBR was 49% (95% CI: 34-64), the median duration of response (DOR) was 8.4 months (95% CI: 4.6-9.6), and median PFS was 5.7 months (95% CI: 3.7-9.2). A recently published longer term data analysis reported that at a median 46-month follow-up, the median overall survival (OS) was 20.7 months (95% CI: 11.8-41.3).
Click to Show/Hide
|
||||
| Related Clinical Trial | |||||
| NCT Number | NCT01897714 | Clinical Status | Phase 1/2 | ||
| Clinical Description | The study will explore escalating doses of melflufen in combination with dexamethasone in small groups of patients to find the maximum tolerated dose of melflufen. That dose will then be used to determine the efficacy and safety profile of melflufen in combination with dexamethasone in a larger group of patients. | ||||
| Experiment 261 Reporting the Activity Data of This PDC | [10] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Median progression-free survival (mPFS) |
11.5 months
|
|||
| Administration Time | 11.9 months | ||||
| MOA of PDC |
Melflufen, a highly lipophilic PDC, takes a novel approach by taking advantage of increased aminopeptidase activity to selectively increase the release and concentration of cytotoxic alkylating agents inside of tumor cells. Being highly lipophilic, melflufen does not require active transport, a process that may be defective in cancer cells and contribute to chemoresistance, but instead rapidly enters cells via passive diffusion. The lipophilic nature of melflufen also likely results in its favorable distribution to bone marrow, a fatty tissue, and the physiological component most relevant to MM. Once inside the tumor cells, melflufen is rapidly hydrolyzed by aminopeptidases, enzymes that are found in normal cells but are overexpressed in MM and upon which cancer cells are particularly dependent. This hydrolysis releases potent alkylating agents - most notably melphalan and des-ethyl melflufen - within the cells. Aminopeptidase-driven release of these hydrophilic molecules, which cannot readily diffuse out, thereby results in intracellular trapping. Leveraging high tumor cell aminopeptidase concentrations to rapidly drive intracellular alkylating agent release may provide a safety advantage over alkylators, such as melphalan, which lack such a mechanism for tumor cell targeting, particularly in tumors with an aggressive phenotype.
Click to Show/Hide
|
||||
| Description |
Results for 33 patients in the melflufen/daratumumab/dexamethasone arm and 10 in the melflufen/bortezomib/dexamethasone arm have been previously reported. Patients in the daratumumab-containing arm had a median age of 64, and a median of two prior therapies. High-risk cytogenetics were present in 42%, and 61% were refractory to their last therapy. At a median treatment duration of 8.4 months, the ORR was 70%, consisting of one sCR, one CR, and ten VGPRs, and median PFS was 11.5 months. No DLTS were reported, and the most common grade ≥3 treatment-related AEs were neutropenia (58%) and thrombocytopenia (55%). There were two fatal AEs (myeloma progression and sepsis; general physical health deterioration) of which sepsis was considered treatment related. In the melflufen/bortezomib/dexamethasone arm, the median age was 71 years, and patients had a median
Click to Show/Hide
|
||||
| Related Clinical Trial | |||||
| NCT Number | NCT03481556 | Clinical Status | Phase 1/2 | ||
| Clinical Description | This is an open-label Phase 1/2a study which will enroll patients that have relapsed or relapsed-refractory multiple myeloma to combination regimens of melflufen with currently approved agents. Patients will receive either melflufen+dexamethasone+bortezomib or melflufen+dexamethasone+daratumumab. | ||||
| Experiment 262 Reporting the Activity Data of This PDC | [1] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Median progression-free survival (mPFS) |
Not reached
|
|||
| Patients Enrolled |
Patients with multi-refractory multiple myeloma.
|
||||
| Administration Time | 9.3 month (median) | ||||
| Administration Dosage | 30 or 40 mg | ||||
| MOA of PDC |
Melflufen is highly lipophilic, which promotes its rapid uptake by cells. Once within the cell, melflufen releases its hydrophilic alkylator payloads via the hydrolytic activity of intracellular peptidases (e.g., aminopeptidases). Aminopeptidases are Zn2+-dependent metalloproteinases that remove amino acids at the N-terminal position from oligopeptides and have been associated with multiple tumorigenic processes such as proliferation, apoptosis, differentiation, angiogenesis, and motility. The dependence of melflufen on aminopeptidases was initially demonstrated by the reduced cytotoxic activity of melflufen-but not the alkylator melphalan-when cells were pretreated with bestatin, an antibiotic that is a potent aminopeptidase inhibitor. In addition, structure analogs designed to resist peptide hydrolysis (N-methyl derivative and derivative with D-amino acid) were shown to be almost 100-fold less potent than melflufen. Subsequent in vitro studies demonstrated that hydrolytic cleavage of melflufen by aminopeptidases releases alkylator payloads, including melphalan. In vitro, the activity of melflufen is multi-pronged, including induction of DNA damage, induction of apoptosis, inhibition of VEGF-dependent cell migration, and inhibition of tumor-associated angiogenesis, which have been further reviewed elsewhere. Downregulation of aminopeptidases resulted in reduced melflufen-mediated cytotoxic activity and apoptotic signaling in cultured cells.
Click to Show/Hide
|
||||
| Experiment 263 Reporting the Activity Data of This PDC | [1] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Median progression-free survival (mPFS) |
3.0 months
|
|||
| Patients Enrolled |
Patients with extramedullary disease.
|
||||
| MOA of PDC |
Melflufen is highly lipophilic, which promotes its rapid uptake by cells. Once within the cell, melflufen releases its hydrophilic alkylator payloads via the hydrolytic activity of intracellular peptidases (e.g., aminopeptidases). Aminopeptidases are Zn2+-dependent metalloproteinases that remove amino acids at the N-terminal position from oligopeptides and have been associated with multiple tumorigenic processes such as proliferation, apoptosis, differentiation, angiogenesis, and motility. The dependence of melflufen on aminopeptidases was initially demonstrated by the reduced cytotoxic activity of melflufen-but not the alkylator melphalan-when cells were pretreated with bestatin, an antibiotic that is a potent aminopeptidase inhibitor. In addition, structure analogs designed to resist peptide hydrolysis (N-methyl derivative and derivative with D-amino acid) were shown to be almost 100-fold less potent than melflufen. Subsequent in vitro studies demonstrated that hydrolytic cleavage of melflufen by aminopeptidases releases alkylator payloads, including melphalan. In vitro, the activity of melflufen is multi-pronged, including induction of DNA damage, induction of apoptosis, inhibition of VEGF-dependent cell migration, and inhibition of tumor-associated angiogenesis, which have been further reviewed elsewhere. Downregulation of aminopeptidases resulted in reduced melflufen-mediated cytotoxic activity and apoptotic signaling in cultured cells.
Click to Show/Hide
|
||||
| Description |
The median PFS and OS were 4.2 and 11.6 months for all patients, 4.0 and 11.3 months for patients with triple-class refractory disease, and 3.0 and 8.1 months for patients with extramedullary disease, respectively.
|
||||
| Experiment 264 Reporting the Activity Data of This PDC | [1] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Median progression-free survival (mPFS) |
4.0 months
|
|||
| Patients Enrolled |
Patients with triple-class refractory disease.
|
||||
| MOA of PDC |
Melflufen is highly lipophilic, which promotes its rapid uptake by cells. Once within the cell, melflufen releases its hydrophilic alkylator payloads via the hydrolytic activity of intracellular peptidases (e.g., aminopeptidases). Aminopeptidases are Zn2+-dependent metalloproteinases that remove amino acids at the N-terminal position from oligopeptides and have been associated with multiple tumorigenic processes such as proliferation, apoptosis, differentiation, angiogenesis, and motility. The dependence of melflufen on aminopeptidases was initially demonstrated by the reduced cytotoxic activity of melflufen-but not the alkylator melphalan-when cells were pretreated with bestatin, an antibiotic that is a potent aminopeptidase inhibitor. In addition, structure analogs designed to resist peptide hydrolysis (N-methyl derivative and derivative with D-amino acid) were shown to be almost 100-fold less potent than melflufen. Subsequent in vitro studies demonstrated that hydrolytic cleavage of melflufen by aminopeptidases releases alkylator payloads, including melphalan. In vitro, the activity of melflufen is multi-pronged, including induction of DNA damage, induction of apoptosis, inhibition of VEGF-dependent cell migration, and inhibition of tumor-associated angiogenesis, which have been further reviewed elsewhere. Downregulation of aminopeptidases resulted in reduced melflufen-mediated cytotoxic activity and apoptotic signaling in cultured cells.
Click to Show/Hide
|
||||
| Description |
The median PFS and OS were 4.2 and 11.6 months for all patients, 4.0 and 11.3 months for patients with triple-class refractory disease, and 3.0 and 8.1 months for patients with extramedullary disease, respectively.
|
||||
| Experiment 265 Reporting the Activity Data of This PDC | [1] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Median progression-free survival (mPFS) |
4.2 months
|
|||
| Patients Enrolled |
Patients with multi-refractory multiple myeloma.
|
||||
| Administration Time | 14.3 week (median) | ||||
| Administration Dosage | 40 mg with dexamethasone (40 mg) | ||||
| MOA of PDC |
Melflufen is highly lipophilic, which promotes its rapid uptake by cells. Once within the cell, melflufen releases its hydrophilic alkylator payloads via the hydrolytic activity of intracellular peptidases (e.g., aminopeptidases). Aminopeptidases are Zn2+-dependent metalloproteinases that remove amino acids at the N-terminal position from oligopeptides and have been associated with multiple tumorigenic processes such as proliferation, apoptosis, differentiation, angiogenesis, and motility. The dependence of melflufen on aminopeptidases was initially demonstrated by the reduced cytotoxic activity of melflufen-but not the alkylator melphalan-when cells were pretreated with bestatin, an antibiotic that is a potent aminopeptidase inhibitor. In addition, structure analogs designed to resist peptide hydrolysis (N-methyl derivative and derivative with D-amino acid) were shown to be almost 100-fold less potent than melflufen. Subsequent in vitro studies demonstrated that hydrolytic cleavage of melflufen by aminopeptidases releases alkylator payloads, including melphalan. In vitro, the activity of melflufen is multi-pronged, including induction of DNA damage, induction of apoptosis, inhibition of VEGF-dependent cell migration, and inhibition of tumor-associated angiogenesis, which have been further reviewed elsewhere. Downregulation of aminopeptidases resulted in reduced melflufen-mediated cytotoxic activity and apoptotic signaling in cultured cells.
Click to Show/Hide
|
||||
| Experiment 266 Reporting the Activity Data of This PDC | [1] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Median progression-free survival (mPFS) |
4.2 months
|
|||
| Patients Enrolled |
All patients.
|
||||
| MOA of PDC |
Melflufen is highly lipophilic, which promotes its rapid uptake by cells. Once within the cell, melflufen releases its hydrophilic alkylator payloads via the hydrolytic activity of intracellular peptidases (e.g., aminopeptidases). Aminopeptidases are Zn2+-dependent metalloproteinases that remove amino acids at the N-terminal position from oligopeptides and have been associated with multiple tumorigenic processes such as proliferation, apoptosis, differentiation, angiogenesis, and motility. The dependence of melflufen on aminopeptidases was initially demonstrated by the reduced cytotoxic activity of melflufen-but not the alkylator melphalan-when cells were pretreated with bestatin, an antibiotic that is a potent aminopeptidase inhibitor. In addition, structure analogs designed to resist peptide hydrolysis (N-methyl derivative and derivative with D-amino acid) were shown to be almost 100-fold less potent than melflufen. Subsequent in vitro studies demonstrated that hydrolytic cleavage of melflufen by aminopeptidases releases alkylator payloads, including melphalan. In vitro, the activity of melflufen is multi-pronged, including induction of DNA damage, induction of apoptosis, inhibition of VEGF-dependent cell migration, and inhibition of tumor-associated angiogenesis, which have been further reviewed elsewhere. Downregulation of aminopeptidases resulted in reduced melflufen-mediated cytotoxic activity and apoptotic signaling in cultured cells.
Click to Show/Hide
|
||||
| Description |
The median PFS and OS were 4.2 and 11.6 months for all patients, 4.0 and 11.3 months for patients with triple-class refractory disease, and 3.0 and 8.1 months for patients with extramedullary disease, respectively.
|
||||
| Experiment 267 Reporting the Activity Data of This PDC | [9] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Median progression-free survival (mPFS) |
4.4 months
|
|||
| Patients Enrolled |
96 relapsed/refractory multiple myeloma patients aged <65 years.
|
||||
| MOA of PDC |
In summary, the interpretation of the results from the OCEAN study were impacted by the heterogeneity of the population, with age and previous success of ASCT therapy identified as prognostic factors with study therapies. The safety profile of melflufen and dexamethasone is primarily characterized by hematologic AEs that are clinically manageable. Observed infection rates, which included COVID-19, were generally low. Taken together, these data support the use of melflufen and dexamethasone in patients who have not received a previous ASCT or who underwent a successful ASCT (ie, TTP >36 months post-ASCT). In addition, the favorable efficacy profile and convenience of monthly outpatient infusions, especially for patients without access to other therapeutics such as CAR T-cell therapy or bispecific antibodies, bode well for this combination translating successfully into real-world practice.
Click to Show/Hide
|
||||
| Description |
In this updated survival analysis, median OS (95% CI) was 20.2 months (15.8-24.3) with melflufen and 24.0 months (19.1-28.7) with pomalidomide (HR, 1.14 [95% CI, 0.91-1.43]; P =.24), with a median follow-up time of 31.8 months and 29.8 months, respectively. Because of imbalance in the number of patients who were randomized but not treated, survival was also evaluated in the safety population: median OS (95% CI) was 21.3 months (16.6-24.8) with melflufen and 24.0 months (19.8-28.7) with pomalidomide (HR, 1.12 [95% CI, 0.89-1.42]; P =.33), with the curves overlapping until 10 months after randomization. Sensitivity analyses revealed that the uneven distribution of randomized but not treated patients impacted OS, but not PFS. Although a similar number of patients received subsequent therapy after OCEAN (melflufen group, 169/246 [69%] patients; pomalidomide group, 164/249 [66%] patients), the type of subsequent therapy and timing of subsequent therapy initiation differed between treatment groups.
Click to Show/Hide
|
||||
| Experiment 268 Reporting the Activity Data of This PDC | [1] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Median progression-free survival (mPFS) |
4.4 months
|
|||
| Patients Enrolled |
Patients with multi-refractory multiple myeloma.
|
||||
| MOA of PDC |
Melflufen is highly lipophilic, which promotes its rapid uptake by cells. Once within the cell, melflufen releases its hydrophilic alkylator payloads via the hydrolytic activity of intracellular peptidases (e.g., aminopeptidases). Aminopeptidases are Zn2+-dependent metalloproteinases that remove amino acids at the N-terminal position from oligopeptides and have been associated with multiple tumorigenic processes such as proliferation, apoptosis, differentiation, angiogenesis, and motility. The dependence of melflufen on aminopeptidases was initially demonstrated by the reduced cytotoxic activity of melflufen-but not the alkylator melphalan-when cells were pretreated with bestatin, an antibiotic that is a potent aminopeptidase inhibitor. In addition, structure analogs designed to resist peptide hydrolysis (N-methyl derivative and derivative with D-amino acid) were shown to be almost 100-fold less potent than melflufen. Subsequent in vitro studies demonstrated that hydrolytic cleavage of melflufen by aminopeptidases releases alkylator payloads, including melphalan. In vitro, the activity of melflufen is multi-pronged, including induction of DNA damage, induction of apoptosis, inhibition of VEGF-dependent cell migration, and inhibition of tumor-associated angiogenesis, which have been further reviewed elsewhere. Downregulation of aminopeptidases resulted in reduced melflufen-mediated cytotoxic activity and apoptotic signaling in cultured cells.
Click to Show/Hide
|
||||
| Description |
Among the 13 patients who received single-agent melflufen, the median number of prior therapies was 5 (range, 4-8), the ORR was 8% (1 PR), median PFS was 4.4 months, and median OS was 15.5 months.
|
||||
| Experiment 269 Reporting the Activity Data of This PDC | [5] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Median progression-free survival (mPFS) |
5.6 months
|
|||
| Patients Enrolled |
153 patients refractory to prior alkylators (melflufen, n=78; pomalidomide, n=75).
|
||||
| MOA of PDC |
Melphalan flufenamide (melflufen), a first-in-class alkylating peptide-drug conjugate, plus dexamethasone demonstrated superior progression-free survival (PFS), but not overall survival (OS), versus pomalidomide plus dexamethasone in relapsed/refractory multiple myeloma in the OCEAN study. Time to progression (TTP) <36 months after a prior autologous stem cell transplantation (ASCT) was a negative prognostic factor for OS with melflufen. This post hoc exploratory analysis evaluated patients refractory to prior alkylators (e.g., cyclophosphamide and melphalan) in OCEAN. In 153 patients refractory to prior alkylators (melflufen, n = 78; pomalidomide, n = 75), the melflufen and pomalidomide arms had similar median PFS (5.6 months [95% CI, 4.2-8.3] vs. 4.7 months [95% CI, 3.1-7.3]; hazard ratio [HR], 0.92 [95% CI, 0.63-1.33]) and OS (23.4 months [95% CI, 14.4-31.7] vs. 20.0 months [95% CI, 12.0-28.7]; HR, 0.92 [95% CI, 0.62-1.38]). Among alkylator-refractory patients with a TTP 36 months after a prior ASCT or no prior ASCT (melflufen, n = 54; pomalidomide, n = 53), the observed median PFS and OS were longer in the melflufen arm than the pomalidomide arm. The safety profile of melflufen was consistent with previous reports. These results suggest that melflufen is safe and effective in patients with alkylator-refractory disease, suggesting differentiated activity from other alkylators.
Click to Show/Hide
|
||||
| Description |
In the overall alkylator-refractory group, the melflufen and pomalidomide arms saw a similar median PFS (5.6 months [95% CI, 4.2-8.3] vs. 4.7 months [95% CI, 3.1-7.3]; HR, 0.92 [95% CI, 0.63-1.33]) and median OS (23.4 months [14.4-31.7] vs. 20.0 months [12.0-28.7]; HR, 0.92 [95% CI, 0.62-1.38]). Corresponding results were observed when evaluating PFS and OS in subgroups by type of prior alkylating agent received. In the melflufen and pomalidomide arms, the ORR was 24.4% and 28.0% in patients refractory to alkylators overall, 22.2% and 25.0% in patients refractory to cyclophosphamide, and 33.3% and 26.1% in patients refractory to melphalan, respectively.
Click to Show/Hide
|
||||
| Experiment 270 Reporting the Activity Data of This PDC | [1] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Median progression-free survival (mPFS) |
5.7 months
|
|||
| Patients Enrolled |
Patients with multi-refractory multiple myeloma.
|
||||
| Administration Time | 28-day cycle | ||||
| Administration Dosage | 40 mg with dexamethasone (40 mg) | ||||
| MOA of PDC |
Melflufen is highly lipophilic, which promotes its rapid uptake by cells. Once within the cell, melflufen releases its hydrophilic alkylator payloads via the hydrolytic activity of intracellular peptidases (e.g., aminopeptidases). Aminopeptidases are Zn2+-dependent metalloproteinases that remove amino acids at the N-terminal position from oligopeptides and have been associated with multiple tumorigenic processes such as proliferation, apoptosis, differentiation, angiogenesis, and motility. The dependence of melflufen on aminopeptidases was initially demonstrated by the reduced cytotoxic activity of melflufen-but not the alkylator melphalan-when cells were pretreated with bestatin, an antibiotic that is a potent aminopeptidase inhibitor. In addition, structure analogs designed to resist peptide hydrolysis (N-methyl derivative and derivative with D-amino acid) were shown to be almost 100-fold less potent than melflufen. Subsequent in vitro studies demonstrated that hydrolytic cleavage of melflufen by aminopeptidases releases alkylator payloads, including melphalan. In vitro, the activity of melflufen is multi-pronged, including induction of DNA damage, induction of apoptosis, inhibition of VEGF-dependent cell migration, and inhibition of tumor-associated angiogenesis, which have been further reviewed elsewhere. Downregulation of aminopeptidases resulted in reduced melflufen-mediated cytotoxic activity and apoptotic signaling in cultured cells.
Click to Show/Hide
|
||||
| Experiment 271 Reporting the Activity Data of This PDC | [9] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Median progression-free survival (mPFS) |
7.2 months
|
|||
| Patients Enrolled |
113 relapsed/refractory multiple myeloma patients aged 65-74 years.
|
||||
| MOA of PDC |
In summary, the interpretation of the results from the OCEAN study were impacted by the heterogeneity of the population, with age and previous success of ASCT therapy identified as prognostic factors with study therapies. The safety profile of melflufen and dexamethasone is primarily characterized by hematologic AEs that are clinically manageable. Observed infection rates, which included COVID-19, were generally low. Taken together, these data support the use of melflufen and dexamethasone in patients who have not received a previous ASCT or who underwent a successful ASCT (ie, TTP >36 months post-ASCT). In addition, the favorable efficacy profile and convenience of monthly outpatient infusions, especially for patients without access to other therapeutics such as CAR T-cell therapy or bispecific antibodies, bode well for this combination translating successfully into real-world practice.
Click to Show/Hide
|
||||
| Description |
In this updated survival analysis, median OS (95% CI) was 20.2 months (15.8-24.3) with melflufen and 24.0 months (19.1-28.7) with pomalidomide (HR, 1.14 [95% CI, 0.91-1.43]; P =.24), with a median follow-up time of 31.8 months and 29.8 months, respectively. Because of imbalance in the number of patients who were randomized but not treated, survival was also evaluated in the safety population: median OS (95% CI) was 21.3 months (16.6-24.8) with melflufen and 24.0 months (19.8-28.7) with pomalidomide (HR, 1.12 [95% CI, 0.89-1.42]; P =.33), with the curves overlapping until 10 months after randomization. Sensitivity analyses revealed that the uneven distribution of randomized but not treated patients impacted OS, but not PFS. Although a similar number of patients received subsequent therapy after OCEAN (melflufen group, 169/246 [69%] patients; pomalidomide group, 164/249 [66%] patients), the type of subsequent therapy and timing of subsequent therapy initiation differed between treatment groups.
Click to Show/Hide
|
||||
| Experiment 272 Reporting the Activity Data of This PDC | [9] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Median progression-free survival (mPFS) |
9.3 months
|
|||
| Patients Enrolled |
37 relapsed/refractory multiple myeloma patients aged 75 years.
|
||||
| MOA of PDC |
In summary, the interpretation of the results from the OCEAN study were impacted by the heterogeneity of the population, with age and previous success of ASCT therapy identified as prognostic factors with study therapies. The safety profile of melflufen and dexamethasone is primarily characterized by hematologic AEs that are clinically manageable. Observed infection rates, which included COVID-19, were generally low. Taken together, these data support the use of melflufen and dexamethasone in patients who have not received a previous ASCT or who underwent a successful ASCT (ie, TTP >36 months post-ASCT). In addition, the favorable efficacy profile and convenience of monthly outpatient infusions, especially for patients without access to other therapeutics such as CAR T-cell therapy or bispecific antibodies, bode well for this combination translating successfully into real-world practice.
Click to Show/Hide
|
||||
| Description |
In this updated survival analysis, median OS (95% CI) was 20.2 months (15.8-24.3) with melflufen and 24.0 months (19.1-28.7) with pomalidomide (HR, 1.14 [95% CI, 0.91-1.43]; P =.24), with a median follow-up time of 31.8 months and 29.8 months, respectively. Because of imbalance in the number of patients who were randomized but not treated, survival was also evaluated in the safety population: median OS (95% CI) was 21.3 months (16.6-24.8) with melflufen and 24.0 months (19.8-28.7) with pomalidomide (HR, 1.12 [95% CI, 0.89-1.42]; P =.33), with the curves overlapping until 10 months after randomization. Sensitivity analyses revealed that the uneven distribution of randomized but not treated patients impacted OS, but not PFS. Although a similar number of patients received subsequent therapy after OCEAN (melflufen group, 169/246 [69%] patients; pomalidomide group, 164/249 [66%] patients), the type of subsequent therapy and timing of subsequent therapy initiation differed between treatment groups.
Click to Show/Hide
|
||||
| Experiment 273 Reporting the Activity Data of This PDC | [1] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Median progression-free survival (mPFS) |
14.3 months
|
|||
| Patients Enrolled |
Patients with multi-refractory multiple myeloma.
|
||||
| Administration Time | 6.2 month (median) | ||||
| Administration Dosage | 30 or 40 mg | ||||
| MOA of PDC |
Melflufen is highly lipophilic, which promotes its rapid uptake by cells. Once within the cell, melflufen releases its hydrophilic alkylator payloads via the hydrolytic activity of intracellular peptidases (e.g., aminopeptidases). Aminopeptidases are Zn2+-dependent metalloproteinases that remove amino acids at the N-terminal position from oligopeptides and have been associated with multiple tumorigenic processes such as proliferation, apoptosis, differentiation, angiogenesis, and motility. The dependence of melflufen on aminopeptidases was initially demonstrated by the reduced cytotoxic activity of melflufen-but not the alkylator melphalan-when cells were pretreated with bestatin, an antibiotic that is a potent aminopeptidase inhibitor. In addition, structure analogs designed to resist peptide hydrolysis (N-methyl derivative and derivative with D-amino acid) were shown to be almost 100-fold less potent than melflufen. Subsequent in vitro studies demonstrated that hydrolytic cleavage of melflufen by aminopeptidases releases alkylator payloads, including melphalan. In vitro, the activity of melflufen is multi-pronged, including induction of DNA damage, induction of apoptosis, inhibition of VEGF-dependent cell migration, and inhibition of tumor-associated angiogenesis, which have been further reviewed elsewhere. Downregulation of aminopeptidases resulted in reduced melflufen-mediated cytotoxic activity and apoptotic signaling in cultured cells.
Click to Show/Hide
|
||||
| Experiment 274 Reporting the Activity Data of This PDC | [9] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Median time to dose reduction |
10.1 weeks
|
|||
| Patients Enrolled |
101 relapsed/refractory multiple myeloma patients with TTP <36 month Post-ASCTb.
|
||||
| MOA of PDC |
In summary, the interpretation of the results from the OCEAN study were impacted by the heterogeneity of the population, with age and previous success of ASCT therapy identified as prognostic factors with study therapies. The safety profile of melflufen and dexamethasone is primarily characterized by hematologic AEs that are clinically manageable. Observed infection rates, which included COVID-19, were generally low. Taken together, these data support the use of melflufen and dexamethasone in patients who have not received a previous ASCT or who underwent a successful ASCT (ie, TTP >36 months post-ASCT). In addition, the favorable efficacy profile and convenience of monthly outpatient infusions, especially for patients without access to other therapeutics such as CAR T-cell therapy or bispecific antibodies, bode well for this combination translating successfully into real-world practice.
Click to Show/Hide
|
||||
| Description |
Given the prognostic importance of TTP <36 months post-ASCT in OCEAN, we evaluated this prognostic factor in a post hoc analysis from the HORIZON study. Among 110 patients with triple-class refractory disease who had received ≥3 prior lines of therapy, 77 (70%) had received a previous ASCT and 58 (53%) had TTP <36 months post-ASCT (Suppl. Table S3). In patients with a TTP >36 months post-ASCT or no ASCT versus patients with a TTP <36 months post-ASCT, ORR was higher (29% vs 22%; Suppl. Table S4) and median DOR (7.6 months vs 3.9 months) and median PFS (4.2 months vs 3.4 months) were longer. Since pomalidomide and lenalidomide both belong to the immunomodulatory drugs, we analyzed if the duration of previous treatment with lenalidomide could have impacted the results. The median duration of lenalidomide was 14.4 months in patients with ASCT and TTP < 36 months, 38.3 months in patients with ASCT and TTP > 36 months, and 14.6 months in patients with no previous ASCT. However, the median PFS for patients treated with pomalidomide did not differ substantially between these groups of patients. The safety profile of melflufen and dexamethasone was generally consistent between patients with a TTP >36 months post-ASCT or no ASCT and patients with a TTP <36 months post-ASCT. In OCEAN among the melflufen group, the frequency of grade 3/4 TEAEs (88% and 92%), serious TEAEs (44% and 38%), and fatal adverse events (AEs; 11% and 13%) was similar in patients with a TTP >36 months post-ASCT or no ASCT and patients with TTP <36 months. However, patients with a TTP >36 months post-ASCT or no ASCT had lower rates of TEAEs leading to treatment discontinuation (23% and 31%), the longer median duration of study treatment (35.1 weeks vs 15.1 weeks), and longer median time to experiencing grade 3/4 thrombocytopenia (11.2 weeks vs 4.1 weeks) and grade 3/4 neutropenia (4.8 weeks vs 2.1 weeks) than patients with a TTP <36 months post-ASCT. In HORIZON, patients with a TTP >36 months post-ASCT or no ASCT had lower rates of grade 3/4 TEAEs (88% and 98%), but higher rates of serious TEAEs (64% and 53%) and similar rates of TEAEs leading to treatment discontinuation (29% and 33%) than patients with a TTP <36 months post-ASCT.
Click to Show/Hide
|
||||
| Experiment 275 Reporting the Activity Data of This PDC | [9] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Median time to dose reduction |
21.6 weeks
|
|||
| Patients Enrolled |
145 patients who has relapsed/refractory multiple myeloma with no previous ASCT or TTP >36 month Post-ASCTa.
|
||||
| MOA of PDC |
In summary, the interpretation of the results from the OCEAN study were impacted by the heterogeneity of the population, with age and previous success of ASCT therapy identified as prognostic factors with study therapies. The safety profile of melflufen and dexamethasone is primarily characterized by hematologic AEs that are clinically manageable. Observed infection rates, which included COVID-19, were generally low. Taken together, these data support the use of melflufen and dexamethasone in patients who have not received a previous ASCT or who underwent a successful ASCT (ie, TTP >36 months post-ASCT). In addition, the favorable efficacy profile and convenience of monthly outpatient infusions, especially for patients without access to other therapeutics such as CAR T-cell therapy or bispecific antibodies, bode well for this combination translating successfully into real-world practice.
Click to Show/Hide
|
||||
| Description |
Given the prognostic importance of TTP <36 months post-ASCT in OCEAN, we evaluated this prognostic factor in a post hoc analysis from the HORIZON study. Among 110 patients with triple-class refractory disease who had received ≥3 prior lines of therapy, 77 (70%) had received a previous ASCT and 58 (53%) had TTP <36 months post-ASCT (Suppl. Table S3). In patients with a TTP >36 months post-ASCT or no ASCT versus patients with a TTP <36 months post-ASCT, ORR was higher (29% vs 22%; Suppl. Table S4) and median DOR (7.6 months vs 3.9 months) and median PFS (4.2 months vs 3.4 months) were longer. Since pomalidomide and lenalidomide both belong to the immunomodulatory drugs, we analyzed if the duration of previous treatment with lenalidomide could have impacted the results. The median duration of lenalidomide was 14.4 months in patients with ASCT and TTP < 36 months, 38.3 months in patients with ASCT and TTP > 36 months, and 14.6 months in patients with no previous ASCT. However, the median PFS for patients treated with pomalidomide did not differ substantially between these groups of patients. The safety profile of melflufen and dexamethasone was generally consistent between patients with a TTP >36 months post-ASCT or no ASCT and patients with a TTP <36 months post-ASCT. In OCEAN among the melflufen group, the frequency of grade 3/4 TEAEs (88% and 92%), serious TEAEs (44% and 38%), and fatal adverse events (AEs; 11% and 13%) was similar in patients with a TTP >36 months post-ASCT or no ASCT and patients with TTP <36 months. However, patients with a TTP >36 months post-ASCT or no ASCT had lower rates of TEAEs leading to treatment discontinuation (23% and 31%), the longer median duration of study treatment (35.1 weeks vs 15.1 weeks), and longer median time to experiencing grade 3/4 thrombocytopenia (11.2 weeks vs 4.1 weeks) and grade 3/4 neutropenia (4.8 weeks vs 2.1 weeks) than patients with a TTP <36 months post-ASCT. In HORIZON, patients with a TTP >36 months post-ASCT or no ASCT had lower rates of grade 3/4 TEAEs (88% and 98%), but higher rates of serious TEAEs (64% and 53%) and similar rates of TEAEs leading to treatment discontinuation (29% and 33%) than patients with a TTP <36 months post-ASCT.
Click to Show/Hide
|
||||
| Experiment 276 Reporting the Activity Data of This PDC | [9] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Median time to grade 3/4 neutropenia |
2.1 weeks
|
|||
| Patients Enrolled |
101 relapsed/refractory multiple myeloma patients with TTP <36 month Post-ASCTb.
|
||||
| MOA of PDC |
In summary, the interpretation of the results from the OCEAN study were impacted by the heterogeneity of the population, with age and previous success of ASCT therapy identified as prognostic factors with study therapies. The safety profile of melflufen and dexamethasone is primarily characterized by hematologic AEs that are clinically manageable. Observed infection rates, which included COVID-19, were generally low. Taken together, these data support the use of melflufen and dexamethasone in patients who have not received a previous ASCT or who underwent a successful ASCT (ie, TTP >36 months post-ASCT). In addition, the favorable efficacy profile and convenience of monthly outpatient infusions, especially for patients without access to other therapeutics such as CAR T-cell therapy or bispecific antibodies, bode well for this combination translating successfully into real-world practice.
Click to Show/Hide
|
||||
| Description |
Given the prognostic importance of TTP <36 months post-ASCT in OCEAN, we evaluated this prognostic factor in a post hoc analysis from the HORIZON study. Among 110 patients with triple-class refractory disease who had received ≥3 prior lines of therapy, 77 (70%) had received a previous ASCT and 58 (53%) had TTP <36 months post-ASCT (Suppl. Table S3). In patients with a TTP >36 months post-ASCT or no ASCT versus patients with a TTP <36 months post-ASCT, ORR was higher (29% vs 22%; Suppl. Table S4) and median DOR (7.6 months vs 3.9 months) and median PFS (4.2 months vs 3.4 months) were longer. Since pomalidomide and lenalidomide both belong to the immunomodulatory drugs, we analyzed if the duration of previous treatment with lenalidomide could have impacted the results. The median duration of lenalidomide was 14.4 months in patients with ASCT and TTP < 36 months, 38.3 months in patients with ASCT and TTP > 36 months, and 14.6 months in patients with no previous ASCT. However, the median PFS for patients treated with pomalidomide did not differ substantially between these groups of patients. The safety profile of melflufen and dexamethasone was generally consistent between patients with a TTP >36 months post-ASCT or no ASCT and patients with a TTP <36 months post-ASCT. In OCEAN among the melflufen group, the frequency of grade 3/4 TEAEs (88% and 92%), serious TEAEs (44% and 38%), and fatal adverse events (AEs; 11% and 13%) was similar in patients with a TTP >36 months post-ASCT or no ASCT and patients with TTP <36 months. However, patients with a TTP >36 months post-ASCT or no ASCT had lower rates of TEAEs leading to treatment discontinuation (23% and 31%), the longer median duration of study treatment (35.1 weeks vs 15.1 weeks), and longer median time to experiencing grade 3/4 thrombocytopenia (11.2 weeks vs 4.1 weeks) and grade 3/4 neutropenia (4.8 weeks vs 2.1 weeks) than patients with a TTP <36 months post-ASCT. In HORIZON, patients with a TTP >36 months post-ASCT or no ASCT had lower rates of grade 3/4 TEAEs (88% and 98%), but higher rates of serious TEAEs (64% and 53%) and similar rates of TEAEs leading to treatment discontinuation (29% and 33%) than patients with a TTP <36 months post-ASCT.
Click to Show/Hide
|
||||
| Experiment 277 Reporting the Activity Data of This PDC | [9] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Median time to grade 3/4 neutropenia |
4.8 weeks
|
|||
| Patients Enrolled |
145 patients who has relapsed/refractory multiple myeloma with no previous ASCT or TTP >36 month Post-ASCTa.
|
||||
| MOA of PDC |
In summary, the interpretation of the results from the OCEAN study were impacted by the heterogeneity of the population, with age and previous success of ASCT therapy identified as prognostic factors with study therapies. The safety profile of melflufen and dexamethasone is primarily characterized by hematologic AEs that are clinically manageable. Observed infection rates, which included COVID-19, were generally low. Taken together, these data support the use of melflufen and dexamethasone in patients who have not received a previous ASCT or who underwent a successful ASCT (ie, TTP >36 months post-ASCT). In addition, the favorable efficacy profile and convenience of monthly outpatient infusions, especially for patients without access to other therapeutics such as CAR T-cell therapy or bispecific antibodies, bode well for this combination translating successfully into real-world practice.
Click to Show/Hide
|
||||
| Description |
Given the prognostic importance of TTP <36 months post-ASCT in OCEAN, we evaluated this prognostic factor in a post hoc analysis from the HORIZON study. Among 110 patients with triple-class refractory disease who had received ≥3 prior lines of therapy, 77 (70%) had received a previous ASCT and 58 (53%) had TTP <36 months post-ASCT (Suppl. Table S3). In patients with a TTP >36 months post-ASCT or no ASCT versus patients with a TTP <36 months post-ASCT, ORR was higher (29% vs 22%; Suppl. Table S4) and median DOR (7.6 months vs 3.9 months) and median PFS (4.2 months vs 3.4 months) were longer. Since pomalidomide and lenalidomide both belong to the immunomodulatory drugs, we analyzed if the duration of previous treatment with lenalidomide could have impacted the results. The median duration of lenalidomide was 14.4 months in patients with ASCT and TTP < 36 months, 38.3 months in patients with ASCT and TTP > 36 months, and 14.6 months in patients with no previous ASCT. However, the median PFS for patients treated with pomalidomide did not differ substantially between these groups of patients. The safety profile of melflufen and dexamethasone was generally consistent between patients with a TTP >36 months post-ASCT or no ASCT and patients with a TTP <36 months post-ASCT. In OCEAN among the melflufen group, the frequency of grade 3/4 TEAEs (88% and 92%), serious TEAEs (44% and 38%), and fatal adverse events (AEs; 11% and 13%) was similar in patients with a TTP >36 months post-ASCT or no ASCT and patients with TTP <36 months. However, patients with a TTP >36 months post-ASCT or no ASCT had lower rates of TEAEs leading to treatment discontinuation (23% and 31%), the longer median duration of study treatment (35.1 weeks vs 15.1 weeks), and longer median time to experiencing grade 3/4 thrombocytopenia (11.2 weeks vs 4.1 weeks) and grade 3/4 neutropenia (4.8 weeks vs 2.1 weeks) than patients with a TTP <36 months post-ASCT. In HORIZON, patients with a TTP >36 months post-ASCT or no ASCT had lower rates of grade 3/4 TEAEs (88% and 98%), but higher rates of serious TEAEs (64% and 53%) and similar rates of TEAEs leading to treatment discontinuation (29% and 33%) than patients with a TTP <36 months post-ASCT.
Click to Show/Hide
|
||||
| Experiment 278 Reporting the Activity Data of This PDC | [9] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Median time to grade 3/4 thrombocytopenia |
4.1 weeks
|
|||
| Patients Enrolled |
101 relapsed/refractory multiple myeloma patients with TTP <36 month Post-ASCTb.
|
||||
| MOA of PDC |
In summary, the interpretation of the results from the OCEAN study were impacted by the heterogeneity of the population, with age and previous success of ASCT therapy identified as prognostic factors with study therapies. The safety profile of melflufen and dexamethasone is primarily characterized by hematologic AEs that are clinically manageable. Observed infection rates, which included COVID-19, were generally low. Taken together, these data support the use of melflufen and dexamethasone in patients who have not received a previous ASCT or who underwent a successful ASCT (ie, TTP >36 months post-ASCT). In addition, the favorable efficacy profile and convenience of monthly outpatient infusions, especially for patients without access to other therapeutics such as CAR T-cell therapy or bispecific antibodies, bode well for this combination translating successfully into real-world practice.
Click to Show/Hide
|
||||
| Description |
Given the prognostic importance of TTP <36 months post-ASCT in OCEAN, we evaluated this prognostic factor in a post hoc analysis from the HORIZON study. Among 110 patients with triple-class refractory disease who had received ≥3 prior lines of therapy, 77 (70%) had received a previous ASCT and 58 (53%) had TTP <36 months post-ASCT (Suppl. Table S3). In patients with a TTP >36 months post-ASCT or no ASCT versus patients with a TTP <36 months post-ASCT, ORR was higher (29% vs 22%; Suppl. Table S4) and median DOR (7.6 months vs 3.9 months) and median PFS (4.2 months vs 3.4 months) were longer. Since pomalidomide and lenalidomide both belong to the immunomodulatory drugs, we analyzed if the duration of previous treatment with lenalidomide could have impacted the results. The median duration of lenalidomide was 14.4 months in patients with ASCT and TTP < 36 months, 38.3 months in patients with ASCT and TTP > 36 months, and 14.6 months in patients with no previous ASCT. However, the median PFS for patients treated with pomalidomide did not differ substantially between these groups of patients. The safety profile of melflufen and dexamethasone was generally consistent between patients with a TTP >36 months post-ASCT or no ASCT and patients with a TTP <36 months post-ASCT. In OCEAN among the melflufen group, the frequency of grade 3/4 TEAEs (88% and 92%), serious TEAEs (44% and 38%), and fatal adverse events (AEs; 11% and 13%) was similar in patients with a TTP >36 months post-ASCT or no ASCT and patients with TTP <36 months. However, patients with a TTP >36 months post-ASCT or no ASCT had lower rates of TEAEs leading to treatment discontinuation (23% and 31%), the longer median duration of study treatment (35.1 weeks vs 15.1 weeks), and longer median time to experiencing grade 3/4 thrombocytopenia (11.2 weeks vs 4.1 weeks) and grade 3/4 neutropenia (4.8 weeks vs 2.1 weeks) than patients with a TTP <36 months post-ASCT. In HORIZON, patients with a TTP >36 months post-ASCT or no ASCT had lower rates of grade 3/4 TEAEs (88% and 98%), but higher rates of serious TEAEs (64% and 53%) and similar rates of TEAEs leading to treatment discontinuation (29% and 33%) than patients with a TTP <36 months post-ASCT.
Click to Show/Hide
|
||||
| Experiment 279 Reporting the Activity Data of This PDC | [9] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Median time to grade 3/4 thrombocytopenia |
11.2 weeks
|
|||
| Patients Enrolled |
145 patients who has relapsed/refractory multiple myeloma with no previous ASCT or TTP >36 month Post-ASCTa.
|
||||
| MOA of PDC |
In summary, the interpretation of the results from the OCEAN study were impacted by the heterogeneity of the population, with age and previous success of ASCT therapy identified as prognostic factors with study therapies. The safety profile of melflufen and dexamethasone is primarily characterized by hematologic AEs that are clinically manageable. Observed infection rates, which included COVID-19, were generally low. Taken together, these data support the use of melflufen and dexamethasone in patients who have not received a previous ASCT or who underwent a successful ASCT (ie, TTP >36 months post-ASCT). In addition, the favorable efficacy profile and convenience of monthly outpatient infusions, especially for patients without access to other therapeutics such as CAR T-cell therapy or bispecific antibodies, bode well for this combination translating successfully into real-world practice.
Click to Show/Hide
|
||||
| Description |
Given the prognostic importance of TTP <36 months post-ASCT in OCEAN, we evaluated this prognostic factor in a post hoc analysis from the HORIZON study. Among 110 patients with triple-class refractory disease who had received ≥3 prior lines of therapy, 77 (70%) had received a previous ASCT and 58 (53%) had TTP <36 months post-ASCT (Suppl. Table S3). In patients with a TTP >36 months post-ASCT or no ASCT versus patients with a TTP <36 months post-ASCT, ORR was higher (29% vs 22%; Suppl. Table S4) and median DOR (7.6 months vs 3.9 months) and median PFS (4.2 months vs 3.4 months) were longer. Since pomalidomide and lenalidomide both belong to the immunomodulatory drugs, we analyzed if the duration of previous treatment with lenalidomide could have impacted the results. The median duration of lenalidomide was 14.4 months in patients with ASCT and TTP < 36 months, 38.3 months in patients with ASCT and TTP > 36 months, and 14.6 months in patients with no previous ASCT. However, the median PFS for patients treated with pomalidomide did not differ substantially between these groups of patients. The safety profile of melflufen and dexamethasone was generally consistent between patients with a TTP >36 months post-ASCT or no ASCT and patients with a TTP <36 months post-ASCT. In OCEAN among the melflufen group, the frequency of grade 3/4 TEAEs (88% and 92%), serious TEAEs (44% and 38%), and fatal adverse events (AEs; 11% and 13%) was similar in patients with a TTP >36 months post-ASCT or no ASCT and patients with TTP <36 months. However, patients with a TTP >36 months post-ASCT or no ASCT had lower rates of TEAEs leading to treatment discontinuation (23% and 31%), the longer median duration of study treatment (35.1 weeks vs 15.1 weeks), and longer median time to experiencing grade 3/4 thrombocytopenia (11.2 weeks vs 4.1 weeks) and grade 3/4 neutropenia (4.8 weeks vs 2.1 weeks) than patients with a TTP <36 months post-ASCT. In HORIZON, patients with a TTP >36 months post-ASCT or no ASCT had lower rates of grade 3/4 TEAEs (88% and 98%), but higher rates of serious TEAEs (64% and 53%) and similar rates of TEAEs leading to treatment discontinuation (29% and 33%) than patients with a TTP <36 months post-ASCT.
Click to Show/Hide
|
||||
| Experiment 280 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Melflufen-related adverse event rate |
92.90%
|
|||
| Patients Enrolled |
14 patients with relapsed refractory multiple myeloma.
|
||||
| Administration Time | 28-day cycle | ||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (melflufen) is a first-in-class peptide-drug conjugate that utilizes increased peptidase expression to selectively release potent alkylating agents inside tumor cells. Melflufen is hydrolyzed by peptidases and esterases to melphalan either directly or through an intermediate metabolite, desethyl-melflufen. The high lipophilicity of melflufen facilitates passive diffusion across cell membranes. The activity and tolerability of melflufen in relapsed/refractory multiple myeloma (RRMM) were demonstrated in the O-12-M1 (NCT01897714), OCEAN (NCT03151811), and HORIZON (NCT02963493) trials.
Click to Show/Hide
|
||||
| Description |
Overall, at least one TEAE was reported in 13 (92.9%) and 13 (100.0%) patients in Arms A and B, respectively (Table 3). During cycle 1, 9 patients (64.3%) and 12 patients (92.3%), respectively, had at least one TEAE. Cumulatively, grade 3 or 4 AEs occurred in 12 (85.7%) and 12 (92.3%) patients, respectively, and serious AEs were reported in 5 (35.7%) and 9 (69.2%) patients, respectively. The most common any-grade AEs in Arms A and B, respectively, were thrombocytopenia (10 [71.4%]; 10 [76.9%]), neutropenia (9 [64.3%]; 9 [69.2%]), and anemia (9 [64.3%]; 7 [53.8%]). No phlebitis or local-infusion-related reactions were reported based on pre- and post-infusion inspection of the IV site, and there were no extravasations observed in Arm A or B. Similarly, VIP scores collected on Day 1 post-infusion and on Day 8 indicated that patients had healthy IV sites (VIP score of 0) with no signs of phlebitis following PVC administration of melflufen. The most common non-hematological AE was positive SARS-CoV-2 test (Arm A: 2 [14.3%]; Arm B: 4 [30.8%]). Pneumonia was the most common serious AE (Arm A: 2 [14.3%]; Arm B: 2 [15.4%]). The most common AE considered related to melflufen and/or dexamethasone by investigators was thrombocytopenia (Arm A: 10 [71.4%]; Arm B: 10 [76.9%]). AEs led to treatment discontinuation in 3 (21.4%) and 6 (46.2%) patients in Arms A and B, respectively.
Click to Show/Hide
|
||||
| Half life period | 75.6 h | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT04412707 | Clinical Status | Phase 2 | ||
| Clinical Description | This is a randomized, two-period, cross-over Phase 2 study, comparing PK, and assessing safety and tolerability and efficacy of peripheral and central intravenous administration of melflufen in patients with RRMM. It is an international study, enrolling patients in US and Europe. The study will enroll patients following at least 2 lines of prior therapy. | ||||
| Experiment 281 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Minimal response rate |
15%
|
|||
| Patients Enrolled |
246 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 282 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Minimal response rate |
17%
|
|||
| Patients Enrolled |
246 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 283 Reporting the Activity Data of This PDC | [2] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Minor response (MR) |
0%
|
|||
| Patients Enrolled |
14 patients no prior ASCT or TTP >36 months after ASCT.
|
||||
| MOA of PDC |
Melphalan flufenamide (melflufen), a first-in-class alkylating peptide-drug conjugate, plus dexamethasone was approved in Europe for use in patients with triple-class refractory relapsed/refractory multiple myeloma (RRMM) with 3 prior lines of therapy and without prior autologous stem cell transplantation (ASCT) or with a time to progression >36 months after prior ASCT. The randomized LIGHTHOUSE study (NCT04649060) assessed melflufen plus daratumumab and dexamethasone (melflufen group) versus daratumumab in patients with RRMM with disease refractory to an immunomodulatory agent and a proteasome inhibitor or who had received 3 prior lines of therapy including an immunomodulatory agent and a proteasome inhibitor. A partial clinical hold issued by the US Food and Drug Administration for all melflufen studies led to financial constraints and premature study closure on February 23rd 2022 (data cut-off date). In total, 54 of 240 planned patients were randomized (melflufen group, N=27; daratumumab group, N=27). Median progression-free survival (PFS) was not reached in the melflufen group versus 4.9 months in the daratumumab group (Hazard Ratio: 0.18 [95% Confidence Interval, 0.05-0.65]; P=0.0032) at a median follow-up time of 7.1 and 6.6 months, respectively. Overall response rate (ORR) was 59% in the melflufen group versus 30% in the daratumumab group (P=0.0300). The most common grade 3 treatment-emergent adverse events in the melflufen group versus daratumumab group were neutropenia (50% vs. 12%), thrombocytopenia (50% vs. 8%), and anemia (32% vs. 19%). Melflufen plus daratumumab and dexamethasone demonstrated superior PFS and ORR versus daratumumab in RRMM and a safety profile comparable to previously published melflufen studies.
Click to Show/Hide
|
||||
| Description |
Efficacy endpoints were more pronounced in favor of the melflufen group compared with the daratumumab group among patients with no prior ASCT or TTP >36 months after a prior ASCT (melflufen group, N=14; daratumumab group, N=15). Median PFS was NR in the melflufen group and 3.9 months (95% CI: 1.4-4.9) in the daratumumab group (HR, 0.06 [95% CI: 0.01-0.49]; log-rank P=0.0005). Fewer OS events were reported in the melflufen group (1 event [7%] vs. 4 events [27%] in the daratumumab group; log-rank P=0.0369). The ORR was 64% (95% CI: 35-87) in the melflufen group and 13% (95% CI: 2-41) in the daratumumab group (P=0.0055). More patients in the melflufen group had a CR (1 patient [7%] vs. 0 patients [0%]) or VGPR (2 patients [14%] vs. 1 patient [7%]) compared with the daratumumab group.
Click to Show/Hide
|
||||
| Related Clinical Trial | |||||
| NCT Number | NCT04649060 | Clinical Status | Phase 3 | ||
| Clinical Description | This was a randomized, controlled, open-label, Phase 3 multicenter study which enrolled patients with Relapsed-Refractory Multiple Myeloma (RRMM) who were either double refractory to an Immunomodulatory Drug (IMiD) and a Proteasome Inhibitor (PI) (regardless of the number of prior lines of therapy), or had received at least 3 prior lines of therapy including an IMiD and a PI. Patients received treatment with melflufen+dexamethasone+daratumumab or daratumumab until documented progressive disease, unacceptable toxicity, or patient/treating physician decision. Patients in the daratumumab treatment arm had the option to receive treatment with melflufen+dexamethasone+daratumumab after confirmed progressive disease. | ||||
| Experiment 284 Reporting the Activity Data of This PDC | [4] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Nausea |
32.00%
|
|||
| Patients Enrolled |
157 patients with multiple myeloma.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melflufen is a first-in-class peptide-drug conjugate, targeting aminopeptidase which has an increased expression in fast-growing and aggressive malignancies. The lipophilicity of melflufen allows for passive diffusion, selectively targeting myeloma cells. Once inside the cell, melflufen is hydrolyzed to active alkylating metabolites melphalan and desethyl-melflufen. Melflufen and the active metabolites trigger irreversible DNA damage, inhibit proliferation, induces apoptosis, and express antiangiogenic effects. In addition, melflufen demonstrated activity in myeloma cells with documented impaired or absent Tp53 expression and documented resistance to bortezomib, dexamethasone, and melphalan.
Click to Show/Hide
|
||||
| Description |
Based on the safety data collected during the HORIZON trial, treatment emergent adverse events occurred in 100% of patients including 100 patients (64%) having at least 1 CTCAE grade 4 adverse effect. Hematologic grade 3 or 4 adverse effects including thrombocytopenia (76%), neutropenia (79%), anemia (43%), and infections (11%) were the most commonly reported. Other adverse effects, such as fatigue (55%), nausea (32%), diarrhea (27%), and decreased appetite (14%), were similar to other alkylating agents. Pyrexia (24%), including febrile neutropenia (5%), and respiratory tract infections (24%) were contributed to hematologic toxicities.
Click to Show/Hide
|
||||
| Experiment 285 Reporting the Activity Data of This PDC | [1] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Nausea |
27.00%
|
|||
| Patients Enrolled |
Patients with multi-refractory multiple myeloma.
|
||||
| MOA of PDC |
Melflufen is highly lipophilic, which promotes its rapid uptake by cells. Once within the cell, melflufen releases its hydrophilic alkylator payloads via the hydrolytic activity of intracellular peptidases (e.g., aminopeptidases). Aminopeptidases are Zn2+-dependent metalloproteinases that remove amino acids at the N-terminal position from oligopeptides and have been associated with multiple tumorigenic processes such as proliferation, apoptosis, differentiation, angiogenesis, and motility. The dependence of melflufen on aminopeptidases was initially demonstrated by the reduced cytotoxic activity of melflufen-but not the alkylator melphalan-when cells were pretreated with bestatin, an antibiotic that is a potent aminopeptidase inhibitor. In addition, structure analogs designed to resist peptide hydrolysis (N-methyl derivative and derivative with D-amino acid) were shown to be almost 100-fold less potent than melflufen. Subsequent in vitro studies demonstrated that hydrolytic cleavage of melflufen by aminopeptidases releases alkylator payloads, including melphalan. In vitro, the activity of melflufen is multi-pronged, including induction of DNA damage, induction of apoptosis, inhibition of VEGF-dependent cell migration, and inhibition of tumor-associated angiogenesis, which have been further reviewed elsewhere. Downregulation of aminopeptidases resulted in reduced melflufen-mediated cytotoxic activity and apoptotic signaling in cultured cells.
Click to Show/Hide
|
||||
| Description |
Melflufen plus dexamethasone was generally manageable in this heavily pretreated patient population [51]. All patients experienced ≥1 AE, most commonly hematologic AEs including thrombocytopenia (73%), neutropenia (69%), and anemia (64%). The most common non-hematologic AEs included pyrexia (40%), asthenia (31%), fatigue (29%), nausea (27%), and diarrhea (24%).
Click to Show/Hide
|
||||
| Experiment 286 Reporting the Activity Data of This PDC | [2] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Neutropenia |
50%
|
|||
| MOA of PDC |
Melphalan flufenamide (melflufen), a first-in-class alkylating peptide-drug conjugate, plus dexamethasone was approved in Europe for use in patients with triple-class refractory relapsed/refractory multiple myeloma (RRMM) with 3 prior lines of therapy and without prior autologous stem cell transplantation (ASCT) or with a time to progression >36 months after prior ASCT. The randomized LIGHTHOUSE study (NCT04649060) assessed melflufen plus daratumumab and dexamethasone (melflufen group) versus daratumumab in patients with RRMM with disease refractory to an immunomodulatory agent and a proteasome inhibitor or who had received 3 prior lines of therapy including an immunomodulatory agent and a proteasome inhibitor. A partial clinical hold issued by the US Food and Drug Administration for all melflufen studies led to financial constraints and premature study closure on February 23rd 2022 (data cut-off date). In total, 54 of 240 planned patients were randomized (melflufen group, N=27; daratumumab group, N=27). Median progression-free survival (PFS) was not reached in the melflufen group versus 4.9 months in the daratumumab group (Hazard Ratio: 0.18 [95% Confidence Interval, 0.05-0.65]; P=0.0032) at a median follow-up time of 7.1 and 6.6 months, respectively. Overall response rate (ORR) was 59% in the melflufen group versus 30% in the daratumumab group (P=0.0300). The most common grade 3 treatment-emergent adverse events in the melflufen group versus daratumumab group were neutropenia (50% vs. 12%), thrombocytopenia (50% vs. 8%), and anemia (32% vs. 19%). Melflufen plus daratumumab and dexamethasone demonstrated superior PFS and ORR versus daratumumab in RRMM and a safety profile comparable to previously published melflufen studies.
Click to Show/Hide
|
||||
| Description |
The safety population included patients who received ≥1 dose of melflufen, daratumumab, or dexamethasone (melflufen group) and 26 patients who received daratumumab monotherapy. In the safety population, ≥1 TEAE was reported in 21 patients (96%) with melflufen, daratumumab, and dexamethasone and 22 patients (85%) with daratumumab. Overall, grade ≥3 TEAE occurred in 18 patients (82%) with melflufen, daratumumab, and dexamethasone and 14 patients (54%) with daratumumab. The most common hematologic grade ≥3 TEAE were neutropenia (melflufen group, 11 patients [50%]; daratumumab group, 3 patients [12%]), thrombocytopenia (melflufen group, 11 patients [50%]; daratumumab group, 2 patients [8%]), and anemia (melflufen group, 7 patients [32%]; daratumumab group, 5 patients [19%]). The most common non-hematologic grade ≥3 TEAE were pneumonia (melflufen group, 2 patients [9%]; daratumumab group, 2 patients [8%]) and femur fracture (melflufen group, 0 patients [0%]; daratumumab group, 2 patients [8%]); of these, 1 event (5%) of pneumonia in the melflufen group and 1 event (4%) of femur fracture in the daratumumab group were considered treatment-related TEAE by the investigator. Serious AE occurred in 6 patients (27%) with melflufen, daratumumab, and dexamethasone, and 12 patients (46%) with daratumumab. The most common serious AE (occurring in ≥4 patients overall) were anemia (melflufen group, 2 patients [9%]; daratumumab group, 3 patients [12%]) and pneumonia (melflufen group, 2 patients [9%]; daratumumab group, 2 patients [8%]). TEAE leading to treatment discontinuation occurred in 2 patients (9%) in the melflufen group (neutropenia and thrombocytopenia, N=1 each) and 4 patients (15%) in the daratumumab group (anemia, disease progression, hypercalcemia, and renal failure, N=1 each). Overall, 5 patients died on study before the crossover: 2 patients who received melflufen, daratumumab, and dexamethasone (1 due to disease progression and 1 due to unknown reasons, both >30 days after the last dose of study treatment) and 3 patients who received daratumumab (1 due to disease progression and 1 due to unknown reasons, both ≤30 days after the last dose of study treatment and 1 due to an AE [COVID-19 pneumonia], >30 days after the last dose of study treatment). In addition, one patient who crossed over to receive melflufen, daratumumab, and dexamethasone after progression on daratumumab died.
Click to Show/Hide
|
||||
| In Vivo Model | 22 relapsed/refractory multiple myeloma. | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT04649060 | Clinical Status | Phase 3 | ||
| Clinical Description | This was a randomized, controlled, open-label, Phase 3 multicenter study which enrolled patients with Relapsed-Refractory Multiple Myeloma (RRMM) who were either double refractory to an Immunomodulatory Drug (IMiD) and a Proteasome Inhibitor (PI) (regardless of the number of prior lines of therapy), or had received at least 3 prior lines of therapy including an IMiD and a PI. Patients received treatment with melflufen+dexamethasone+daratumumab or daratumumab until documented progressive disease, unacceptable toxicity, or patient/treating physician decision. Patients in the daratumumab treatment arm had the option to receive treatment with melflufen+dexamethasone+daratumumab after confirmed progressive disease. | ||||
| Experiment 287 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Neutropenia |
64.30%
|
|||
| Patients Enrolled |
14 patients with relapsed refractory multiple myeloma.
|
||||
| Administration Time | 28-day cycle | ||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (melflufen) is a first-in-class peptide-drug conjugate that utilizes increased peptidase expression to selectively release potent alkylating agents inside tumor cells. Melflufen is hydrolyzed by peptidases and esterases to melphalan either directly or through an intermediate metabolite, desethyl-melflufen. The high lipophilicity of melflufen facilitates passive diffusion across cell membranes. The activity and tolerability of melflufen in relapsed/refractory multiple myeloma (RRMM) were demonstrated in the O-12-M1 (NCT01897714), OCEAN (NCT03151811), and HORIZON (NCT02963493) trials.
Click to Show/Hide
|
||||
| Description |
Overall, at least one TEAE was reported in 13 (92.9%) and 13 (100.0%) patients in Arms A and B, respectively (Table 3). During cycle 1, 9 patients (64.3%) and 12 patients (92.3%), respectively, had at least one TEAE. Cumulatively, grade 3 or 4 AEs occurred in 12 (85.7%) and 12 (92.3%) patients, respectively, and serious AEs were reported in 5 (35.7%) and 9 (69.2%) patients, respectively. The most common any-grade AEs in Arms A and B, respectively, were thrombocytopenia (10 [71.4%]; 10 [76.9%]), neutropenia (9 [64.3%]; 9 [69.2%]), and anemia (9 [64.3%]; 7 [53.8%]). No phlebitis or local-infusion-related reactions were reported based on pre- and post-infusion inspection of the IV site, and there were no extravasations observed in Arm A or B. Similarly, VIP scores collected on Day 1 post-infusion and on Day 8 indicated that patients had healthy IV sites (VIP score of 0) with no signs of phlebitis following PVC administration of melflufen. The most common non-hematological AE was positive SARS-CoV-2 test (Arm A: 2 [14.3%]; Arm B: 4 [30.8%]). Pneumonia was the most common serious AE (Arm A: 2 [14.3%]; Arm B: 2 [15.4%]). The most common AE considered related to melflufen and/or dexamethasone by investigators was thrombocytopenia (Arm A: 10 [71.4%]; Arm B: 10 [76.9%]). AEs led to treatment discontinuation in 3 (21.4%) and 6 (46.2%) patients in Arms A and B, respectively.
Click to Show/Hide
|
||||
| Half life period | 75.6 h | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT04412707 | Clinical Status | Phase 2 | ||
| Clinical Description | This is a randomized, two-period, cross-over Phase 2 study, comparing PK, and assessing safety and tolerability and efficacy of peripheral and central intravenous administration of melflufen in patients with RRMM. It is an international study, enrolling patients in US and Europe. The study will enroll patients following at least 2 lines of prior therapy. | ||||
| Experiment 288 Reporting the Activity Data of This PDC | [4] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Neutropenia |
5.00%
|
|||
| Patients Enrolled |
157 patients with multiple myeloma.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melflufen is a first-in-class peptide-drug conjugate, targeting aminopeptidase which has an increased expression in fast-growing and aggressive malignancies. The lipophilicity of melflufen allows for passive diffusion, selectively targeting myeloma cells. Once inside the cell, melflufen is hydrolyzed to active alkylating metabolites melphalan and desethyl-melflufen. Melflufen and the active metabolites trigger irreversible DNA damage, inhibit proliferation, induces apoptosis, and express antiangiogenic effects. In addition, melflufen demonstrated activity in myeloma cells with documented impaired or absent Tp53 expression and documented resistance to bortezomib, dexamethasone, and melphalan.
Click to Show/Hide
|
||||
| Description |
Based on the safety data collected during the HORIZON trial, treatment emergent adverse events occurred in 100% of patients including 100 patients (64%) having at least 1 CTCAE grade 4 adverse effect. Hematologic grade 3 or 4 adverse effects including thrombocytopenia (76%), neutropenia (79%), anemia (43%), and infections (11%) were the most commonly reported. Other adverse effects, such as fatigue (55%), nausea (32%), diarrhea (27%), and decreased appetite (14%), were similar to other alkylating agents. Pyrexia (24%), including febrile neutropenia (5%), and respiratory tract infections (24%) were contributed to hematologic toxicities.
Click to Show/Hide
|
||||
| Experiment 289 Reporting the Activity Data of This PDC | [4] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Neutropenia |
79.00%
|
|||
| Patients Enrolled |
157 patients with multiple myeloma.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melflufen is a first-in-class peptide-drug conjugate, targeting aminopeptidase which has an increased expression in fast-growing and aggressive malignancies. The lipophilicity of melflufen allows for passive diffusion, selectively targeting myeloma cells. Once inside the cell, melflufen is hydrolyzed to active alkylating metabolites melphalan and desethyl-melflufen. Melflufen and the active metabolites trigger irreversible DNA damage, inhibit proliferation, induces apoptosis, and express antiangiogenic effects. In addition, melflufen demonstrated activity in myeloma cells with documented impaired or absent Tp53 expression and documented resistance to bortezomib, dexamethasone, and melphalan.
Click to Show/Hide
|
||||
| Description |
Based on the safety data collected during the HORIZON trial, treatment emergent adverse events occurred in 100% of patients including 100 patients (64%) having at least 1 CTCAE grade 4 adverse effect. Hematologic grade 3 or 4 adverse effects including thrombocytopenia (76%), neutropenia (79%), anemia (43%), and infections (11%) were the most commonly reported. Other adverse effects, such as fatigue (55%), nausea (32%), diarrhea (27%), and decreased appetite (14%), were similar to other alkylating agents. Pyrexia (24%), including febrile neutropenia (5%), and respiratory tract infections (24%) were contributed to hematologic toxicities.
Click to Show/Hide
|
||||
| Experiment 290 Reporting the Activity Data of This PDC | [9] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Neutropenia |
62%
|
|||
| Patients Enrolled |
101 relapsed/refractory multiple myeloma patients with TTP <36 month Post-ASCTb.
|
||||
| MOA of PDC |
In summary, the interpretation of the results from the OCEAN study were impacted by the heterogeneity of the population, with age and previous success of ASCT therapy identified as prognostic factors with study therapies. The safety profile of melflufen and dexamethasone is primarily characterized by hematologic AEs that are clinically manageable. Observed infection rates, which included COVID-19, were generally low. Taken together, these data support the use of melflufen and dexamethasone in patients who have not received a previous ASCT or who underwent a successful ASCT (ie, TTP >36 months post-ASCT). In addition, the favorable efficacy profile and convenience of monthly outpatient infusions, especially for patients without access to other therapeutics such as CAR T-cell therapy or bispecific antibodies, bode well for this combination translating successfully into real-world practice.
Click to Show/Hide
|
||||
| Description |
Given the prognostic importance of TTP <36 months post-ASCT in OCEAN, we evaluated this prognostic factor in a post hoc analysis from the HORIZON study. Among 110 patients with triple-class refractory disease who had received ≥3 prior lines of therapy, 77 (70%) had received a previous ASCT and 58 (53%) had TTP <36 months post-ASCT (Suppl. Table S3). In patients with a TTP >36 months post-ASCT or no ASCT versus patients with a TTP <36 months post-ASCT, ORR was higher (29% vs 22%; Suppl. Table S4) and median DOR (7.6 months vs 3.9 months) and median PFS (4.2 months vs 3.4 months) were longer. Since pomalidomide and lenalidomide both belong to the immunomodulatory drugs, we analyzed if the duration of previous treatment with lenalidomide could have impacted the results. The median duration of lenalidomide was 14.4 months in patients with ASCT and TTP < 36 months, 38.3 months in patients with ASCT and TTP > 36 months, and 14.6 months in patients with no previous ASCT. However, the median PFS for patients treated with pomalidomide did not differ substantially between these groups of patients. The safety profile of melflufen and dexamethasone was generally consistent between patients with a TTP >36 months post-ASCT or no ASCT and patients with a TTP <36 months post-ASCT. In OCEAN among the melflufen group, the frequency of grade 3/4 TEAEs (88% and 92%), serious TEAEs (44% and 38%), and fatal adverse events (AEs; 11% and 13%) was similar in patients with a TTP >36 months post-ASCT or no ASCT and patients with TTP <36 months. However, patients with a TTP >36 months post-ASCT or no ASCT had lower rates of TEAEs leading to treatment discontinuation (23% and 31%), the longer median duration of study treatment (35.1 weeks vs 15.1 weeks), and longer median time to experiencing grade 3/4 thrombocytopenia (11.2 weeks vs 4.1 weeks) and grade 3/4 neutropenia (4.8 weeks vs 2.1 weeks) than patients with a TTP <36 months post-ASCT. In HORIZON, patients with a TTP >36 months post-ASCT or no ASCT had lower rates of grade 3/4 TEAEs (88% and 98%), but higher rates of serious TEAEs (64% and 53%) and similar rates of TEAEs leading to treatment discontinuation (29% and 33%) than patients with a TTP <36 months post-ASCT.
Click to Show/Hide
|
||||
| Experiment 291 Reporting the Activity Data of This PDC | [9] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Neutropenia |
66%
|
|||
| Patients Enrolled |
145 patients who has relapsed/refractory multiple myeloma with no previous ASCT or TTP >36 month Post-ASCTa.
|
||||
| MOA of PDC |
In summary, the interpretation of the results from the OCEAN study were impacted by the heterogeneity of the population, with age and previous success of ASCT therapy identified as prognostic factors with study therapies. The safety profile of melflufen and dexamethasone is primarily characterized by hematologic AEs that are clinically manageable. Observed infection rates, which included COVID-19, were generally low. Taken together, these data support the use of melflufen and dexamethasone in patients who have not received a previous ASCT or who underwent a successful ASCT (ie, TTP >36 months post-ASCT). In addition, the favorable efficacy profile and convenience of monthly outpatient infusions, especially for patients without access to other therapeutics such as CAR T-cell therapy or bispecific antibodies, bode well for this combination translating successfully into real-world practice.
Click to Show/Hide
|
||||
| Description |
Given the prognostic importance of TTP <36 months post-ASCT in OCEAN, we evaluated this prognostic factor in a post hoc analysis from the HORIZON study. Among 110 patients with triple-class refractory disease who had received ≥3 prior lines of therapy, 77 (70%) had received a previous ASCT and 58 (53%) had TTP <36 months post-ASCT (Suppl. Table S3). In patients with a TTP >36 months post-ASCT or no ASCT versus patients with a TTP <36 months post-ASCT, ORR was higher (29% vs 22%; Suppl. Table S4) and median DOR (7.6 months vs 3.9 months) and median PFS (4.2 months vs 3.4 months) were longer. Since pomalidomide and lenalidomide both belong to the immunomodulatory drugs, we analyzed if the duration of previous treatment with lenalidomide could have impacted the results. The median duration of lenalidomide was 14.4 months in patients with ASCT and TTP < 36 months, 38.3 months in patients with ASCT and TTP > 36 months, and 14.6 months in patients with no previous ASCT. However, the median PFS for patients treated with pomalidomide did not differ substantially between these groups of patients. The safety profile of melflufen and dexamethasone was generally consistent between patients with a TTP >36 months post-ASCT or no ASCT and patients with a TTP <36 months post-ASCT. In OCEAN among the melflufen group, the frequency of grade 3/4 TEAEs (88% and 92%), serious TEAEs (44% and 38%), and fatal adverse events (AEs; 11% and 13%) was similar in patients with a TTP >36 months post-ASCT or no ASCT and patients with TTP <36 months. However, patients with a TTP >36 months post-ASCT or no ASCT had lower rates of TEAEs leading to treatment discontinuation (23% and 31%), the longer median duration of study treatment (35.1 weeks vs 15.1 weeks), and longer median time to experiencing grade 3/4 thrombocytopenia (11.2 weeks vs 4.1 weeks) and grade 3/4 neutropenia (4.8 weeks vs 2.1 weeks) than patients with a TTP <36 months post-ASCT. In HORIZON, patients with a TTP >36 months post-ASCT or no ASCT had lower rates of grade 3/4 TEAEs (88% and 98%), but higher rates of serious TEAEs (64% and 53%) and similar rates of TEAEs leading to treatment discontinuation (29% and 33%) than patients with a TTP <36 months post-ASCT.
Click to Show/Hide
|
||||
| Experiment 292 Reporting the Activity Data of This PDC | [1] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Neutropenia |
69.00%
|
|||
| Patients Enrolled |
Patients with multi-refractory multiple myeloma.
|
||||
| MOA of PDC |
Melflufen is highly lipophilic, which promotes its rapid uptake by cells. Once within the cell, melflufen releases its hydrophilic alkylator payloads via the hydrolytic activity of intracellular peptidases (e.g., aminopeptidases). Aminopeptidases are Zn2+-dependent metalloproteinases that remove amino acids at the N-terminal position from oligopeptides and have been associated with multiple tumorigenic processes such as proliferation, apoptosis, differentiation, angiogenesis, and motility. The dependence of melflufen on aminopeptidases was initially demonstrated by the reduced cytotoxic activity of melflufen-but not the alkylator melphalan-when cells were pretreated with bestatin, an antibiotic that is a potent aminopeptidase inhibitor. In addition, structure analogs designed to resist peptide hydrolysis (N-methyl derivative and derivative with D-amino acid) were shown to be almost 100-fold less potent than melflufen. Subsequent in vitro studies demonstrated that hydrolytic cleavage of melflufen by aminopeptidases releases alkylator payloads, including melphalan. In vitro, the activity of melflufen is multi-pronged, including induction of DNA damage, induction of apoptosis, inhibition of VEGF-dependent cell migration, and inhibition of tumor-associated angiogenesis, which have been further reviewed elsewhere. Downregulation of aminopeptidases resulted in reduced melflufen-mediated cytotoxic activity and apoptotic signaling in cultured cells.
Click to Show/Hide
|
||||
| Description |
Melflufen plus dexamethasone was generally manageable in this heavily pretreated patient population [51]. All patients experienced ≥1 AE, most commonly hematologic AEs including thrombocytopenia (73%), neutropenia (69%), and anemia (64%). The most common non-hematologic AEs included pyrexia (40%), asthenia (31%), fatigue (29%), nausea (27%), and diarrhea (24%).
Click to Show/Hide
|
||||
| Experiment 293 Reporting the Activity Data of This PDC | [5] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Neutropenia |
73.85%
|
|||
| Patients Enrolled |
153 patients refractory to prior alkylators (melflufen, n=78; pomalidomide, n=75).
|
||||
| MOA of PDC |
Melphalan flufenamide (melflufen), a first-in-class alkylating peptide-drug conjugate, plus dexamethasone demonstrated superior progression-free survival (PFS), but not overall survival (OS), versus pomalidomide plus dexamethasone in relapsed/refractory multiple myeloma in the OCEAN study. Time to progression (TTP) <36 months after a prior autologous stem cell transplantation (ASCT) was a negative prognostic factor for OS with melflufen. This post hoc exploratory analysis evaluated patients refractory to prior alkylators (e.g., cyclophosphamide and melphalan) in OCEAN. In 153 patients refractory to prior alkylators (melflufen, n = 78; pomalidomide, n = 75), the melflufen and pomalidomide arms had similar median PFS (5.6 months [95% CI, 4.2-8.3] vs. 4.7 months [95% CI, 3.1-7.3]; hazard ratio [HR], 0.92 [95% CI, 0.63-1.33]) and OS (23.4 months [95% CI, 14.4-31.7] vs. 20.0 months [95% CI, 12.0-28.7]; HR, 0.92 [95% CI, 0.62-1.38]). Among alkylator-refractory patients with a TTP 36 months after a prior ASCT or no prior ASCT (melflufen, n = 54; pomalidomide, n = 53), the observed median PFS and OS were longer in the melflufen arm than the pomalidomide arm. The safety profile of melflufen was consistent with previous reports. These results suggest that melflufen is safe and effective in patients with alkylator-refractory disease, suggesting differentiated activity from other alkylators.
Click to Show/Hide
|
||||
| Description |
Overall, the safety profile of melflufen plus dexamethasone in the alkylator-refractory group was consistent between treatment arms (Table 2). In the melflufen and pomalidomide arms, respectively, the frequency of treatment-emergent adverse events (TEAEs; 99% vs. 97%), Grade 3 or 4 TEAEs (85% vs. 82%), serious TEAEs (49% vs. 53%), and fatal TEAEs (19% vs. 16%) were similar (Table 2). However, melflufen compared with pomalidomide saw more dose modifications (76% vs. 67%) and dose reductions (47% vs. 14%), comparable dose delays (57% vs. 51%) but less treatment discontinuation (27% vs. 34%). When comparing patients refractory and not refractory to prior alkylators, rates of TEAEs were generally comparable except for slightly lower rates of serious and fatal TEAEs observed in patients not refractory to alkylators. Among Grade 3 or 4 TEAEs of special interest, melflufen saw more thrombocytopenia (73% vs. 14%), neutropenia (65% vs. 55%), and leukopenia or white blood cell decrease (14% vs. 3%), but less infection (15% vs. 26%), than pomalidomide. Notably, melflufen compared with pomalidomide saw a longer median time to dose reduction (106 days [range, 28-443] vs. 47 days [range, 28-225]), Grade 3 or 4 thrombocytopenia (52 days [range, 15-451] vs. 19 days [range, 8-91]), and Grade 3 or 4 neutropenia (36 days [range, 8-561] vs. 22 days [range, 8-470]).
Click to Show/Hide
|
||||
| Experiment 294 Reporting the Activity Data of This PDC | [9] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Neutropenia concurrent with grade 3/4 infection |
2%
|
|||
| Patients Enrolled |
145 patients who has relapsed/refractory multiple myeloma with no previous ASCT or TTP >36 month Post-ASCTa.
|
||||
| MOA of PDC |
In summary, the interpretation of the results from the OCEAN study were impacted by the heterogeneity of the population, with age and previous success of ASCT therapy identified as prognostic factors with study therapies. The safety profile of melflufen and dexamethasone is primarily characterized by hematologic AEs that are clinically manageable. Observed infection rates, which included COVID-19, were generally low. Taken together, these data support the use of melflufen and dexamethasone in patients who have not received a previous ASCT or who underwent a successful ASCT (ie, TTP >36 months post-ASCT). In addition, the favorable efficacy profile and convenience of monthly outpatient infusions, especially for patients without access to other therapeutics such as CAR T-cell therapy or bispecific antibodies, bode well for this combination translating successfully into real-world practice.
Click to Show/Hide
|
||||
| Description |
Given the prognostic importance of TTP <36 months post-ASCT in OCEAN, we evaluated this prognostic factor in a post hoc analysis from the HORIZON study. Among 110 patients with triple-class refractory disease who had received ≥3 prior lines of therapy, 77 (70%) had received a previous ASCT and 58 (53%) had TTP <36 months post-ASCT (Suppl. Table S3). In patients with a TTP >36 months post-ASCT or no ASCT versus patients with a TTP <36 months post-ASCT, ORR was higher (29% vs 22%; Suppl. Table S4) and median DOR (7.6 months vs 3.9 months) and median PFS (4.2 months vs 3.4 months) were longer. Since pomalidomide and lenalidomide both belong to the immunomodulatory drugs, we analyzed if the duration of previous treatment with lenalidomide could have impacted the results. The median duration of lenalidomide was 14.4 months in patients with ASCT and TTP < 36 months, 38.3 months in patients with ASCT and TTP > 36 months, and 14.6 months in patients with no previous ASCT. However, the median PFS for patients treated with pomalidomide did not differ substantially between these groups of patients. The safety profile of melflufen and dexamethasone was generally consistent between patients with a TTP >36 months post-ASCT or no ASCT and patients with a TTP <36 months post-ASCT. In OCEAN among the melflufen group, the frequency of grade 3/4 TEAEs (88% and 92%), serious TEAEs (44% and 38%), and fatal adverse events (AEs; 11% and 13%) was similar in patients with a TTP >36 months post-ASCT or no ASCT and patients with TTP <36 months. However, patients with a TTP >36 months post-ASCT or no ASCT had lower rates of TEAEs leading to treatment discontinuation (23% and 31%), the longer median duration of study treatment (35.1 weeks vs 15.1 weeks), and longer median time to experiencing grade 3/4 thrombocytopenia (11.2 weeks vs 4.1 weeks) and grade 3/4 neutropenia (4.8 weeks vs 2.1 weeks) than patients with a TTP <36 months post-ASCT. In HORIZON, patients with a TTP >36 months post-ASCT or no ASCT had lower rates of grade 3/4 TEAEs (88% and 98%), but higher rates of serious TEAEs (64% and 53%) and similar rates of TEAEs leading to treatment discontinuation (29% and 33%) than patients with a TTP <36 months post-ASCT.
Click to Show/Hide
|
||||
| Experiment 295 Reporting the Activity Data of This PDC | [9] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Neutropenia concurrent with grade 3/4 infection |
4%
|
|||
| Patients Enrolled |
101 relapsed/refractory multiple myeloma patients with TTP <36 month Post-ASCTb.
|
||||
| MOA of PDC |
In summary, the interpretation of the results from the OCEAN study were impacted by the heterogeneity of the population, with age and previous success of ASCT therapy identified as prognostic factors with study therapies. The safety profile of melflufen and dexamethasone is primarily characterized by hematologic AEs that are clinically manageable. Observed infection rates, which included COVID-19, were generally low. Taken together, these data support the use of melflufen and dexamethasone in patients who have not received a previous ASCT or who underwent a successful ASCT (ie, TTP >36 months post-ASCT). In addition, the favorable efficacy profile and convenience of monthly outpatient infusions, especially for patients without access to other therapeutics such as CAR T-cell therapy or bispecific antibodies, bode well for this combination translating successfully into real-world practice.
Click to Show/Hide
|
||||
| Description |
Given the prognostic importance of TTP <36 months post-ASCT in OCEAN, we evaluated this prognostic factor in a post hoc analysis from the HORIZON study. Among 110 patients with triple-class refractory disease who had received ≥3 prior lines of therapy, 77 (70%) had received a previous ASCT and 58 (53%) had TTP <36 months post-ASCT (Suppl. Table S3). In patients with a TTP >36 months post-ASCT or no ASCT versus patients with a TTP <36 months post-ASCT, ORR was higher (29% vs 22%; Suppl. Table S4) and median DOR (7.6 months vs 3.9 months) and median PFS (4.2 months vs 3.4 months) were longer. Since pomalidomide and lenalidomide both belong to the immunomodulatory drugs, we analyzed if the duration of previous treatment with lenalidomide could have impacted the results. The median duration of lenalidomide was 14.4 months in patients with ASCT and TTP < 36 months, 38.3 months in patients with ASCT and TTP > 36 months, and 14.6 months in patients with no previous ASCT. However, the median PFS for patients treated with pomalidomide did not differ substantially between these groups of patients. The safety profile of melflufen and dexamethasone was generally consistent between patients with a TTP >36 months post-ASCT or no ASCT and patients with a TTP <36 months post-ASCT. In OCEAN among the melflufen group, the frequency of grade 3/4 TEAEs (88% and 92%), serious TEAEs (44% and 38%), and fatal adverse events (AEs; 11% and 13%) was similar in patients with a TTP >36 months post-ASCT or no ASCT and patients with TTP <36 months. However, patients with a TTP >36 months post-ASCT or no ASCT had lower rates of TEAEs leading to treatment discontinuation (23% and 31%), the longer median duration of study treatment (35.1 weeks vs 15.1 weeks), and longer median time to experiencing grade 3/4 thrombocytopenia (11.2 weeks vs 4.1 weeks) and grade 3/4 neutropenia (4.8 weeks vs 2.1 weeks) than patients with a TTP <36 months post-ASCT. In HORIZON, patients with a TTP >36 months post-ASCT or no ASCT had lower rates of grade 3/4 TEAEs (88% and 98%), but higher rates of serious TEAEs (64% and 53%) and similar rates of TEAEs leading to treatment discontinuation (29% and 33%) than patients with a TTP <36 months post-ASCT.
Click to Show/Hide
|
||||
| Experiment 296 Reporting the Activity Data of This PDC | [5] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Neutropenia concurrent with grade 3/4 infection |
100%
|
|||
| Patients Enrolled |
153 patients refractory to prior alkylators (melflufen, n=78; pomalidomide, n=75).
|
||||
| MOA of PDC |
Melphalan flufenamide (melflufen), a first-in-class alkylating peptide-drug conjugate, plus dexamethasone demonstrated superior progression-free survival (PFS), but not overall survival (OS), versus pomalidomide plus dexamethasone in relapsed/refractory multiple myeloma in the OCEAN study. Time to progression (TTP) <36 months after a prior autologous stem cell transplantation (ASCT) was a negative prognostic factor for OS with melflufen. This post hoc exploratory analysis evaluated patients refractory to prior alkylators (e.g., cyclophosphamide and melphalan) in OCEAN. In 153 patients refractory to prior alkylators (melflufen, n = 78; pomalidomide, n = 75), the melflufen and pomalidomide arms had similar median PFS (5.6 months [95% CI, 4.2-8.3] vs. 4.7 months [95% CI, 3.1-7.3]; hazard ratio [HR], 0.92 [95% CI, 0.63-1.33]) and OS (23.4 months [95% CI, 14.4-31.7] vs. 20.0 months [95% CI, 12.0-28.7]; HR, 0.92 [95% CI, 0.62-1.38]). Among alkylator-refractory patients with a TTP 36 months after a prior ASCT or no prior ASCT (melflufen, n = 54; pomalidomide, n = 53), the observed median PFS and OS were longer in the melflufen arm than the pomalidomide arm. The safety profile of melflufen was consistent with previous reports. These results suggest that melflufen is safe and effective in patients with alkylator-refractory disease, suggesting differentiated activity from other alkylators.
Click to Show/Hide
|
||||
| Description |
Overall, the safety profile of melflufen plus dexamethasone in the alkylator-refractory group was consistent between treatment arms (Table 2). In the melflufen and pomalidomide arms, respectively, the frequency of treatment-emergent adverse events (TEAEs; 99% vs. 97%), Grade 3 or 4 TEAEs (85% vs. 82%), serious TEAEs (49% vs. 53%), and fatal TEAEs (19% vs. 16%) were similar (Table 2). However, melflufen compared with pomalidomide saw more dose modifications (76% vs. 67%) and dose reductions (47% vs. 14%), comparable dose delays (57% vs. 51%) but less treatment discontinuation (27% vs. 34%). When comparing patients refractory and not refractory to prior alkylators, rates of TEAEs were generally comparable except for slightly lower rates of serious and fatal TEAEs observed in patients not refractory to alkylators. Among Grade 3 or 4 TEAEs of special interest, melflufen saw more thrombocytopenia (73% vs. 14%), neutropenia (65% vs. 55%), and leukopenia or white blood cell decrease (14% vs. 3%), but less infection (15% vs. 26%), than pomalidomide. Notably, melflufen compared with pomalidomide saw a longer median time to dose reduction (106 days [range, 28-443] vs. 47 days [range, 28-225]), Grade 3 or 4 thrombocytopenia (52 days [range, 15-451] vs. 19 days [range, 8-91]), and Grade 3 or 4 neutropenia (36 days [range, 8-561] vs. 22 days [range, 8-470]).
Click to Show/Hide
|
||||
| Experiment 297 Reporting the Activity Data of This PDC | [2] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Neutrophil count decrease |
9%
|
|||
| MOA of PDC |
Melphalan flufenamide (melflufen), a first-in-class alkylating peptide-drug conjugate, plus dexamethasone was approved in Europe for use in patients with triple-class refractory relapsed/refractory multiple myeloma (RRMM) with 3 prior lines of therapy and without prior autologous stem cell transplantation (ASCT) or with a time to progression >36 months after prior ASCT. The randomized LIGHTHOUSE study (NCT04649060) assessed melflufen plus daratumumab and dexamethasone (melflufen group) versus daratumumab in patients with RRMM with disease refractory to an immunomodulatory agent and a proteasome inhibitor or who had received 3 prior lines of therapy including an immunomodulatory agent and a proteasome inhibitor. A partial clinical hold issued by the US Food and Drug Administration for all melflufen studies led to financial constraints and premature study closure on February 23rd 2022 (data cut-off date). In total, 54 of 240 planned patients were randomized (melflufen group, N=27; daratumumab group, N=27). Median progression-free survival (PFS) was not reached in the melflufen group versus 4.9 months in the daratumumab group (Hazard Ratio: 0.18 [95% Confidence Interval, 0.05-0.65]; P=0.0032) at a median follow-up time of 7.1 and 6.6 months, respectively. Overall response rate (ORR) was 59% in the melflufen group versus 30% in the daratumumab group (P=0.0300). The most common grade 3 treatment-emergent adverse events in the melflufen group versus daratumumab group were neutropenia (50% vs. 12%), thrombocytopenia (50% vs. 8%), and anemia (32% vs. 19%). Melflufen plus daratumumab and dexamethasone demonstrated superior PFS and ORR versus daratumumab in RRMM and a safety profile comparable to previously published melflufen studies.
Click to Show/Hide
|
||||
| Description |
The safety population included patients who received ≥1 dose of melflufen, daratumumab, or dexamethasone (melflufen group) and 26 patients who received daratumumab monotherapy. In the safety population, ≥1 TEAE was reported in 21 patients (96%) with melflufen, daratumumab, and dexamethasone and 22 patients (85%) with daratumumab. Overall, grade ≥3 TEAE occurred in 18 patients (82%) with melflufen, daratumumab, and dexamethasone and 14 patients (54%) with daratumumab. The most common hematologic grade ≥3 TEAE were neutropenia (melflufen group, 11 patients [50%]; daratumumab group, 3 patients [12%]), thrombocytopenia (melflufen group, 11 patients [50%]; daratumumab group, 2 patients [8%]), and anemia (melflufen group, 7 patients [32%]; daratumumab group, 5 patients [19%]). The most common non-hematologic grade ≥3 TEAE were pneumonia (melflufen group, 2 patients [9%]; daratumumab group, 2 patients [8%]) and femur fracture (melflufen group, 0 patients [0%]; daratumumab group, 2 patients [8%]); of these, 1 event (5%) of pneumonia in the melflufen group and 1 event (4%) of femur fracture in the daratumumab group were considered treatment-related TEAE by the investigator. Serious AE occurred in 6 patients (27%) with melflufen, daratumumab, and dexamethasone, and 12 patients (46%) with daratumumab. The most common serious AE (occurring in ≥4 patients overall) were anemia (melflufen group, 2 patients [9%]; daratumumab group, 3 patients [12%]) and pneumonia (melflufen group, 2 patients [9%]; daratumumab group, 2 patients [8%]). TEAE leading to treatment discontinuation occurred in 2 patients (9%) in the melflufen group (neutropenia and thrombocytopenia, N=1 each) and 4 patients (15%) in the daratumumab group (anemia, disease progression, hypercalcemia, and renal failure, N=1 each). Overall, 5 patients died on study before the crossover: 2 patients who received melflufen, daratumumab, and dexamethasone (1 due to disease progression and 1 due to unknown reasons, both >30 days after the last dose of study treatment) and 3 patients who received daratumumab (1 due to disease progression and 1 due to unknown reasons, both ≤30 days after the last dose of study treatment and 1 due to an AE [COVID-19 pneumonia], >30 days after the last dose of study treatment). In addition, one patient who crossed over to receive melflufen, daratumumab, and dexamethasone after progression on daratumumab died.
Click to Show/Hide
|
||||
| In Vivo Model | 22 relapsed/refractory multiple myeloma. | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT04649060 | Clinical Status | Phase 3 | ||
| Clinical Description | This was a randomized, controlled, open-label, Phase 3 multicenter study which enrolled patients with Relapsed-Refractory Multiple Myeloma (RRMM) who were either double refractory to an Immunomodulatory Drug (IMiD) and a Proteasome Inhibitor (PI) (regardless of the number of prior lines of therapy), or had received at least 3 prior lines of therapy including an IMiD and a PI. Patients received treatment with melflufen+dexamethasone+daratumumab or daratumumab until documented progressive disease, unacceptable toxicity, or patient/treating physician decision. Patients in the daratumumab treatment arm had the option to receive treatment with melflufen+dexamethasone+daratumumab after confirmed progressive disease. | ||||
| Experiment 298 Reporting the Activity Data of This PDC | [10] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Objective response rate (ORR) |
27%
|
|||
| Administration Time | 15.5 months | ||||
| MOA of PDC |
Melflufen, a highly lipophilic PDC, takes a novel approach by taking advantage of increased aminopeptidase activity to selectively increase the release and concentration of cytotoxic alkylating agents inside of tumor cells. Being highly lipophilic, melflufen does not require active transport, a process that may be defective in cancer cells and contribute to chemoresistance, but instead rapidly enters cells via passive diffusion. The lipophilic nature of melflufen also likely results in its favorable distribution to bone marrow, a fatty tissue, and the physiological component most relevant to MM. Once inside the tumor cells, melflufen is rapidly hydrolyzed by aminopeptidases, enzymes that are found in normal cells but are overexpressed in MM and upon which cancer cells are particularly dependent. This hydrolysis releases potent alkylating agents - most notably melphalan and des-ethyl melflufen - within the cells. Aminopeptidase-driven release of these hydrophilic molecules, which cannot readily diffuse out, thereby results in intracellular trapping. Leveraging high tumor cell aminopeptidase concentrations to rapidly drive intracellular alkylating agent release may provide a safety advantage over alkylators, such as melphalan, which lack such a mechanism for tumor cell targeting, particularly in tumors with an aggressive phenotype.
Click to Show/Hide
|
||||
| Description |
OCEAN randomized patients to 28-day cycles of melflufen 40 mg intravenous on day 1 plus dexamethasone 40 mg oral (days 1, 8, 15, and 22) or pomalidomide 4 mg oral (days 1-21) plus dexamethasone 40 mg oral (days 1, 8, 15, and 22). The primary objective was to compare the PFS of melflufen plus dexamethasone and pomalidomide plus dexamethasone by independent review. Secondary endpoints include comparing ORR, OS, and safety and tolerability. Notably, the OCEAN patient population and study design mirrored those of the MM-003 study to allow for the most robust comparison between melflufen and pomalidomide. Primary results of the OCEAN trial were recently published, with additional survival follow-up ongoing. In total, 495 patients were randomized (246 to the melflufen arm and 249 to the pomalidomide arm). The study met its primary endpoints, with melflufen plus dexamethasone demonstrating a superior PFS to pomalidomide plus dexamethasone (median PFS: 6.8 months vs 4.9 months; hazard ratio [HR], 0.79 [95% CI, 0.64-0.98]; P = 0.03), but OS favored pomalidomide plus dexamethasone (median OS: 19.8 months vs 25.0 months; HR, 1.10 [95% CI, 0.85-1.44]; not significant). However, additional exploratory and post-hoc analyses identified previous ASCT and age as significant prognostic factors, which is not surprising given that transplant eligibility and age are generally correlated. Patients who had not received a previous ASCT (melflufen, n = 121; pomalidomide, n = 129) had better PFS and OS with melflufen plus dexamethasone than with pomalidomide plus dexamethasone (median PFS: 9.3 months vs 4.6 months; HR, 0.59 [95% CI, 0.44-0.79]; P < 0.001; median OS: 21.6 months vs 16.5 months; HR, 0.78 [95% CI, 0.55-1.12]; not significant), while patients who had received previous ASCT (melflufen, n = 125; pomalidomide, n = 120) saw similar PFS between groups but worse OS with melflufen plus dexamethasone than with pomalidomide plus dexamethasone (median PFS: 4.4 months vs 5.2 months; HR, 1.06 [95% CI, 0.79-1.43]; not significant; median OS: 16.7 months vs 31.0 months; HR, 1.61 [95% CI, 1.09-2.40]; P = 0.02). In patients aged ≥75, PFS was more favorable with melflufen (HR, 0.43 [95% CI, 0.24-0.76]; P = 0.003) but in patients aged <65, OS data favored pomalidomide (HR, 1.71 [95% CI, 1.09-2.69]; P = 0.02). Safety was evaluated in patients who received at least one dose of study medication (melflufen, n = 228; pomalidomide, n = 246).
Click to Show/Hide
|
||||
| Related Clinical Trial | |||||
| NCT Number | NCT03151811 | Clinical Status | Phase 3 | ||
| Clinical Description | This was a randomized, controlled, open-label, Phase 3 multicenter study which enrolled patients with RRMM following 2-4 lines of prior therapy and who were refractory to lenalidomide in the last line of therapy as demonstrated by disease progression on or within 60 days of completion of the last dose of lenalidomide. Patients received either melflufen+dex or pomalidomide+dex. | ||||
| Experiment 299 Reporting the Activity Data of This PDC | [2] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Objective response rate (ORR) |
59% (39-78)
|
|||
| MOA of PDC |
Melphalan flufenamide (melflufen), a first-in-class alkylating peptide-drug conjugate, plus dexamethasone was approved in Europe for use in patients with triple-class refractory relapsed/refractory multiple myeloma (RRMM) with 3 prior lines of therapy and without prior autologous stem cell transplantation (ASCT) or with a time to progression >36 months after prior ASCT. The randomized LIGHTHOUSE study (NCT04649060) assessed melflufen plus daratumumab and dexamethasone (melflufen group) versus daratumumab in patients with RRMM with disease refractory to an immunomodulatory agent and a proteasome inhibitor or who had received 3 prior lines of therapy including an immunomodulatory agent and a proteasome inhibitor. A partial clinical hold issued by the US Food and Drug Administration for all melflufen studies led to financial constraints and premature study closure on February 23rd 2022 (data cut-off date). In total, 54 of 240 planned patients were randomized (melflufen group, N=27; daratumumab group, N=27). Median progression-free survival (PFS) was not reached in the melflufen group versus 4.9 months in the daratumumab group (Hazard Ratio: 0.18 [95% Confidence Interval, 0.05-0.65]; P=0.0032) at a median follow-up time of 7.1 and 6.6 months, respectively. Overall response rate (ORR) was 59% in the melflufen group versus 30% in the daratumumab group (P=0.0300). The most common grade 3 treatment-emergent adverse events in the melflufen group versus daratumumab group were neutropenia (50% vs. 12%), thrombocytopenia (50% vs. 8%), and anemia (32% vs. 19%). Melflufen plus daratumumab and dexamethasone demonstrated superior PFS and ORR versus daratumumab in RRMM and a safety profile comparable to previously published melflufen studies.
Click to Show/Hide
|
||||
| Description |
In the ITT population, with a median follow-up of 7.1 months in the melflufen group, the median PFS was not reached (NR) and with a median follow-up of 6.6 months in the daratumumab group, the median PFS was 4.9 months (95% CI: 3.4-NR; HR: 0.18 [95% CI: 0.05-0.65]; log-rankP=0.0032). OS was immature, with 2 events (7%) in the melflufen group and 4 events (15%) in the daratumumab group (HR: 0.47 [95% CI: 0.09-2.57]; log-rankP=0.3721) at a median follow-up of 7.6 months and 6.6 months, respectively. The ORR was 59% (95% CI: 39-78) in the melflufen group and 30% (95% CI: 14-50) in the daratumumab group (P=0.0300). More patients in the melflufen group had a complete response (CR; 1 patient [4%]vs. 0 patients [0%]) and very good partial response (VGPR; 4 patients [15%]vs. 3 patients [11%]) compared with the daratumumab group.
Click to Show/Hide
|
||||
| In Vivo Model | 27 Intent-to-treat (ITT) population. | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT04649060 | Clinical Status | Phase 3 | ||
| Clinical Description | This was a randomized, controlled, open-label, Phase 3 multicenter study which enrolled patients with Relapsed-Refractory Multiple Myeloma (RRMM) who were either double refractory to an Immunomodulatory Drug (IMiD) and a Proteasome Inhibitor (PI) (regardless of the number of prior lines of therapy), or had received at least 3 prior lines of therapy including an IMiD and a PI. Patients received treatment with melflufen+dexamethasone+daratumumab or daratumumab until documented progressive disease, unacceptable toxicity, or patient/treating physician decision. Patients in the daratumumab treatment arm had the option to receive treatment with melflufen+dexamethasone+daratumumab after confirmed progressive disease. | ||||
| Experiment 300 Reporting the Activity Data of This PDC | [2] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Objective response rate (ORR) |
64% (35-87)
|
|||
| Patients Enrolled |
14 patients no prior ASCT or TTP >36 months after ASCT.
|
||||
| MOA of PDC |
Melphalan flufenamide (melflufen), a first-in-class alkylating peptide-drug conjugate, plus dexamethasone was approved in Europe for use in patients with triple-class refractory relapsed/refractory multiple myeloma (RRMM) with 3 prior lines of therapy and without prior autologous stem cell transplantation (ASCT) or with a time to progression >36 months after prior ASCT. The randomized LIGHTHOUSE study (NCT04649060) assessed melflufen plus daratumumab and dexamethasone (melflufen group) versus daratumumab in patients with RRMM with disease refractory to an immunomodulatory agent and a proteasome inhibitor or who had received 3 prior lines of therapy including an immunomodulatory agent and a proteasome inhibitor. A partial clinical hold issued by the US Food and Drug Administration for all melflufen studies led to financial constraints and premature study closure on February 23rd 2022 (data cut-off date). In total, 54 of 240 planned patients were randomized (melflufen group, N=27; daratumumab group, N=27). Median progression-free survival (PFS) was not reached in the melflufen group versus 4.9 months in the daratumumab group (Hazard Ratio: 0.18 [95% Confidence Interval, 0.05-0.65]; P=0.0032) at a median follow-up time of 7.1 and 6.6 months, respectively. Overall response rate (ORR) was 59% in the melflufen group versus 30% in the daratumumab group (P=0.0300). The most common grade 3 treatment-emergent adverse events in the melflufen group versus daratumumab group were neutropenia (50% vs. 12%), thrombocytopenia (50% vs. 8%), and anemia (32% vs. 19%). Melflufen plus daratumumab and dexamethasone demonstrated superior PFS and ORR versus daratumumab in RRMM and a safety profile comparable to previously published melflufen studies.
Click to Show/Hide
|
||||
| Description |
Efficacy endpoints were more pronounced in favor of the melflufen group compared with the daratumumab group among patients with no prior ASCT or TTP >36 months after a prior ASCT (melflufen group, N=14; daratumumab group, N=15). Median PFS was NR in the melflufen group and 3.9 months (95% CI: 1.4-4.9) in the daratumumab group (HR, 0.06 [95% CI: 0.01-0.49]; log-rank P=0.0005). Fewer OS events were reported in the melflufen group (1 event [7%] vs. 4 events [27%] in the daratumumab group; log-rank P=0.0369). The ORR was 64% (95% CI: 35-87) in the melflufen group and 13% (95% CI: 2-41) in the daratumumab group (P=0.0055). More patients in the melflufen group had a CR (1 patient [7%] vs. 0 patients [0%]) or VGPR (2 patients [14%] vs. 1 patient [7%]) compared with the daratumumab group.
Click to Show/Hide
|
||||
| Related Clinical Trial | |||||
| NCT Number | NCT04649060 | Clinical Status | Phase 3 | ||
| Clinical Description | This was a randomized, controlled, open-label, Phase 3 multicenter study which enrolled patients with Relapsed-Refractory Multiple Myeloma (RRMM) who were either double refractory to an Immunomodulatory Drug (IMiD) and a Proteasome Inhibitor (PI) (regardless of the number of prior lines of therapy), or had received at least 3 prior lines of therapy including an IMiD and a PI. Patients received treatment with melflufen+dexamethasone+daratumumab or daratumumab until documented progressive disease, unacceptable toxicity, or patient/treating physician decision. Patients in the daratumumab treatment arm had the option to receive treatment with melflufen+dexamethasone+daratumumab after confirmed progressive disease. | ||||
| Experiment 301 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Objective response rate (ORR) |
28.60%
|
|||
| Patients Enrolled |
14 patients with relapsed refractory multiple myeloma.
|
||||
| Administration Time | 28-day cycle | ||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (melflufen) is a first-in-class peptide-drug conjugate that utilizes increased peptidase expression to selectively release potent alkylating agents inside tumor cells. Melflufen is hydrolyzed by peptidases and esterases to melphalan either directly or through an intermediate metabolite, desethyl-melflufen. The high lipophilicity of melflufen facilitates passive diffusion across cell membranes. The activity and tolerability of melflufen in relapsed/refractory multiple myeloma (RRMM) were demonstrated in the O-12-M1 (NCT01897714), OCEAN (NCT03151811), and HORIZON (NCT02963493) trials.
Click to Show/Hide
|
||||
| Description |
In Arm A, 4 of the 14 patients achieved an overall response (ORR 28.6% [95% CI: 8.4-58.1]) including 1 patient with CR, and the CBR was 57.1% (95% CI: 28.9-82.3). In Arm B, 1 of the 13 patients achieved an overall response (ORR 7.7% [95% CI: 0.2-36.0]), consisting of a PR, and the CBR was 15.4% (95% CI: 1.9-45.4). In the overall study population, 5 patients had an overall response (ORR 18.5% [95% CI: 6.3-38.1]). DOR data were insufficient to evaluate due to early termination of the study, the low number of patient events (1 in Arm A, 0 in Arm B), and the limited number of responses. Based on the 5 patients who had a response of PR or better at study termination (4 in Arm A, 1 in Arm B), the median TTR was 2.4 months in Arm A, 5.1 months in Arm B, and 2.6 months overall. Based on the 8 and 5 progression events in Arm A and Arm B, respectively, the median TTP was 5.8 months and 4.8 months, respectively, with a median TTP of 5.8 months in the overall population. The median PFS was 5.2 months (95% CI: 2.7 to not evaluable) and 2.9 months (95% CI: 1.5-4.6) in Arms A and B, respectively. For the overall study population, median PFS was 3.7 months (95% CI: 2.7-5.8).
Click to Show/Hide
|
||||
| Half life period | 75.6 h | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT04412707 | Clinical Status | Phase 2 | ||
| Clinical Description | This is a randomized, two-period, cross-over Phase 2 study, comparing PK, and assessing safety and tolerability and efficacy of peripheral and central intravenous administration of melflufen in patients with RRMM. It is an international study, enrolling patients in US and Europe. The study will enroll patients following at least 2 lines of prior therapy. | ||||
| Experiment 302 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Objective response rate (ORR) |
28.60%
|
|||
| Patients Enrolled |
14 patients with relapsed refractory multiple myeloma.
|
||||
| Administration Time | 28-day cycle | ||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (melflufen) is a first-in-class peptide-drug conjugate that utilizes increased peptidase expression to selectively release potent alkylating agents inside tumor cells. Melflufen is hydrolyzed by peptidases and esterases to melphalan either directly or through an intermediate metabolite, desethyl-melflufen. The high lipophilicity of melflufen facilitates passive diffusion across cell membranes. The activity and tolerability of melflufen in relapsed/refractory multiple myeloma (RRMM) were demonstrated in the O-12-M1 (NCT01897714), OCEAN (NCT03151811), and HORIZON (NCT02963493) trials.
Click to Show/Hide
|
||||
| Description |
In Arm A, 4 of the 14 patients achieved an overall response (ORR 28.6% [95% CI: 8.4-58.1]) including 1 patient with CR, and the CBR was 57.1% (95% CI: 28.9-82.3). In Arm B, 1 of the 13 patients achieved an overall response (ORR 7.7% [95% CI: 0.2-36.0]), consisting of a PR, and the CBR was 15.4% (95% CI: 1.9-45.4). In the overall study population, 5 patients had an overall response (ORR 18.5% [95% CI: 6.3-38.1]). DOR data were insufficient to evaluate due to early termination of the study, the low number of patient events (1 in Arm A, 0 in Arm B), and the limited number of responses. Based on the 5 patients who had a response of PR or better at study termination (4 in Arm A, 1 in Arm B), the median TTR was 2.4 months in Arm A, 5.1 months in Arm B, and 2.6 months overall. Based on the 8 and 5 progression events in Arm A and Arm B, respectively, the median TTP was 5.8 months and 4.8 months, respectively, with a median TTP of 5.8 months in the overall population. The median PFS was 5.2 months (95% CI: 2.7 to not evaluable) and 2.9 months (95% CI: 1.5-4.6) in Arms A and B, respectively. For the overall study population, median PFS was 3.7 months (95% CI: 2.7-5.8).
Click to Show/Hide
|
||||
| Half life period | 75.6 h | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT04412707 | Clinical Status | Phase 2 | ||
| Clinical Description | This is a randomized, two-period, cross-over Phase 2 study, comparing PK, and assessing safety and tolerability and efficacy of peripheral and central intravenous administration of melflufen in patients with RRMM. It is an international study, enrolling patients in US and Europe. The study will enroll patients following at least 2 lines of prior therapy. | ||||
| Experiment 303 Reporting the Activity Data of This PDC | [10] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Objective response rate (ORR) |
29% (22-7)
|
|||
| Administration Time | 14 months | ||||
| MOA of PDC |
Melflufen, a highly lipophilic PDC, takes a novel approach by taking advantage of increased aminopeptidase activity to selectively increase the release and concentration of cytotoxic alkylating agents inside of tumor cells. Being highly lipophilic, melflufen does not require active transport, a process that may be defective in cancer cells and contribute to chemoresistance, but instead rapidly enters cells via passive diffusion. The lipophilic nature of melflufen also likely results in its favorable distribution to bone marrow, a fatty tissue, and the physiological component most relevant to MM. Once inside the tumor cells, melflufen is rapidly hydrolyzed by aminopeptidases, enzymes that are found in normal cells but are overexpressed in MM and upon which cancer cells are particularly dependent. This hydrolysis releases potent alkylating agents - most notably melphalan and des-ethyl melflufen - within the cells. Aminopeptidase-driven release of these hydrophilic molecules, which cannot readily diffuse out, thereby results in intracellular trapping. Leveraging high tumor cell aminopeptidase concentrations to rapidly drive intracellular alkylating agent release may provide a safety advantage over alkylators, such as melphalan, which lack such a mechanism for tumor cell targeting, particularly in tumors with an aggressive phenotype.
Click to Show/Hide
|
||||
| Description |
Extensive subgroup analyses have been carried out using O-12-M1 and HORIZON data. In HORIZON, patients with triple-refractory disease and those with disease refractory to anti-CD38 mAbs in the last line had efficacy outcomes similar to those in the overall patient population. Patients with MM refractory to anti-CD38 mAbs in the last line (n = 63) had better response (ORR 35% versus 31%), median PFS (4.6 versus 3.4 months) and OS (15.4 versus 9.3 months) than patients in the MAMMOTH trial treated with conventional chemotherapy (n = 275). Baseline characteristics were similar in these two trials, except that in HORIZON, patients were more heavily pretreated (median 5 versus 4 therapies). Among patients in HORIZON whose disease was alkylator-refractory in any prior line (n = 92), the ORR was 21% and median PFS was 3.8 months. None of the seven patients with melphalan-refractory disease, however, had an objective response by independent review. This contrasts with the 44% ORR observed in nine patients with melphalan-refractory disease in O-12-M1. All seven patients in HORIZON, however, were at least triple-class refractory, and none had achieved a CR in any prior line.
Click to Show/Hide
|
||||
| Related Clinical Trial | |||||
| NCT Number | NCT02963493 | Clinical Status | Phase 2 | ||
| Clinical Description | This study will evaluate melflufen in combination with dexamethasone in adult patients with relapsed or refractory multiple myeloma in whose disease is refractory to pomalidomide and/or an anti-CD38 monoclonal antibody. All patients in the study will be treated with melflufen on Day 1 and dexamethasone on Days 1, 8, 15 and 22 of each 28-day cycle. | ||||
| Experiment 304 Reporting the Activity Data of This PDC | [7] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Objective response rate (ORR) |
8%
|
|||
| Administration Time | Iv infusion of 40 mg melflufen on day 1 of each 28-day treatment cycle | ||||
| Administration Dosage | Melflufen 40 mg (Single Agent) | ||||
| MOA of PDC |
The antineoplastic activity of melflufen is dependent upon the expression of aminopeptidases, like APN (also known as CD18), which cleave melflufen into melphalan and p-Fluorophenylalanine. Following aminopeptidase-dependent cleavage, the hydrophilic alkylating metabolite melphalan accumulates in myeloma cells. This enrichment of the cytotoxic payload has a substantial impact on the antimyeloma activity of melflufen.
Click to Show/Hide
|
||||
| Description |
In the phase 2 single-agent cohort, the overall response rate was 8% (one of 13 patients; 02-360) and the clinical benefit rate was 23% (three of 13; 5-54).
|
||||
| In Vivo Model | Aged 18 years or older, had relapsed and refractory multiple myeloma, had received two or more previous lines of therapy (including lenalidomide and bortezomib). | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT01897714 | Clinical Status | Phase 1/2 | ||
| Clinical Description | The study will explore escalating doses of melflufen in combination with dexamethasone in small groups of patients to find the maximum tolerated dose of melflufen. That dose will then be used to determine the efficacy and safety profile of melflufen in combination with dexamethasone in a larger group of patients. | ||||
| Experiment 305 Reporting the Activity Data of This PDC | [7] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Objective response rate (ORR) |
31%
|
|||
| Administration Time | Iv infusion of 40 mg melflufen on day 1 of each 21-day or 28-day treatment cycles, in combination with 40 mg dexamet hasone (oral or iv) on days 1, 8 and 15 of each 21-day treatment cycles. for any patients on the 28-day treatment sc hedule, an additional dose of 40 mg dexamet hasone was administered on day 22 of each treatment cycle | ||||
| Administration Dosage | Melflufen 40 mg + Dexamethasone | ||||
| MOA of PDC |
The antineoplastic activity of melflufen is dependent upon the expression of aminopeptidases, like APN (also known as CD18), which cleave melflufen into melphalan and p-Fluorophenylalanine. Following aminopeptidase-dependent cleavage, the hydrophilic alkylating metabolite melphalan accumulates in myeloma cells. This enrichment of the cytotoxic payload has a substantial impact on the antimyeloma activity of melflufen.
Click to Show/Hide
|
||||
| Description |
In phase 2, patients treated with combination therapy achieved an overall response rate of 31% (14 of 45 patients; 95% CI 18-47) and clinical benefit rate of 49% (22 of 45; 34-64)
|
||||
| In Vivo Model | Aged 18 years or older, had relapsed and refractory multiple myeloma, had received two or more previous lines of therapy (including lenalidomide and bortezomib). | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT01897714 | Clinical Status | Phase 1/2 | ||
| Clinical Description | The study will explore escalating doses of melflufen in combination with dexamethasone in small groups of patients to find the maximum tolerated dose of melflufen. That dose will then be used to determine the efficacy and safety profile of melflufen in combination with dexamethasone in a larger group of patients. | ||||
| Experiment 306 Reporting the Activity Data of This PDC | [10] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Objective response rate (ORR) |
31% (18-7)
|
|||
| Patients Enrolled |
Patients with multiple myeloma.
|
||||
| Administration Time | 27.9 months | ||||
| MOA of PDC |
Melflufen, a highly lipophilic PDC, takes a novel approach by taking advantage of increased aminopeptidase activity to selectively increase the release and concentration of cytotoxic alkylating agents inside of tumor cells. Being highly lipophilic, melflufen does not require active transport, a process that may be defective in cancer cells and contribute to chemoresistance, but instead rapidly enters cells via passive diffusion. The lipophilic nature of melflufen also likely results in its favorable distribution to bone marrow, a fatty tissue, and the physiological component most relevant to MM. Once inside the tumor cells, melflufen is rapidly hydrolyzed by aminopeptidases, enzymes that are found in normal cells but are overexpressed in MM and upon which cancer cells are particularly dependent. This hydrolysis releases potent alkylating agents - most notably melphalan and des-ethyl melflufen - within the cells. Aminopeptidase-driven release of these hydrophilic molecules, which cannot readily diffuse out, thereby results in intracellular trapping. Leveraging high tumor cell aminopeptidase concentrations to rapidly drive intracellular alkylating agent release may provide a safety advantage over alkylators, such as melphalan, which lack such a mechanism for tumor cell targeting, particularly in tumors with an aggressive phenotype.
Click to Show/Hide
|
||||
| Description |
Forty-five patients received melflufen plus dexamethasone in the phase II portion of the study. The median age was 66 years, 67% were male, the median prior therapies were 4 (range, 3-5), 67% were double refractory (PI and IMiD), 58% had received previous ASCT, 20% had International Staging System (ISS) stage 3 disease, and 44% had high-risk cytogenetics. At a median follow-up time of 27.9 months, the ORR in this cohort was 31% (95% CI: 18-47), including 11% very good partial response (VGPR). No complete responses (CRs) occurred. Interestingly, among patients whose disease was refractory to melphalan in any prior line, the ORR was 44%. The CBR was 49% (95% CI: 34-64), the median duration of response (DOR) was 8.4 months (95% CI: 4.6-9.6), and median PFS was 5.7 months (95% CI: 3.7-9.2). A recently published longer term data analysis reported that at a median 46-month follow-up, the median overall survival (OS) was 20.7 months (95% CI: 11.8-41.3).
Click to Show/Hide
|
||||
| Related Clinical Trial | |||||
| NCT Number | NCT01897714 | Clinical Status | Phase 1/2 | ||
| Clinical Description | The study will explore escalating doses of melflufen in combination with dexamethasone in small groups of patients to find the maximum tolerated dose of melflufen. That dose will then be used to determine the efficacy and safety profile of melflufen in combination with dexamethasone in a larger group of patients. | ||||
| Experiment 307 Reporting the Activity Data of This PDC | [10] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Objective response rate (ORR) |
70%
|
|||
| Administration Time | 11.9 months | ||||
| MOA of PDC |
Melflufen, a highly lipophilic PDC, takes a novel approach by taking advantage of increased aminopeptidase activity to selectively increase the release and concentration of cytotoxic alkylating agents inside of tumor cells. Being highly lipophilic, melflufen does not require active transport, a process that may be defective in cancer cells and contribute to chemoresistance, but instead rapidly enters cells via passive diffusion. The lipophilic nature of melflufen also likely results in its favorable distribution to bone marrow, a fatty tissue, and the physiological component most relevant to MM. Once inside the tumor cells, melflufen is rapidly hydrolyzed by aminopeptidases, enzymes that are found in normal cells but are overexpressed in MM and upon which cancer cells are particularly dependent. This hydrolysis releases potent alkylating agents - most notably melphalan and des-ethyl melflufen - within the cells. Aminopeptidase-driven release of these hydrophilic molecules, which cannot readily diffuse out, thereby results in intracellular trapping. Leveraging high tumor cell aminopeptidase concentrations to rapidly drive intracellular alkylating agent release may provide a safety advantage over alkylators, such as melphalan, which lack such a mechanism for tumor cell targeting, particularly in tumors with an aggressive phenotype.
Click to Show/Hide
|
||||
| Description |
Results for 33 patients in the melflufen/daratumumab/dexamethasone arm and 10 in the melflufen/bortezomib/dexamethasone arm have been previously reported. Patients in the daratumumab-containing arm had a median age of 64, and a median of two prior therapies. High-risk cytogenetics were present in 42%, and 61% were refractory to their last therapy. At a median treatment duration of 8.4 months, the ORR was 70%, consisting of one sCR, one CR, and ten VGPRs, and median PFS was 11.5 months. No DLTS were reported, and the most common grade ≥3 treatment-related AEs were neutropenia (58%) and thrombocytopenia (55%). There were two fatal AEs (myeloma progression and sepsis; general physical health deterioration) of which sepsis was considered treatment related. In the melflufen/bortezomib/dexamethasone arm, the median age was 71 years, and patients had a median
Click to Show/Hide
|
||||
| Related Clinical Trial | |||||
| NCT Number | NCT03481556 | Clinical Status | Phase 1/2 | ||
| Clinical Description | This is an open-label Phase 1/2a study which will enroll patients that have relapsed or relapsed-refractory multiple myeloma to combination regimens of melflufen with currently approved agents. Patients will receive either melflufen+dexamethasone+bortezomib or melflufen+dexamethasone+daratumumab. | ||||
| Experiment 308 Reporting the Activity Data of This PDC | [4] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Overall response rate (ORR) |
8.00%
|
|||
| Patients Enrolled |
81 patients with multiple myeloma.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melflufen is a first-in-class peptide-drug conjugate, targeting aminopeptidase which has an increased expression in fast-growing and aggressive malignancies. The lipophilicity of melflufen allows for passive diffusion, selectively targeting myeloma cells. Once inside the cell, melflufen is hydrolyzed to active alkylating metabolites melphalan and desethyl-melflufen. Melflufen and the active metabolites trigger irreversible DNA damage, inhibit proliferation, induces apoptosis, and express antiangiogenic effects. In addition, melflufen demonstrated activity in myeloma cells with documented impaired or absent Tp53 expression and documented resistance to bortezomib, dexamethasone, and melphalan.
Click to Show/Hide
|
||||
| Description |
The phase I arm established 40 mg of melflufen as the maximum tolerated dose in combination with dexamethasone. The phase II arm found an overall response rate (ORR) of 31% (14 patients) and clinical benefit rate, defined as first occurrence of disease response including minimal response or better, of 49% (22 patients) in the melflufen and dexamethasone group compared with an ORR of 8% (1 patient) and clinical benefit rate of 23% (3 patients) in the melflufen group. Based on these findings, melflufen 40 mg plus dexamethasone 40 mg was deemed a feasible treatment regimen for relapsed and refractory multiple myeloma and appropriate to proceed to a larger phase II trial.
Click to Show/Hide
|
||||
| Experiment 309 Reporting the Activity Data of This PDC | [4] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Overall response rate (ORR) |
26%
|
|||
| Patients Enrolled |
Patients with triple-class refractory disease group multiple myeloma.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melflufen is a first-in-class peptide-drug conjugate, targeting aminopeptidase which has an increased expression in fast-growing and aggressive malignancies. The lipophilicity of melflufen allows for passive diffusion, selectively targeting myeloma cells. Once inside the cell, melflufen is hydrolyzed to active alkylating metabolites melphalan and desethyl-melflufen. Melflufen and the active metabolites trigger irreversible DNA damage, inhibit proliferation, induces apoptosis, and express antiangiogenic effects. In addition, melflufen demonstrated activity in myeloma cells with documented impaired or absent Tp53 expression and documented resistance to bortezomib, dexamethasone, and melphalan.
Click to Show/Hide
|
||||
| Description |
The primary outcome of the study was ORR, defined based on the International Myeloma Working Group (IMWG) uniform response criteria. Investigators included a preplanned subgroup analysis in patients with triple-class refractory disease defined as refractory to at least 1 immunomodulator, 1 proteosome inhibitor, and 1 anti-CD38 antibody. From December 28, 2016, to October 14, 2019, investigators enrolled 157 patients across 17 sites that received at least 1 dose of melflufen. Patient baseline demographics included median age of 65 years old, an average of 5 previous lines of therapy, and 98% of patients were refractory to their previous line of therapy. A total of 131 patients (83%) discontinued treatment due to either disease progression or adverse effects. The median ORR was 29% (22%-37%) for the all treatment group and 26% (18%-35%) in the triple-class refractory disease group. The median duration of at least partial response or better was 5.5 months (3.9-7.6 months) in the all treatment group and 4.4 months (3.4-7.6 months) in the triple-class refractory disease group. Median overall survival (OS) was 11.6 months (9.3-15.4 months) in the all treatment group and 16.5 months (11.5-18.5 months) in the triple-class refractory group.
Click to Show/Hide
|
||||
| Experiment 310 Reporting the Activity Data of This PDC | [4] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Overall response rate (ORR) |
29.00%
|
|||
| Patients Enrolled |
157 patients with multiple myeloma.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melflufen is a first-in-class peptide-drug conjugate, targeting aminopeptidase which has an increased expression in fast-growing and aggressive malignancies. The lipophilicity of melflufen allows for passive diffusion, selectively targeting myeloma cells. Once inside the cell, melflufen is hydrolyzed to active alkylating metabolites melphalan and desethyl-melflufen. Melflufen and the active metabolites trigger irreversible DNA damage, inhibit proliferation, induces apoptosis, and express antiangiogenic effects. In addition, melflufen demonstrated activity in myeloma cells with documented impaired or absent Tp53 expression and documented resistance to bortezomib, dexamethasone, and melphalan.
Click to Show/Hide
|
||||
| Description |
The primary outcome of the study was ORR, defined based on the International Myeloma Working Group (IMWG) uniform response criteria. Investigators included a preplanned subgroup analysis in patients with triple-class refractory disease defined as refractory to at least 1 immunomodulator, 1 proteosome inhibitor, and 1 anti-CD38 antibody. From December 28, 2016, to October 14, 2019, investigators enrolled 157 patients across 17 sites that received at least 1 dose of melflufen. Patient baseline demographics included median age of 65 years old, an average of 5 previous lines of therapy, and 98% of patients were refractory to their previous line of therapy. A total of 131 patients (83%) discontinued treatment due to either disease progression or adverse effects. The median ORR was 29% (22%-37%) for the all treatment group and 26% (18%-35%) in the triple-class refractory disease group. The median duration of at least partial response or better was 5.5 months (3.9-7.6 months) in the all treatment group and 4.4 months (3.4-7.6 months) in the triple-class refractory disease group. Median overall survival (OS) was 11.6 months (9.3-15.4 months) in the all treatment group and 16.5 months (11.5-18.5 months) in the triple-class refractory group.
Click to Show/Hide
|
||||
| Experiment 311 Reporting the Activity Data of This PDC | [1] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Overall response rate (ORR) |
8.00%
|
|||
| Patients Enrolled |
Patients with multi-refractory multiple myeloma.
|
||||
| MOA of PDC |
Melflufen is highly lipophilic, which promotes its rapid uptake by cells. Once within the cell, melflufen releases its hydrophilic alkylator payloads via the hydrolytic activity of intracellular peptidases (e.g., aminopeptidases). Aminopeptidases are Zn2+-dependent metalloproteinases that remove amino acids at the N-terminal position from oligopeptides and have been associated with multiple tumorigenic processes such as proliferation, apoptosis, differentiation, angiogenesis, and motility. The dependence of melflufen on aminopeptidases was initially demonstrated by the reduced cytotoxic activity of melflufen-but not the alkylator melphalan-when cells were pretreated with bestatin, an antibiotic that is a potent aminopeptidase inhibitor. In addition, structure analogs designed to resist peptide hydrolysis (N-methyl derivative and derivative with D-amino acid) were shown to be almost 100-fold less potent than melflufen. Subsequent in vitro studies demonstrated that hydrolytic cleavage of melflufen by aminopeptidases releases alkylator payloads, including melphalan. In vitro, the activity of melflufen is multi-pronged, including induction of DNA damage, induction of apoptosis, inhibition of VEGF-dependent cell migration, and inhibition of tumor-associated angiogenesis, which have been further reviewed elsewhere. Downregulation of aminopeptidases resulted in reduced melflufen-mediated cytotoxic activity and apoptotic signaling in cultured cells.
Click to Show/Hide
|
||||
| Description |
Among the 13 patients who received single-agent melflufen, the median number of prior therapies was 5 (range, 4-8), the ORR was 8% (1 PR), median PFS was 4.4 months, and median OS was 15.5 months.
|
||||
| Experiment 312 Reporting the Activity Data of This PDC | [1] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Overall response rate (ORR) |
21.00%
|
|||
| Patients Enrolled |
Patients with high-risk cytogenetics.
|
||||
| MOA of PDC |
Melflufen is highly lipophilic, which promotes its rapid uptake by cells. Once within the cell, melflufen releases its hydrophilic alkylator payloads via the hydrolytic activity of intracellular peptidases (e.g., aminopeptidases). Aminopeptidases are Zn2+-dependent metalloproteinases that remove amino acids at the N-terminal position from oligopeptides and have been associated with multiple tumorigenic processes such as proliferation, apoptosis, differentiation, angiogenesis, and motility. The dependence of melflufen on aminopeptidases was initially demonstrated by the reduced cytotoxic activity of melflufen-but not the alkylator melphalan-when cells were pretreated with bestatin, an antibiotic that is a potent aminopeptidase inhibitor. In addition, structure analogs designed to resist peptide hydrolysis (N-methyl derivative and derivative with D-amino acid) were shown to be almost 100-fold less potent than melflufen. Subsequent in vitro studies demonstrated that hydrolytic cleavage of melflufen by aminopeptidases releases alkylator payloads, including melphalan. In vitro, the activity of melflufen is multi-pronged, including induction of DNA damage, induction of apoptosis, inhibition of VEGF-dependent cell migration, and inhibition of tumor-associated angiogenesis, which have been further reviewed elsewhere. Downregulation of aminopeptidases resulted in reduced melflufen-mediated cytotoxic activity and apoptotic signaling in cultured cells.
Click to Show/Hide
|
||||
| Description |
Among 125 patients evaluable for response, the ORR (≥PR) was 29%, with 1 patient achieving a stringent complete response (CR) and 10 patients achieving a VGPR. The median duration of response was 4.4 months. The ORR was 21% among 47 patients with high-risk cytogenetics, 24% among 93 patients with triple-class refractory disease, and 24% among 42 patients with extramedullary disease.
Click to Show/Hide
|
||||
| Experiment 313 Reporting the Activity Data of This PDC | [1] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Overall response rate (ORR) |
24.00%
|
|||
| Patients Enrolled |
Patients with triple-class refractory disease.
|
||||
| MOA of PDC |
Melflufen is highly lipophilic, which promotes its rapid uptake by cells. Once within the cell, melflufen releases its hydrophilic alkylator payloads via the hydrolytic activity of intracellular peptidases (e.g., aminopeptidases). Aminopeptidases are Zn2+-dependent metalloproteinases that remove amino acids at the N-terminal position from oligopeptides and have been associated with multiple tumorigenic processes such as proliferation, apoptosis, differentiation, angiogenesis, and motility. The dependence of melflufen on aminopeptidases was initially demonstrated by the reduced cytotoxic activity of melflufen-but not the alkylator melphalan-when cells were pretreated with bestatin, an antibiotic that is a potent aminopeptidase inhibitor. In addition, structure analogs designed to resist peptide hydrolysis (N-methyl derivative and derivative with D-amino acid) were shown to be almost 100-fold less potent than melflufen. Subsequent in vitro studies demonstrated that hydrolytic cleavage of melflufen by aminopeptidases releases alkylator payloads, including melphalan. In vitro, the activity of melflufen is multi-pronged, including induction of DNA damage, induction of apoptosis, inhibition of VEGF-dependent cell migration, and inhibition of tumor-associated angiogenesis, which have been further reviewed elsewhere. Downregulation of aminopeptidases resulted in reduced melflufen-mediated cytotoxic activity and apoptotic signaling in cultured cells.
Click to Show/Hide
|
||||
| Description |
Among 125 patients evaluable for response, the ORR (≥PR) was 29%, with 1 patient achieving a stringent complete response (CR) and 10 patients achieving a VGPR. The median duration of response was 4.4 months. The ORR was 21% among 47 patients with high-risk cytogenetics, 24% among 93 patients with triple-class refractory disease, and 24% among 42 patients with extramedullary disease.
Click to Show/Hide
|
||||
| Experiment 314 Reporting the Activity Data of This PDC | [1] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Overall response rate (ORR) |
24.00%
|
|||
| Patients Enrolled |
Patients with extramedullary disease.
|
||||
| MOA of PDC |
Melflufen is highly lipophilic, which promotes its rapid uptake by cells. Once within the cell, melflufen releases its hydrophilic alkylator payloads via the hydrolytic activity of intracellular peptidases (e.g., aminopeptidases). Aminopeptidases are Zn2+-dependent metalloproteinases that remove amino acids at the N-terminal position from oligopeptides and have been associated with multiple tumorigenic processes such as proliferation, apoptosis, differentiation, angiogenesis, and motility. The dependence of melflufen on aminopeptidases was initially demonstrated by the reduced cytotoxic activity of melflufen-but not the alkylator melphalan-when cells were pretreated with bestatin, an antibiotic that is a potent aminopeptidase inhibitor. In addition, structure analogs designed to resist peptide hydrolysis (N-methyl derivative and derivative with D-amino acid) were shown to be almost 100-fold less potent than melflufen. Subsequent in vitro studies demonstrated that hydrolytic cleavage of melflufen by aminopeptidases releases alkylator payloads, including melphalan. In vitro, the activity of melflufen is multi-pronged, including induction of DNA damage, induction of apoptosis, inhibition of VEGF-dependent cell migration, and inhibition of tumor-associated angiogenesis, which have been further reviewed elsewhere. Downregulation of aminopeptidases resulted in reduced melflufen-mediated cytotoxic activity and apoptotic signaling in cultured cells.
Click to Show/Hide
|
||||
| Description |
Among 125 patients evaluable for response, the ORR (≥PR) was 29%, with 1 patient achieving a stringent complete response (CR) and 10 patients achieving a VGPR. The median duration of response was 4.4 months. The ORR was 21% among 47 patients with high-risk cytogenetics, 24% among 93 patients with triple-class refractory disease, and 24% among 42 patients with extramedullary disease.
Click to Show/Hide
|
||||
| Experiment 315 Reporting the Activity Data of This PDC | [1] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Overall response rate (ORR) |
29.00%
|
|||
| Patients Enrolled |
Patients with multi-refractory multiple myeloma.
|
||||
| Administration Time | 14.3 week (median) | ||||
| Administration Dosage | 40 mg with dexamethasone (40 mg) | ||||
| MOA of PDC |
Melflufen is highly lipophilic, which promotes its rapid uptake by cells. Once within the cell, melflufen releases its hydrophilic alkylator payloads via the hydrolytic activity of intracellular peptidases (e.g., aminopeptidases). Aminopeptidases are Zn2+-dependent metalloproteinases that remove amino acids at the N-terminal position from oligopeptides and have been associated with multiple tumorigenic processes such as proliferation, apoptosis, differentiation, angiogenesis, and motility. The dependence of melflufen on aminopeptidases was initially demonstrated by the reduced cytotoxic activity of melflufen-but not the alkylator melphalan-when cells were pretreated with bestatin, an antibiotic that is a potent aminopeptidase inhibitor. In addition, structure analogs designed to resist peptide hydrolysis (N-methyl derivative and derivative with D-amino acid) were shown to be almost 100-fold less potent than melflufen. Subsequent in vitro studies demonstrated that hydrolytic cleavage of melflufen by aminopeptidases releases alkylator payloads, including melphalan. In vitro, the activity of melflufen is multi-pronged, including induction of DNA damage, induction of apoptosis, inhibition of VEGF-dependent cell migration, and inhibition of tumor-associated angiogenesis, which have been further reviewed elsewhere. Downregulation of aminopeptidases resulted in reduced melflufen-mediated cytotoxic activity and apoptotic signaling in cultured cells.
Click to Show/Hide
|
||||
| Experiment 316 Reporting the Activity Data of This PDC | [1] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Overall response rate (ORR) |
29.00%
|
|||
| Patients Enrolled |
Patients evaluable for response.
|
||||
| MOA of PDC |
Melflufen is highly lipophilic, which promotes its rapid uptake by cells. Once within the cell, melflufen releases its hydrophilic alkylator payloads via the hydrolytic activity of intracellular peptidases (e.g., aminopeptidases). Aminopeptidases are Zn2+-dependent metalloproteinases that remove amino acids at the N-terminal position from oligopeptides and have been associated with multiple tumorigenic processes such as proliferation, apoptosis, differentiation, angiogenesis, and motility. The dependence of melflufen on aminopeptidases was initially demonstrated by the reduced cytotoxic activity of melflufen-but not the alkylator melphalan-when cells were pretreated with bestatin, an antibiotic that is a potent aminopeptidase inhibitor. In addition, structure analogs designed to resist peptide hydrolysis (N-methyl derivative and derivative with D-amino acid) were shown to be almost 100-fold less potent than melflufen. Subsequent in vitro studies demonstrated that hydrolytic cleavage of melflufen by aminopeptidases releases alkylator payloads, including melphalan. In vitro, the activity of melflufen is multi-pronged, including induction of DNA damage, induction of apoptosis, inhibition of VEGF-dependent cell migration, and inhibition of tumor-associated angiogenesis, which have been further reviewed elsewhere. Downregulation of aminopeptidases resulted in reduced melflufen-mediated cytotoxic activity and apoptotic signaling in cultured cells.
Click to Show/Hide
|
||||
| Description |
Among 125 patients evaluable for response, the ORR (≥PR) was 29%, with 1 patient achieving a stringent complete response (CR) and 10 patients achieving a VGPR. The median duration of response was 4.4 months. The ORR was 21% among 47 patients with high-risk cytogenetics, 24% among 93 patients with triple-class refractory disease, and 24% among 42 patients with extramedullary disease.
Click to Show/Hide
|
||||
| Experiment 317 Reporting the Activity Data of This PDC | [1] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Overall response rate (ORR) |
31.00%
|
|||
| Patients Enrolled |
Patients with multi-refractory multiple myeloma.
|
||||
| Administration Time | 28-day cycle | ||||
| Administration Dosage | 40 mg with dexamethasone (40 mg) | ||||
| MOA of PDC |
Melflufen is highly lipophilic, which promotes its rapid uptake by cells. Once within the cell, melflufen releases its hydrophilic alkylator payloads via the hydrolytic activity of intracellular peptidases (e.g., aminopeptidases). Aminopeptidases are Zn2+-dependent metalloproteinases that remove amino acids at the N-terminal position from oligopeptides and have been associated with multiple tumorigenic processes such as proliferation, apoptosis, differentiation, angiogenesis, and motility. The dependence of melflufen on aminopeptidases was initially demonstrated by the reduced cytotoxic activity of melflufen-but not the alkylator melphalan-when cells were pretreated with bestatin, an antibiotic that is a potent aminopeptidase inhibitor. In addition, structure analogs designed to resist peptide hydrolysis (N-methyl derivative and derivative with D-amino acid) were shown to be almost 100-fold less potent than melflufen. Subsequent in vitro studies demonstrated that hydrolytic cleavage of melflufen by aminopeptidases releases alkylator payloads, including melphalan. In vitro, the activity of melflufen is multi-pronged, including induction of DNA damage, induction of apoptosis, inhibition of VEGF-dependent cell migration, and inhibition of tumor-associated angiogenesis, which have been further reviewed elsewhere. Downregulation of aminopeptidases resulted in reduced melflufen-mediated cytotoxic activity and apoptotic signaling in cultured cells.
Click to Show/Hide
|
||||
| Experiment 318 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Overall response rate (ORR) |
32.00%
|
|||
| Patients Enrolled |
246 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 319 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Overall response rate (ORR) |
33.00%
|
|||
| Patients Enrolled |
246 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 320 Reporting the Activity Data of This PDC | [1] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Overall response rate (ORR) |
67%
|
|||
| Patients Enrolled |
Patients with multi-refractory multiple myeloma.
|
||||
| Administration Time | 9.3 month (median) | ||||
| Administration Dosage | 30 or 40 mg | ||||
| MOA of PDC |
Melflufen is highly lipophilic, which promotes its rapid uptake by cells. Once within the cell, melflufen releases its hydrophilic alkylator payloads via the hydrolytic activity of intracellular peptidases (e.g., aminopeptidases). Aminopeptidases are Zn2+-dependent metalloproteinases that remove amino acids at the N-terminal position from oligopeptides and have been associated with multiple tumorigenic processes such as proliferation, apoptosis, differentiation, angiogenesis, and motility. The dependence of melflufen on aminopeptidases was initially demonstrated by the reduced cytotoxic activity of melflufen-but not the alkylator melphalan-when cells were pretreated with bestatin, an antibiotic that is a potent aminopeptidase inhibitor. In addition, structure analogs designed to resist peptide hydrolysis (N-methyl derivative and derivative with D-amino acid) were shown to be almost 100-fold less potent than melflufen. Subsequent in vitro studies demonstrated that hydrolytic cleavage of melflufen by aminopeptidases releases alkylator payloads, including melphalan. In vitro, the activity of melflufen is multi-pronged, including induction of DNA damage, induction of apoptosis, inhibition of VEGF-dependent cell migration, and inhibition of tumor-associated angiogenesis, which have been further reviewed elsewhere. Downregulation of aminopeptidases resulted in reduced melflufen-mediated cytotoxic activity and apoptotic signaling in cultured cells.
Click to Show/Hide
|
||||
| Experiment 321 Reporting the Activity Data of This PDC | [1] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Overall response rate (ORR) |
76.00%
|
|||
| Patients Enrolled |
Patients with multi-refractory multiple myeloma.
|
||||
| Administration Time | 6.2 month (median) | ||||
| Administration Dosage | 30 or 40 mg | ||||
| MOA of PDC |
Melflufen is highly lipophilic, which promotes its rapid uptake by cells. Once within the cell, melflufen releases its hydrophilic alkylator payloads via the hydrolytic activity of intracellular peptidases (e.g., aminopeptidases). Aminopeptidases are Zn2+-dependent metalloproteinases that remove amino acids at the N-terminal position from oligopeptides and have been associated with multiple tumorigenic processes such as proliferation, apoptosis, differentiation, angiogenesis, and motility. The dependence of melflufen on aminopeptidases was initially demonstrated by the reduced cytotoxic activity of melflufen-but not the alkylator melphalan-when cells were pretreated with bestatin, an antibiotic that is a potent aminopeptidase inhibitor. In addition, structure analogs designed to resist peptide hydrolysis (N-methyl derivative and derivative with D-amino acid) were shown to be almost 100-fold less potent than melflufen. Subsequent in vitro studies demonstrated that hydrolytic cleavage of melflufen by aminopeptidases releases alkylator payloads, including melphalan. In vitro, the activity of melflufen is multi-pronged, including induction of DNA damage, induction of apoptosis, inhibition of VEGF-dependent cell migration, and inhibition of tumor-associated angiogenesis, which have been further reviewed elsewhere. Downregulation of aminopeptidases resulted in reduced melflufen-mediated cytotoxic activity and apoptotic signaling in cultured cells.
Click to Show/Hide
|
||||
| Experiment 322 Reporting the Activity Data of This PDC | [2] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Partial response (PR) |
11%
|
|||
| MOA of PDC |
Melphalan flufenamide (melflufen), a first-in-class alkylating peptide-drug conjugate, plus dexamethasone was approved in Europe for use in patients with triple-class refractory relapsed/refractory multiple myeloma (RRMM) with 3 prior lines of therapy and without prior autologous stem cell transplantation (ASCT) or with a time to progression >36 months after prior ASCT. The randomized LIGHTHOUSE study (NCT04649060) assessed melflufen plus daratumumab and dexamethasone (melflufen group) versus daratumumab in patients with RRMM with disease refractory to an immunomodulatory agent and a proteasome inhibitor or who had received 3 prior lines of therapy including an immunomodulatory agent and a proteasome inhibitor. A partial clinical hold issued by the US Food and Drug Administration for all melflufen studies led to financial constraints and premature study closure on February 23rd 2022 (data cut-off date). In total, 54 of 240 planned patients were randomized (melflufen group, N=27; daratumumab group, N=27). Median progression-free survival (PFS) was not reached in the melflufen group versus 4.9 months in the daratumumab group (Hazard Ratio: 0.18 [95% Confidence Interval, 0.05-0.65]; P=0.0032) at a median follow-up time of 7.1 and 6.6 months, respectively. Overall response rate (ORR) was 59% in the melflufen group versus 30% in the daratumumab group (P=0.0300). The most common grade 3 treatment-emergent adverse events in the melflufen group versus daratumumab group were neutropenia (50% vs. 12%), thrombocytopenia (50% vs. 8%), and anemia (32% vs. 19%). Melflufen plus daratumumab and dexamethasone demonstrated superior PFS and ORR versus daratumumab in RRMM and a safety profile comparable to previously published melflufen studies.
Click to Show/Hide
|
||||
| Description |
In the ITT population, with a median follow-up of 7.1 months in the melflufen group, the median PFS was not reached (NR) and with a median follow-up of 6.6 months in the daratumumab group, the median PFS was 4.9 months (95% CI: 3.4-NR; HR: 0.18 [95% CI: 0.05-0.65]; log-rankP=0.0032). OS was immature, with 2 events (7%) in the melflufen group and 4 events (15%) in the daratumumab group (HR: 0.47 [95% CI: 0.09-2.57]; log-rankP=0.3721) at a median follow-up of 7.6 months and 6.6 months, respectively. The ORR was 59% (95% CI: 39-78) in the melflufen group and 30% (95% CI: 14-50) in the daratumumab group (P=0.0300). More patients in the melflufen group had a complete response (CR; 1 patient [4%]vs. 0 patients [0%]) and very good partial response (VGPR; 4 patients [15%]vs. 3 patients [11%]) compared with the daratumumab group.
Click to Show/Hide
|
||||
| In Vivo Model | 27 Intent-to-treat (ITT) population. | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT04649060 | Clinical Status | Phase 3 | ||
| Clinical Description | This was a randomized, controlled, open-label, Phase 3 multicenter study which enrolled patients with Relapsed-Refractory Multiple Myeloma (RRMM) who were either double refractory to an Immunomodulatory Drug (IMiD) and a Proteasome Inhibitor (PI) (regardless of the number of prior lines of therapy), or had received at least 3 prior lines of therapy including an IMiD and a PI. Patients received treatment with melflufen+dexamethasone+daratumumab or daratumumab until documented progressive disease, unacceptable toxicity, or patient/treating physician decision. Patients in the daratumumab treatment arm had the option to receive treatment with melflufen+dexamethasone+daratumumab after confirmed progressive disease. | ||||
| Experiment 323 Reporting the Activity Data of This PDC | [2] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Partial response (PR) |
11%
|
|||
| MOA of PDC |
Melphalan flufenamide (melflufen), a first-in-class alkylating peptide-drug conjugate, plus dexamethasone was approved in Europe for use in patients with triple-class refractory relapsed/refractory multiple myeloma (RRMM) with 3 prior lines of therapy and without prior autologous stem cell transplantation (ASCT) or with a time to progression >36 months after prior ASCT. The randomized LIGHTHOUSE study (NCT04649060) assessed melflufen plus daratumumab and dexamethasone (melflufen group) versus daratumumab in patients with RRMM with disease refractory to an immunomodulatory agent and a proteasome inhibitor or who had received 3 prior lines of therapy including an immunomodulatory agent and a proteasome inhibitor. A partial clinical hold issued by the US Food and Drug Administration for all melflufen studies led to financial constraints and premature study closure on February 23rd 2022 (data cut-off date). In total, 54 of 240 planned patients were randomized (melflufen group, N=27; daratumumab group, N=27). Median progression-free survival (PFS) was not reached in the melflufen group versus 4.9 months in the daratumumab group (Hazard Ratio: 0.18 [95% Confidence Interval, 0.05-0.65]; P=0.0032) at a median follow-up time of 7.1 and 6.6 months, respectively. Overall response rate (ORR) was 59% in the melflufen group versus 30% in the daratumumab group (P=0.0300). The most common grade 3 treatment-emergent adverse events in the melflufen group versus daratumumab group were neutropenia (50% vs. 12%), thrombocytopenia (50% vs. 8%), and anemia (32% vs. 19%). Melflufen plus daratumumab and dexamethasone demonstrated superior PFS and ORR versus daratumumab in RRMM and a safety profile comparable to previously published melflufen studies.
Click to Show/Hide
|
||||
| Description |
In the ITT population, with a median follow-up of 7.1 months in the melflufen group, the median PFS was not reached (NR) and with a median follow-up of 6.6 months in the daratumumab group, the median PFS was 4.9 months (95% CI: 3.4-NR; HR: 0.18 [95% CI: 0.05-0.65]; log-rankP=0.0032). OS was immature, with 2 events (7%) in the melflufen group and 4 events (15%) in the daratumumab group (HR: 0.47 [95% CI: 0.09-2.57]; log-rankP=0.3721) at a median follow-up of 7.6 months and 6.6 months, respectively. The ORR was 59% (95% CI: 39-78) in the melflufen group and 30% (95% CI: 14-50) in the daratumumab group (P=0.0300). More patients in the melflufen group had a complete response (CR; 1 patient [4%]vs. 0 patients [0%]) and very good partial response (VGPR; 4 patients [15%]vs. 3 patients [11%]) compared with the daratumumab group.
Click to Show/Hide
|
||||
| In Vivo Model | 27 Intent-to-treat (ITT) population. | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT04649060 | Clinical Status | Phase 3 | ||
| Clinical Description | This was a randomized, controlled, open-label, Phase 3 multicenter study which enrolled patients with Relapsed-Refractory Multiple Myeloma (RRMM) who were either double refractory to an Immunomodulatory Drug (IMiD) and a Proteasome Inhibitor (PI) (regardless of the number of prior lines of therapy), or had received at least 3 prior lines of therapy including an IMiD and a PI. Patients received treatment with melflufen+dexamethasone+daratumumab or daratumumab until documented progressive disease, unacceptable toxicity, or patient/treating physician decision. Patients in the daratumumab treatment arm had the option to receive treatment with melflufen+dexamethasone+daratumumab after confirmed progressive disease. | ||||
| Experiment 324 Reporting the Activity Data of This PDC | [2] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Partial response (PR) |
14%
|
|||
| Patients Enrolled |
14 patients no prior ASCT or TTP >36 months after ASCT.
|
||||
| MOA of PDC |
Melphalan flufenamide (melflufen), a first-in-class alkylating peptide-drug conjugate, plus dexamethasone was approved in Europe for use in patients with triple-class refractory relapsed/refractory multiple myeloma (RRMM) with 3 prior lines of therapy and without prior autologous stem cell transplantation (ASCT) or with a time to progression >36 months after prior ASCT. The randomized LIGHTHOUSE study (NCT04649060) assessed melflufen plus daratumumab and dexamethasone (melflufen group) versus daratumumab in patients with RRMM with disease refractory to an immunomodulatory agent and a proteasome inhibitor or who had received 3 prior lines of therapy including an immunomodulatory agent and a proteasome inhibitor. A partial clinical hold issued by the US Food and Drug Administration for all melflufen studies led to financial constraints and premature study closure on February 23rd 2022 (data cut-off date). In total, 54 of 240 planned patients were randomized (melflufen group, N=27; daratumumab group, N=27). Median progression-free survival (PFS) was not reached in the melflufen group versus 4.9 months in the daratumumab group (Hazard Ratio: 0.18 [95% Confidence Interval, 0.05-0.65]; P=0.0032) at a median follow-up time of 7.1 and 6.6 months, respectively. Overall response rate (ORR) was 59% in the melflufen group versus 30% in the daratumumab group (P=0.0300). The most common grade 3 treatment-emergent adverse events in the melflufen group versus daratumumab group were neutropenia (50% vs. 12%), thrombocytopenia (50% vs. 8%), and anemia (32% vs. 19%). Melflufen plus daratumumab and dexamethasone demonstrated superior PFS and ORR versus daratumumab in RRMM and a safety profile comparable to previously published melflufen studies.
Click to Show/Hide
|
||||
| Description |
Efficacy endpoints were more pronounced in favor of the melflufen group compared with the daratumumab group among patients with no prior ASCT or TTP >36 months after a prior ASCT (melflufen group, N=14; daratumumab group, N=15). Median PFS was NR in the melflufen group and 3.9 months (95% CI: 1.4-4.9) in the daratumumab group (HR, 0.06 [95% CI: 0.01-0.49]; log-rank P=0.0005). Fewer OS events were reported in the melflufen group (1 event [7%] vs. 4 events [27%] in the daratumumab group; log-rank P=0.0369). The ORR was 64% (95% CI: 35-87) in the melflufen group and 13% (95% CI: 2-41) in the daratumumab group (P=0.0055). More patients in the melflufen group had a CR (1 patient [7%] vs. 0 patients [0%]) or VGPR (2 patients [14%] vs. 1 patient [7%]) compared with the daratumumab group.
Click to Show/Hide
|
||||
| Related Clinical Trial | |||||
| NCT Number | NCT04649060 | Clinical Status | Phase 3 | ||
| Clinical Description | This was a randomized, controlled, open-label, Phase 3 multicenter study which enrolled patients with Relapsed-Refractory Multiple Myeloma (RRMM) who were either double refractory to an Immunomodulatory Drug (IMiD) and a Proteasome Inhibitor (PI) (regardless of the number of prior lines of therapy), or had received at least 3 prior lines of therapy including an IMiD and a PI. Patients received treatment with melflufen+dexamethasone+daratumumab or daratumumab until documented progressive disease, unacceptable toxicity, or patient/treating physician decision. Patients in the daratumumab treatment arm had the option to receive treatment with melflufen+dexamethasone+daratumumab after confirmed progressive disease. | ||||
| Experiment 325 Reporting the Activity Data of This PDC | [2] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Partial response (PR) |
41%
|
|||
| MOA of PDC |
Melphalan flufenamide (melflufen), a first-in-class alkylating peptide-drug conjugate, plus dexamethasone was approved in Europe for use in patients with triple-class refractory relapsed/refractory multiple myeloma (RRMM) with 3 prior lines of therapy and without prior autologous stem cell transplantation (ASCT) or with a time to progression >36 months after prior ASCT. The randomized LIGHTHOUSE study (NCT04649060) assessed melflufen plus daratumumab and dexamethasone (melflufen group) versus daratumumab in patients with RRMM with disease refractory to an immunomodulatory agent and a proteasome inhibitor or who had received 3 prior lines of therapy including an immunomodulatory agent and a proteasome inhibitor. A partial clinical hold issued by the US Food and Drug Administration for all melflufen studies led to financial constraints and premature study closure on February 23rd 2022 (data cut-off date). In total, 54 of 240 planned patients were randomized (melflufen group, N=27; daratumumab group, N=27). Median progression-free survival (PFS) was not reached in the melflufen group versus 4.9 months in the daratumumab group (Hazard Ratio: 0.18 [95% Confidence Interval, 0.05-0.65]; P=0.0032) at a median follow-up time of 7.1 and 6.6 months, respectively. Overall response rate (ORR) was 59% in the melflufen group versus 30% in the daratumumab group (P=0.0300). The most common grade 3 treatment-emergent adverse events in the melflufen group versus daratumumab group were neutropenia (50% vs. 12%), thrombocytopenia (50% vs. 8%), and anemia (32% vs. 19%). Melflufen plus daratumumab and dexamethasone demonstrated superior PFS and ORR versus daratumumab in RRMM and a safety profile comparable to previously published melflufen studies.
Click to Show/Hide
|
||||
| Description |
In the ITT population, with a median follow-up of 7.1 months in the melflufen group, the median PFS was not reached (NR) and with a median follow-up of 6.6 months in the daratumumab group, the median PFS was 4.9 months (95% CI: 3.4-NR; HR: 0.18 [95% CI: 0.05-0.65]; log-rankP=0.0032). OS was immature, with 2 events (7%) in the melflufen group and 4 events (15%) in the daratumumab group (HR: 0.47 [95% CI: 0.09-2.57]; log-rankP=0.3721) at a median follow-up of 7.6 months and 6.6 months, respectively. The ORR was 59% (95% CI: 39-78) in the melflufen group and 30% (95% CI: 14-50) in the daratumumab group (P=0.0300). More patients in the melflufen group had a complete response (CR; 1 patient [4%]vs. 0 patients [0%]) and very good partial response (VGPR; 4 patients [15%]vs. 3 patients [11%]) compared with the daratumumab group.
Click to Show/Hide
|
||||
| In Vivo Model | 27 Intent-to-treat (ITT) population. | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT04649060 | Clinical Status | Phase 3 | ||
| Clinical Description | This was a randomized, controlled, open-label, Phase 3 multicenter study which enrolled patients with Relapsed-Refractory Multiple Myeloma (RRMM) who were either double refractory to an Immunomodulatory Drug (IMiD) and a Proteasome Inhibitor (PI) (regardless of the number of prior lines of therapy), or had received at least 3 prior lines of therapy including an IMiD and a PI. Patients received treatment with melflufen+dexamethasone+daratumumab or daratumumab until documented progressive disease, unacceptable toxicity, or patient/treating physician decision. Patients in the daratumumab treatment arm had the option to receive treatment with melflufen+dexamethasone+daratumumab after confirmed progressive disease. | ||||
| Experiment 326 Reporting the Activity Data of This PDC | [2] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Partial response (PR) |
43%
|
|||
| Patients Enrolled |
14 patients no prior ASCT or TTP >36 months after ASCT.
|
||||
| MOA of PDC |
Melphalan flufenamide (melflufen), a first-in-class alkylating peptide-drug conjugate, plus dexamethasone was approved in Europe for use in patients with triple-class refractory relapsed/refractory multiple myeloma (RRMM) with 3 prior lines of therapy and without prior autologous stem cell transplantation (ASCT) or with a time to progression >36 months after prior ASCT. The randomized LIGHTHOUSE study (NCT04649060) assessed melflufen plus daratumumab and dexamethasone (melflufen group) versus daratumumab in patients with RRMM with disease refractory to an immunomodulatory agent and a proteasome inhibitor or who had received 3 prior lines of therapy including an immunomodulatory agent and a proteasome inhibitor. A partial clinical hold issued by the US Food and Drug Administration for all melflufen studies led to financial constraints and premature study closure on February 23rd 2022 (data cut-off date). In total, 54 of 240 planned patients were randomized (melflufen group, N=27; daratumumab group, N=27). Median progression-free survival (PFS) was not reached in the melflufen group versus 4.9 months in the daratumumab group (Hazard Ratio: 0.18 [95% Confidence Interval, 0.05-0.65]; P=0.0032) at a median follow-up time of 7.1 and 6.6 months, respectively. Overall response rate (ORR) was 59% in the melflufen group versus 30% in the daratumumab group (P=0.0300). The most common grade 3 treatment-emergent adverse events in the melflufen group versus daratumumab group were neutropenia (50% vs. 12%), thrombocytopenia (50% vs. 8%), and anemia (32% vs. 19%). Melflufen plus daratumumab and dexamethasone demonstrated superior PFS and ORR versus daratumumab in RRMM and a safety profile comparable to previously published melflufen studies.
Click to Show/Hide
|
||||
| Description |
Efficacy endpoints were more pronounced in favor of the melflufen group compared with the daratumumab group among patients with no prior ASCT or TTP >36 months after a prior ASCT (melflufen group, N=14; daratumumab group, N=15). Median PFS was NR in the melflufen group and 3.9 months (95% CI: 1.4-4.9) in the daratumumab group (HR, 0.06 [95% CI: 0.01-0.49]; log-rank P=0.0005). Fewer OS events were reported in the melflufen group (1 event [7%] vs. 4 events [27%] in the daratumumab group; log-rank P=0.0369). The ORR was 64% (95% CI: 35-87) in the melflufen group and 13% (95% CI: 2-41) in the daratumumab group (P=0.0055). More patients in the melflufen group had a CR (1 patient [7%] vs. 0 patients [0%]) or VGPR (2 patients [14%] vs. 1 patient [7%]) compared with the daratumumab group.
Click to Show/Hide
|
||||
| Related Clinical Trial | |||||
| NCT Number | NCT04649060 | Clinical Status | Phase 3 | ||
| Clinical Description | This was a randomized, controlled, open-label, Phase 3 multicenter study which enrolled patients with Relapsed-Refractory Multiple Myeloma (RRMM) who were either double refractory to an Immunomodulatory Drug (IMiD) and a Proteasome Inhibitor (PI) (regardless of the number of prior lines of therapy), or had received at least 3 prior lines of therapy including an IMiD and a PI. Patients received treatment with melflufen+dexamethasone+daratumumab or daratumumab until documented progressive disease, unacceptable toxicity, or patient/treating physician decision. Patients in the daratumumab treatment arm had the option to receive treatment with melflufen+dexamethasone+daratumumab after confirmed progressive disease. | ||||
| Experiment 327 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Partial response (PR) |
21.40%
|
|||
| Patients Enrolled |
14 patients with relapsed refractory multiple myeloma.
|
||||
| Administration Time | 28-day cycle | ||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (melflufen) is a first-in-class peptide-drug conjugate that utilizes increased peptidase expression to selectively release potent alkylating agents inside tumor cells. Melflufen is hydrolyzed by peptidases and esterases to melphalan either directly or through an intermediate metabolite, desethyl-melflufen. The high lipophilicity of melflufen facilitates passive diffusion across cell membranes. The activity and tolerability of melflufen in relapsed/refractory multiple myeloma (RRMM) were demonstrated in the O-12-M1 (NCT01897714), OCEAN (NCT03151811), and HORIZON (NCT02963493) trials.
Click to Show/Hide
|
||||
| Description |
In Arm A, 4 of the 14 patients achieved an overall response (ORR 28.6% [95% CI: 8.4-58.1]) including 1 patient with CR, and the CBR was 57.1% (95% CI: 28.9-82.3). In Arm B, 1 of the 13 patients achieved an overall response (ORR 7.7% [95% CI: 0.2-36.0]), consisting of a PR, and the CBR was 15.4% (95% CI: 1.9-45.4). In the overall study population, 5 patients had an overall response (ORR 18.5% [95% CI: 6.3-38.1]). DOR data were insufficient to evaluate due to early termination of the study, the low number of patient events (1 in Arm A, 0 in Arm B), and the limited number of responses. Based on the 5 patients who had a response of PR or better at study termination (4 in Arm A, 1 in Arm B), the median TTR was 2.4 months in Arm A, 5.1 months in Arm B, and 2.6 months overall. Based on the 8 and 5 progression events in Arm A and Arm B, respectively, the median TTP was 5.8 months and 4.8 months, respectively, with a median TTP of 5.8 months in the overall population. The median PFS was 5.2 months (95% CI: 2.7 to not evaluable) and 2.9 months (95% CI: 1.5-4.6) in Arms A and B, respectively. For the overall study population, median PFS was 3.7 months (95% CI: 2.7-5.8).
Click to Show/Hide
|
||||
| Half life period | 75.6 h | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT04412707 | Clinical Status | Phase 2 | ||
| Clinical Description | This is a randomized, two-period, cross-over Phase 2 study, comparing PK, and assessing safety and tolerability and efficacy of peripheral and central intravenous administration of melflufen in patients with RRMM. It is an international study, enrolling patients in US and Europe. The study will enroll patients following at least 2 lines of prior therapy. | ||||
| Experiment 328 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Partial response (PR) |
9%
|
|||
| Patients Enrolled |
246 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 329 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Partial response (PR) |
10%
|
|||
| Patients Enrolled |
246 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 330 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Partial response (PR) |
19%
|
|||
| Patients Enrolled |
246 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 331 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Partial response (PR) |
20%
|
|||
| Patients Enrolled |
246 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 332 Reporting the Activity Data of This PDC | [2] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Pneumonia |
9%
|
|||
| MOA of PDC |
Melphalan flufenamide (melflufen), a first-in-class alkylating peptide-drug conjugate, plus dexamethasone was approved in Europe for use in patients with triple-class refractory relapsed/refractory multiple myeloma (RRMM) with 3 prior lines of therapy and without prior autologous stem cell transplantation (ASCT) or with a time to progression >36 months after prior ASCT. The randomized LIGHTHOUSE study (NCT04649060) assessed melflufen plus daratumumab and dexamethasone (melflufen group) versus daratumumab in patients with RRMM with disease refractory to an immunomodulatory agent and a proteasome inhibitor or who had received 3 prior lines of therapy including an immunomodulatory agent and a proteasome inhibitor. A partial clinical hold issued by the US Food and Drug Administration for all melflufen studies led to financial constraints and premature study closure on February 23rd 2022 (data cut-off date). In total, 54 of 240 planned patients were randomized (melflufen group, N=27; daratumumab group, N=27). Median progression-free survival (PFS) was not reached in the melflufen group versus 4.9 months in the daratumumab group (Hazard Ratio: 0.18 [95% Confidence Interval, 0.05-0.65]; P=0.0032) at a median follow-up time of 7.1 and 6.6 months, respectively. Overall response rate (ORR) was 59% in the melflufen group versus 30% in the daratumumab group (P=0.0300). The most common grade 3 treatment-emergent adverse events in the melflufen group versus daratumumab group were neutropenia (50% vs. 12%), thrombocytopenia (50% vs. 8%), and anemia (32% vs. 19%). Melflufen plus daratumumab and dexamethasone demonstrated superior PFS and ORR versus daratumumab in RRMM and a safety profile comparable to previously published melflufen studies.
Click to Show/Hide
|
||||
| Description |
The safety population included patients who received ≥1 dose of melflufen, daratumumab, or dexamethasone (melflufen group) and 26 patients who received daratumumab monotherapy. In the safety population, ≥1 TEAE was reported in 21 patients (96%) with melflufen, daratumumab, and dexamethasone and 22 patients (85%) with daratumumab. Overall, grade ≥3 TEAE occurred in 18 patients (82%) with melflufen, daratumumab, and dexamethasone and 14 patients (54%) with daratumumab. The most common hematologic grade ≥3 TEAE were neutropenia (melflufen group, 11 patients [50%]; daratumumab group, 3 patients [12%]), thrombocytopenia (melflufen group, 11 patients [50%]; daratumumab group, 2 patients [8%]), and anemia (melflufen group, 7 patients [32%]; daratumumab group, 5 patients [19%]). The most common non-hematologic grade ≥3 TEAE were pneumonia (melflufen group, 2 patients [9%]; daratumumab group, 2 patients [8%]) and femur fracture (melflufen group, 0 patients [0%]; daratumumab group, 2 patients [8%]); of these, 1 event (5%) of pneumonia in the melflufen group and 1 event (4%) of femur fracture in the daratumumab group were considered treatment-related TEAE by the investigator. Serious AE occurred in 6 patients (27%) with melflufen, daratumumab, and dexamethasone, and 12 patients (46%) with daratumumab. The most common serious AE (occurring in ≥4 patients overall) were anemia (melflufen group, 2 patients [9%]; daratumumab group, 3 patients [12%]) and pneumonia (melflufen group, 2 patients [9%]; daratumumab group, 2 patients [8%]). TEAE leading to treatment discontinuation occurred in 2 patients (9%) in the melflufen group (neutropenia and thrombocytopenia, N=1 each) and 4 patients (15%) in the daratumumab group (anemia, disease progression, hypercalcemia, and renal failure, N=1 each). Overall, 5 patients died on study before the crossover: 2 patients who received melflufen, daratumumab, and dexamethasone (1 due to disease progression and 1 due to unknown reasons, both >30 days after the last dose of study treatment) and 3 patients who received daratumumab (1 due to disease progression and 1 due to unknown reasons, both ≤30 days after the last dose of study treatment and 1 due to an AE [COVID-19 pneumonia], >30 days after the last dose of study treatment). In addition, one patient who crossed over to receive melflufen, daratumumab, and dexamethasone after progression on daratumumab died.
Click to Show/Hide
|
||||
| In Vivo Model | 22 relapsed/refractory multiple myeloma. | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT04649060 | Clinical Status | Phase 3 | ||
| Clinical Description | This was a randomized, controlled, open-label, Phase 3 multicenter study which enrolled patients with Relapsed-Refractory Multiple Myeloma (RRMM) who were either double refractory to an Immunomodulatory Drug (IMiD) and a Proteasome Inhibitor (PI) (regardless of the number of prior lines of therapy), or had received at least 3 prior lines of therapy including an IMiD and a PI. Patients received treatment with melflufen+dexamethasone+daratumumab or daratumumab until documented progressive disease, unacceptable toxicity, or patient/treating physician decision. Patients in the daratumumab treatment arm had the option to receive treatment with melflufen+dexamethasone+daratumumab after confirmed progressive disease. | ||||
| Experiment 333 Reporting the Activity Data of This PDC | [2] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Pneumonia |
9%
|
|||
| MOA of PDC |
Melphalan flufenamide (melflufen), a first-in-class alkylating peptide-drug conjugate, plus dexamethasone was approved in Europe for use in patients with triple-class refractory relapsed/refractory multiple myeloma (RRMM) with 3 prior lines of therapy and without prior autologous stem cell transplantation (ASCT) or with a time to progression >36 months after prior ASCT. The randomized LIGHTHOUSE study (NCT04649060) assessed melflufen plus daratumumab and dexamethasone (melflufen group) versus daratumumab in patients with RRMM with disease refractory to an immunomodulatory agent and a proteasome inhibitor or who had received 3 prior lines of therapy including an immunomodulatory agent and a proteasome inhibitor. A partial clinical hold issued by the US Food and Drug Administration for all melflufen studies led to financial constraints and premature study closure on February 23rd 2022 (data cut-off date). In total, 54 of 240 planned patients were randomized (melflufen group, N=27; daratumumab group, N=27). Median progression-free survival (PFS) was not reached in the melflufen group versus 4.9 months in the daratumumab group (Hazard Ratio: 0.18 [95% Confidence Interval, 0.05-0.65]; P=0.0032) at a median follow-up time of 7.1 and 6.6 months, respectively. Overall response rate (ORR) was 59% in the melflufen group versus 30% in the daratumumab group (P=0.0300). The most common grade 3 treatment-emergent adverse events in the melflufen group versus daratumumab group were neutropenia (50% vs. 12%), thrombocytopenia (50% vs. 8%), and anemia (32% vs. 19%). Melflufen plus daratumumab and dexamethasone demonstrated superior PFS and ORR versus daratumumab in RRMM and a safety profile comparable to previously published melflufen studies.
Click to Show/Hide
|
||||
| Description |
The safety population included patients who received ≥1 dose of melflufen, daratumumab, or dexamethasone (melflufen group) and 26 patients who received daratumumab monotherapy. In the safety population, ≥1 TEAE was reported in 21 patients (96%) with melflufen, daratumumab, and dexamethasone and 22 patients (85%) with daratumumab. Overall, grade ≥3 TEAE occurred in 18 patients (82%) with melflufen, daratumumab, and dexamethasone and 14 patients (54%) with daratumumab. The most common hematologic grade ≥3 TEAE were neutropenia (melflufen group, 11 patients [50%]; daratumumab group, 3 patients [12%]), thrombocytopenia (melflufen group, 11 patients [50%]; daratumumab group, 2 patients [8%]), and anemia (melflufen group, 7 patients [32%]; daratumumab group, 5 patients [19%]). The most common non-hematologic grade ≥3 TEAE were pneumonia (melflufen group, 2 patients [9%]; daratumumab group, 2 patients [8%]) and femur fracture (melflufen group, 0 patients [0%]; daratumumab group, 2 patients [8%]); of these, 1 event (5%) of pneumonia in the melflufen group and 1 event (4%) of femur fracture in the daratumumab group were considered treatment-related TEAE by the investigator. Serious AE occurred in 6 patients (27%) with melflufen, daratumumab, and dexamethasone, and 12 patients (46%) with daratumumab. The most common serious AE (occurring in ≥4 patients overall) were anemia (melflufen group, 2 patients [9%]; daratumumab group, 3 patients [12%]) and pneumonia (melflufen group, 2 patients [9%]; daratumumab group, 2 patients [8%]). TEAE leading to treatment discontinuation occurred in 2 patients (9%) in the melflufen group (neutropenia and thrombocytopenia, N=1 each) and 4 patients (15%) in the daratumumab group (anemia, disease progression, hypercalcemia, and renal failure, N=1 each). Overall, 5 patients died on study before the crossover: 2 patients who received melflufen, daratumumab, and dexamethasone (1 due to disease progression and 1 due to unknown reasons, both >30 days after the last dose of study treatment) and 3 patients who received daratumumab (1 due to disease progression and 1 due to unknown reasons, both ≤30 days after the last dose of study treatment and 1 due to an AE [COVID-19 pneumonia], >30 days after the last dose of study treatment). In addition, one patient who crossed over to receive melflufen, daratumumab, and dexamethasone after progression on daratumumab died.
Click to Show/Hide
|
||||
| In Vivo Model | 22 relapsed/refractory multiple myeloma. | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT04649060 | Clinical Status | Phase 3 | ||
| Clinical Description | This was a randomized, controlled, open-label, Phase 3 multicenter study which enrolled patients with Relapsed-Refractory Multiple Myeloma (RRMM) who were either double refractory to an Immunomodulatory Drug (IMiD) and a Proteasome Inhibitor (PI) (regardless of the number of prior lines of therapy), or had received at least 3 prior lines of therapy including an IMiD and a PI. Patients received treatment with melflufen+dexamethasone+daratumumab or daratumumab until documented progressive disease, unacceptable toxicity, or patient/treating physician decision. Patients in the daratumumab treatment arm had the option to receive treatment with melflufen+dexamethasone+daratumumab after confirmed progressive disease. | ||||
| Experiment 334 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Pneumonia |
21.40%
|
|||
| Patients Enrolled |
14 patients with relapsed refractory multiple myeloma.
|
||||
| Administration Time | 28-day cycle | ||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (melflufen) is a first-in-class peptide-drug conjugate that utilizes increased peptidase expression to selectively release potent alkylating agents inside tumor cells. Melflufen is hydrolyzed by peptidases and esterases to melphalan either directly or through an intermediate metabolite, desethyl-melflufen. The high lipophilicity of melflufen facilitates passive diffusion across cell membranes. The activity and tolerability of melflufen in relapsed/refractory multiple myeloma (RRMM) were demonstrated in the O-12-M1 (NCT01897714), OCEAN (NCT03151811), and HORIZON (NCT02963493) trials.
Click to Show/Hide
|
||||
| Description |
Overall, at least one TEAE was reported in 13 (92.9%) and 13 (100.0%) patients in Arms A and B, respectively (Table 3). During cycle 1, 9 patients (64.3%) and 12 patients (92.3%), respectively, had at least one TEAE. Cumulatively, grade 3 or 4 AEs occurred in 12 (85.7%) and 12 (92.3%) patients, respectively, and serious AEs were reported in 5 (35.7%) and 9 (69.2%) patients, respectively. The most common any-grade AEs in Arms A and B, respectively, were thrombocytopenia (10 [71.4%]; 10 [76.9%]), neutropenia (9 [64.3%]; 9 [69.2%]), and anemia (9 [64.3%]; 7 [53.8%]). No phlebitis or local-infusion-related reactions were reported based on pre- and post-infusion inspection of the IV site, and there were no extravasations observed in Arm A or B. Similarly, VIP scores collected on Day 1 post-infusion and on Day 8 indicated that patients had healthy IV sites (VIP score of 0) with no signs of phlebitis following PVC administration of melflufen. The most common non-hematological AE was positive SARS-CoV-2 test (Arm A: 2 [14.3%]; Arm B: 4 [30.8%]). Pneumonia was the most common serious AE (Arm A: 2 [14.3%]; Arm B: 2 [15.4%]). The most common AE considered related to melflufen and/or dexamethasone by investigators was thrombocytopenia (Arm A: 10 [71.4%]; Arm B: 10 [76.9%]). AEs led to treatment discontinuation in 3 (21.4%) and 6 (46.2%) patients in Arms A and B, respectively.
Click to Show/Hide
|
||||
| Half life period | 75.6 h | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT04412707 | Clinical Status | Phase 2 | ||
| Clinical Description | This is a randomized, two-period, cross-over Phase 2 study, comparing PK, and assessing safety and tolerability and efficacy of peripheral and central intravenous administration of melflufen in patients with RRMM. It is an international study, enrolling patients in US and Europe. The study will enroll patients following at least 2 lines of prior therapy. | ||||
| Experiment 335 Reporting the Activity Data of This PDC | [2] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Progressive Disease (PD) |
14%
|
|||
| Patients Enrolled |
14 patients no prior ASCT or TTP >36 months after ASCT.
|
||||
| MOA of PDC |
Melphalan flufenamide (melflufen), a first-in-class alkylating peptide-drug conjugate, plus dexamethasone was approved in Europe for use in patients with triple-class refractory relapsed/refractory multiple myeloma (RRMM) with 3 prior lines of therapy and without prior autologous stem cell transplantation (ASCT) or with a time to progression >36 months after prior ASCT. The randomized LIGHTHOUSE study (NCT04649060) assessed melflufen plus daratumumab and dexamethasone (melflufen group) versus daratumumab in patients with RRMM with disease refractory to an immunomodulatory agent and a proteasome inhibitor or who had received 3 prior lines of therapy including an immunomodulatory agent and a proteasome inhibitor. A partial clinical hold issued by the US Food and Drug Administration for all melflufen studies led to financial constraints and premature study closure on February 23rd 2022 (data cut-off date). In total, 54 of 240 planned patients were randomized (melflufen group, N=27; daratumumab group, N=27). Median progression-free survival (PFS) was not reached in the melflufen group versus 4.9 months in the daratumumab group (Hazard Ratio: 0.18 [95% Confidence Interval, 0.05-0.65]; P=0.0032) at a median follow-up time of 7.1 and 6.6 months, respectively. Overall response rate (ORR) was 59% in the melflufen group versus 30% in the daratumumab group (P=0.0300). The most common grade 3 treatment-emergent adverse events in the melflufen group versus daratumumab group were neutropenia (50% vs. 12%), thrombocytopenia (50% vs. 8%), and anemia (32% vs. 19%). Melflufen plus daratumumab and dexamethasone demonstrated superior PFS and ORR versus daratumumab in RRMM and a safety profile comparable to previously published melflufen studies.
Click to Show/Hide
|
||||
| Description |
Efficacy endpoints were more pronounced in favor of the melflufen group compared with the daratumumab group among patients with no prior ASCT or TTP >36 months after a prior ASCT (melflufen group, N=14; daratumumab group, N=15). Median PFS was NR in the melflufen group and 3.9 months (95% CI: 1.4-4.9) in the daratumumab group (HR, 0.06 [95% CI: 0.01-0.49]; log-rank P=0.0005). Fewer OS events were reported in the melflufen group (1 event [7%] vs. 4 events [27%] in the daratumumab group; log-rank P=0.0369). The ORR was 64% (95% CI: 35-87) in the melflufen group and 13% (95% CI: 2-41) in the daratumumab group (P=0.0055). More patients in the melflufen group had a CR (1 patient [7%] vs. 0 patients [0%]) or VGPR (2 patients [14%] vs. 1 patient [7%]) compared with the daratumumab group.
Click to Show/Hide
|
||||
| Related Clinical Trial | |||||
| NCT Number | NCT04649060 | Clinical Status | Phase 3 | ||
| Clinical Description | This was a randomized, controlled, open-label, Phase 3 multicenter study which enrolled patients with Relapsed-Refractory Multiple Myeloma (RRMM) who were either double refractory to an Immunomodulatory Drug (IMiD) and a Proteasome Inhibitor (PI) (regardless of the number of prior lines of therapy), or had received at least 3 prior lines of therapy including an IMiD and a PI. Patients received treatment with melflufen+dexamethasone+daratumumab or daratumumab until documented progressive disease, unacceptable toxicity, or patient/treating physician decision. Patients in the daratumumab treatment arm had the option to receive treatment with melflufen+dexamethasone+daratumumab after confirmed progressive disease. | ||||
| Experiment 336 Reporting the Activity Data of This PDC | [2] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Progressive Disease (PD) |
15%
|
|||
| MOA of PDC |
Melphalan flufenamide (melflufen), a first-in-class alkylating peptide-drug conjugate, plus dexamethasone was approved in Europe for use in patients with triple-class refractory relapsed/refractory multiple myeloma (RRMM) with 3 prior lines of therapy and without prior autologous stem cell transplantation (ASCT) or with a time to progression >36 months after prior ASCT. The randomized LIGHTHOUSE study (NCT04649060) assessed melflufen plus daratumumab and dexamethasone (melflufen group) versus daratumumab in patients with RRMM with disease refractory to an immunomodulatory agent and a proteasome inhibitor or who had received 3 prior lines of therapy including an immunomodulatory agent and a proteasome inhibitor. A partial clinical hold issued by the US Food and Drug Administration for all melflufen studies led to financial constraints and premature study closure on February 23rd 2022 (data cut-off date). In total, 54 of 240 planned patients were randomized (melflufen group, N=27; daratumumab group, N=27). Median progression-free survival (PFS) was not reached in the melflufen group versus 4.9 months in the daratumumab group (Hazard Ratio: 0.18 [95% Confidence Interval, 0.05-0.65]; P=0.0032) at a median follow-up time of 7.1 and 6.6 months, respectively. Overall response rate (ORR) was 59% in the melflufen group versus 30% in the daratumumab group (P=0.0300). The most common grade 3 treatment-emergent adverse events in the melflufen group versus daratumumab group were neutropenia (50% vs. 12%), thrombocytopenia (50% vs. 8%), and anemia (32% vs. 19%). Melflufen plus daratumumab and dexamethasone demonstrated superior PFS and ORR versus daratumumab in RRMM and a safety profile comparable to previously published melflufen studies.
Click to Show/Hide
|
||||
| Description |
In the ITT population, with a median follow-up of 7.1 months in the melflufen group, the median PFS was not reached (NR) and with a median follow-up of 6.6 months in the daratumumab group, the median PFS was 4.9 months (95% CI: 3.4-NR; HR: 0.18 [95% CI: 0.05-0.65]; log-rankP=0.0032). OS was immature, with 2 events (7%) in the melflufen group and 4 events (15%) in the daratumumab group (HR: 0.47 [95% CI: 0.09-2.57]; log-rankP=0.3721) at a median follow-up of 7.6 months and 6.6 months, respectively. The ORR was 59% (95% CI: 39-78) in the melflufen group and 30% (95% CI: 14-50) in the daratumumab group (P=0.0300). More patients in the melflufen group had a complete response (CR; 1 patient [4%]vs. 0 patients [0%]) and very good partial response (VGPR; 4 patients [15%]vs. 3 patients [11%]) compared with the daratumumab group.
Click to Show/Hide
|
||||
| In Vivo Model | 27 Intent-to-treat (ITT) population. | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT04649060 | Clinical Status | Phase 3 | ||
| Clinical Description | This was a randomized, controlled, open-label, Phase 3 multicenter study which enrolled patients with Relapsed-Refractory Multiple Myeloma (RRMM) who were either double refractory to an Immunomodulatory Drug (IMiD) and a Proteasome Inhibitor (PI) (regardless of the number of prior lines of therapy), or had received at least 3 prior lines of therapy including an IMiD and a PI. Patients received treatment with melflufen+dexamethasone+daratumumab or daratumumab until documented progressive disease, unacceptable toxicity, or patient/treating physician decision. Patients in the daratumumab treatment arm had the option to receive treatment with melflufen+dexamethasone+daratumumab after confirmed progressive disease. | ||||
| Experiment 337 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Progressive Disease (PD) |
14.30%
|
|||
| Patients Enrolled |
14 patients with relapsed refractory multiple myeloma.
|
||||
| Administration Time | 28-day cycle | ||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (melflufen) is a first-in-class peptide-drug conjugate that utilizes increased peptidase expression to selectively release potent alkylating agents inside tumor cells. Melflufen is hydrolyzed by peptidases and esterases to melphalan either directly or through an intermediate metabolite, desethyl-melflufen. The high lipophilicity of melflufen facilitates passive diffusion across cell membranes. The activity and tolerability of melflufen in relapsed/refractory multiple myeloma (RRMM) were demonstrated in the O-12-M1 (NCT01897714), OCEAN (NCT03151811), and HORIZON (NCT02963493) trials.
Click to Show/Hide
|
||||
| Description |
In Arm A, 4 of the 14 patients achieved an overall response (ORR 28.6% [95% CI: 8.4-58.1]) including 1 patient with CR, and the CBR was 57.1% (95% CI: 28.9-82.3). In Arm B, 1 of the 13 patients achieved an overall response (ORR 7.7% [95% CI: 0.2-36.0]), consisting of a PR, and the CBR was 15.4% (95% CI: 1.9-45.4). In the overall study population, 5 patients had an overall response (ORR 18.5% [95% CI: 6.3-38.1]). DOR data were insufficient to evaluate due to early termination of the study, the low number of patient events (1 in Arm A, 0 in Arm B), and the limited number of responses. Based on the 5 patients who had a response of PR or better at study termination (4 in Arm A, 1 in Arm B), the median TTR was 2.4 months in Arm A, 5.1 months in Arm B, and 2.6 months overall. Based on the 8 and 5 progression events in Arm A and Arm B, respectively, the median TTP was 5.8 months and 4.8 months, respectively, with a median TTP of 5.8 months in the overall population. The median PFS was 5.2 months (95% CI: 2.7 to not evaluable) and 2.9 months (95% CI: 1.5-4.6) in Arms A and B, respectively. For the overall study population, median PFS was 3.7 months (95% CI: 2.7-5.8).
Click to Show/Hide
|
||||
| Half life period | 75.6 h | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT04412707 | Clinical Status | Phase 2 | ||
| Clinical Description | This is a randomized, two-period, cross-over Phase 2 study, comparing PK, and assessing safety and tolerability and efficacy of peripheral and central intravenous administration of melflufen in patients with RRMM. It is an international study, enrolling patients in US and Europe. The study will enroll patients following at least 2 lines of prior therapy. | ||||
| Experiment 338 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Progressive disease (PD) |
15%
|
|||
| Patients Enrolled |
246 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 339 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Progressive disease (PD) |
19%
|
|||
| Patients Enrolled |
246 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 340 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Pyrexia |
14.30%
|
|||
| Patients Enrolled |
14 patients with relapsed refractory multiple myeloma.
|
||||
| Administration Time | 28-day cycle | ||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (melflufen) is a first-in-class peptide-drug conjugate that utilizes increased peptidase expression to selectively release potent alkylating agents inside tumor cells. Melflufen is hydrolyzed by peptidases and esterases to melphalan either directly or through an intermediate metabolite, desethyl-melflufen. The high lipophilicity of melflufen facilitates passive diffusion across cell membranes. The activity and tolerability of melflufen in relapsed/refractory multiple myeloma (RRMM) were demonstrated in the O-12-M1 (NCT01897714), OCEAN (NCT03151811), and HORIZON (NCT02963493) trials.
Click to Show/Hide
|
||||
| Description |
Overall, at least one TEAE was reported in 13 (92.9%) and 13 (100.0%) patients in Arms A and B, respectively (Table 3). During cycle 1, 9 patients (64.3%) and 12 patients (92.3%), respectively, had at least one TEAE. Cumulatively, grade 3 or 4 AEs occurred in 12 (85.7%) and 12 (92.3%) patients, respectively, and serious AEs were reported in 5 (35.7%) and 9 (69.2%) patients, respectively. The most common any-grade AEs in Arms A and B, respectively, were thrombocytopenia (10 [71.4%]; 10 [76.9%]), neutropenia (9 [64.3%]; 9 [69.2%]), and anemia (9 [64.3%]; 7 [53.8%]). No phlebitis or local-infusion-related reactions were reported based on pre- and post-infusion inspection of the IV site, and there were no extravasations observed in Arm A or B. Similarly, VIP scores collected on Day 1 post-infusion and on Day 8 indicated that patients had healthy IV sites (VIP score of 0) with no signs of phlebitis following PVC administration of melflufen. The most common non-hematological AE was positive SARS-CoV-2 test (Arm A: 2 [14.3%]; Arm B: 4 [30.8%]). Pneumonia was the most common serious AE (Arm A: 2 [14.3%]; Arm B: 2 [15.4%]). The most common AE considered related to melflufen and/or dexamethasone by investigators was thrombocytopenia (Arm A: 10 [71.4%]; Arm B: 10 [76.9%]). AEs led to treatment discontinuation in 3 (21.4%) and 6 (46.2%) patients in Arms A and B, respectively.
Click to Show/Hide
|
||||
| Half life period | 75.6 h | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT04412707 | Clinical Status | Phase 2 | ||
| Clinical Description | This is a randomized, two-period, cross-over Phase 2 study, comparing PK, and assessing safety and tolerability and efficacy of peripheral and central intravenous administration of melflufen in patients with RRMM. It is an international study, enrolling patients in US and Europe. The study will enroll patients following at least 2 lines of prior therapy. | ||||
| Experiment 341 Reporting the Activity Data of This PDC | [4] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Pyrexia |
24%
|
|||
| Patients Enrolled |
157 patients with multiple myeloma.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melflufen is a first-in-class peptide-drug conjugate, targeting aminopeptidase which has an increased expression in fast-growing and aggressive malignancies. The lipophilicity of melflufen allows for passive diffusion, selectively targeting myeloma cells. Once inside the cell, melflufen is hydrolyzed to active alkylating metabolites melphalan and desethyl-melflufen. Melflufen and the active metabolites trigger irreversible DNA damage, inhibit proliferation, induces apoptosis, and express antiangiogenic effects. In addition, melflufen demonstrated activity in myeloma cells with documented impaired or absent Tp53 expression and documented resistance to bortezomib, dexamethasone, and melphalan.
Click to Show/Hide
|
||||
| Description |
Based on the safety data collected during the HORIZON trial, treatment emergent adverse events occurred in 100% of patients including 100 patients (64%) having at least 1 CTCAE grade 4 adverse effect. Hematologic grade 3 or 4 adverse effects including thrombocytopenia (76%), neutropenia (79%), anemia (43%), and infections (11%) were the most commonly reported. Other adverse effects, such as fatigue (55%), nausea (32%), diarrhea (27%), and decreased appetite (14%), were similar to other alkylating agents. Pyrexia (24%), including febrile neutropenia (5%), and respiratory tract infections (24%) were contributed to hematologic toxicities.
Click to Show/Hide
|
||||
| Experiment 342 Reporting the Activity Data of This PDC | [1] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Pyrexia |
40%
|
|||
| Patients Enrolled |
Patients with multi-refractory multiple myeloma.
|
||||
| MOA of PDC |
Melflufen is highly lipophilic, which promotes its rapid uptake by cells. Once within the cell, melflufen releases its hydrophilic alkylator payloads via the hydrolytic activity of intracellular peptidases (e.g., aminopeptidases). Aminopeptidases are Zn2+-dependent metalloproteinases that remove amino acids at the N-terminal position from oligopeptides and have been associated with multiple tumorigenic processes such as proliferation, apoptosis, differentiation, angiogenesis, and motility. The dependence of melflufen on aminopeptidases was initially demonstrated by the reduced cytotoxic activity of melflufen-but not the alkylator melphalan-when cells were pretreated with bestatin, an antibiotic that is a potent aminopeptidase inhibitor. In addition, structure analogs designed to resist peptide hydrolysis (N-methyl derivative and derivative with D-amino acid) were shown to be almost 100-fold less potent than melflufen. Subsequent in vitro studies demonstrated that hydrolytic cleavage of melflufen by aminopeptidases releases alkylator payloads, including melphalan. In vitro, the activity of melflufen is multi-pronged, including induction of DNA damage, induction of apoptosis, inhibition of VEGF-dependent cell migration, and inhibition of tumor-associated angiogenesis, which have been further reviewed elsewhere. Downregulation of aminopeptidases resulted in reduced melflufen-mediated cytotoxic activity and apoptotic signaling in cultured cells.
Click to Show/Hide
|
||||
| Description |
Melflufen plus dexamethasone was generally manageable in this heavily pretreated patient population [51]. All patients experienced ≥1 AE, most commonly hematologic AEs including thrombocytopenia (73%), neutropenia (69%), and anemia (64%). The most common non-hematologic AEs included pyrexia (40%), asthenia (31%), fatigue (29%), nausea (27%), and diarrhea (24%).
Click to Show/Hide
|
||||
| Experiment 343 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Rash |
14.30%
|
|||
| Patients Enrolled |
14 patients with relapsed refractory multiple myeloma.
|
||||
| Administration Time | 28-day cycle | ||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (melflufen) is a first-in-class peptide-drug conjugate that utilizes increased peptidase expression to selectively release potent alkylating agents inside tumor cells. Melflufen is hydrolyzed by peptidases and esterases to melphalan either directly or through an intermediate metabolite, desethyl-melflufen. The high lipophilicity of melflufen facilitates passive diffusion across cell membranes. The activity and tolerability of melflufen in relapsed/refractory multiple myeloma (RRMM) were demonstrated in the O-12-M1 (NCT01897714), OCEAN (NCT03151811), and HORIZON (NCT02963493) trials.
Click to Show/Hide
|
||||
| Description |
Overall, at least one TEAE was reported in 13 (92.9%) and 13 (100.0%) patients in Arms A and B, respectively (Table 3). During cycle 1, 9 patients (64.3%) and 12 patients (92.3%), respectively, had at least one TEAE. Cumulatively, grade 3 or 4 AEs occurred in 12 (85.7%) and 12 (92.3%) patients, respectively, and serious AEs were reported in 5 (35.7%) and 9 (69.2%) patients, respectively. The most common any-grade AEs in Arms A and B, respectively, were thrombocytopenia (10 [71.4%]; 10 [76.9%]), neutropenia (9 [64.3%]; 9 [69.2%]), and anemia (9 [64.3%]; 7 [53.8%]). No phlebitis or local-infusion-related reactions were reported based on pre- and post-infusion inspection of the IV site, and there were no extravasations observed in Arm A or B. Similarly, VIP scores collected on Day 1 post-infusion and on Day 8 indicated that patients had healthy IV sites (VIP score of 0) with no signs of phlebitis following PVC administration of melflufen. The most common non-hematological AE was positive SARS-CoV-2 test (Arm A: 2 [14.3%]; Arm B: 4 [30.8%]). Pneumonia was the most common serious AE (Arm A: 2 [14.3%]; Arm B: 2 [15.4%]). The most common AE considered related to melflufen and/or dexamethasone by investigators was thrombocytopenia (Arm A: 10 [71.4%]; Arm B: 10 [76.9%]). AEs led to treatment discontinuation in 3 (21.4%) and 6 (46.2%) patients in Arms A and B, respectively.
Click to Show/Hide
|
||||
| Half life period | 75.6 h | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT04412707 | Clinical Status | Phase 2 | ||
| Clinical Description | This is a randomized, two-period, cross-over Phase 2 study, comparing PK, and assessing safety and tolerability and efficacy of peripheral and central intravenous administration of melflufen in patients with RRMM. It is an international study, enrolling patients in US and Europe. The study will enroll patients following at least 2 lines of prior therapy. | ||||
| Experiment 344 Reporting the Activity Data of This PDC | [1] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Rate of adverse events |
36%
|
|||
| Patients Enrolled |
Patients with multi-refractory multiple myeloma.
|
||||
| Administration Time | 6.2 month (median) | ||||
| Administration Dosage | 30 or 40 mg | ||||
| MOA of PDC |
Melflufen is highly lipophilic, which promotes its rapid uptake by cells. Once within the cell, melflufen releases its hydrophilic alkylator payloads via the hydrolytic activity of intracellular peptidases (e.g., aminopeptidases). Aminopeptidases are Zn2+-dependent metalloproteinases that remove amino acids at the N-terminal position from oligopeptides and have been associated with multiple tumorigenic processes such as proliferation, apoptosis, differentiation, angiogenesis, and motility. The dependence of melflufen on aminopeptidases was initially demonstrated by the reduced cytotoxic activity of melflufen-but not the alkylator melphalan-when cells were pretreated with bestatin, an antibiotic that is a potent aminopeptidase inhibitor. In addition, structure analogs designed to resist peptide hydrolysis (N-methyl derivative and derivative with D-amino acid) were shown to be almost 100-fold less potent than melflufen. Subsequent in vitro studies demonstrated that hydrolytic cleavage of melflufen by aminopeptidases releases alkylator payloads, including melphalan. In vitro, the activity of melflufen is multi-pronged, including induction of DNA damage, induction of apoptosis, inhibition of VEGF-dependent cell migration, and inhibition of tumor-associated angiogenesis, which have been further reviewed elsewhere. Downregulation of aminopeptidases resulted in reduced melflufen-mediated cytotoxic activity and apoptotic signaling in cultured cells.
Click to Show/Hide
|
||||
| Experiment 345 Reporting the Activity Data of This PDC | [1] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Rate of adverse events |
38%
|
|||
| Patients Enrolled |
Patients with multi-refractory multiple myeloma.
|
||||
| Administration Time | 28-day cycle | ||||
| Administration Dosage | 40 mg with dexamethasone (40 mg) | ||||
| MOA of PDC |
Melflufen is highly lipophilic, which promotes its rapid uptake by cells. Once within the cell, melflufen releases its hydrophilic alkylator payloads via the hydrolytic activity of intracellular peptidases (e.g., aminopeptidases). Aminopeptidases are Zn2+-dependent metalloproteinases that remove amino acids at the N-terminal position from oligopeptides and have been associated with multiple tumorigenic processes such as proliferation, apoptosis, differentiation, angiogenesis, and motility. The dependence of melflufen on aminopeptidases was initially demonstrated by the reduced cytotoxic activity of melflufen-but not the alkylator melphalan-when cells were pretreated with bestatin, an antibiotic that is a potent aminopeptidase inhibitor. In addition, structure analogs designed to resist peptide hydrolysis (N-methyl derivative and derivative with D-amino acid) were shown to be almost 100-fold less potent than melflufen. Subsequent in vitro studies demonstrated that hydrolytic cleavage of melflufen by aminopeptidases releases alkylator payloads, including melphalan. In vitro, the activity of melflufen is multi-pronged, including induction of DNA damage, induction of apoptosis, inhibition of VEGF-dependent cell migration, and inhibition of tumor-associated angiogenesis, which have been further reviewed elsewhere. Downregulation of aminopeptidases resulted in reduced melflufen-mediated cytotoxic activity and apoptotic signaling in cultured cells.
Click to Show/Hide
|
||||
| Experiment 346 Reporting the Activity Data of This PDC | [1] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Rate of adverse events |
83%
|
|||
| Patients Enrolled |
Patients with multi-refractory multiple myeloma.
|
||||
| Administration Time | 9.3 month (median) | ||||
| Administration Dosage | 30 or 40 mg | ||||
| MOA of PDC |
Melflufen is highly lipophilic, which promotes its rapid uptake by cells. Once within the cell, melflufen releases its hydrophilic alkylator payloads via the hydrolytic activity of intracellular peptidases (e.g., aminopeptidases). Aminopeptidases are Zn2+-dependent metalloproteinases that remove amino acids at the N-terminal position from oligopeptides and have been associated with multiple tumorigenic processes such as proliferation, apoptosis, differentiation, angiogenesis, and motility. The dependence of melflufen on aminopeptidases was initially demonstrated by the reduced cytotoxic activity of melflufen-but not the alkylator melphalan-when cells were pretreated with bestatin, an antibiotic that is a potent aminopeptidase inhibitor. In addition, structure analogs designed to resist peptide hydrolysis (N-methyl derivative and derivative with D-amino acid) were shown to be almost 100-fold less potent than melflufen. Subsequent in vitro studies demonstrated that hydrolytic cleavage of melflufen by aminopeptidases releases alkylator payloads, including melphalan. In vitro, the activity of melflufen is multi-pronged, including induction of DNA damage, induction of apoptosis, inhibition of VEGF-dependent cell migration, and inhibition of tumor-associated angiogenesis, which have been further reviewed elsewhere. Downregulation of aminopeptidases resulted in reduced melflufen-mediated cytotoxic activity and apoptotic signaling in cultured cells.
Click to Show/Hide
|
||||
| Experiment 347 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Respiratory tract infection |
14.30%
|
|||
| Patients Enrolled |
14 patients with relapsed refractory multiple myeloma.
|
||||
| Administration Time | 28-day cycle | ||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (melflufen) is a first-in-class peptide-drug conjugate that utilizes increased peptidase expression to selectively release potent alkylating agents inside tumor cells. Melflufen is hydrolyzed by peptidases and esterases to melphalan either directly or through an intermediate metabolite, desethyl-melflufen. The high lipophilicity of melflufen facilitates passive diffusion across cell membranes. The activity and tolerability of melflufen in relapsed/refractory multiple myeloma (RRMM) were demonstrated in the O-12-M1 (NCT01897714), OCEAN (NCT03151811), and HORIZON (NCT02963493) trials.
Click to Show/Hide
|
||||
| Description |
Overall, at least one TEAE was reported in 13 (92.9%) and 13 (100.0%) patients in Arms A and B, respectively (Table 3). During cycle 1, 9 patients (64.3%) and 12 patients (92.3%), respectively, had at least one TEAE. Cumulatively, grade 3 or 4 AEs occurred in 12 (85.7%) and 12 (92.3%) patients, respectively, and serious AEs were reported in 5 (35.7%) and 9 (69.2%) patients, respectively. The most common any-grade AEs in Arms A and B, respectively, were thrombocytopenia (10 [71.4%]; 10 [76.9%]), neutropenia (9 [64.3%]; 9 [69.2%]), and anemia (9 [64.3%]; 7 [53.8%]). No phlebitis or local-infusion-related reactions were reported based on pre- and post-infusion inspection of the IV site, and there were no extravasations observed in Arm A or B. Similarly, VIP scores collected on Day 1 post-infusion and on Day 8 indicated that patients had healthy IV sites (VIP score of 0) with no signs of phlebitis following PVC administration of melflufen. The most common non-hematological AE was positive SARS-CoV-2 test (Arm A: 2 [14.3%]; Arm B: 4 [30.8%]). Pneumonia was the most common serious AE (Arm A: 2 [14.3%]; Arm B: 2 [15.4%]). The most common AE considered related to melflufen and/or dexamethasone by investigators was thrombocytopenia (Arm A: 10 [71.4%]; Arm B: 10 [76.9%]). AEs led to treatment discontinuation in 3 (21.4%) and 6 (46.2%) patients in Arms A and B, respectively.
Click to Show/Hide
|
||||
| Half life period | 75.6 h | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT04412707 | Clinical Status | Phase 2 | ||
| Clinical Description | This is a randomized, two-period, cross-over Phase 2 study, comparing PK, and assessing safety and tolerability and efficacy of peripheral and central intravenous administration of melflufen in patients with RRMM. It is an international study, enrolling patients in US and Europe. The study will enroll patients following at least 2 lines of prior therapy. | ||||
| Experiment 348 Reporting the Activity Data of This PDC | [4] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Respiratory tract infection |
24%
|
|||
| Patients Enrolled |
157 patients with multiple myeloma.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melflufen is a first-in-class peptide-drug conjugate, targeting aminopeptidase which has an increased expression in fast-growing and aggressive malignancies. The lipophilicity of melflufen allows for passive diffusion, selectively targeting myeloma cells. Once inside the cell, melflufen is hydrolyzed to active alkylating metabolites melphalan and desethyl-melflufen. Melflufen and the active metabolites trigger irreversible DNA damage, inhibit proliferation, induces apoptosis, and express antiangiogenic effects. In addition, melflufen demonstrated activity in myeloma cells with documented impaired or absent Tp53 expression and documented resistance to bortezomib, dexamethasone, and melphalan.
Click to Show/Hide
|
||||
| Description |
Based on the safety data collected during the HORIZON trial, treatment emergent adverse events occurred in 100% of patients including 100 patients (64%) having at least 1 CTCAE grade 4 adverse effect. Hematologic grade 3 or 4 adverse effects including thrombocytopenia (76%), neutropenia (79%), anemia (43%), and infections (11%) were the most commonly reported. Other adverse effects, such as fatigue (55%), nausea (32%), diarrhea (27%), and decreased appetite (14%), were similar to other alkylating agents. Pyrexia (24%), including febrile neutropenia (5%), and respiratory tract infections (24%) were contributed to hematologic toxicities.
Click to Show/Hide
|
||||
| Experiment 349 Reporting the Activity Data of This PDC | [2] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Serious adverse event rate |
27%
|
|||
| MOA of PDC |
Melphalan flufenamide (melflufen), a first-in-class alkylating peptide-drug conjugate, plus dexamethasone was approved in Europe for use in patients with triple-class refractory relapsed/refractory multiple myeloma (RRMM) with 3 prior lines of therapy and without prior autologous stem cell transplantation (ASCT) or with a time to progression >36 months after prior ASCT. The randomized LIGHTHOUSE study (NCT04649060) assessed melflufen plus daratumumab and dexamethasone (melflufen group) versus daratumumab in patients with RRMM with disease refractory to an immunomodulatory agent and a proteasome inhibitor or who had received 3 prior lines of therapy including an immunomodulatory agent and a proteasome inhibitor. A partial clinical hold issued by the US Food and Drug Administration for all melflufen studies led to financial constraints and premature study closure on February 23rd 2022 (data cut-off date). In total, 54 of 240 planned patients were randomized (melflufen group, N=27; daratumumab group, N=27). Median progression-free survival (PFS) was not reached in the melflufen group versus 4.9 months in the daratumumab group (Hazard Ratio: 0.18 [95% Confidence Interval, 0.05-0.65]; P=0.0032) at a median follow-up time of 7.1 and 6.6 months, respectively. Overall response rate (ORR) was 59% in the melflufen group versus 30% in the daratumumab group (P=0.0300). The most common grade 3 treatment-emergent adverse events in the melflufen group versus daratumumab group were neutropenia (50% vs. 12%), thrombocytopenia (50% vs. 8%), and anemia (32% vs. 19%). Melflufen plus daratumumab and dexamethasone demonstrated superior PFS and ORR versus daratumumab in RRMM and a safety profile comparable to previously published melflufen studies.
Click to Show/Hide
|
||||
| Description |
The safety population included patients who received ≥1 dose of melflufen, daratumumab, or dexamethasone (melflufen group) and 26 patients who received daratumumab monotherapy. In the safety population, ≥1 TEAE was reported in 21 patients (96%) with melflufen, daratumumab, and dexamethasone and 22 patients (85%) with daratumumab. Overall, grade ≥3 TEAE occurred in 18 patients (82%) with melflufen, daratumumab, and dexamethasone and 14 patients (54%) with daratumumab. The most common hematologic grade ≥3 TEAE were neutropenia (melflufen group, 11 patients [50%]; daratumumab group, 3 patients [12%]), thrombocytopenia (melflufen group, 11 patients [50%]; daratumumab group, 2 patients [8%]), and anemia (melflufen group, 7 patients [32%]; daratumumab group, 5 patients [19%]). The most common non-hematologic grade ≥3 TEAE were pneumonia (melflufen group, 2 patients [9%]; daratumumab group, 2 patients [8%]) and femur fracture (melflufen group, 0 patients [0%]; daratumumab group, 2 patients [8%]); of these, 1 event (5%) of pneumonia in the melflufen group and 1 event (4%) of femur fracture in the daratumumab group were considered treatment-related TEAE by the investigator. Serious AE occurred in 6 patients (27%) with melflufen, daratumumab, and dexamethasone, and 12 patients (46%) with daratumumab. The most common serious AE (occurring in ≥4 patients overall) were anemia (melflufen group, 2 patients [9%]; daratumumab group, 3 patients [12%]) and pneumonia (melflufen group, 2 patients [9%]; daratumumab group, 2 patients [8%]). TEAE leading to treatment discontinuation occurred in 2 patients (9%) in the melflufen group (neutropenia and thrombocytopenia, N=1 each) and 4 patients (15%) in the daratumumab group (anemia, disease progression, hypercalcemia, and renal failure, N=1 each). Overall, 5 patients died on study before the crossover: 2 patients who received melflufen, daratumumab, and dexamethasone (1 due to disease progression and 1 due to unknown reasons, both >30 days after the last dose of study treatment) and 3 patients who received daratumumab (1 due to disease progression and 1 due to unknown reasons, both ≤30 days after the last dose of study treatment and 1 due to an AE [COVID-19 pneumonia], >30 days after the last dose of study treatment). In addition, one patient who crossed over to receive melflufen, daratumumab, and dexamethasone after progression on daratumumab died.
Click to Show/Hide
|
||||
| In Vivo Model | 22 relapsed/refractory multiple myeloma. | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT04649060 | Clinical Status | Phase 3 | ||
| Clinical Description | This was a randomized, controlled, open-label, Phase 3 multicenter study which enrolled patients with Relapsed-Refractory Multiple Myeloma (RRMM) who were either double refractory to an Immunomodulatory Drug (IMiD) and a Proteasome Inhibitor (PI) (regardless of the number of prior lines of therapy), or had received at least 3 prior lines of therapy including an IMiD and a PI. Patients received treatment with melflufen+dexamethasone+daratumumab or daratumumab until documented progressive disease, unacceptable toxicity, or patient/treating physician decision. Patients in the daratumumab treatment arm had the option to receive treatment with melflufen+dexamethasone+daratumumab after confirmed progressive disease. | ||||
| Experiment 350 Reporting the Activity Data of This PDC | [2] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Stable disease (SD) |
4%
|
|||
| MOA of PDC |
Melphalan flufenamide (melflufen), a first-in-class alkylating peptide-drug conjugate, plus dexamethasone was approved in Europe for use in patients with triple-class refractory relapsed/refractory multiple myeloma (RRMM) with 3 prior lines of therapy and without prior autologous stem cell transplantation (ASCT) or with a time to progression >36 months after prior ASCT. The randomized LIGHTHOUSE study (NCT04649060) assessed melflufen plus daratumumab and dexamethasone (melflufen group) versus daratumumab in patients with RRMM with disease refractory to an immunomodulatory agent and a proteasome inhibitor or who had received 3 prior lines of therapy including an immunomodulatory agent and a proteasome inhibitor. A partial clinical hold issued by the US Food and Drug Administration for all melflufen studies led to financial constraints and premature study closure on February 23rd 2022 (data cut-off date). In total, 54 of 240 planned patients were randomized (melflufen group, N=27; daratumumab group, N=27). Median progression-free survival (PFS) was not reached in the melflufen group versus 4.9 months in the daratumumab group (Hazard Ratio: 0.18 [95% Confidence Interval, 0.05-0.65]; P=0.0032) at a median follow-up time of 7.1 and 6.6 months, respectively. Overall response rate (ORR) was 59% in the melflufen group versus 30% in the daratumumab group (P=0.0300). The most common grade 3 treatment-emergent adverse events in the melflufen group versus daratumumab group were neutropenia (50% vs. 12%), thrombocytopenia (50% vs. 8%), and anemia (32% vs. 19%). Melflufen plus daratumumab and dexamethasone demonstrated superior PFS and ORR versus daratumumab in RRMM and a safety profile comparable to previously published melflufen studies.
Click to Show/Hide
|
||||
| Description |
In the ITT population, with a median follow-up of 7.1 months in the melflufen group, the median PFS was not reached (NR) and with a median follow-up of 6.6 months in the daratumumab group, the median PFS was 4.9 months (95% CI: 3.4-NR; HR: 0.18 [95% CI: 0.05-0.65]; log-rankP=0.0032). OS was immature, with 2 events (7%) in the melflufen group and 4 events (15%) in the daratumumab group (HR: 0.47 [95% CI: 0.09-2.57]; log-rankP=0.3721) at a median follow-up of 7.6 months and 6.6 months, respectively. The ORR was 59% (95% CI: 39-78) in the melflufen group and 30% (95% CI: 14-50) in the daratumumab group (P=0.0300). More patients in the melflufen group had a complete response (CR; 1 patient [4%]vs. 0 patients [0%]) and very good partial response (VGPR; 4 patients [15%]vs. 3 patients [11%]) compared with the daratumumab group.
Click to Show/Hide
|
||||
| In Vivo Model | 27 Intent-to-treat (ITT) population. | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT04649060 | Clinical Status | Phase 3 | ||
| Clinical Description | This was a randomized, controlled, open-label, Phase 3 multicenter study which enrolled patients with Relapsed-Refractory Multiple Myeloma (RRMM) who were either double refractory to an Immunomodulatory Drug (IMiD) and a Proteasome Inhibitor (PI) (regardless of the number of prior lines of therapy), or had received at least 3 prior lines of therapy including an IMiD and a PI. Patients received treatment with melflufen+dexamethasone+daratumumab or daratumumab until documented progressive disease, unacceptable toxicity, or patient/treating physician decision. Patients in the daratumumab treatment arm had the option to receive treatment with melflufen+dexamethasone+daratumumab after confirmed progressive disease. | ||||
| Experiment 351 Reporting the Activity Data of This PDC | [2] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Stable disease (SD) |
7%
|
|||
| Patients Enrolled |
14 patients no prior ASCT or TTP >36 months after ASCT.
|
||||
| MOA of PDC |
Melphalan flufenamide (melflufen), a first-in-class alkylating peptide-drug conjugate, plus dexamethasone was approved in Europe for use in patients with triple-class refractory relapsed/refractory multiple myeloma (RRMM) with 3 prior lines of therapy and without prior autologous stem cell transplantation (ASCT) or with a time to progression >36 months after prior ASCT. The randomized LIGHTHOUSE study (NCT04649060) assessed melflufen plus daratumumab and dexamethasone (melflufen group) versus daratumumab in patients with RRMM with disease refractory to an immunomodulatory agent and a proteasome inhibitor or who had received 3 prior lines of therapy including an immunomodulatory agent and a proteasome inhibitor. A partial clinical hold issued by the US Food and Drug Administration for all melflufen studies led to financial constraints and premature study closure on February 23rd 2022 (data cut-off date). In total, 54 of 240 planned patients were randomized (melflufen group, N=27; daratumumab group, N=27). Median progression-free survival (PFS) was not reached in the melflufen group versus 4.9 months in the daratumumab group (Hazard Ratio: 0.18 [95% Confidence Interval, 0.05-0.65]; P=0.0032) at a median follow-up time of 7.1 and 6.6 months, respectively. Overall response rate (ORR) was 59% in the melflufen group versus 30% in the daratumumab group (P=0.0300). The most common grade 3 treatment-emergent adverse events in the melflufen group versus daratumumab group were neutropenia (50% vs. 12%), thrombocytopenia (50% vs. 8%), and anemia (32% vs. 19%). Melflufen plus daratumumab and dexamethasone demonstrated superior PFS and ORR versus daratumumab in RRMM and a safety profile comparable to previously published melflufen studies.
Click to Show/Hide
|
||||
| Description |
Efficacy endpoints were more pronounced in favor of the melflufen group compared with the daratumumab group among patients with no prior ASCT or TTP >36 months after a prior ASCT (melflufen group, N=14; daratumumab group, N=15). Median PFS was NR in the melflufen group and 3.9 months (95% CI: 1.4-4.9) in the daratumumab group (HR, 0.06 [95% CI: 0.01-0.49]; log-rank P=0.0005). Fewer OS events were reported in the melflufen group (1 event [7%] vs. 4 events [27%] in the daratumumab group; log-rank P=0.0369). The ORR was 64% (95% CI: 35-87) in the melflufen group and 13% (95% CI: 2-41) in the daratumumab group (P=0.0055). More patients in the melflufen group had a CR (1 patient [7%] vs. 0 patients [0%]) or VGPR (2 patients [14%] vs. 1 patient [7%]) compared with the daratumumab group.
Click to Show/Hide
|
||||
| Related Clinical Trial | |||||
| NCT Number | NCT04649060 | Clinical Status | Phase 3 | ||
| Clinical Description | This was a randomized, controlled, open-label, Phase 3 multicenter study which enrolled patients with Relapsed-Refractory Multiple Myeloma (RRMM) who were either double refractory to an Immunomodulatory Drug (IMiD) and a Proteasome Inhibitor (PI) (regardless of the number of prior lines of therapy), or had received at least 3 prior lines of therapy including an IMiD and a PI. Patients received treatment with melflufen+dexamethasone+daratumumab or daratumumab until documented progressive disease, unacceptable toxicity, or patient/treating physician decision. Patients in the daratumumab treatment arm had the option to receive treatment with melflufen+dexamethasone+daratumumab after confirmed progressive disease. | ||||
| Experiment 352 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Stable disease (SD) |
14.30%
|
|||
| Patients Enrolled |
14 patients with relapsed refractory multiple myeloma.
|
||||
| Administration Time | 28-day cycle | ||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (melflufen) is a first-in-class peptide-drug conjugate that utilizes increased peptidase expression to selectively release potent alkylating agents inside tumor cells. Melflufen is hydrolyzed by peptidases and esterases to melphalan either directly or through an intermediate metabolite, desethyl-melflufen. The high lipophilicity of melflufen facilitates passive diffusion across cell membranes. The activity and tolerability of melflufen in relapsed/refractory multiple myeloma (RRMM) were demonstrated in the O-12-M1 (NCT01897714), OCEAN (NCT03151811), and HORIZON (NCT02963493) trials.
Click to Show/Hide
|
||||
| Description |
In Arm A, 4 of the 14 patients achieved an overall response (ORR 28.6% [95% CI: 8.4-58.1]) including 1 patient with CR, and the CBR was 57.1% (95% CI: 28.9-82.3). In Arm B, 1 of the 13 patients achieved an overall response (ORR 7.7% [95% CI: 0.2-36.0]), consisting of a PR, and the CBR was 15.4% (95% CI: 1.9-45.4). In the overall study population, 5 patients had an overall response (ORR 18.5% [95% CI: 6.3-38.1]). DOR data were insufficient to evaluate due to early termination of the study, the low number of patient events (1 in Arm A, 0 in Arm B), and the limited number of responses. Based on the 5 patients who had a response of PR or better at study termination (4 in Arm A, 1 in Arm B), the median TTR was 2.4 months in Arm A, 5.1 months in Arm B, and 2.6 months overall. Based on the 8 and 5 progression events in Arm A and Arm B, respectively, the median TTP was 5.8 months and 4.8 months, respectively, with a median TTP of 5.8 months in the overall population. The median PFS was 5.2 months (95% CI: 2.7 to not evaluable) and 2.9 months (95% CI: 1.5-4.6) in Arms A and B, respectively. For the overall study population, median PFS was 3.7 months (95% CI: 2.7-5.8).
Click to Show/Hide
|
||||
| Half life period | 75.6 h | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT04412707 | Clinical Status | Phase 2 | ||
| Clinical Description | This is a randomized, two-period, cross-over Phase 2 study, comparing PK, and assessing safety and tolerability and efficacy of peripheral and central intravenous administration of melflufen in patients with RRMM. It is an international study, enrolling patients in US and Europe. The study will enroll patients following at least 2 lines of prior therapy. | ||||
| Experiment 353 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Stable disease (SD) |
24%
|
|||
| Patients Enrolled |
246 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 354 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Stable disease (SD) |
28%
|
|||
| Patients Enrolled |
246 patients with multiple myeloma refractory to lenalidomide.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (known as melflufen) is a first-in-class peptide-drug conjugate that targets aminopeptidases and thereby rapidly releases alkylating agents inside tumour cells. Due to its high lipophilicity and affinity for aminopeptidases, melflufen can passively enter tumour cells and release cytotoxic, hydrophilic alkylating agents (melphalan and desethyl-melflufen) that remain trapped within cells. Melflufen uses a novel approach, whereby increased aminopeptidase activity is used to achieve selective release of alkylating agents inside tumour cells.
Click to Show/Hide
|
||||
| Description |
In the safety population, the median duration of treatment was 58 months (IQR 28-111) in the melflufen group and 51 months (26-92) in the pomalidomide group. Patients received a median of five treatment cycles in each treatment group (melflufen: IQR 3-11; pomalidomide: IQR 3-10). The most common treatment-emergent adverse events by preferred term and treatment group are summarised in table 2 and the appendix (pp 23-31 ), and disaggregated by sex in the appendix (pp 32-35 ). The most common haematological grade 3 or 4 events in the melflufen and pomalidomide groups were neutropenia (123 [54%] of 228 vs 102 [41%] of 246), thrombocytopenia (143 [63%] vs 26 [11%]), and anaemia (97 [43%] vs 44 [18%]), and the most common grade 3 or 4 non-haematological event was pneumonia (ten [4%] vs 20 [8%]). The most common grade 3 or 4 treatment-related treatment-emergent adverse events in the melflufen and pomalidomide groups were thrombocytopenia (138 [61%] vs 22 [9%]), neutropenia (122 [54%] vs 97 [39%]), anaemia (87 [38%] vs 25 [10%] ). Serious treatment-emergent adverse events occurred in 95 (42%) patients in the melflufen group and 113 (46%) patients in the pomalidomide group, the most common of which were pneumonia (13 [6%] vs 21 [9%]), COVID-19 pneumonia (11 [5%] vs nine [4%]), and thrombocytopenia (nine [4%] vs three [1%]), and were considered to be treatment related in 42 (18%) in the melflufen group and 52 (21%) in the pomalidomide group. In the safety population, 106 (46%) patients in the melflufen group and 106 (43%) patients in the pomalidomide group died overall. 23 (10%) patients in the melflufen group and 33 (13%) in the pomalidomide group died within 30 days of receiving their last dose of study drug; 83 (36%) in the melflufen group and 73 (30%), in the pomalidomide group died 30 days after having received their last dose of study medication. Additionally, 13 patients who were randomly assigned but not treated died (assigned to melflufen group, 11 [61%] of 18; pomalidomide group, two [67%] of three). In an exploratory analysis of prespecified subgroups of clinical relevance in the ITT population, progression-free survival data favoured melflufen in most subgroups, including patients aged 75 years and older (HR 043 [95% CI 024-076]; p=00031) and patients without a previous autologous HSCT (HR 059 [044-079]; p=00004). By contrast, overall survival data favoured pomalidomide in patients younger than 65 years (HR 171 [95% CI 109-269]; p=0019) and those with a previous autologous HSCT (HR 161 [109-240]; p=0017). Age and previous autologous HSCT remained significant prognostic factors on the basis of an interaction test.
Click to Show/Hide
|
||||
| Experiment 355 Reporting the Activity Data of This PDC | [2] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Thrombocytopenia |
50%
|
|||
| MOA of PDC |
Melphalan flufenamide (melflufen), a first-in-class alkylating peptide-drug conjugate, plus dexamethasone was approved in Europe for use in patients with triple-class refractory relapsed/refractory multiple myeloma (RRMM) with 3 prior lines of therapy and without prior autologous stem cell transplantation (ASCT) or with a time to progression >36 months after prior ASCT. The randomized LIGHTHOUSE study (NCT04649060) assessed melflufen plus daratumumab and dexamethasone (melflufen group) versus daratumumab in patients with RRMM with disease refractory to an immunomodulatory agent and a proteasome inhibitor or who had received 3 prior lines of therapy including an immunomodulatory agent and a proteasome inhibitor. A partial clinical hold issued by the US Food and Drug Administration for all melflufen studies led to financial constraints and premature study closure on February 23rd 2022 (data cut-off date). In total, 54 of 240 planned patients were randomized (melflufen group, N=27; daratumumab group, N=27). Median progression-free survival (PFS) was not reached in the melflufen group versus 4.9 months in the daratumumab group (Hazard Ratio: 0.18 [95% Confidence Interval, 0.05-0.65]; P=0.0032) at a median follow-up time of 7.1 and 6.6 months, respectively. Overall response rate (ORR) was 59% in the melflufen group versus 30% in the daratumumab group (P=0.0300). The most common grade 3 treatment-emergent adverse events in the melflufen group versus daratumumab group were neutropenia (50% vs. 12%), thrombocytopenia (50% vs. 8%), and anemia (32% vs. 19%). Melflufen plus daratumumab and dexamethasone demonstrated superior PFS and ORR versus daratumumab in RRMM and a safety profile comparable to previously published melflufen studies.
Click to Show/Hide
|
||||
| Description |
The safety population included patients who received ≥1 dose of melflufen, daratumumab, or dexamethasone (melflufen group) and 26 patients who received daratumumab monotherapy. In the safety population, ≥1 TEAE was reported in 21 patients (96%) with melflufen, daratumumab, and dexamethasone and 22 patients (85%) with daratumumab. Overall, grade ≥3 TEAE occurred in 18 patients (82%) with melflufen, daratumumab, and dexamethasone and 14 patients (54%) with daratumumab. The most common hematologic grade ≥3 TEAE were neutropenia (melflufen group, 11 patients [50%]; daratumumab group, 3 patients [12%]), thrombocytopenia (melflufen group, 11 patients [50%]; daratumumab group, 2 patients [8%]), and anemia (melflufen group, 7 patients [32%]; daratumumab group, 5 patients [19%]). The most common non-hematologic grade ≥3 TEAE were pneumonia (melflufen group, 2 patients [9%]; daratumumab group, 2 patients [8%]) and femur fracture (melflufen group, 0 patients [0%]; daratumumab group, 2 patients [8%]); of these, 1 event (5%) of pneumonia in the melflufen group and 1 event (4%) of femur fracture in the daratumumab group were considered treatment-related TEAE by the investigator. Serious AE occurred in 6 patients (27%) with melflufen, daratumumab, and dexamethasone, and 12 patients (46%) with daratumumab. The most common serious AE (occurring in ≥4 patients overall) were anemia (melflufen group, 2 patients [9%]; daratumumab group, 3 patients [12%]) and pneumonia (melflufen group, 2 patients [9%]; daratumumab group, 2 patients [8%]). TEAE leading to treatment discontinuation occurred in 2 patients (9%) in the melflufen group (neutropenia and thrombocytopenia, N=1 each) and 4 patients (15%) in the daratumumab group (anemia, disease progression, hypercalcemia, and renal failure, N=1 each). Overall, 5 patients died on study before the crossover: 2 patients who received melflufen, daratumumab, and dexamethasone (1 due to disease progression and 1 due to unknown reasons, both >30 days after the last dose of study treatment) and 3 patients who received daratumumab (1 due to disease progression and 1 due to unknown reasons, both ≤30 days after the last dose of study treatment and 1 due to an AE [COVID-19 pneumonia], >30 days after the last dose of study treatment). In addition, one patient who crossed over to receive melflufen, daratumumab, and dexamethasone after progression on daratumumab died.
Click to Show/Hide
|
||||
| In Vivo Model | 22 relapsed/refractory multiple myeloma. | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT04649060 | Clinical Status | Phase 3 | ||
| Clinical Description | This was a randomized, controlled, open-label, Phase 3 multicenter study which enrolled patients with Relapsed-Refractory Multiple Myeloma (RRMM) who were either double refractory to an Immunomodulatory Drug (IMiD) and a Proteasome Inhibitor (PI) (regardless of the number of prior lines of therapy), or had received at least 3 prior lines of therapy including an IMiD and a PI. Patients received treatment with melflufen+dexamethasone+daratumumab or daratumumab until documented progressive disease, unacceptable toxicity, or patient/treating physician decision. Patients in the daratumumab treatment arm had the option to receive treatment with melflufen+dexamethasone+daratumumab after confirmed progressive disease. | ||||
| Experiment 356 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Thrombocytopenia |
71.40%
|
|||
| Patients Enrolled |
14 patients with relapsed refractory multiple myeloma.
|
||||
| Administration Time | 28-day cycle | ||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (melflufen) is a first-in-class peptide-drug conjugate that utilizes increased peptidase expression to selectively release potent alkylating agents inside tumor cells. Melflufen is hydrolyzed by peptidases and esterases to melphalan either directly or through an intermediate metabolite, desethyl-melflufen. The high lipophilicity of melflufen facilitates passive diffusion across cell membranes. The activity and tolerability of melflufen in relapsed/refractory multiple myeloma (RRMM) were demonstrated in the O-12-M1 (NCT01897714), OCEAN (NCT03151811), and HORIZON (NCT02963493) trials.
Click to Show/Hide
|
||||
| Description |
Overall, at least one TEAE was reported in 13 (92.9%) and 13 (100.0%) patients in Arms A and B, respectively (Table 3). During cycle 1, 9 patients (64.3%) and 12 patients (92.3%), respectively, had at least one TEAE. Cumulatively, grade 3 or 4 AEs occurred in 12 (85.7%) and 12 (92.3%) patients, respectively, and serious AEs were reported in 5 (35.7%) and 9 (69.2%) patients, respectively. The most common any-grade AEs in Arms A and B, respectively, were thrombocytopenia (10 [71.4%]; 10 [76.9%]), neutropenia (9 [64.3%]; 9 [69.2%]), and anemia (9 [64.3%]; 7 [53.8%]). No phlebitis or local-infusion-related reactions were reported based on pre- and post-infusion inspection of the IV site, and there were no extravasations observed in Arm A or B. Similarly, VIP scores collected on Day 1 post-infusion and on Day 8 indicated that patients had healthy IV sites (VIP score of 0) with no signs of phlebitis following PVC administration of melflufen. The most common non-hematological AE was positive SARS-CoV-2 test (Arm A: 2 [14.3%]; Arm B: 4 [30.8%]). Pneumonia was the most common serious AE (Arm A: 2 [14.3%]; Arm B: 2 [15.4%]). The most common AE considered related to melflufen and/or dexamethasone by investigators was thrombocytopenia (Arm A: 10 [71.4%]; Arm B: 10 [76.9%]). AEs led to treatment discontinuation in 3 (21.4%) and 6 (46.2%) patients in Arms A and B, respectively.
Click to Show/Hide
|
||||
| Half life period | 75.6 h | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT04412707 | Clinical Status | Phase 2 | ||
| Clinical Description | This is a randomized, two-period, cross-over Phase 2 study, comparing PK, and assessing safety and tolerability and efficacy of peripheral and central intravenous administration of melflufen in patients with RRMM. It is an international study, enrolling patients in US and Europe. The study will enroll patients following at least 2 lines of prior therapy. | ||||
| Experiment 357 Reporting the Activity Data of This PDC | [4] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Thrombocytopenia |
76.00%
|
|||
| Patients Enrolled |
157 patients with multiple myeloma.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melflufen is a first-in-class peptide-drug conjugate, targeting aminopeptidase which has an increased expression in fast-growing and aggressive malignancies. The lipophilicity of melflufen allows for passive diffusion, selectively targeting myeloma cells. Once inside the cell, melflufen is hydrolyzed to active alkylating metabolites melphalan and desethyl-melflufen. Melflufen and the active metabolites trigger irreversible DNA damage, inhibit proliferation, induces apoptosis, and express antiangiogenic effects. In addition, melflufen demonstrated activity in myeloma cells with documented impaired or absent Tp53 expression and documented resistance to bortezomib, dexamethasone, and melphalan.
Click to Show/Hide
|
||||
| Description |
Based on the safety data collected during the HORIZON trial, treatment emergent adverse events occurred in 100% of patients including 100 patients (64%) having at least 1 CTCAE grade 4 adverse effect. Hematologic grade 3 or 4 adverse effects including thrombocytopenia (76%), neutropenia (79%), anemia (43%), and infections (11%) were the most commonly reported. Other adverse effects, such as fatigue (55%), nausea (32%), diarrhea (27%), and decreased appetite (14%), were similar to other alkylating agents. Pyrexia (24%), including febrile neutropenia (5%), and respiratory tract infections (24%) were contributed to hematologic toxicities.
Click to Show/Hide
|
||||
| Experiment 358 Reporting the Activity Data of This PDC | [9] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Thrombocytopenia |
70%
|
|||
| Patients Enrolled |
145 patients who has relapsed/refractory multiple myeloma with no previous ASCT or TTP >36 month Post-ASCTa.
|
||||
| MOA of PDC |
In summary, the interpretation of the results from the OCEAN study were impacted by the heterogeneity of the population, with age and previous success of ASCT therapy identified as prognostic factors with study therapies. The safety profile of melflufen and dexamethasone is primarily characterized by hematologic AEs that are clinically manageable. Observed infection rates, which included COVID-19, were generally low. Taken together, these data support the use of melflufen and dexamethasone in patients who have not received a previous ASCT or who underwent a successful ASCT (ie, TTP >36 months post-ASCT). In addition, the favorable efficacy profile and convenience of monthly outpatient infusions, especially for patients without access to other therapeutics such as CAR T-cell therapy or bispecific antibodies, bode well for this combination translating successfully into real-world practice.
Click to Show/Hide
|
||||
| Description |
Given the prognostic importance of TTP <36 months post-ASCT in OCEAN, we evaluated this prognostic factor in a post hoc analysis from the HORIZON study. Among 110 patients with triple-class refractory disease who had received ≥3 prior lines of therapy, 77 (70%) had received a previous ASCT and 58 (53%) had TTP <36 months post-ASCT (Suppl. Table S3). In patients with a TTP >36 months post-ASCT or no ASCT versus patients with a TTP <36 months post-ASCT, ORR was higher (29% vs 22%; Suppl. Table S4) and median DOR (7.6 months vs 3.9 months) and median PFS (4.2 months vs 3.4 months) were longer. Since pomalidomide and lenalidomide both belong to the immunomodulatory drugs, we analyzed if the duration of previous treatment with lenalidomide could have impacted the results. The median duration of lenalidomide was 14.4 months in patients with ASCT and TTP < 36 months, 38.3 months in patients with ASCT and TTP > 36 months, and 14.6 months in patients with no previous ASCT. However, the median PFS for patients treated with pomalidomide did not differ substantially between these groups of patients. The safety profile of melflufen and dexamethasone was generally consistent between patients with a TTP >36 months post-ASCT or no ASCT and patients with a TTP <36 months post-ASCT. In OCEAN among the melflufen group, the frequency of grade 3/4 TEAEs (88% and 92%), serious TEAEs (44% and 38%), and fatal adverse events (AEs; 11% and 13%) was similar in patients with a TTP >36 months post-ASCT or no ASCT and patients with TTP <36 months. However, patients with a TTP >36 months post-ASCT or no ASCT had lower rates of TEAEs leading to treatment discontinuation (23% and 31%), the longer median duration of study treatment (35.1 weeks vs 15.1 weeks), and longer median time to experiencing grade 3/4 thrombocytopenia (11.2 weeks vs 4.1 weeks) and grade 3/4 neutropenia (4.8 weeks vs 2.1 weeks) than patients with a TTP <36 months post-ASCT. In HORIZON, patients with a TTP >36 months post-ASCT or no ASCT had lower rates of grade 3/4 TEAEs (88% and 98%), but higher rates of serious TEAEs (64% and 53%) and similar rates of TEAEs leading to treatment discontinuation (29% and 33%) than patients with a TTP <36 months post-ASCT.
Click to Show/Hide
|
||||
| Experiment 359 Reporting the Activity Data of This PDC | [1] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Thrombocytopenia |
73.00%
|
|||
| Patients Enrolled |
Patients with multi-refractory multiple myeloma.
|
||||
| MOA of PDC |
Melflufen is highly lipophilic, which promotes its rapid uptake by cells. Once within the cell, melflufen releases its hydrophilic alkylator payloads via the hydrolytic activity of intracellular peptidases (e.g., aminopeptidases). Aminopeptidases are Zn2+-dependent metalloproteinases that remove amino acids at the N-terminal position from oligopeptides and have been associated with multiple tumorigenic processes such as proliferation, apoptosis, differentiation, angiogenesis, and motility. The dependence of melflufen on aminopeptidases was initially demonstrated by the reduced cytotoxic activity of melflufen-but not the alkylator melphalan-when cells were pretreated with bestatin, an antibiotic that is a potent aminopeptidase inhibitor. In addition, structure analogs designed to resist peptide hydrolysis (N-methyl derivative and derivative with D-amino acid) were shown to be almost 100-fold less potent than melflufen. Subsequent in vitro studies demonstrated that hydrolytic cleavage of melflufen by aminopeptidases releases alkylator payloads, including melphalan. In vitro, the activity of melflufen is multi-pronged, including induction of DNA damage, induction of apoptosis, inhibition of VEGF-dependent cell migration, and inhibition of tumor-associated angiogenesis, which have been further reviewed elsewhere. Downregulation of aminopeptidases resulted in reduced melflufen-mediated cytotoxic activity and apoptotic signaling in cultured cells.
Click to Show/Hide
|
||||
| Description |
Melflufen plus dexamethasone was generally manageable in this heavily pretreated patient population [51]. All patients experienced ≥1 AE, most commonly hematologic AEs including thrombocytopenia (73%), neutropenia (69%), and anemia (64%). The most common non-hematologic AEs included pyrexia (40%), asthenia (31%), fatigue (29%), nausea (27%), and diarrhea (24%).
Click to Show/Hide
|
||||
| Experiment 360 Reporting the Activity Data of This PDC | [5] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Thrombocytopenia |
73.97%
|
|||
| Patients Enrolled |
153 patients refractory to prior alkylators (melflufen, n=78; pomalidomide, n=75).
|
||||
| MOA of PDC |
Melphalan flufenamide (melflufen), a first-in-class alkylating peptide-drug conjugate, plus dexamethasone demonstrated superior progression-free survival (PFS), but not overall survival (OS), versus pomalidomide plus dexamethasone in relapsed/refractory multiple myeloma in the OCEAN study. Time to progression (TTP) <36 months after a prior autologous stem cell transplantation (ASCT) was a negative prognostic factor for OS with melflufen. This post hoc exploratory analysis evaluated patients refractory to prior alkylators (e.g., cyclophosphamide and melphalan) in OCEAN. In 153 patients refractory to prior alkylators (melflufen, n = 78; pomalidomide, n = 75), the melflufen and pomalidomide arms had similar median PFS (5.6 months [95% CI, 4.2-8.3] vs. 4.7 months [95% CI, 3.1-7.3]; hazard ratio [HR], 0.92 [95% CI, 0.63-1.33]) and OS (23.4 months [95% CI, 14.4-31.7] vs. 20.0 months [95% CI, 12.0-28.7]; HR, 0.92 [95% CI, 0.62-1.38]). Among alkylator-refractory patients with a TTP 36 months after a prior ASCT or no prior ASCT (melflufen, n = 54; pomalidomide, n = 53), the observed median PFS and OS were longer in the melflufen arm than the pomalidomide arm. The safety profile of melflufen was consistent with previous reports. These results suggest that melflufen is safe and effective in patients with alkylator-refractory disease, suggesting differentiated activity from other alkylators.
Click to Show/Hide
|
||||
| Description |
Overall, the safety profile of melflufen plus dexamethasone in the alkylator-refractory group was consistent between treatment arms (Table 2). In the melflufen and pomalidomide arms, respectively, the frequency of treatment-emergent adverse events (TEAEs; 99% vs. 97%), Grade 3 or 4 TEAEs (85% vs. 82%), serious TEAEs (49% vs. 53%), and fatal TEAEs (19% vs. 16%) were similar (Table 2). However, melflufen compared with pomalidomide saw more dose modifications (76% vs. 67%) and dose reductions (47% vs. 14%), comparable dose delays (57% vs. 51%) but less treatment discontinuation (27% vs. 34%). When comparing patients refractory and not refractory to prior alkylators, rates of TEAEs were generally comparable except for slightly lower rates of serious and fatal TEAEs observed in patients not refractory to alkylators. Among Grade 3 or 4 TEAEs of special interest, melflufen saw more thrombocytopenia (73% vs. 14%), neutropenia (65% vs. 55%), and leukopenia or white blood cell decrease (14% vs. 3%), but less infection (15% vs. 26%), than pomalidomide. Notably, melflufen compared with pomalidomide saw a longer median time to dose reduction (106 days [range, 28-443] vs. 47 days [range, 28-225]), Grade 3 or 4 thrombocytopenia (52 days [range, 15-451] vs. 19 days [range, 8-91]), and Grade 3 or 4 neutropenia (36 days [range, 8-561] vs. 22 days [range, 8-470]).
Click to Show/Hide
|
||||
| Experiment 361 Reporting the Activity Data of This PDC | [9] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Thrombocytopenia |
86%
|
|||
| Patients Enrolled |
101 relapsed/refractory multiple myeloma patients with TTP <36 month Post-ASCTb.
|
||||
| MOA of PDC |
In summary, the interpretation of the results from the OCEAN study were impacted by the heterogeneity of the population, with age and previous success of ASCT therapy identified as prognostic factors with study therapies. The safety profile of melflufen and dexamethasone is primarily characterized by hematologic AEs that are clinically manageable. Observed infection rates, which included COVID-19, were generally low. Taken together, these data support the use of melflufen and dexamethasone in patients who have not received a previous ASCT or who underwent a successful ASCT (ie, TTP >36 months post-ASCT). In addition, the favorable efficacy profile and convenience of monthly outpatient infusions, especially for patients without access to other therapeutics such as CAR T-cell therapy or bispecific antibodies, bode well for this combination translating successfully into real-world practice.
Click to Show/Hide
|
||||
| Description |
Given the prognostic importance of TTP <36 months post-ASCT in OCEAN, we evaluated this prognostic factor in a post hoc analysis from the HORIZON study. Among 110 patients with triple-class refractory disease who had received ≥3 prior lines of therapy, 77 (70%) had received a previous ASCT and 58 (53%) had TTP <36 months post-ASCT (Suppl. Table S3). In patients with a TTP >36 months post-ASCT or no ASCT versus patients with a TTP <36 months post-ASCT, ORR was higher (29% vs 22%; Suppl. Table S4) and median DOR (7.6 months vs 3.9 months) and median PFS (4.2 months vs 3.4 months) were longer. Since pomalidomide and lenalidomide both belong to the immunomodulatory drugs, we analyzed if the duration of previous treatment with lenalidomide could have impacted the results. The median duration of lenalidomide was 14.4 months in patients with ASCT and TTP < 36 months, 38.3 months in patients with ASCT and TTP > 36 months, and 14.6 months in patients with no previous ASCT. However, the median PFS for patients treated with pomalidomide did not differ substantially between these groups of patients. The safety profile of melflufen and dexamethasone was generally consistent between patients with a TTP >36 months post-ASCT or no ASCT and patients with a TTP <36 months post-ASCT. In OCEAN among the melflufen group, the frequency of grade 3/4 TEAEs (88% and 92%), serious TEAEs (44% and 38%), and fatal adverse events (AEs; 11% and 13%) was similar in patients with a TTP >36 months post-ASCT or no ASCT and patients with TTP <36 months. However, patients with a TTP >36 months post-ASCT or no ASCT had lower rates of TEAEs leading to treatment discontinuation (23% and 31%), the longer median duration of study treatment (35.1 weeks vs 15.1 weeks), and longer median time to experiencing grade 3/4 thrombocytopenia (11.2 weeks vs 4.1 weeks) and grade 3/4 neutropenia (4.8 weeks vs 2.1 weeks) than patients with a TTP <36 months post-ASCT. In HORIZON, patients with a TTP >36 months post-ASCT or no ASCT had lower rates of grade 3/4 TEAEs (88% and 98%), but higher rates of serious TEAEs (64% and 53%) and similar rates of TEAEs leading to treatment discontinuation (29% and 33%) than patients with a TTP <36 months post-ASCT.
Click to Show/Hide
|
||||
| Experiment 362 Reporting the Activity Data of This PDC | [5] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Thrombocytopenia concurrent with grade 3/4 bleeding |
100%
|
|||
| Patients Enrolled |
153 patients refractory to prior alkylators (melflufen, n=78; pomalidomide, n=75).
|
||||
| MOA of PDC |
Melphalan flufenamide (melflufen), a first-in-class alkylating peptide-drug conjugate, plus dexamethasone demonstrated superior progression-free survival (PFS), but not overall survival (OS), versus pomalidomide plus dexamethasone in relapsed/refractory multiple myeloma in the OCEAN study. Time to progression (TTP) <36 months after a prior autologous stem cell transplantation (ASCT) was a negative prognostic factor for OS with melflufen. This post hoc exploratory analysis evaluated patients refractory to prior alkylators (e.g., cyclophosphamide and melphalan) in OCEAN. In 153 patients refractory to prior alkylators (melflufen, n = 78; pomalidomide, n = 75), the melflufen and pomalidomide arms had similar median PFS (5.6 months [95% CI, 4.2-8.3] vs. 4.7 months [95% CI, 3.1-7.3]; hazard ratio [HR], 0.92 [95% CI, 0.63-1.33]) and OS (23.4 months [95% CI, 14.4-31.7] vs. 20.0 months [95% CI, 12.0-28.7]; HR, 0.92 [95% CI, 0.62-1.38]). Among alkylator-refractory patients with a TTP 36 months after a prior ASCT or no prior ASCT (melflufen, n = 54; pomalidomide, n = 53), the observed median PFS and OS were longer in the melflufen arm than the pomalidomide arm. The safety profile of melflufen was consistent with previous reports. These results suggest that melflufen is safe and effective in patients with alkylator-refractory disease, suggesting differentiated activity from other alkylators.
Click to Show/Hide
|
||||
| Description |
Overall, the safety profile of melflufen plus dexamethasone in the alkylator-refractory group was consistent between treatment arms (Table 2). In the melflufen and pomalidomide arms, respectively, the frequency of treatment-emergent adverse events (TEAEs; 99% vs. 97%), Grade 3 or 4 TEAEs (85% vs. 82%), serious TEAEs (49% vs. 53%), and fatal TEAEs (19% vs. 16%) were similar (Table 2). However, melflufen compared with pomalidomide saw more dose modifications (76% vs. 67%) and dose reductions (47% vs. 14%), comparable dose delays (57% vs. 51%) but less treatment discontinuation (27% vs. 34%). When comparing patients refractory and not refractory to prior alkylators, rates of TEAEs were generally comparable except for slightly lower rates of serious and fatal TEAEs observed in patients not refractory to alkylators. Among Grade 3 or 4 TEAEs of special interest, melflufen saw more thrombocytopenia (73% vs. 14%), neutropenia (65% vs. 55%), and leukopenia or white blood cell decrease (14% vs. 3%), but less infection (15% vs. 26%), than pomalidomide. Notably, melflufen compared with pomalidomide saw a longer median time to dose reduction (106 days [range, 28-443] vs. 47 days [range, 28-225]), Grade 3 or 4 thrombocytopenia (52 days [range, 15-451] vs. 19 days [range, 8-91]), and Grade 3 or 4 neutropenia (36 days [range, 8-561] vs. 22 days [range, 8-470]).
Click to Show/Hide
|
||||
| Experiment 363 Reporting the Activity Data of This PDC | [9] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Thrombocytopenia concurrent with hemorrhage |
0%
|
|||
| Patients Enrolled |
101 relapsed/refractory multiple myeloma patients with TTP <36 month Post-ASCTb.
|
||||
| MOA of PDC |
In summary, the interpretation of the results from the OCEAN study were impacted by the heterogeneity of the population, with age and previous success of ASCT therapy identified as prognostic factors with study therapies. The safety profile of melflufen and dexamethasone is primarily characterized by hematologic AEs that are clinically manageable. Observed infection rates, which included COVID-19, were generally low. Taken together, these data support the use of melflufen and dexamethasone in patients who have not received a previous ASCT or who underwent a successful ASCT (ie, TTP >36 months post-ASCT). In addition, the favorable efficacy profile and convenience of monthly outpatient infusions, especially for patients without access to other therapeutics such as CAR T-cell therapy or bispecific antibodies, bode well for this combination translating successfully into real-world practice.
Click to Show/Hide
|
||||
| Description |
Given the prognostic importance of TTP <36 months post-ASCT in OCEAN, we evaluated this prognostic factor in a post hoc analysis from the HORIZON study. Among 110 patients with triple-class refractory disease who had received ≥3 prior lines of therapy, 77 (70%) had received a previous ASCT and 58 (53%) had TTP <36 months post-ASCT (Suppl. Table S3). In patients with a TTP >36 months post-ASCT or no ASCT versus patients with a TTP <36 months post-ASCT, ORR was higher (29% vs 22%; Suppl. Table S4) and median DOR (7.6 months vs 3.9 months) and median PFS (4.2 months vs 3.4 months) were longer. Since pomalidomide and lenalidomide both belong to the immunomodulatory drugs, we analyzed if the duration of previous treatment with lenalidomide could have impacted the results. The median duration of lenalidomide was 14.4 months in patients with ASCT and TTP < 36 months, 38.3 months in patients with ASCT and TTP > 36 months, and 14.6 months in patients with no previous ASCT. However, the median PFS for patients treated with pomalidomide did not differ substantially between these groups of patients. The safety profile of melflufen and dexamethasone was generally consistent between patients with a TTP >36 months post-ASCT or no ASCT and patients with a TTP <36 months post-ASCT. In OCEAN among the melflufen group, the frequency of grade 3/4 TEAEs (88% and 92%), serious TEAEs (44% and 38%), and fatal adverse events (AEs; 11% and 13%) was similar in patients with a TTP >36 months post-ASCT or no ASCT and patients with TTP <36 months. However, patients with a TTP >36 months post-ASCT or no ASCT had lower rates of TEAEs leading to treatment discontinuation (23% and 31%), the longer median duration of study treatment (35.1 weeks vs 15.1 weeks), and longer median time to experiencing grade 3/4 thrombocytopenia (11.2 weeks vs 4.1 weeks) and grade 3/4 neutropenia (4.8 weeks vs 2.1 weeks) than patients with a TTP <36 months post-ASCT. In HORIZON, patients with a TTP >36 months post-ASCT or no ASCT had lower rates of grade 3/4 TEAEs (88% and 98%), but higher rates of serious TEAEs (64% and 53%) and similar rates of TEAEs leading to treatment discontinuation (29% and 33%) than patients with a TTP <36 months post-ASCT.
Click to Show/Hide
|
||||
| Experiment 364 Reporting the Activity Data of This PDC | [9] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Thrombocytopenia concurrent with hemorrhage |
1%
|
|||
| Patients Enrolled |
145 patients who has relapsed/refractory multiple myeloma with no previous ASCT or TTP >36 month Post-ASCTa.
|
||||
| MOA of PDC |
In summary, the interpretation of the results from the OCEAN study were impacted by the heterogeneity of the population, with age and previous success of ASCT therapy identified as prognostic factors with study therapies. The safety profile of melflufen and dexamethasone is primarily characterized by hematologic AEs that are clinically manageable. Observed infection rates, which included COVID-19, were generally low. Taken together, these data support the use of melflufen and dexamethasone in patients who have not received a previous ASCT or who underwent a successful ASCT (ie, TTP >36 months post-ASCT). In addition, the favorable efficacy profile and convenience of monthly outpatient infusions, especially for patients without access to other therapeutics such as CAR T-cell therapy or bispecific antibodies, bode well for this combination translating successfully into real-world practice.
Click to Show/Hide
|
||||
| Description |
Given the prognostic importance of TTP <36 months post-ASCT in OCEAN, we evaluated this prognostic factor in a post hoc analysis from the HORIZON study. Among 110 patients with triple-class refractory disease who had received ≥3 prior lines of therapy, 77 (70%) had received a previous ASCT and 58 (53%) had TTP <36 months post-ASCT (Suppl. Table S3). In patients with a TTP >36 months post-ASCT or no ASCT versus patients with a TTP <36 months post-ASCT, ORR was higher (29% vs 22%; Suppl. Table S4) and median DOR (7.6 months vs 3.9 months) and median PFS (4.2 months vs 3.4 months) were longer. Since pomalidomide and lenalidomide both belong to the immunomodulatory drugs, we analyzed if the duration of previous treatment with lenalidomide could have impacted the results. The median duration of lenalidomide was 14.4 months in patients with ASCT and TTP < 36 months, 38.3 months in patients with ASCT and TTP > 36 months, and 14.6 months in patients with no previous ASCT. However, the median PFS for patients treated with pomalidomide did not differ substantially between these groups of patients. The safety profile of melflufen and dexamethasone was generally consistent between patients with a TTP >36 months post-ASCT or no ASCT and patients with a TTP <36 months post-ASCT. In OCEAN among the melflufen group, the frequency of grade 3/4 TEAEs (88% and 92%), serious TEAEs (44% and 38%), and fatal adverse events (AEs; 11% and 13%) was similar in patients with a TTP >36 months post-ASCT or no ASCT and patients with TTP <36 months. However, patients with a TTP >36 months post-ASCT or no ASCT had lower rates of TEAEs leading to treatment discontinuation (23% and 31%), the longer median duration of study treatment (35.1 weeks vs 15.1 weeks), and longer median time to experiencing grade 3/4 thrombocytopenia (11.2 weeks vs 4.1 weeks) and grade 3/4 neutropenia (4.8 weeks vs 2.1 weeks) than patients with a TTP <36 months post-ASCT. In HORIZON, patients with a TTP >36 months post-ASCT or no ASCT had lower rates of grade 3/4 TEAEs (88% and 98%), but higher rates of serious TEAEs (64% and 53%) and similar rates of TEAEs leading to treatment discontinuation (29% and 33%) than patients with a TTP <36 months post-ASCT.
Click to Show/Hide
|
||||
| Experiment 365 Reporting the Activity Data of This PDC | [5] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Time to dose reduction |
106 Day
|
|||
| Patients Enrolled |
153 patients refractory to prior alkylators (melflufen, n=78; pomalidomide, n=75).
|
||||
| MOA of PDC |
Melphalan flufenamide (melflufen), a first-in-class alkylating peptide-drug conjugate, plus dexamethasone demonstrated superior progression-free survival (PFS), but not overall survival (OS), versus pomalidomide plus dexamethasone in relapsed/refractory multiple myeloma in the OCEAN study. Time to progression (TTP) <36 months after a prior autologous stem cell transplantation (ASCT) was a negative prognostic factor for OS with melflufen. This post hoc exploratory analysis evaluated patients refractory to prior alkylators (e.g., cyclophosphamide and melphalan) in OCEAN. In 153 patients refractory to prior alkylators (melflufen, n = 78; pomalidomide, n = 75), the melflufen and pomalidomide arms had similar median PFS (5.6 months [95% CI, 4.2-8.3] vs. 4.7 months [95% CI, 3.1-7.3]; hazard ratio [HR], 0.92 [95% CI, 0.63-1.33]) and OS (23.4 months [95% CI, 14.4-31.7] vs. 20.0 months [95% CI, 12.0-28.7]; HR, 0.92 [95% CI, 0.62-1.38]). Among alkylator-refractory patients with a TTP 36 months after a prior ASCT or no prior ASCT (melflufen, n = 54; pomalidomide, n = 53), the observed median PFS and OS were longer in the melflufen arm than the pomalidomide arm. The safety profile of melflufen was consistent with previous reports. These results suggest that melflufen is safe and effective in patients with alkylator-refractory disease, suggesting differentiated activity from other alkylators.
Click to Show/Hide
|
||||
| Description |
Overall, the safety profile of melflufen plus dexamethasone in the alkylator-refractory group was consistent between treatment arms (Table 2). In the melflufen and pomalidomide arms, respectively, the frequency of treatment-emergent adverse events (TEAEs; 99% vs. 97%), Grade 3 or 4 TEAEs (85% vs. 82%), serious TEAEs (49% vs. 53%), and fatal TEAEs (19% vs. 16%) were similar (Table 2). However, melflufen compared with pomalidomide saw more dose modifications (76% vs. 67%) and dose reductions (47% vs. 14%), comparable dose delays (57% vs. 51%) but less treatment discontinuation (27% vs. 34%). When comparing patients refractory and not refractory to prior alkylators, rates of TEAEs were generally comparable except for slightly lower rates of serious and fatal TEAEs observed in patients not refractory to alkylators. Among Grade 3 or 4 TEAEs of special interest, melflufen saw more thrombocytopenia (73% vs. 14%), neutropenia (65% vs. 55%), and leukopenia or white blood cell decrease (14% vs. 3%), but less infection (15% vs. 26%), than pomalidomide. Notably, melflufen compared with pomalidomide saw a longer median time to dose reduction (106 days [range, 28-443] vs. 47 days [range, 28-225]), Grade 3 or 4 thrombocytopenia (52 days [range, 15-451] vs. 19 days [range, 8-91]), and Grade 3 or 4 neutropenia (36 days [range, 8-561] vs. 22 days [range, 8-470]).
Click to Show/Hide
|
||||
| Experiment 366 Reporting the Activity Data of This PDC | [5] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Time to grade 3/4 neutropenia |
36 Day
|
|||
| Patients Enrolled |
153 patients refractory to prior alkylators (melflufen, n=78; pomalidomide, n=75).
|
||||
| MOA of PDC |
Melphalan flufenamide (melflufen), a first-in-class alkylating peptide-drug conjugate, plus dexamethasone demonstrated superior progression-free survival (PFS), but not overall survival (OS), versus pomalidomide plus dexamethasone in relapsed/refractory multiple myeloma in the OCEAN study. Time to progression (TTP) <36 months after a prior autologous stem cell transplantation (ASCT) was a negative prognostic factor for OS with melflufen. This post hoc exploratory analysis evaluated patients refractory to prior alkylators (e.g., cyclophosphamide and melphalan) in OCEAN. In 153 patients refractory to prior alkylators (melflufen, n = 78; pomalidomide, n = 75), the melflufen and pomalidomide arms had similar median PFS (5.6 months [95% CI, 4.2-8.3] vs. 4.7 months [95% CI, 3.1-7.3]; hazard ratio [HR], 0.92 [95% CI, 0.63-1.33]) and OS (23.4 months [95% CI, 14.4-31.7] vs. 20.0 months [95% CI, 12.0-28.7]; HR, 0.92 [95% CI, 0.62-1.38]). Among alkylator-refractory patients with a TTP 36 months after a prior ASCT or no prior ASCT (melflufen, n = 54; pomalidomide, n = 53), the observed median PFS and OS were longer in the melflufen arm than the pomalidomide arm. The safety profile of melflufen was consistent with previous reports. These results suggest that melflufen is safe and effective in patients with alkylator-refractory disease, suggesting differentiated activity from other alkylators.
Click to Show/Hide
|
||||
| Description |
Overall, the safety profile of melflufen plus dexamethasone in the alkylator-refractory group was consistent between treatment arms (Table 2). In the melflufen and pomalidomide arms, respectively, the frequency of treatment-emergent adverse events (TEAEs; 99% vs. 97%), Grade 3 or 4 TEAEs (85% vs. 82%), serious TEAEs (49% vs. 53%), and fatal TEAEs (19% vs. 16%) were similar (Table 2). However, melflufen compared with pomalidomide saw more dose modifications (76% vs. 67%) and dose reductions (47% vs. 14%), comparable dose delays (57% vs. 51%) but less treatment discontinuation (27% vs. 34%). When comparing patients refractory and not refractory to prior alkylators, rates of TEAEs were generally comparable except for slightly lower rates of serious and fatal TEAEs observed in patients not refractory to alkylators. Among Grade 3 or 4 TEAEs of special interest, melflufen saw more thrombocytopenia (73% vs. 14%), neutropenia (65% vs. 55%), and leukopenia or white blood cell decrease (14% vs. 3%), but less infection (15% vs. 26%), than pomalidomide. Notably, melflufen compared with pomalidomide saw a longer median time to dose reduction (106 days [range, 28-443] vs. 47 days [range, 28-225]), Grade 3 or 4 thrombocytopenia (52 days [range, 15-451] vs. 19 days [range, 8-91]), and Grade 3 or 4 neutropenia (36 days [range, 8-561] vs. 22 days [range, 8-470]).
Click to Show/Hide
|
||||
| Experiment 367 Reporting the Activity Data of This PDC | [5] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Time to grade 3/4 thrombocytopenia |
52 Day
|
|||
| Patients Enrolled |
153 patients refractory to prior alkylators (melflufen, n=78; pomalidomide, n=75).
|
||||
| MOA of PDC |
Melphalan flufenamide (melflufen), a first-in-class alkylating peptide-drug conjugate, plus dexamethasone demonstrated superior progression-free survival (PFS), but not overall survival (OS), versus pomalidomide plus dexamethasone in relapsed/refractory multiple myeloma in the OCEAN study. Time to progression (TTP) <36 months after a prior autologous stem cell transplantation (ASCT) was a negative prognostic factor for OS with melflufen. This post hoc exploratory analysis evaluated patients refractory to prior alkylators (e.g., cyclophosphamide and melphalan) in OCEAN. In 153 patients refractory to prior alkylators (melflufen, n = 78; pomalidomide, n = 75), the melflufen and pomalidomide arms had similar median PFS (5.6 months [95% CI, 4.2-8.3] vs. 4.7 months [95% CI, 3.1-7.3]; hazard ratio [HR], 0.92 [95% CI, 0.63-1.33]) and OS (23.4 months [95% CI, 14.4-31.7] vs. 20.0 months [95% CI, 12.0-28.7]; HR, 0.92 [95% CI, 0.62-1.38]). Among alkylator-refractory patients with a TTP 36 months after a prior ASCT or no prior ASCT (melflufen, n = 54; pomalidomide, n = 53), the observed median PFS and OS were longer in the melflufen arm than the pomalidomide arm. The safety profile of melflufen was consistent with previous reports. These results suggest that melflufen is safe and effective in patients with alkylator-refractory disease, suggesting differentiated activity from other alkylators.
Click to Show/Hide
|
||||
| Description |
Overall, the safety profile of melflufen plus dexamethasone in the alkylator-refractory group was consistent between treatment arms (Table 2). In the melflufen and pomalidomide arms, respectively, the frequency of treatment-emergent adverse events (TEAEs; 99% vs. 97%), Grade 3 or 4 TEAEs (85% vs. 82%), serious TEAEs (49% vs. 53%), and fatal TEAEs (19% vs. 16%) were similar (Table 2). However, melflufen compared with pomalidomide saw more dose modifications (76% vs. 67%) and dose reductions (47% vs. 14%), comparable dose delays (57% vs. 51%) but less treatment discontinuation (27% vs. 34%). When comparing patients refractory and not refractory to prior alkylators, rates of TEAEs were generally comparable except for slightly lower rates of serious and fatal TEAEs observed in patients not refractory to alkylators. Among Grade 3 or 4 TEAEs of special interest, melflufen saw more thrombocytopenia (73% vs. 14%), neutropenia (65% vs. 55%), and leukopenia or white blood cell decrease (14% vs. 3%), but less infection (15% vs. 26%), than pomalidomide. Notably, melflufen compared with pomalidomide saw a longer median time to dose reduction (106 days [range, 28-443] vs. 47 days [range, 28-225]), Grade 3 or 4 thrombocytopenia (52 days [range, 15-451] vs. 19 days [range, 8-91]), and Grade 3 or 4 neutropenia (36 days [range, 8-561] vs. 22 days [range, 8-470]).
Click to Show/Hide
|
||||
| Experiment 368 Reporting the Activity Data of This PDC | [2] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Treatment-emergent adverse event |
96%
|
|||
| MOA of PDC |
Melphalan flufenamide (melflufen), a first-in-class alkylating peptide-drug conjugate, plus dexamethasone was approved in Europe for use in patients with triple-class refractory relapsed/refractory multiple myeloma (RRMM) with 3 prior lines of therapy and without prior autologous stem cell transplantation (ASCT) or with a time to progression >36 months after prior ASCT. The randomized LIGHTHOUSE study (NCT04649060) assessed melflufen plus daratumumab and dexamethasone (melflufen group) versus daratumumab in patients with RRMM with disease refractory to an immunomodulatory agent and a proteasome inhibitor or who had received 3 prior lines of therapy including an immunomodulatory agent and a proteasome inhibitor. A partial clinical hold issued by the US Food and Drug Administration for all melflufen studies led to financial constraints and premature study closure on February 23rd 2022 (data cut-off date). In total, 54 of 240 planned patients were randomized (melflufen group, N=27; daratumumab group, N=27). Median progression-free survival (PFS) was not reached in the melflufen group versus 4.9 months in the daratumumab group (Hazard Ratio: 0.18 [95% Confidence Interval, 0.05-0.65]; P=0.0032) at a median follow-up time of 7.1 and 6.6 months, respectively. Overall response rate (ORR) was 59% in the melflufen group versus 30% in the daratumumab group (P=0.0300). The most common grade 3 treatment-emergent adverse events in the melflufen group versus daratumumab group were neutropenia (50% vs. 12%), thrombocytopenia (50% vs. 8%), and anemia (32% vs. 19%). Melflufen plus daratumumab and dexamethasone demonstrated superior PFS and ORR versus daratumumab in RRMM and a safety profile comparable to previously published melflufen studies.
Click to Show/Hide
|
||||
| Description |
The safety population included patients who received ≥1 dose of melflufen, daratumumab, or dexamethasone (melflufen group) and 26 patients who received daratumumab monotherapy. In the safety population, ≥1 TEAE was reported in 21 patients (96%) with melflufen, daratumumab, and dexamethasone and 22 patients (85%) with daratumumab. Overall, grade ≥3 TEAE occurred in 18 patients (82%) with melflufen, daratumumab, and dexamethasone and 14 patients (54%) with daratumumab. The most common hematologic grade ≥3 TEAE were neutropenia (melflufen group, 11 patients [50%]; daratumumab group, 3 patients [12%]), thrombocytopenia (melflufen group, 11 patients [50%]; daratumumab group, 2 patients [8%]), and anemia (melflufen group, 7 patients [32%]; daratumumab group, 5 patients [19%]). The most common non-hematologic grade ≥3 TEAE were pneumonia (melflufen group, 2 patients [9%]; daratumumab group, 2 patients [8%]) and femur fracture (melflufen group, 0 patients [0%]; daratumumab group, 2 patients [8%]); of these, 1 event (5%) of pneumonia in the melflufen group and 1 event (4%) of femur fracture in the daratumumab group were considered treatment-related TEAE by the investigator. Serious AE occurred in 6 patients (27%) with melflufen, daratumumab, and dexamethasone, and 12 patients (46%) with daratumumab. The most common serious AE (occurring in ≥4 patients overall) were anemia (melflufen group, 2 patients [9%]; daratumumab group, 3 patients [12%]) and pneumonia (melflufen group, 2 patients [9%]; daratumumab group, 2 patients [8%]). TEAE leading to treatment discontinuation occurred in 2 patients (9%) in the melflufen group (neutropenia and thrombocytopenia, N=1 each) and 4 patients (15%) in the daratumumab group (anemia, disease progression, hypercalcemia, and renal failure, N=1 each). Overall, 5 patients died on study before the crossover: 2 patients who received melflufen, daratumumab, and dexamethasone (1 due to disease progression and 1 due to unknown reasons, both >30 days after the last dose of study treatment) and 3 patients who received daratumumab (1 due to disease progression and 1 due to unknown reasons, both ≤30 days after the last dose of study treatment and 1 due to an AE [COVID-19 pneumonia], >30 days after the last dose of study treatment). In addition, one patient who crossed over to receive melflufen, daratumumab, and dexamethasone after progression on daratumumab died.
Click to Show/Hide
|
||||
| In Vivo Model | 22 relapsed/refractory multiple myeloma. | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT04649060 | Clinical Status | Phase 3 | ||
| Clinical Description | This was a randomized, controlled, open-label, Phase 3 multicenter study which enrolled patients with Relapsed-Refractory Multiple Myeloma (RRMM) who were either double refractory to an Immunomodulatory Drug (IMiD) and a Proteasome Inhibitor (PI) (regardless of the number of prior lines of therapy), or had received at least 3 prior lines of therapy including an IMiD and a PI. Patients received treatment with melflufen+dexamethasone+daratumumab or daratumumab until documented progressive disease, unacceptable toxicity, or patient/treating physician decision. Patients in the daratumumab treatment arm had the option to receive treatment with melflufen+dexamethasone+daratumumab after confirmed progressive disease. | ||||
| Experiment 369 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Treatment-emergent adverse event |
7.10%
|
|||
| Patients Enrolled |
14 patients with relapsed refractory multiple myeloma.
|
||||
| Administration Time | 28-day cycle | ||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (melflufen) is a first-in-class peptide-drug conjugate that utilizes increased peptidase expression to selectively release potent alkylating agents inside tumor cells. Melflufen is hydrolyzed by peptidases and esterases to melphalan either directly or through an intermediate metabolite, desethyl-melflufen. The high lipophilicity of melflufen facilitates passive diffusion across cell membranes. The activity and tolerability of melflufen in relapsed/refractory multiple myeloma (RRMM) were demonstrated in the O-12-M1 (NCT01897714), OCEAN (NCT03151811), and HORIZON (NCT02963493) trials.
Click to Show/Hide
|
||||
| Description |
Overall, at least one TEAE was reported in 13 (92.9%) and 13 (100.0%) patients in Arms A and B, respectively (Table 3). During cycle 1, 9 patients (64.3%) and 12 patients (92.3%), respectively, had at least one TEAE. Cumulatively, grade 3 or 4 AEs occurred in 12 (85.7%) and 12 (92.3%) patients, respectively, and serious AEs were reported in 5 (35.7%) and 9 (69.2%) patients, respectively. The most common any-grade AEs in Arms A and B, respectively, were thrombocytopenia (10 [71.4%]; 10 [76.9%]), neutropenia (9 [64.3%]; 9 [69.2%]), and anemia (9 [64.3%]; 7 [53.8%]). No phlebitis or local-infusion-related reactions were reported based on pre- and post-infusion inspection of the IV site, and there were no extravasations observed in Arm A or B. Similarly, VIP scores collected on Day 1 post-infusion and on Day 8 indicated that patients had healthy IV sites (VIP score of 0) with no signs of phlebitis following PVC administration of melflufen. The most common non-hematological AE was positive SARS-CoV-2 test (Arm A: 2 [14.3%]; Arm B: 4 [30.8%]). Pneumonia was the most common serious AE (Arm A: 2 [14.3%]; Arm B: 2 [15.4%]). The most common AE considered related to melflufen and/or dexamethasone by investigators was thrombocytopenia (Arm A: 10 [71.4%]; Arm B: 10 [76.9%]). AEs led to treatment discontinuation in 3 (21.4%) and 6 (46.2%) patients in Arms A and B, respectively.
Click to Show/Hide
|
||||
| Half life period | 75.6 h | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT04412707 | Clinical Status | Phase 2 | ||
| Clinical Description | This is a randomized, two-period, cross-over Phase 2 study, comparing PK, and assessing safety and tolerability and efficacy of peripheral and central intravenous administration of melflufen in patients with RRMM. It is an international study, enrolling patients in US and Europe. The study will enroll patients following at least 2 lines of prior therapy. | ||||
| Experiment 370 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Treatment-emergent adverse event |
21.40%
|
|||
| Patients Enrolled |
14 patients with relapsed refractory multiple myeloma.
|
||||
| Administration Time | 28-day cycle | ||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (melflufen) is a first-in-class peptide-drug conjugate that utilizes increased peptidase expression to selectively release potent alkylating agents inside tumor cells. Melflufen is hydrolyzed by peptidases and esterases to melphalan either directly or through an intermediate metabolite, desethyl-melflufen. The high lipophilicity of melflufen facilitates passive diffusion across cell membranes. The activity and tolerability of melflufen in relapsed/refractory multiple myeloma (RRMM) were demonstrated in the O-12-M1 (NCT01897714), OCEAN (NCT03151811), and HORIZON (NCT02963493) trials.
Click to Show/Hide
|
||||
| Description |
Overall, at least one TEAE was reported in 13 (92.9%) and 13 (100.0%) patients in Arms A and B, respectively (Table 3). During cycle 1, 9 patients (64.3%) and 12 patients (92.3%), respectively, had at least one TEAE. Cumulatively, grade 3 or 4 AEs occurred in 12 (85.7%) and 12 (92.3%) patients, respectively, and serious AEs were reported in 5 (35.7%) and 9 (69.2%) patients, respectively. The most common any-grade AEs in Arms A and B, respectively, were thrombocytopenia (10 [71.4%]; 10 [76.9%]), neutropenia (9 [64.3%]; 9 [69.2%]), and anemia (9 [64.3%]; 7 [53.8%]). No phlebitis or local-infusion-related reactions were reported based on pre- and post-infusion inspection of the IV site, and there were no extravasations observed in Arm A or B. Similarly, VIP scores collected on Day 1 post-infusion and on Day 8 indicated that patients had healthy IV sites (VIP score of 0) with no signs of phlebitis following PVC administration of melflufen. The most common non-hematological AE was positive SARS-CoV-2 test (Arm A: 2 [14.3%]; Arm B: 4 [30.8%]). Pneumonia was the most common serious AE (Arm A: 2 [14.3%]; Arm B: 2 [15.4%]). The most common AE considered related to melflufen and/or dexamethasone by investigators was thrombocytopenia (Arm A: 10 [71.4%]; Arm B: 10 [76.9%]). AEs led to treatment discontinuation in 3 (21.4%) and 6 (46.2%) patients in Arms A and B, respectively.
Click to Show/Hide
|
||||
| Half life period | 75.6 h | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT04412707 | Clinical Status | Phase 2 | ||
| Clinical Description | This is a randomized, two-period, cross-over Phase 2 study, comparing PK, and assessing safety and tolerability and efficacy of peripheral and central intravenous administration of melflufen in patients with RRMM. It is an international study, enrolling patients in US and Europe. The study will enroll patients following at least 2 lines of prior therapy. | ||||
| Experiment 371 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Treatment-emergent adverse event |
21.40%
|
|||
| Patients Enrolled |
14 patients with relapsed refractory multiple myeloma.
|
||||
| Administration Time | 28-day cycle | ||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (melflufen) is a first-in-class peptide-drug conjugate that utilizes increased peptidase expression to selectively release potent alkylating agents inside tumor cells. Melflufen is hydrolyzed by peptidases and esterases to melphalan either directly or through an intermediate metabolite, desethyl-melflufen. The high lipophilicity of melflufen facilitates passive diffusion across cell membranes. The activity and tolerability of melflufen in relapsed/refractory multiple myeloma (RRMM) were demonstrated in the O-12-M1 (NCT01897714), OCEAN (NCT03151811), and HORIZON (NCT02963493) trials.
Click to Show/Hide
|
||||
| Description |
Overall, at least one TEAE was reported in 13 (92.9%) and 13 (100.0%) patients in Arms A and B, respectively (Table 3). During cycle 1, 9 patients (64.3%) and 12 patients (92.3%), respectively, had at least one TEAE. Cumulatively, grade 3 or 4 AEs occurred in 12 (85.7%) and 12 (92.3%) patients, respectively, and serious AEs were reported in 5 (35.7%) and 9 (69.2%) patients, respectively. The most common any-grade AEs in Arms A and B, respectively, were thrombocytopenia (10 [71.4%]; 10 [76.9%]), neutropenia (9 [64.3%]; 9 [69.2%]), and anemia (9 [64.3%]; 7 [53.8%]). No phlebitis or local-infusion-related reactions were reported based on pre- and post-infusion inspection of the IV site, and there were no extravasations observed in Arm A or B. Similarly, VIP scores collected on Day 1 post-infusion and on Day 8 indicated that patients had healthy IV sites (VIP score of 0) with no signs of phlebitis following PVC administration of melflufen. The most common non-hematological AE was positive SARS-CoV-2 test (Arm A: 2 [14.3%]; Arm B: 4 [30.8%]). Pneumonia was the most common serious AE (Arm A: 2 [14.3%]; Arm B: 2 [15.4%]). The most common AE considered related to melflufen and/or dexamethasone by investigators was thrombocytopenia (Arm A: 10 [71.4%]; Arm B: 10 [76.9%]). AEs led to treatment discontinuation in 3 (21.4%) and 6 (46.2%) patients in Arms A and B, respectively.
Click to Show/Hide
|
||||
| Half life period | 75.6 h | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT04412707 | Clinical Status | Phase 2 | ||
| Clinical Description | This is a randomized, two-period, cross-over Phase 2 study, comparing PK, and assessing safety and tolerability and efficacy of peripheral and central intravenous administration of melflufen in patients with RRMM. It is an international study, enrolling patients in US and Europe. The study will enroll patients following at least 2 lines of prior therapy. | ||||
| Experiment 372 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Treatment-emergent adverse event |
35.70%
|
|||
| Patients Enrolled |
14 patients with relapsed refractory multiple myeloma.
|
||||
| Administration Time | 28-day cycle | ||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (melflufen) is a first-in-class peptide-drug conjugate that utilizes increased peptidase expression to selectively release potent alkylating agents inside tumor cells. Melflufen is hydrolyzed by peptidases and esterases to melphalan either directly or through an intermediate metabolite, desethyl-melflufen. The high lipophilicity of melflufen facilitates passive diffusion across cell membranes. The activity and tolerability of melflufen in relapsed/refractory multiple myeloma (RRMM) were demonstrated in the O-12-M1 (NCT01897714), OCEAN (NCT03151811), and HORIZON (NCT02963493) trials.
Click to Show/Hide
|
||||
| Description |
Overall, at least one TEAE was reported in 13 (92.9%) and 13 (100.0%) patients in Arms A and B, respectively (Table 3). During cycle 1, 9 patients (64.3%) and 12 patients (92.3%), respectively, had at least one TEAE. Cumulatively, grade 3 or 4 AEs occurred in 12 (85.7%) and 12 (92.3%) patients, respectively, and serious AEs were reported in 5 (35.7%) and 9 (69.2%) patients, respectively. The most common any-grade AEs in Arms A and B, respectively, were thrombocytopenia (10 [71.4%]; 10 [76.9%]), neutropenia (9 [64.3%]; 9 [69.2%]), and anemia (9 [64.3%]; 7 [53.8%]). No phlebitis or local-infusion-related reactions were reported based on pre- and post-infusion inspection of the IV site, and there were no extravasations observed in Arm A or B. Similarly, VIP scores collected on Day 1 post-infusion and on Day 8 indicated that patients had healthy IV sites (VIP score of 0) with no signs of phlebitis following PVC administration of melflufen. The most common non-hematological AE was positive SARS-CoV-2 test (Arm A: 2 [14.3%]; Arm B: 4 [30.8%]). Pneumonia was the most common serious AE (Arm A: 2 [14.3%]; Arm B: 2 [15.4%]). The most common AE considered related to melflufen and/or dexamethasone by investigators was thrombocytopenia (Arm A: 10 [71.4%]; Arm B: 10 [76.9%]). AEs led to treatment discontinuation in 3 (21.4%) and 6 (46.2%) patients in Arms A and B, respectively.
Click to Show/Hide
|
||||
| Half life period | 75.6 h | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT04412707 | Clinical Status | Phase 2 | ||
| Clinical Description | This is a randomized, two-period, cross-over Phase 2 study, comparing PK, and assessing safety and tolerability and efficacy of peripheral and central intravenous administration of melflufen in patients with RRMM. It is an international study, enrolling patients in US and Europe. The study will enroll patients following at least 2 lines of prior therapy. | ||||
| Experiment 373 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Treatment-emergent adverse event |
71.40%
|
|||
| Patients Enrolled |
14 patients with relapsed refractory multiple myeloma.
|
||||
| Administration Time | 28-day cycle | ||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (melflufen) is a first-in-class peptide-drug conjugate that utilizes increased peptidase expression to selectively release potent alkylating agents inside tumor cells. Melflufen is hydrolyzed by peptidases and esterases to melphalan either directly or through an intermediate metabolite, desethyl-melflufen. The high lipophilicity of melflufen facilitates passive diffusion across cell membranes. The activity and tolerability of melflufen in relapsed/refractory multiple myeloma (RRMM) were demonstrated in the O-12-M1 (NCT01897714), OCEAN (NCT03151811), and HORIZON (NCT02963493) trials.
Click to Show/Hide
|
||||
| Description |
Overall, at least one TEAE was reported in 13 (92.9%) and 13 (100.0%) patients in Arms A and B, respectively (Table 3). During cycle 1, 9 patients (64.3%) and 12 patients (92.3%), respectively, had at least one TEAE. Cumulatively, grade 3 or 4 AEs occurred in 12 (85.7%) and 12 (92.3%) patients, respectively, and serious AEs were reported in 5 (35.7%) and 9 (69.2%) patients, respectively. The most common any-grade AEs in Arms A and B, respectively, were thrombocytopenia (10 [71.4%]; 10 [76.9%]), neutropenia (9 [64.3%]; 9 [69.2%]), and anemia (9 [64.3%]; 7 [53.8%]). No phlebitis or local-infusion-related reactions were reported based on pre- and post-infusion inspection of the IV site, and there were no extravasations observed in Arm A or B. Similarly, VIP scores collected on Day 1 post-infusion and on Day 8 indicated that patients had healthy IV sites (VIP score of 0) with no signs of phlebitis following PVC administration of melflufen. The most common non-hematological AE was positive SARS-CoV-2 test (Arm A: 2 [14.3%]; Arm B: 4 [30.8%]). Pneumonia was the most common serious AE (Arm A: 2 [14.3%]; Arm B: 2 [15.4%]). The most common AE considered related to melflufen and/or dexamethasone by investigators was thrombocytopenia (Arm A: 10 [71.4%]; Arm B: 10 [76.9%]). AEs led to treatment discontinuation in 3 (21.4%) and 6 (46.2%) patients in Arms A and B, respectively.
Click to Show/Hide
|
||||
| Half life period | 75.6 h | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT04412707 | Clinical Status | Phase 2 | ||
| Clinical Description | This is a randomized, two-period, cross-over Phase 2 study, comparing PK, and assessing safety and tolerability and efficacy of peripheral and central intravenous administration of melflufen in patients with RRMM. It is an international study, enrolling patients in US and Europe. The study will enroll patients following at least 2 lines of prior therapy. | ||||
| Experiment 374 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Treatment-emergent adverse event |
92.90%
|
|||
| Patients Enrolled |
14 patients with relapsed refractory multiple myeloma.
|
||||
| Administration Time | 28-day cycle | ||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (melflufen) is a first-in-class peptide-drug conjugate that utilizes increased peptidase expression to selectively release potent alkylating agents inside tumor cells. Melflufen is hydrolyzed by peptidases and esterases to melphalan either directly or through an intermediate metabolite, desethyl-melflufen. The high lipophilicity of melflufen facilitates passive diffusion across cell membranes. The activity and tolerability of melflufen in relapsed/refractory multiple myeloma (RRMM) were demonstrated in the O-12-M1 (NCT01897714), OCEAN (NCT03151811), and HORIZON (NCT02963493) trials.
Click to Show/Hide
|
||||
| Description |
Overall, at least one TEAE was reported in 13 (92.9%) and 13 (100.0%) patients in Arms A and B, respectively (Table 3). During cycle 1, 9 patients (64.3%) and 12 patients (92.3%), respectively, had at least one TEAE. Cumulatively, grade 3 or 4 AEs occurred in 12 (85.7%) and 12 (92.3%) patients, respectively, and serious AEs were reported in 5 (35.7%) and 9 (69.2%) patients, respectively. The most common any-grade AEs in Arms A and B, respectively, were thrombocytopenia (10 [71.4%]; 10 [76.9%]), neutropenia (9 [64.3%]; 9 [69.2%]), and anemia (9 [64.3%]; 7 [53.8%]). No phlebitis or local-infusion-related reactions were reported based on pre- and post-infusion inspection of the IV site, and there were no extravasations observed in Arm A or B. Similarly, VIP scores collected on Day 1 post-infusion and on Day 8 indicated that patients had healthy IV sites (VIP score of 0) with no signs of phlebitis following PVC administration of melflufen. The most common non-hematological AE was positive SARS-CoV-2 test (Arm A: 2 [14.3%]; Arm B: 4 [30.8%]). Pneumonia was the most common serious AE (Arm A: 2 [14.3%]; Arm B: 2 [15.4%]). The most common AE considered related to melflufen and/or dexamethasone by investigators was thrombocytopenia (Arm A: 10 [71.4%]; Arm B: 10 [76.9%]). AEs led to treatment discontinuation in 3 (21.4%) and 6 (46.2%) patients in Arms A and B, respectively.
Click to Show/Hide
|
||||
| Half life period | 75.6 h | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT04412707 | Clinical Status | Phase 2 | ||
| Clinical Description | This is a randomized, two-period, cross-over Phase 2 study, comparing PK, and assessing safety and tolerability and efficacy of peripheral and central intravenous administration of melflufen in patients with RRMM. It is an international study, enrolling patients in US and Europe. The study will enroll patients following at least 2 lines of prior therapy. | ||||
| Experiment 375 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Treatment-emergent adverse event |
92.90%
|
|||
| Patients Enrolled |
14 patients with relapsed refractory multiple myeloma.
|
||||
| Administration Time | 28-day cycle | ||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (melflufen) is a first-in-class peptide-drug conjugate that utilizes increased peptidase expression to selectively release potent alkylating agents inside tumor cells. Melflufen is hydrolyzed by peptidases and esterases to melphalan either directly or through an intermediate metabolite, desethyl-melflufen. The high lipophilicity of melflufen facilitates passive diffusion across cell membranes. The activity and tolerability of melflufen in relapsed/refractory multiple myeloma (RRMM) were demonstrated in the O-12-M1 (NCT01897714), OCEAN (NCT03151811), and HORIZON (NCT02963493) trials.
Click to Show/Hide
|
||||
| Description |
Overall, at least one TEAE was reported in 13 (92.9%) and 13 (100.0%) patients in Arms A and B, respectively (Table 3). During cycle 1, 9 patients (64.3%) and 12 patients (92.3%), respectively, had at least one TEAE. Cumulatively, grade 3 or 4 AEs occurred in 12 (85.7%) and 12 (92.3%) patients, respectively, and serious AEs were reported in 5 (35.7%) and 9 (69.2%) patients, respectively. The most common any-grade AEs in Arms A and B, respectively, were thrombocytopenia (10 [71.4%]; 10 [76.9%]), neutropenia (9 [64.3%]; 9 [69.2%]), and anemia (9 [64.3%]; 7 [53.8%]). No phlebitis or local-infusion-related reactions were reported based on pre- and post-infusion inspection of the IV site, and there were no extravasations observed in Arm A or B. Similarly, VIP scores collected on Day 1 post-infusion and on Day 8 indicated that patients had healthy IV sites (VIP score of 0) with no signs of phlebitis following PVC administration of melflufen. The most common non-hematological AE was positive SARS-CoV-2 test (Arm A: 2 [14.3%]; Arm B: 4 [30.8%]). Pneumonia was the most common serious AE (Arm A: 2 [14.3%]; Arm B: 2 [15.4%]). The most common AE considered related to melflufen and/or dexamethasone by investigators was thrombocytopenia (Arm A: 10 [71.4%]; Arm B: 10 [76.9%]). AEs led to treatment discontinuation in 3 (21.4%) and 6 (46.2%) patients in Arms A and B, respectively.
Click to Show/Hide
|
||||
| Half life period | 75.6 h | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT04412707 | Clinical Status | Phase 2 | ||
| Clinical Description | This is a randomized, two-period, cross-over Phase 2 study, comparing PK, and assessing safety and tolerability and efficacy of peripheral and central intravenous administration of melflufen in patients with RRMM. It is an international study, enrolling patients in US and Europe. The study will enroll patients following at least 2 lines of prior therapy. | ||||
| Experiment 376 Reporting the Activity Data of This PDC | [4] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Treatment-emergent adverse event |
100.00%
|
|||
| Patients Enrolled |
157 patients with multiple myeloma.
|
||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melflufen is a first-in-class peptide-drug conjugate, targeting aminopeptidase which has an increased expression in fast-growing and aggressive malignancies. The lipophilicity of melflufen allows for passive diffusion, selectively targeting myeloma cells. Once inside the cell, melflufen is hydrolyzed to active alkylating metabolites melphalan and desethyl-melflufen. Melflufen and the active metabolites trigger irreversible DNA damage, inhibit proliferation, induces apoptosis, and express antiangiogenic effects. In addition, melflufen demonstrated activity in myeloma cells with documented impaired or absent Tp53 expression and documented resistance to bortezomib, dexamethasone, and melphalan.
Click to Show/Hide
|
||||
| Description |
Based on the safety data collected during the HORIZON trial, treatment emergent adverse events occurred in 100% of patients including 100 patients (64%) having at least 1 CTCAE grade 4 adverse effect. Hematologic grade 3 or 4 adverse effects including thrombocytopenia (76%), neutropenia (79%), anemia (43%), and infections (11%) were the most commonly reported. Other adverse effects, such as fatigue (55%), nausea (32%), diarrhea (27%), and decreased appetite (14%), were similar to other alkylating agents. Pyrexia (24%), including febrile neutropenia (5%), and respiratory tract infections (24%) were contributed to hematologic toxicities.
Click to Show/Hide
|
||||
| Experiment 377 Reporting the Activity Data of This PDC | [9] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Treatment-emergent adverse event |
11%
|
|||
| Patients Enrolled |
145 patients who has relapsed/refractory multiple myeloma with no previous ASCT or TTP >36 month Post-ASCTa.
|
||||
| MOA of PDC |
In summary, the interpretation of the results from the OCEAN study were impacted by the heterogeneity of the population, with age and previous success of ASCT therapy identified as prognostic factors with study therapies. The safety profile of melflufen and dexamethasone is primarily characterized by hematologic AEs that are clinically manageable. Observed infection rates, which included COVID-19, were generally low. Taken together, these data support the use of melflufen and dexamethasone in patients who have not received a previous ASCT or who underwent a successful ASCT (ie, TTP >36 months post-ASCT). In addition, the favorable efficacy profile and convenience of monthly outpatient infusions, especially for patients without access to other therapeutics such as CAR T-cell therapy or bispecific antibodies, bode well for this combination translating successfully into real-world practice.
Click to Show/Hide
|
||||
| Description |
Given the prognostic importance of TTP <36 months post-ASCT in OCEAN, we evaluated this prognostic factor in a post hoc analysis from the HORIZON study. Among 110 patients with triple-class refractory disease who had received ≥3 prior lines of therapy, 77 (70%) had received a previous ASCT and 58 (53%) had TTP <36 months post-ASCT (Suppl. Table S3). In patients with a TTP >36 months post-ASCT or no ASCT versus patients with a TTP <36 months post-ASCT, ORR was higher (29% vs 22%; Suppl. Table S4) and median DOR (7.6 months vs 3.9 months) and median PFS (4.2 months vs 3.4 months) were longer. Since pomalidomide and lenalidomide both belong to the immunomodulatory drugs, we analyzed if the duration of previous treatment with lenalidomide could have impacted the results. The median duration of lenalidomide was 14.4 months in patients with ASCT and TTP < 36 months, 38.3 months in patients with ASCT and TTP > 36 months, and 14.6 months in patients with no previous ASCT. However, the median PFS for patients treated with pomalidomide did not differ substantially between these groups of patients. The safety profile of melflufen and dexamethasone was generally consistent between patients with a TTP >36 months post-ASCT or no ASCT and patients with a TTP <36 months post-ASCT. In OCEAN among the melflufen group, the frequency of grade 3/4 TEAEs (88% and 92%), serious TEAEs (44% and 38%), and fatal adverse events (AEs; 11% and 13%) was similar in patients with a TTP >36 months post-ASCT or no ASCT and patients with TTP <36 months. However, patients with a TTP >36 months post-ASCT or no ASCT had lower rates of TEAEs leading to treatment discontinuation (23% and 31%), the longer median duration of study treatment (35.1 weeks vs 15.1 weeks), and longer median time to experiencing grade 3/4 thrombocytopenia (11.2 weeks vs 4.1 weeks) and grade 3/4 neutropenia (4.8 weeks vs 2.1 weeks) than patients with a TTP <36 months post-ASCT. In HORIZON, patients with a TTP >36 months post-ASCT or no ASCT had lower rates of grade 3/4 TEAEs (88% and 98%), but higher rates of serious TEAEs (64% and 53%) and similar rates of TEAEs leading to treatment discontinuation (29% and 33%) than patients with a TTP <36 months post-ASCT.
Click to Show/Hide
|
||||
| Experiment 378 Reporting the Activity Data of This PDC | [9] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Treatment-emergent adverse event |
13%
|
|||
| Patients Enrolled |
101 relapsed/refractory multiple myeloma patients with TTP <36 month Post-ASCTb.
|
||||
| MOA of PDC |
In summary, the interpretation of the results from the OCEAN study were impacted by the heterogeneity of the population, with age and previous success of ASCT therapy identified as prognostic factors with study therapies. The safety profile of melflufen and dexamethasone is primarily characterized by hematologic AEs that are clinically manageable. Observed infection rates, which included COVID-19, were generally low. Taken together, these data support the use of melflufen and dexamethasone in patients who have not received a previous ASCT or who underwent a successful ASCT (ie, TTP >36 months post-ASCT). In addition, the favorable efficacy profile and convenience of monthly outpatient infusions, especially for patients without access to other therapeutics such as CAR T-cell therapy or bispecific antibodies, bode well for this combination translating successfully into real-world practice.
Click to Show/Hide
|
||||
| Description |
Given the prognostic importance of TTP <36 months post-ASCT in OCEAN, we evaluated this prognostic factor in a post hoc analysis from the HORIZON study. Among 110 patients with triple-class refractory disease who had received ≥3 prior lines of therapy, 77 (70%) had received a previous ASCT and 58 (53%) had TTP <36 months post-ASCT (Suppl. Table S3). In patients with a TTP >36 months post-ASCT or no ASCT versus patients with a TTP <36 months post-ASCT, ORR was higher (29% vs 22%; Suppl. Table S4) and median DOR (7.6 months vs 3.9 months) and median PFS (4.2 months vs 3.4 months) were longer. Since pomalidomide and lenalidomide both belong to the immunomodulatory drugs, we analyzed if the duration of previous treatment with lenalidomide could have impacted the results. The median duration of lenalidomide was 14.4 months in patients with ASCT and TTP < 36 months, 38.3 months in patients with ASCT and TTP > 36 months, and 14.6 months in patients with no previous ASCT. However, the median PFS for patients treated with pomalidomide did not differ substantially between these groups of patients. The safety profile of melflufen and dexamethasone was generally consistent between patients with a TTP >36 months post-ASCT or no ASCT and patients with a TTP <36 months post-ASCT. In OCEAN among the melflufen group, the frequency of grade 3/4 TEAEs (88% and 92%), serious TEAEs (44% and 38%), and fatal adverse events (AEs; 11% and 13%) was similar in patients with a TTP >36 months post-ASCT or no ASCT and patients with TTP <36 months. However, patients with a TTP >36 months post-ASCT or no ASCT had lower rates of TEAEs leading to treatment discontinuation (23% and 31%), the longer median duration of study treatment (35.1 weeks vs 15.1 weeks), and longer median time to experiencing grade 3/4 thrombocytopenia (11.2 weeks vs 4.1 weeks) and grade 3/4 neutropenia (4.8 weeks vs 2.1 weeks) than patients with a TTP <36 months post-ASCT. In HORIZON, patients with a TTP >36 months post-ASCT or no ASCT had lower rates of grade 3/4 TEAEs (88% and 98%), but higher rates of serious TEAEs (64% and 53%) and similar rates of TEAEs leading to treatment discontinuation (29% and 33%) than patients with a TTP <36 months post-ASCT.
Click to Show/Hide
|
||||
| Experiment 379 Reporting the Activity Data of This PDC | [1] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Treatment-emergent adverse event |
17.00%
|
|||
| Patients Enrolled |
Patients with multi-refractory multiple myeloma.
|
||||
| Administration Time | 9.3 month (median) | ||||
| Administration Dosage | 30 or 40 mg | ||||
| MOA of PDC |
Melflufen is highly lipophilic, which promotes its rapid uptake by cells. Once within the cell, melflufen releases its hydrophilic alkylator payloads via the hydrolytic activity of intracellular peptidases (e.g., aminopeptidases). Aminopeptidases are Zn2+-dependent metalloproteinases that remove amino acids at the N-terminal position from oligopeptides and have been associated with multiple tumorigenic processes such as proliferation, apoptosis, differentiation, angiogenesis, and motility. The dependence of melflufen on aminopeptidases was initially demonstrated by the reduced cytotoxic activity of melflufen-but not the alkylator melphalan-when cells were pretreated with bestatin, an antibiotic that is a potent aminopeptidase inhibitor. In addition, structure analogs designed to resist peptide hydrolysis (N-methyl derivative and derivative with D-amino acid) were shown to be almost 100-fold less potent than melflufen. Subsequent in vitro studies demonstrated that hydrolytic cleavage of melflufen by aminopeptidases releases alkylator payloads, including melphalan. In vitro, the activity of melflufen is multi-pronged, including induction of DNA damage, induction of apoptosis, inhibition of VEGF-dependent cell migration, and inhibition of tumor-associated angiogenesis, which have been further reviewed elsewhere. Downregulation of aminopeptidases resulted in reduced melflufen-mediated cytotoxic activity and apoptotic signaling in cultured cells.
Click to Show/Hide
|
||||
| Experiment 380 Reporting the Activity Data of This PDC | [1] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Treatment-emergent adverse event |
18.00%
|
|||
| Patients Enrolled |
Patients with multi-refractory multiple myeloma.
|
||||
| Administration Time | 6.2 month (median) | ||||
| Administration Dosage | 30 or 40 mg | ||||
| MOA of PDC |
Melflufen is highly lipophilic, which promotes its rapid uptake by cells. Once within the cell, melflufen releases its hydrophilic alkylator payloads via the hydrolytic activity of intracellular peptidases (e.g., aminopeptidases). Aminopeptidases are Zn2+-dependent metalloproteinases that remove amino acids at the N-terminal position from oligopeptides and have been associated with multiple tumorigenic processes such as proliferation, apoptosis, differentiation, angiogenesis, and motility. The dependence of melflufen on aminopeptidases was initially demonstrated by the reduced cytotoxic activity of melflufen-but not the alkylator melphalan-when cells were pretreated with bestatin, an antibiotic that is a potent aminopeptidase inhibitor. In addition, structure analogs designed to resist peptide hydrolysis (N-methyl derivative and derivative with D-amino acid) were shown to be almost 100-fold less potent than melflufen. Subsequent in vitro studies demonstrated that hydrolytic cleavage of melflufen by aminopeptidases releases alkylator payloads, including melphalan. In vitro, the activity of melflufen is multi-pronged, including induction of DNA damage, induction of apoptosis, inhibition of VEGF-dependent cell migration, and inhibition of tumor-associated angiogenesis, which have been further reviewed elsewhere. Downregulation of aminopeptidases resulted in reduced melflufen-mediated cytotoxic activity and apoptotic signaling in cultured cells.
Click to Show/Hide
|
||||
| Experiment 381 Reporting the Activity Data of This PDC | [9] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Treatment-emergent adverse event |
23%
|
|||
| Patients Enrolled |
145 patients who has relapsed/refractory multiple myeloma with no previous ASCT or TTP >36 month Post-ASCTa.
|
||||
| MOA of PDC |
In summary, the interpretation of the results from the OCEAN study were impacted by the heterogeneity of the population, with age and previous success of ASCT therapy identified as prognostic factors with study therapies. The safety profile of melflufen and dexamethasone is primarily characterized by hematologic AEs that are clinically manageable. Observed infection rates, which included COVID-19, were generally low. Taken together, these data support the use of melflufen and dexamethasone in patients who have not received a previous ASCT or who underwent a successful ASCT (ie, TTP >36 months post-ASCT). In addition, the favorable efficacy profile and convenience of monthly outpatient infusions, especially for patients without access to other therapeutics such as CAR T-cell therapy or bispecific antibodies, bode well for this combination translating successfully into real-world practice.
Click to Show/Hide
|
||||
| Description |
Given the prognostic importance of TTP <36 months post-ASCT in OCEAN, we evaluated this prognostic factor in a post hoc analysis from the HORIZON study. Among 110 patients with triple-class refractory disease who had received ≥3 prior lines of therapy, 77 (70%) had received a previous ASCT and 58 (53%) had TTP <36 months post-ASCT (Suppl. Table S3). In patients with a TTP >36 months post-ASCT or no ASCT versus patients with a TTP <36 months post-ASCT, ORR was higher (29% vs 22%; Suppl. Table S4) and median DOR (7.6 months vs 3.9 months) and median PFS (4.2 months vs 3.4 months) were longer. Since pomalidomide and lenalidomide both belong to the immunomodulatory drugs, we analyzed if the duration of previous treatment with lenalidomide could have impacted the results. The median duration of lenalidomide was 14.4 months in patients with ASCT and TTP < 36 months, 38.3 months in patients with ASCT and TTP > 36 months, and 14.6 months in patients with no previous ASCT. However, the median PFS for patients treated with pomalidomide did not differ substantially between these groups of patients. The safety profile of melflufen and dexamethasone was generally consistent between patients with a TTP >36 months post-ASCT or no ASCT and patients with a TTP <36 months post-ASCT. In OCEAN among the melflufen group, the frequency of grade 3/4 TEAEs (88% and 92%), serious TEAEs (44% and 38%), and fatal adverse events (AEs; 11% and 13%) was similar in patients with a TTP >36 months post-ASCT or no ASCT and patients with TTP <36 months. However, patients with a TTP >36 months post-ASCT or no ASCT had lower rates of TEAEs leading to treatment discontinuation (23% and 31%), the longer median duration of study treatment (35.1 weeks vs 15.1 weeks), and longer median time to experiencing grade 3/4 thrombocytopenia (11.2 weeks vs 4.1 weeks) and grade 3/4 neutropenia (4.8 weeks vs 2.1 weeks) than patients with a TTP <36 months post-ASCT. In HORIZON, patients with a TTP >36 months post-ASCT or no ASCT had lower rates of grade 3/4 TEAEs (88% and 98%), but higher rates of serious TEAEs (64% and 53%) and similar rates of TEAEs leading to treatment discontinuation (29% and 33%) than patients with a TTP <36 months post-ASCT.
Click to Show/Hide
|
||||
| Experiment 382 Reporting the Activity Data of This PDC | [1] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Treatment-emergent adverse event |
27.00%
|
|||
| Patients Enrolled |
Patients with multi-refractory multiple myeloma.
|
||||
| Administration Time | 28-day cycle | ||||
| Administration Dosage | 40 mg with dexamethasone (40 mg) | ||||
| MOA of PDC |
Melflufen is highly lipophilic, which promotes its rapid uptake by cells. Once within the cell, melflufen releases its hydrophilic alkylator payloads via the hydrolytic activity of intracellular peptidases (e.g., aminopeptidases). Aminopeptidases are Zn2+-dependent metalloproteinases that remove amino acids at the N-terminal position from oligopeptides and have been associated with multiple tumorigenic processes such as proliferation, apoptosis, differentiation, angiogenesis, and motility. The dependence of melflufen on aminopeptidases was initially demonstrated by the reduced cytotoxic activity of melflufen-but not the alkylator melphalan-when cells were pretreated with bestatin, an antibiotic that is a potent aminopeptidase inhibitor. In addition, structure analogs designed to resist peptide hydrolysis (N-methyl derivative and derivative with D-amino acid) were shown to be almost 100-fold less potent than melflufen. Subsequent in vitro studies demonstrated that hydrolytic cleavage of melflufen by aminopeptidases releases alkylator payloads, including melphalan. In vitro, the activity of melflufen is multi-pronged, including induction of DNA damage, induction of apoptosis, inhibition of VEGF-dependent cell migration, and inhibition of tumor-associated angiogenesis, which have been further reviewed elsewhere. Downregulation of aminopeptidases resulted in reduced melflufen-mediated cytotoxic activity and apoptotic signaling in cultured cells.
Click to Show/Hide
|
||||
| Experiment 383 Reporting the Activity Data of This PDC | [9] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Treatment-emergent adverse event |
31%
|
|||
| Patients Enrolled |
101 relapsed/refractory multiple myeloma patients with TTP <36 month Post-ASCTb.
|
||||
| MOA of PDC |
In summary, the interpretation of the results from the OCEAN study were impacted by the heterogeneity of the population, with age and previous success of ASCT therapy identified as prognostic factors with study therapies. The safety profile of melflufen and dexamethasone is primarily characterized by hematologic AEs that are clinically manageable. Observed infection rates, which included COVID-19, were generally low. Taken together, these data support the use of melflufen and dexamethasone in patients who have not received a previous ASCT or who underwent a successful ASCT (ie, TTP >36 months post-ASCT). In addition, the favorable efficacy profile and convenience of monthly outpatient infusions, especially for patients without access to other therapeutics such as CAR T-cell therapy or bispecific antibodies, bode well for this combination translating successfully into real-world practice.
Click to Show/Hide
|
||||
| Description |
Given the prognostic importance of TTP <36 months post-ASCT in OCEAN, we evaluated this prognostic factor in a post hoc analysis from the HORIZON study. Among 110 patients with triple-class refractory disease who had received ≥3 prior lines of therapy, 77 (70%) had received a previous ASCT and 58 (53%) had TTP <36 months post-ASCT (Suppl. Table S3). In patients with a TTP >36 months post-ASCT or no ASCT versus patients with a TTP <36 months post-ASCT, ORR was higher (29% vs 22%; Suppl. Table S4) and median DOR (7.6 months vs 3.9 months) and median PFS (4.2 months vs 3.4 months) were longer. Since pomalidomide and lenalidomide both belong to the immunomodulatory drugs, we analyzed if the duration of previous treatment with lenalidomide could have impacted the results. The median duration of lenalidomide was 14.4 months in patients with ASCT and TTP < 36 months, 38.3 months in patients with ASCT and TTP > 36 months, and 14.6 months in patients with no previous ASCT. However, the median PFS for patients treated with pomalidomide did not differ substantially between these groups of patients. The safety profile of melflufen and dexamethasone was generally consistent between patients with a TTP >36 months post-ASCT or no ASCT and patients with a TTP <36 months post-ASCT. In OCEAN among the melflufen group, the frequency of grade 3/4 TEAEs (88% and 92%), serious TEAEs (44% and 38%), and fatal adverse events (AEs; 11% and 13%) was similar in patients with a TTP >36 months post-ASCT or no ASCT and patients with TTP <36 months. However, patients with a TTP >36 months post-ASCT or no ASCT had lower rates of TEAEs leading to treatment discontinuation (23% and 31%), the longer median duration of study treatment (35.1 weeks vs 15.1 weeks), and longer median time to experiencing grade 3/4 thrombocytopenia (11.2 weeks vs 4.1 weeks) and grade 3/4 neutropenia (4.8 weeks vs 2.1 weeks) than patients with a TTP <36 months post-ASCT. In HORIZON, patients with a TTP >36 months post-ASCT or no ASCT had lower rates of grade 3/4 TEAEs (88% and 98%), but higher rates of serious TEAEs (64% and 53%) and similar rates of TEAEs leading to treatment discontinuation (29% and 33%) than patients with a TTP <36 months post-ASCT.
Click to Show/Hide
|
||||
| Experiment 384 Reporting the Activity Data of This PDC | [9] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Treatment-emergent adverse event |
38%
|
|||
| Patients Enrolled |
101 relapsed/refractory multiple myeloma patients with TTP <36 month Post-ASCTb.
|
||||
| MOA of PDC |
In summary, the interpretation of the results from the OCEAN study were impacted by the heterogeneity of the population, with age and previous success of ASCT therapy identified as prognostic factors with study therapies. The safety profile of melflufen and dexamethasone is primarily characterized by hematologic AEs that are clinically manageable. Observed infection rates, which included COVID-19, were generally low. Taken together, these data support the use of melflufen and dexamethasone in patients who have not received a previous ASCT or who underwent a successful ASCT (ie, TTP >36 months post-ASCT). In addition, the favorable efficacy profile and convenience of monthly outpatient infusions, especially for patients without access to other therapeutics such as CAR T-cell therapy or bispecific antibodies, bode well for this combination translating successfully into real-world practice.
Click to Show/Hide
|
||||
| Description |
Given the prognostic importance of TTP <36 months post-ASCT in OCEAN, we evaluated this prognostic factor in a post hoc analysis from the HORIZON study. Among 110 patients with triple-class refractory disease who had received ≥3 prior lines of therapy, 77 (70%) had received a previous ASCT and 58 (53%) had TTP <36 months post-ASCT (Suppl. Table S3). In patients with a TTP >36 months post-ASCT or no ASCT versus patients with a TTP <36 months post-ASCT, ORR was higher (29% vs 22%; Suppl. Table S4) and median DOR (7.6 months vs 3.9 months) and median PFS (4.2 months vs 3.4 months) were longer. Since pomalidomide and lenalidomide both belong to the immunomodulatory drugs, we analyzed if the duration of previous treatment with lenalidomide could have impacted the results. The median duration of lenalidomide was 14.4 months in patients with ASCT and TTP < 36 months, 38.3 months in patients with ASCT and TTP > 36 months, and 14.6 months in patients with no previous ASCT. However, the median PFS for patients treated with pomalidomide did not differ substantially between these groups of patients. The safety profile of melflufen and dexamethasone was generally consistent between patients with a TTP >36 months post-ASCT or no ASCT and patients with a TTP <36 months post-ASCT. In OCEAN among the melflufen group, the frequency of grade 3/4 TEAEs (88% and 92%), serious TEAEs (44% and 38%), and fatal adverse events (AEs; 11% and 13%) was similar in patients with a TTP >36 months post-ASCT or no ASCT and patients with TTP <36 months. However, patients with a TTP >36 months post-ASCT or no ASCT had lower rates of TEAEs leading to treatment discontinuation (23% and 31%), the longer median duration of study treatment (35.1 weeks vs 15.1 weeks), and longer median time to experiencing grade 3/4 thrombocytopenia (11.2 weeks vs 4.1 weeks) and grade 3/4 neutropenia (4.8 weeks vs 2.1 weeks) than patients with a TTP <36 months post-ASCT. In HORIZON, patients with a TTP >36 months post-ASCT or no ASCT had lower rates of grade 3/4 TEAEs (88% and 98%), but higher rates of serious TEAEs (64% and 53%) and similar rates of TEAEs leading to treatment discontinuation (29% and 33%) than patients with a TTP <36 months post-ASCT.
Click to Show/Hide
|
||||
| Experiment 385 Reporting the Activity Data of This PDC | [9] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Treatment-emergent adverse event |
44%
|
|||
| Patients Enrolled |
145 patients who has relapsed/refractory multiple myeloma with no previous ASCT or TTP >36 month Post-ASCTa.
|
||||
| MOA of PDC |
In summary, the interpretation of the results from the OCEAN study were impacted by the heterogeneity of the population, with age and previous success of ASCT therapy identified as prognostic factors with study therapies. The safety profile of melflufen and dexamethasone is primarily characterized by hematologic AEs that are clinically manageable. Observed infection rates, which included COVID-19, were generally low. Taken together, these data support the use of melflufen and dexamethasone in patients who have not received a previous ASCT or who underwent a successful ASCT (ie, TTP >36 months post-ASCT). In addition, the favorable efficacy profile and convenience of monthly outpatient infusions, especially for patients without access to other therapeutics such as CAR T-cell therapy or bispecific antibodies, bode well for this combination translating successfully into real-world practice.
Click to Show/Hide
|
||||
| Description |
Given the prognostic importance of TTP <36 months post-ASCT in OCEAN, we evaluated this prognostic factor in a post hoc analysis from the HORIZON study. Among 110 patients with triple-class refractory disease who had received ≥3 prior lines of therapy, 77 (70%) had received a previous ASCT and 58 (53%) had TTP <36 months post-ASCT (Suppl. Table S3). In patients with a TTP >36 months post-ASCT or no ASCT versus patients with a TTP <36 months post-ASCT, ORR was higher (29% vs 22%; Suppl. Table S4) and median DOR (7.6 months vs 3.9 months) and median PFS (4.2 months vs 3.4 months) were longer. Since pomalidomide and lenalidomide both belong to the immunomodulatory drugs, we analyzed if the duration of previous treatment with lenalidomide could have impacted the results. The median duration of lenalidomide was 14.4 months in patients with ASCT and TTP < 36 months, 38.3 months in patients with ASCT and TTP > 36 months, and 14.6 months in patients with no previous ASCT. However, the median PFS for patients treated with pomalidomide did not differ substantially between these groups of patients. The safety profile of melflufen and dexamethasone was generally consistent between patients with a TTP >36 months post-ASCT or no ASCT and patients with a TTP <36 months post-ASCT. In OCEAN among the melflufen group, the frequency of grade 3/4 TEAEs (88% and 92%), serious TEAEs (44% and 38%), and fatal adverse events (AEs; 11% and 13%) was similar in patients with a TTP >36 months post-ASCT or no ASCT and patients with TTP <36 months. However, patients with a TTP >36 months post-ASCT or no ASCT had lower rates of TEAEs leading to treatment discontinuation (23% and 31%), the longer median duration of study treatment (35.1 weeks vs 15.1 weeks), and longer median time to experiencing grade 3/4 thrombocytopenia (11.2 weeks vs 4.1 weeks) and grade 3/4 neutropenia (4.8 weeks vs 2.1 weeks) than patients with a TTP <36 months post-ASCT. In HORIZON, patients with a TTP >36 months post-ASCT or no ASCT had lower rates of grade 3/4 TEAEs (88% and 98%), but higher rates of serious TEAEs (64% and 53%) and similar rates of TEAEs leading to treatment discontinuation (29% and 33%) than patients with a TTP <36 months post-ASCT.
Click to Show/Hide
|
||||
| Experiment 386 Reporting the Activity Data of This PDC | [9] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Treatment-emergent adverse event |
45%
|
|||
| Patients Enrolled |
101 relapsed/refractory multiple myeloma patients with TTP <36 month Post-ASCTb.
|
||||
| MOA of PDC |
In summary, the interpretation of the results from the OCEAN study were impacted by the heterogeneity of the population, with age and previous success of ASCT therapy identified as prognostic factors with study therapies. The safety profile of melflufen and dexamethasone is primarily characterized by hematologic AEs that are clinically manageable. Observed infection rates, which included COVID-19, were generally low. Taken together, these data support the use of melflufen and dexamethasone in patients who have not received a previous ASCT or who underwent a successful ASCT (ie, TTP >36 months post-ASCT). In addition, the favorable efficacy profile and convenience of monthly outpatient infusions, especially for patients without access to other therapeutics such as CAR T-cell therapy or bispecific antibodies, bode well for this combination translating successfully into real-world practice.
Click to Show/Hide
|
||||
| Description |
Given the prognostic importance of TTP <36 months post-ASCT in OCEAN, we evaluated this prognostic factor in a post hoc analysis from the HORIZON study. Among 110 patients with triple-class refractory disease who had received ≥3 prior lines of therapy, 77 (70%) had received a previous ASCT and 58 (53%) had TTP <36 months post-ASCT (Suppl. Table S3). In patients with a TTP >36 months post-ASCT or no ASCT versus patients with a TTP <36 months post-ASCT, ORR was higher (29% vs 22%; Suppl. Table S4) and median DOR (7.6 months vs 3.9 months) and median PFS (4.2 months vs 3.4 months) were longer. Since pomalidomide and lenalidomide both belong to the immunomodulatory drugs, we analyzed if the duration of previous treatment with lenalidomide could have impacted the results. The median duration of lenalidomide was 14.4 months in patients with ASCT and TTP < 36 months, 38.3 months in patients with ASCT and TTP > 36 months, and 14.6 months in patients with no previous ASCT. However, the median PFS for patients treated with pomalidomide did not differ substantially between these groups of patients. The safety profile of melflufen and dexamethasone was generally consistent between patients with a TTP >36 months post-ASCT or no ASCT and patients with a TTP <36 months post-ASCT. In OCEAN among the melflufen group, the frequency of grade 3/4 TEAEs (88% and 92%), serious TEAEs (44% and 38%), and fatal adverse events (AEs; 11% and 13%) was similar in patients with a TTP >36 months post-ASCT or no ASCT and patients with TTP <36 months. However, patients with a TTP >36 months post-ASCT or no ASCT had lower rates of TEAEs leading to treatment discontinuation (23% and 31%), the longer median duration of study treatment (35.1 weeks vs 15.1 weeks), and longer median time to experiencing grade 3/4 thrombocytopenia (11.2 weeks vs 4.1 weeks) and grade 3/4 neutropenia (4.8 weeks vs 2.1 weeks) than patients with a TTP <36 months post-ASCT. In HORIZON, patients with a TTP >36 months post-ASCT or no ASCT had lower rates of grade 3/4 TEAEs (88% and 98%), but higher rates of serious TEAEs (64% and 53%) and similar rates of TEAEs leading to treatment discontinuation (29% and 33%) than patients with a TTP <36 months post-ASCT.
Click to Show/Hide
|
||||
| Experiment 387 Reporting the Activity Data of This PDC | [9] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Treatment-emergent adverse event |
48%
|
|||
| Patients Enrolled |
145 patients who has relapsed/refractory multiple myeloma with no previous ASCT or TTP >36 month Post-ASCTa.
|
||||
| MOA of PDC |
In summary, the interpretation of the results from the OCEAN study were impacted by the heterogeneity of the population, with age and previous success of ASCT therapy identified as prognostic factors with study therapies. The safety profile of melflufen and dexamethasone is primarily characterized by hematologic AEs that are clinically manageable. Observed infection rates, which included COVID-19, were generally low. Taken together, these data support the use of melflufen and dexamethasone in patients who have not received a previous ASCT or who underwent a successful ASCT (ie, TTP >36 months post-ASCT). In addition, the favorable efficacy profile and convenience of monthly outpatient infusions, especially for patients without access to other therapeutics such as CAR T-cell therapy or bispecific antibodies, bode well for this combination translating successfully into real-world practice.
Click to Show/Hide
|
||||
| Description |
Given the prognostic importance of TTP <36 months post-ASCT in OCEAN, we evaluated this prognostic factor in a post hoc analysis from the HORIZON study. Among 110 patients with triple-class refractory disease who had received ≥3 prior lines of therapy, 77 (70%) had received a previous ASCT and 58 (53%) had TTP <36 months post-ASCT (Suppl. Table S3). In patients with a TTP >36 months post-ASCT or no ASCT versus patients with a TTP <36 months post-ASCT, ORR was higher (29% vs 22%; Suppl. Table S4) and median DOR (7.6 months vs 3.9 months) and median PFS (4.2 months vs 3.4 months) were longer. Since pomalidomide and lenalidomide both belong to the immunomodulatory drugs, we analyzed if the duration of previous treatment with lenalidomide could have impacted the results. The median duration of lenalidomide was 14.4 months in patients with ASCT and TTP < 36 months, 38.3 months in patients with ASCT and TTP > 36 months, and 14.6 months in patients with no previous ASCT. However, the median PFS for patients treated with pomalidomide did not differ substantially between these groups of patients. The safety profile of melflufen and dexamethasone was generally consistent between patients with a TTP >36 months post-ASCT or no ASCT and patients with a TTP <36 months post-ASCT. In OCEAN among the melflufen group, the frequency of grade 3/4 TEAEs (88% and 92%), serious TEAEs (44% and 38%), and fatal adverse events (AEs; 11% and 13%) was similar in patients with a TTP >36 months post-ASCT or no ASCT and patients with TTP <36 months. However, patients with a TTP >36 months post-ASCT or no ASCT had lower rates of TEAEs leading to treatment discontinuation (23% and 31%), the longer median duration of study treatment (35.1 weeks vs 15.1 weeks), and longer median time to experiencing grade 3/4 thrombocytopenia (11.2 weeks vs 4.1 weeks) and grade 3/4 neutropenia (4.8 weeks vs 2.1 weeks) than patients with a TTP <36 months post-ASCT. In HORIZON, patients with a TTP >36 months post-ASCT or no ASCT had lower rates of grade 3/4 TEAEs (88% and 98%), but higher rates of serious TEAEs (64% and 53%) and similar rates of TEAEs leading to treatment discontinuation (29% and 33%) than patients with a TTP <36 months post-ASCT.
Click to Show/Hide
|
||||
| Experiment 388 Reporting the Activity Data of This PDC | [9] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Treatment-emergent adverse event |
58%
|
|||
| Patients Enrolled |
145 patients who has relapsed/refractory multiple myeloma with no previous ASCT or TTP >36 month Post-ASCTa.
|
||||
| MOA of PDC |
In summary, the interpretation of the results from the OCEAN study were impacted by the heterogeneity of the population, with age and previous success of ASCT therapy identified as prognostic factors with study therapies. The safety profile of melflufen and dexamethasone is primarily characterized by hematologic AEs that are clinically manageable. Observed infection rates, which included COVID-19, were generally low. Taken together, these data support the use of melflufen and dexamethasone in patients who have not received a previous ASCT or who underwent a successful ASCT (ie, TTP >36 months post-ASCT). In addition, the favorable efficacy profile and convenience of monthly outpatient infusions, especially for patients without access to other therapeutics such as CAR T-cell therapy or bispecific antibodies, bode well for this combination translating successfully into real-world practice.
Click to Show/Hide
|
||||
| Description |
Given the prognostic importance of TTP <36 months post-ASCT in OCEAN, we evaluated this prognostic factor in a post hoc analysis from the HORIZON study. Among 110 patients with triple-class refractory disease who had received ≥3 prior lines of therapy, 77 (70%) had received a previous ASCT and 58 (53%) had TTP <36 months post-ASCT (Suppl. Table S3). In patients with a TTP >36 months post-ASCT or no ASCT versus patients with a TTP <36 months post-ASCT, ORR was higher (29% vs 22%; Suppl. Table S4) and median DOR (7.6 months vs 3.9 months) and median PFS (4.2 months vs 3.4 months) were longer. Since pomalidomide and lenalidomide both belong to the immunomodulatory drugs, we analyzed if the duration of previous treatment with lenalidomide could have impacted the results. The median duration of lenalidomide was 14.4 months in patients with ASCT and TTP < 36 months, 38.3 months in patients with ASCT and TTP > 36 months, and 14.6 months in patients with no previous ASCT. However, the median PFS for patients treated with pomalidomide did not differ substantially between these groups of patients. The safety profile of melflufen and dexamethasone was generally consistent between patients with a TTP >36 months post-ASCT or no ASCT and patients with a TTP <36 months post-ASCT. In OCEAN among the melflufen group, the frequency of grade 3/4 TEAEs (88% and 92%), serious TEAEs (44% and 38%), and fatal adverse events (AEs; 11% and 13%) was similar in patients with a TTP >36 months post-ASCT or no ASCT and patients with TTP <36 months. However, patients with a TTP >36 months post-ASCT or no ASCT had lower rates of TEAEs leading to treatment discontinuation (23% and 31%), the longer median duration of study treatment (35.1 weeks vs 15.1 weeks), and longer median time to experiencing grade 3/4 thrombocytopenia (11.2 weeks vs 4.1 weeks) and grade 3/4 neutropenia (4.8 weeks vs 2.1 weeks) than patients with a TTP <36 months post-ASCT. In HORIZON, patients with a TTP >36 months post-ASCT or no ASCT had lower rates of grade 3/4 TEAEs (88% and 98%), but higher rates of serious TEAEs (64% and 53%) and similar rates of TEAEs leading to treatment discontinuation (29% and 33%) than patients with a TTP <36 months post-ASCT.
Click to Show/Hide
|
||||
| Experiment 389 Reporting the Activity Data of This PDC | [9] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Treatment-emergent adverse event |
63%
|
|||
| Patients Enrolled |
101 relapsed/refractory multiple myeloma patients with TTP <36 month Post-ASCTb.
|
||||
| MOA of PDC |
In summary, the interpretation of the results from the OCEAN study were impacted by the heterogeneity of the population, with age and previous success of ASCT therapy identified as prognostic factors with study therapies. The safety profile of melflufen and dexamethasone is primarily characterized by hematologic AEs that are clinically manageable. Observed infection rates, which included COVID-19, were generally low. Taken together, these data support the use of melflufen and dexamethasone in patients who have not received a previous ASCT or who underwent a successful ASCT (ie, TTP >36 months post-ASCT). In addition, the favorable efficacy profile and convenience of monthly outpatient infusions, especially for patients without access to other therapeutics such as CAR T-cell therapy or bispecific antibodies, bode well for this combination translating successfully into real-world practice.
Click to Show/Hide
|
||||
| Description |
Given the prognostic importance of TTP <36 months post-ASCT in OCEAN, we evaluated this prognostic factor in a post hoc analysis from the HORIZON study. Among 110 patients with triple-class refractory disease who had received ≥3 prior lines of therapy, 77 (70%) had received a previous ASCT and 58 (53%) had TTP <36 months post-ASCT (Suppl. Table S3). In patients with a TTP >36 months post-ASCT or no ASCT versus patients with a TTP <36 months post-ASCT, ORR was higher (29% vs 22%; Suppl. Table S4) and median DOR (7.6 months vs 3.9 months) and median PFS (4.2 months vs 3.4 months) were longer. Since pomalidomide and lenalidomide both belong to the immunomodulatory drugs, we analyzed if the duration of previous treatment with lenalidomide could have impacted the results. The median duration of lenalidomide was 14.4 months in patients with ASCT and TTP < 36 months, 38.3 months in patients with ASCT and TTP > 36 months, and 14.6 months in patients with no previous ASCT. However, the median PFS for patients treated with pomalidomide did not differ substantially between these groups of patients. The safety profile of melflufen and dexamethasone was generally consistent between patients with a TTP >36 months post-ASCT or no ASCT and patients with a TTP <36 months post-ASCT. In OCEAN among the melflufen group, the frequency of grade 3/4 TEAEs (88% and 92%), serious TEAEs (44% and 38%), and fatal adverse events (AEs; 11% and 13%) was similar in patients with a TTP >36 months post-ASCT or no ASCT and patients with TTP <36 months. However, patients with a TTP >36 months post-ASCT or no ASCT had lower rates of TEAEs leading to treatment discontinuation (23% and 31%), the longer median duration of study treatment (35.1 weeks vs 15.1 weeks), and longer median time to experiencing grade 3/4 thrombocytopenia (11.2 weeks vs 4.1 weeks) and grade 3/4 neutropenia (4.8 weeks vs 2.1 weeks) than patients with a TTP <36 months post-ASCT. In HORIZON, patients with a TTP >36 months post-ASCT or no ASCT had lower rates of grade 3/4 TEAEs (88% and 98%), but higher rates of serious TEAEs (64% and 53%) and similar rates of TEAEs leading to treatment discontinuation (29% and 33%) than patients with a TTP <36 months post-ASCT.
Click to Show/Hide
|
||||
| Experiment 390 Reporting the Activity Data of This PDC | [5] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Treatment-emergent adverse event |
73.47%
|
|||
| Patients Enrolled |
153 patients refractory to prior alkylators (melflufen, n=78; pomalidomide, n=75).
|
||||
| MOA of PDC |
Melphalan flufenamide (melflufen), a first-in-class alkylating peptide-drug conjugate, plus dexamethasone demonstrated superior progression-free survival (PFS), but not overall survival (OS), versus pomalidomide plus dexamethasone in relapsed/refractory multiple myeloma in the OCEAN study. Time to progression (TTP) <36 months after a prior autologous stem cell transplantation (ASCT) was a negative prognostic factor for OS with melflufen. This post hoc exploratory analysis evaluated patients refractory to prior alkylators (e.g., cyclophosphamide and melphalan) in OCEAN. In 153 patients refractory to prior alkylators (melflufen, n = 78; pomalidomide, n = 75), the melflufen and pomalidomide arms had similar median PFS (5.6 months [95% CI, 4.2-8.3] vs. 4.7 months [95% CI, 3.1-7.3]; hazard ratio [HR], 0.92 [95% CI, 0.63-1.33]) and OS (23.4 months [95% CI, 14.4-31.7] vs. 20.0 months [95% CI, 12.0-28.7]; HR, 0.92 [95% CI, 0.62-1.38]). Among alkylator-refractory patients with a TTP 36 months after a prior ASCT or no prior ASCT (melflufen, n = 54; pomalidomide, n = 53), the observed median PFS and OS were longer in the melflufen arm than the pomalidomide arm. The safety profile of melflufen was consistent with previous reports. These results suggest that melflufen is safe and effective in patients with alkylator-refractory disease, suggesting differentiated activity from other alkylators.
Click to Show/Hide
|
||||
| Description |
Overall, the safety profile of melflufen plus dexamethasone in the alkylator-refractory group was consistent between treatment arms (Table 2). In the melflufen and pomalidomide arms, respectively, the frequency of treatment-emergent adverse events (TEAEs; 99% vs. 97%), Grade 3 or 4 TEAEs (85% vs. 82%), serious TEAEs (49% vs. 53%), and fatal TEAEs (19% vs. 16%) were similar (Table 2). However, melflufen compared with pomalidomide saw more dose modifications (76% vs. 67%) and dose reductions (47% vs. 14%), comparable dose delays (57% vs. 51%) but less treatment discontinuation (27% vs. 34%). When comparing patients refractory and not refractory to prior alkylators, rates of TEAEs were generally comparable except for slightly lower rates of serious and fatal TEAEs observed in patients not refractory to alkylators. Among Grade 3 or 4 TEAEs of special interest, melflufen saw more thrombocytopenia (73% vs. 14%), neutropenia (65% vs. 55%), and leukopenia or white blood cell decrease (14% vs. 3%), but less infection (15% vs. 26%), than pomalidomide. Notably, melflufen compared with pomalidomide saw a longer median time to dose reduction (106 days [range, 28-443] vs. 47 days [range, 28-225]), Grade 3 or 4 thrombocytopenia (52 days [range, 15-451] vs. 19 days [range, 8-91]), and Grade 3 or 4 neutropenia (36 days [range, 8-561] vs. 22 days [range, 8-470]).
Click to Show/Hide
|
||||
| Experiment 391 Reporting the Activity Data of This PDC | [5] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Treatment-emergent adverse event |
73.68%
|
|||
| Patients Enrolled |
153 patients refractory to prior alkylators (melflufen, n=78; pomalidomide, n=75).
|
||||
| MOA of PDC |
Melphalan flufenamide (melflufen), a first-in-class alkylating peptide-drug conjugate, plus dexamethasone demonstrated superior progression-free survival (PFS), but not overall survival (OS), versus pomalidomide plus dexamethasone in relapsed/refractory multiple myeloma in the OCEAN study. Time to progression (TTP) <36 months after a prior autologous stem cell transplantation (ASCT) was a negative prognostic factor for OS with melflufen. This post hoc exploratory analysis evaluated patients refractory to prior alkylators (e.g., cyclophosphamide and melphalan) in OCEAN. In 153 patients refractory to prior alkylators (melflufen, n = 78; pomalidomide, n = 75), the melflufen and pomalidomide arms had similar median PFS (5.6 months [95% CI, 4.2-8.3] vs. 4.7 months [95% CI, 3.1-7.3]; hazard ratio [HR], 0.92 [95% CI, 0.63-1.33]) and OS (23.4 months [95% CI, 14.4-31.7] vs. 20.0 months [95% CI, 12.0-28.7]; HR, 0.92 [95% CI, 0.62-1.38]). Among alkylator-refractory patients with a TTP 36 months after a prior ASCT or no prior ASCT (melflufen, n = 54; pomalidomide, n = 53), the observed median PFS and OS were longer in the melflufen arm than the pomalidomide arm. The safety profile of melflufen was consistent with previous reports. These results suggest that melflufen is safe and effective in patients with alkylator-refractory disease, suggesting differentiated activity from other alkylators.
Click to Show/Hide
|
||||
| Description |
Overall, the safety profile of melflufen plus dexamethasone in the alkylator-refractory group was consistent between treatment arms (Table 2). In the melflufen and pomalidomide arms, respectively, the frequency of treatment-emergent adverse events (TEAEs; 99% vs. 97%), Grade 3 or 4 TEAEs (85% vs. 82%), serious TEAEs (49% vs. 53%), and fatal TEAEs (19% vs. 16%) were similar (Table 2). However, melflufen compared with pomalidomide saw more dose modifications (76% vs. 67%) and dose reductions (47% vs. 14%), comparable dose delays (57% vs. 51%) but less treatment discontinuation (27% vs. 34%). When comparing patients refractory and not refractory to prior alkylators, rates of TEAEs were generally comparable except for slightly lower rates of serious and fatal TEAEs observed in patients not refractory to alkylators. Among Grade 3 or 4 TEAEs of special interest, melflufen saw more thrombocytopenia (73% vs. 14%), neutropenia (65% vs. 55%), and leukopenia or white blood cell decrease (14% vs. 3%), but less infection (15% vs. 26%), than pomalidomide. Notably, melflufen compared with pomalidomide saw a longer median time to dose reduction (106 days [range, 28-443] vs. 47 days [range, 28-225]), Grade 3 or 4 thrombocytopenia (52 days [range, 15-451] vs. 19 days [range, 8-91]), and Grade 3 or 4 neutropenia (36 days [range, 8-561] vs. 22 days [range, 8-470]).
Click to Show/Hide
|
||||
| Experiment 392 Reporting the Activity Data of This PDC | [5] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Treatment-emergent adverse event |
73.74%
|
|||
| Patients Enrolled |
153 patients refractory to prior alkylators (melflufen, n=78; pomalidomide, n=75).
|
||||
| MOA of PDC |
Melphalan flufenamide (melflufen), a first-in-class alkylating peptide-drug conjugate, plus dexamethasone demonstrated superior progression-free survival (PFS), but not overall survival (OS), versus pomalidomide plus dexamethasone in relapsed/refractory multiple myeloma in the OCEAN study. Time to progression (TTP) <36 months after a prior autologous stem cell transplantation (ASCT) was a negative prognostic factor for OS with melflufen. This post hoc exploratory analysis evaluated patients refractory to prior alkylators (e.g., cyclophosphamide and melphalan) in OCEAN. In 153 patients refractory to prior alkylators (melflufen, n = 78; pomalidomide, n = 75), the melflufen and pomalidomide arms had similar median PFS (5.6 months [95% CI, 4.2-8.3] vs. 4.7 months [95% CI, 3.1-7.3]; hazard ratio [HR], 0.92 [95% CI, 0.63-1.33]) and OS (23.4 months [95% CI, 14.4-31.7] vs. 20.0 months [95% CI, 12.0-28.7]; HR, 0.92 [95% CI, 0.62-1.38]). Among alkylator-refractory patients with a TTP 36 months after a prior ASCT or no prior ASCT (melflufen, n = 54; pomalidomide, n = 53), the observed median PFS and OS were longer in the melflufen arm than the pomalidomide arm. The safety profile of melflufen was consistent with previous reports. These results suggest that melflufen is safe and effective in patients with alkylator-refractory disease, suggesting differentiated activity from other alkylators.
Click to Show/Hide
|
||||
| Description |
Overall, the safety profile of melflufen plus dexamethasone in the alkylator-refractory group was consistent between treatment arms (Table 2). In the melflufen and pomalidomide arms, respectively, the frequency of treatment-emergent adverse events (TEAEs; 99% vs. 97%), Grade 3 or 4 TEAEs (85% vs. 82%), serious TEAEs (49% vs. 53%), and fatal TEAEs (19% vs. 16%) were similar (Table 2). However, melflufen compared with pomalidomide saw more dose modifications (76% vs. 67%) and dose reductions (47% vs. 14%), comparable dose delays (57% vs. 51%) but less treatment discontinuation (27% vs. 34%). When comparing patients refractory and not refractory to prior alkylators, rates of TEAEs were generally comparable except for slightly lower rates of serious and fatal TEAEs observed in patients not refractory to alkylators. Among Grade 3 or 4 TEAEs of special interest, melflufen saw more thrombocytopenia (73% vs. 14%), neutropenia (65% vs. 55%), and leukopenia or white blood cell decrease (14% vs. 3%), but less infection (15% vs. 26%), than pomalidomide. Notably, melflufen compared with pomalidomide saw a longer median time to dose reduction (106 days [range, 28-443] vs. 47 days [range, 28-225]), Grade 3 or 4 thrombocytopenia (52 days [range, 15-451] vs. 19 days [range, 8-91]), and Grade 3 or 4 neutropenia (36 days [range, 8-561] vs. 22 days [range, 8-470]).
Click to Show/Hide
|
||||
| Experiment 393 Reporting the Activity Data of This PDC | [5] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Treatment-emergent adverse event |
74.07%
|
|||
| Patients Enrolled |
153 patients refractory to prior alkylators (melflufen, n=78; pomalidomide, n=75).
|
||||
| MOA of PDC |
Melphalan flufenamide (melflufen), a first-in-class alkylating peptide-drug conjugate, plus dexamethasone demonstrated superior progression-free survival (PFS), but not overall survival (OS), versus pomalidomide plus dexamethasone in relapsed/refractory multiple myeloma in the OCEAN study. Time to progression (TTP) <36 months after a prior autologous stem cell transplantation (ASCT) was a negative prognostic factor for OS with melflufen. This post hoc exploratory analysis evaluated patients refractory to prior alkylators (e.g., cyclophosphamide and melphalan) in OCEAN. In 153 patients refractory to prior alkylators (melflufen, n = 78; pomalidomide, n = 75), the melflufen and pomalidomide arms had similar median PFS (5.6 months [95% CI, 4.2-8.3] vs. 4.7 months [95% CI, 3.1-7.3]; hazard ratio [HR], 0.92 [95% CI, 0.63-1.33]) and OS (23.4 months [95% CI, 14.4-31.7] vs. 20.0 months [95% CI, 12.0-28.7]; HR, 0.92 [95% CI, 0.62-1.38]). Among alkylator-refractory patients with a TTP 36 months after a prior ASCT or no prior ASCT (melflufen, n = 54; pomalidomide, n = 53), the observed median PFS and OS were longer in the melflufen arm than the pomalidomide arm. The safety profile of melflufen was consistent with previous reports. These results suggest that melflufen is safe and effective in patients with alkylator-refractory disease, suggesting differentiated activity from other alkylators.
Click to Show/Hide
|
||||
| Description |
Overall, the safety profile of melflufen plus dexamethasone in the alkylator-refractory group was consistent between treatment arms (Table 2). In the melflufen and pomalidomide arms, respectively, the frequency of treatment-emergent adverse events (TEAEs; 99% vs. 97%), Grade 3 or 4 TEAEs (85% vs. 82%), serious TEAEs (49% vs. 53%), and fatal TEAEs (19% vs. 16%) were similar (Table 2). However, melflufen compared with pomalidomide saw more dose modifications (76% vs. 67%) and dose reductions (47% vs. 14%), comparable dose delays (57% vs. 51%) but less treatment discontinuation (27% vs. 34%). When comparing patients refractory and not refractory to prior alkylators, rates of TEAEs were generally comparable except for slightly lower rates of serious and fatal TEAEs observed in patients not refractory to alkylators. Among Grade 3 or 4 TEAEs of special interest, melflufen saw more thrombocytopenia (73% vs. 14%), neutropenia (65% vs. 55%), and leukopenia or white blood cell decrease (14% vs. 3%), but less infection (15% vs. 26%), than pomalidomide. Notably, melflufen compared with pomalidomide saw a longer median time to dose reduction (106 days [range, 28-443] vs. 47 days [range, 28-225]), Grade 3 or 4 thrombocytopenia (52 days [range, 15-451] vs. 19 days [range, 8-91]), and Grade 3 or 4 neutropenia (36 days [range, 8-561] vs. 22 days [range, 8-470]).
Click to Show/Hide
|
||||
| Experiment 394 Reporting the Activity Data of This PDC | [5] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Treatment-emergent adverse event |
74.12%
|
|||
| Patients Enrolled |
153 patients refractory to prior alkylators (melflufen, n=78; pomalidomide, n=75).
|
||||
| MOA of PDC |
Melphalan flufenamide (melflufen), a first-in-class alkylating peptide-drug conjugate, plus dexamethasone demonstrated superior progression-free survival (PFS), but not overall survival (OS), versus pomalidomide plus dexamethasone in relapsed/refractory multiple myeloma in the OCEAN study. Time to progression (TTP) <36 months after a prior autologous stem cell transplantation (ASCT) was a negative prognostic factor for OS with melflufen. This post hoc exploratory analysis evaluated patients refractory to prior alkylators (e.g., cyclophosphamide and melphalan) in OCEAN. In 153 patients refractory to prior alkylators (melflufen, n = 78; pomalidomide, n = 75), the melflufen and pomalidomide arms had similar median PFS (5.6 months [95% CI, 4.2-8.3] vs. 4.7 months [95% CI, 3.1-7.3]; hazard ratio [HR], 0.92 [95% CI, 0.63-1.33]) and OS (23.4 months [95% CI, 14.4-31.7] vs. 20.0 months [95% CI, 12.0-28.7]; HR, 0.92 [95% CI, 0.62-1.38]). Among alkylator-refractory patients with a TTP 36 months after a prior ASCT or no prior ASCT (melflufen, n = 54; pomalidomide, n = 53), the observed median PFS and OS were longer in the melflufen arm than the pomalidomide arm. The safety profile of melflufen was consistent with previous reports. These results suggest that melflufen is safe and effective in patients with alkylator-refractory disease, suggesting differentiated activity from other alkylators.
Click to Show/Hide
|
||||
| Description |
Overall, the safety profile of melflufen plus dexamethasone in the alkylator-refractory group was consistent between treatment arms (Table 2). In the melflufen and pomalidomide arms, respectively, the frequency of treatment-emergent adverse events (TEAEs; 99% vs. 97%), Grade 3 or 4 TEAEs (85% vs. 82%), serious TEAEs (49% vs. 53%), and fatal TEAEs (19% vs. 16%) were similar (Table 2). However, melflufen compared with pomalidomide saw more dose modifications (76% vs. 67%) and dose reductions (47% vs. 14%), comparable dose delays (57% vs. 51%) but less treatment discontinuation (27% vs. 34%). When comparing patients refractory and not refractory to prior alkylators, rates of TEAEs were generally comparable except for slightly lower rates of serious and fatal TEAEs observed in patients not refractory to alkylators. Among Grade 3 or 4 TEAEs of special interest, melflufen saw more thrombocytopenia (73% vs. 14%), neutropenia (65% vs. 55%), and leukopenia or white blood cell decrease (14% vs. 3%), but less infection (15% vs. 26%), than pomalidomide. Notably, melflufen compared with pomalidomide saw a longer median time to dose reduction (106 days [range, 28-443] vs. 47 days [range, 28-225]), Grade 3 or 4 thrombocytopenia (52 days [range, 15-451] vs. 19 days [range, 8-91]), and Grade 3 or 4 neutropenia (36 days [range, 8-561] vs. 22 days [range, 8-470]).
Click to Show/Hide
|
||||
| Experiment 395 Reporting the Activity Data of This PDC | [5] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Treatment-emergent adverse event |
74.47%
|
|||
| Patients Enrolled |
153 patients refractory to prior alkylators (melflufen, n=78; pomalidomide, n=75).
|
||||
| MOA of PDC |
Melphalan flufenamide (melflufen), a first-in-class alkylating peptide-drug conjugate, plus dexamethasone demonstrated superior progression-free survival (PFS), but not overall survival (OS), versus pomalidomide plus dexamethasone in relapsed/refractory multiple myeloma in the OCEAN study. Time to progression (TTP) <36 months after a prior autologous stem cell transplantation (ASCT) was a negative prognostic factor for OS with melflufen. This post hoc exploratory analysis evaluated patients refractory to prior alkylators (e.g., cyclophosphamide and melphalan) in OCEAN. In 153 patients refractory to prior alkylators (melflufen, n = 78; pomalidomide, n = 75), the melflufen and pomalidomide arms had similar median PFS (5.6 months [95% CI, 4.2-8.3] vs. 4.7 months [95% CI, 3.1-7.3]; hazard ratio [HR], 0.92 [95% CI, 0.63-1.33]) and OS (23.4 months [95% CI, 14.4-31.7] vs. 20.0 months [95% CI, 12.0-28.7]; HR, 0.92 [95% CI, 0.62-1.38]). Among alkylator-refractory patients with a TTP 36 months after a prior ASCT or no prior ASCT (melflufen, n = 54; pomalidomide, n = 53), the observed median PFS and OS were longer in the melflufen arm than the pomalidomide arm. The safety profile of melflufen was consistent with previous reports. These results suggest that melflufen is safe and effective in patients with alkylator-refractory disease, suggesting differentiated activity from other alkylators.
Click to Show/Hide
|
||||
| Description |
Overall, the safety profile of melflufen plus dexamethasone in the alkylator-refractory group was consistent between treatment arms (Table 2). In the melflufen and pomalidomide arms, respectively, the frequency of treatment-emergent adverse events (TEAEs; 99% vs. 97%), Grade 3 or 4 TEAEs (85% vs. 82%), serious TEAEs (49% vs. 53%), and fatal TEAEs (19% vs. 16%) were similar (Table 2). However, melflufen compared with pomalidomide saw more dose modifications (76% vs. 67%) and dose reductions (47% vs. 14%), comparable dose delays (57% vs. 51%) but less treatment discontinuation (27% vs. 34%). When comparing patients refractory and not refractory to prior alkylators, rates of TEAEs were generally comparable except for slightly lower rates of serious and fatal TEAEs observed in patients not refractory to alkylators. Among Grade 3 or 4 TEAEs of special interest, melflufen saw more thrombocytopenia (73% vs. 14%), neutropenia (65% vs. 55%), and leukopenia or white blood cell decrease (14% vs. 3%), but less infection (15% vs. 26%), than pomalidomide. Notably, melflufen compared with pomalidomide saw a longer median time to dose reduction (106 days [range, 28-443] vs. 47 days [range, 28-225]), Grade 3 or 4 thrombocytopenia (52 days [range, 15-451] vs. 19 days [range, 8-91]), and Grade 3 or 4 neutropenia (36 days [range, 8-561] vs. 22 days [range, 8-470]).
Click to Show/Hide
|
||||
| Experiment 396 Reporting the Activity Data of This PDC | [1] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Treatment-emergent adverse event |
82.00%
|
|||
| Patients Enrolled |
Patients with multi-refractory multiple myeloma.
|
||||
| Administration Time | 6.2 month (median) | ||||
| Administration Dosage | 30 or 40 mg | ||||
| MOA of PDC |
Melflufen is highly lipophilic, which promotes its rapid uptake by cells. Once within the cell, melflufen releases its hydrophilic alkylator payloads via the hydrolytic activity of intracellular peptidases (e.g., aminopeptidases). Aminopeptidases are Zn2+-dependent metalloproteinases that remove amino acids at the N-terminal position from oligopeptides and have been associated with multiple tumorigenic processes such as proliferation, apoptosis, differentiation, angiogenesis, and motility. The dependence of melflufen on aminopeptidases was initially demonstrated by the reduced cytotoxic activity of melflufen-but not the alkylator melphalan-when cells were pretreated with bestatin, an antibiotic that is a potent aminopeptidase inhibitor. In addition, structure analogs designed to resist peptide hydrolysis (N-methyl derivative and derivative with D-amino acid) were shown to be almost 100-fold less potent than melflufen. Subsequent in vitro studies demonstrated that hydrolytic cleavage of melflufen by aminopeptidases releases alkylator payloads, including melphalan. In vitro, the activity of melflufen is multi-pronged, including induction of DNA damage, induction of apoptosis, inhibition of VEGF-dependent cell migration, and inhibition of tumor-associated angiogenesis, which have been further reviewed elsewhere. Downregulation of aminopeptidases resulted in reduced melflufen-mediated cytotoxic activity and apoptotic signaling in cultured cells.
Click to Show/Hide
|
||||
| Experiment 397 Reporting the Activity Data of This PDC | [9] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Treatment-emergent adverse event |
88%
|
|||
| Patients Enrolled |
145 patients who has relapsed/refractory multiple myeloma with no previous ASCT or TTP >36 month Post-ASCTa.
|
||||
| MOA of PDC |
In summary, the interpretation of the results from the OCEAN study were impacted by the heterogeneity of the population, with age and previous success of ASCT therapy identified as prognostic factors with study therapies. The safety profile of melflufen and dexamethasone is primarily characterized by hematologic AEs that are clinically manageable. Observed infection rates, which included COVID-19, were generally low. Taken together, these data support the use of melflufen and dexamethasone in patients who have not received a previous ASCT or who underwent a successful ASCT (ie, TTP >36 months post-ASCT). In addition, the favorable efficacy profile and convenience of monthly outpatient infusions, especially for patients without access to other therapeutics such as CAR T-cell therapy or bispecific antibodies, bode well for this combination translating successfully into real-world practice.
Click to Show/Hide
|
||||
| Description |
Given the prognostic importance of TTP <36 months post-ASCT in OCEAN, we evaluated this prognostic factor in a post hoc analysis from the HORIZON study. Among 110 patients with triple-class refractory disease who had received ≥3 prior lines of therapy, 77 (70%) had received a previous ASCT and 58 (53%) had TTP <36 months post-ASCT (Suppl. Table S3). In patients with a TTP >36 months post-ASCT or no ASCT versus patients with a TTP <36 months post-ASCT, ORR was higher (29% vs 22%; Suppl. Table S4) and median DOR (7.6 months vs 3.9 months) and median PFS (4.2 months vs 3.4 months) were longer. Since pomalidomide and lenalidomide both belong to the immunomodulatory drugs, we analyzed if the duration of previous treatment with lenalidomide could have impacted the results. The median duration of lenalidomide was 14.4 months in patients with ASCT and TTP < 36 months, 38.3 months in patients with ASCT and TTP > 36 months, and 14.6 months in patients with no previous ASCT. However, the median PFS for patients treated with pomalidomide did not differ substantially between these groups of patients. The safety profile of melflufen and dexamethasone was generally consistent between patients with a TTP >36 months post-ASCT or no ASCT and patients with a TTP <36 months post-ASCT. In OCEAN among the melflufen group, the frequency of grade 3/4 TEAEs (88% and 92%), serious TEAEs (44% and 38%), and fatal adverse events (AEs; 11% and 13%) was similar in patients with a TTP >36 months post-ASCT or no ASCT and patients with TTP <36 months. However, patients with a TTP >36 months post-ASCT or no ASCT had lower rates of TEAEs leading to treatment discontinuation (23% and 31%), the longer median duration of study treatment (35.1 weeks vs 15.1 weeks), and longer median time to experiencing grade 3/4 thrombocytopenia (11.2 weeks vs 4.1 weeks) and grade 3/4 neutropenia (4.8 weeks vs 2.1 weeks) than patients with a TTP <36 months post-ASCT. In HORIZON, patients with a TTP >36 months post-ASCT or no ASCT had lower rates of grade 3/4 TEAEs (88% and 98%), but higher rates of serious TEAEs (64% and 53%) and similar rates of TEAEs leading to treatment discontinuation (29% and 33%) than patients with a TTP <36 months post-ASCT.
Click to Show/Hide
|
||||
| Experiment 398 Reporting the Activity Data of This PDC | [9] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Treatment-emergent adverse event |
92%
|
|||
| Patients Enrolled |
101 relapsed/refractory multiple myeloma patients with TTP <36 month Post-ASCTb.
|
||||
| MOA of PDC |
In summary, the interpretation of the results from the OCEAN study were impacted by the heterogeneity of the population, with age and previous success of ASCT therapy identified as prognostic factors with study therapies. The safety profile of melflufen and dexamethasone is primarily characterized by hematologic AEs that are clinically manageable. Observed infection rates, which included COVID-19, were generally low. Taken together, these data support the use of melflufen and dexamethasone in patients who have not received a previous ASCT or who underwent a successful ASCT (ie, TTP >36 months post-ASCT). In addition, the favorable efficacy profile and convenience of monthly outpatient infusions, especially for patients without access to other therapeutics such as CAR T-cell therapy or bispecific antibodies, bode well for this combination translating successfully into real-world practice.
Click to Show/Hide
|
||||
| Description |
Given the prognostic importance of TTP <36 months post-ASCT in OCEAN, we evaluated this prognostic factor in a post hoc analysis from the HORIZON study. Among 110 patients with triple-class refractory disease who had received ≥3 prior lines of therapy, 77 (70%) had received a previous ASCT and 58 (53%) had TTP <36 months post-ASCT (Suppl. Table S3). In patients with a TTP >36 months post-ASCT or no ASCT versus patients with a TTP <36 months post-ASCT, ORR was higher (29% vs 22%; Suppl. Table S4) and median DOR (7.6 months vs 3.9 months) and median PFS (4.2 months vs 3.4 months) were longer. Since pomalidomide and lenalidomide both belong to the immunomodulatory drugs, we analyzed if the duration of previous treatment with lenalidomide could have impacted the results. The median duration of lenalidomide was 14.4 months in patients with ASCT and TTP < 36 months, 38.3 months in patients with ASCT and TTP > 36 months, and 14.6 months in patients with no previous ASCT. However, the median PFS for patients treated with pomalidomide did not differ substantially between these groups of patients. The safety profile of melflufen and dexamethasone was generally consistent between patients with a TTP >36 months post-ASCT or no ASCT and patients with a TTP <36 months post-ASCT. In OCEAN among the melflufen group, the frequency of grade 3/4 TEAEs (88% and 92%), serious TEAEs (44% and 38%), and fatal adverse events (AEs; 11% and 13%) was similar in patients with a TTP >36 months post-ASCT or no ASCT and patients with TTP <36 months. However, patients with a TTP >36 months post-ASCT or no ASCT had lower rates of TEAEs leading to treatment discontinuation (23% and 31%), the longer median duration of study treatment (35.1 weeks vs 15.1 weeks), and longer median time to experiencing grade 3/4 thrombocytopenia (11.2 weeks vs 4.1 weeks) and grade 3/4 neutropenia (4.8 weeks vs 2.1 weeks) than patients with a TTP <36 months post-ASCT. In HORIZON, patients with a TTP >36 months post-ASCT or no ASCT had lower rates of grade 3/4 TEAEs (88% and 98%), but higher rates of serious TEAEs (64% and 53%) and similar rates of TEAEs leading to treatment discontinuation (29% and 33%) than patients with a TTP <36 months post-ASCT.
Click to Show/Hide
|
||||
| Experiment 399 Reporting the Activity Data of This PDC | [9] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Treatment-emergent adverse event |
99%
|
|||
| Patients Enrolled |
145 patients who has relapsed/refractory multiple myeloma with no previous ASCT or TTP >36 month Post-ASCTa.
|
||||
| MOA of PDC |
In summary, the interpretation of the results from the OCEAN study were impacted by the heterogeneity of the population, with age and previous success of ASCT therapy identified as prognostic factors with study therapies. The safety profile of melflufen and dexamethasone is primarily characterized by hematologic AEs that are clinically manageable. Observed infection rates, which included COVID-19, were generally low. Taken together, these data support the use of melflufen and dexamethasone in patients who have not received a previous ASCT or who underwent a successful ASCT (ie, TTP >36 months post-ASCT). In addition, the favorable efficacy profile and convenience of monthly outpatient infusions, especially for patients without access to other therapeutics such as CAR T-cell therapy or bispecific antibodies, bode well for this combination translating successfully into real-world practice.
Click to Show/Hide
|
||||
| Description |
Given the prognostic importance of TTP <36 months post-ASCT in OCEAN, we evaluated this prognostic factor in a post hoc analysis from the HORIZON study. Among 110 patients with triple-class refractory disease who had received ≥3 prior lines of therapy, 77 (70%) had received a previous ASCT and 58 (53%) had TTP <36 months post-ASCT (Suppl. Table S3). In patients with a TTP >36 months post-ASCT or no ASCT versus patients with a TTP <36 months post-ASCT, ORR was higher (29% vs 22%; Suppl. Table S4) and median DOR (7.6 months vs 3.9 months) and median PFS (4.2 months vs 3.4 months) were longer. Since pomalidomide and lenalidomide both belong to the immunomodulatory drugs, we analyzed if the duration of previous treatment with lenalidomide could have impacted the results. The median duration of lenalidomide was 14.4 months in patients with ASCT and TTP < 36 months, 38.3 months in patients with ASCT and TTP > 36 months, and 14.6 months in patients with no previous ASCT. However, the median PFS for patients treated with pomalidomide did not differ substantially between these groups of patients. The safety profile of melflufen and dexamethasone was generally consistent between patients with a TTP >36 months post-ASCT or no ASCT and patients with a TTP <36 months post-ASCT. In OCEAN among the melflufen group, the frequency of grade 3/4 TEAEs (88% and 92%), serious TEAEs (44% and 38%), and fatal adverse events (AEs; 11% and 13%) was similar in patients with a TTP >36 months post-ASCT or no ASCT and patients with TTP <36 months. However, patients with a TTP >36 months post-ASCT or no ASCT had lower rates of TEAEs leading to treatment discontinuation (23% and 31%), the longer median duration of study treatment (35.1 weeks vs 15.1 weeks), and longer median time to experiencing grade 3/4 thrombocytopenia (11.2 weeks vs 4.1 weeks) and grade 3/4 neutropenia (4.8 weeks vs 2.1 weeks) than patients with a TTP <36 months post-ASCT. In HORIZON, patients with a TTP >36 months post-ASCT or no ASCT had lower rates of grade 3/4 TEAEs (88% and 98%), but higher rates of serious TEAEs (64% and 53%) and similar rates of TEAEs leading to treatment discontinuation (29% and 33%) than patients with a TTP <36 months post-ASCT.
Click to Show/Hide
|
||||
| Experiment 400 Reporting the Activity Data of This PDC | [9] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Treatment-emergent adverse event |
99%
|
|||
| Patients Enrolled |
101 relapsed/refractory multiple myeloma patients with TTP <36 month Post-ASCTb.
|
||||
| MOA of PDC |
In summary, the interpretation of the results from the OCEAN study were impacted by the heterogeneity of the population, with age and previous success of ASCT therapy identified as prognostic factors with study therapies. The safety profile of melflufen and dexamethasone is primarily characterized by hematologic AEs that are clinically manageable. Observed infection rates, which included COVID-19, were generally low. Taken together, these data support the use of melflufen and dexamethasone in patients who have not received a previous ASCT or who underwent a successful ASCT (ie, TTP >36 months post-ASCT). In addition, the favorable efficacy profile and convenience of monthly outpatient infusions, especially for patients without access to other therapeutics such as CAR T-cell therapy or bispecific antibodies, bode well for this combination translating successfully into real-world practice.
Click to Show/Hide
|
||||
| Description |
Given the prognostic importance of TTP <36 months post-ASCT in OCEAN, we evaluated this prognostic factor in a post hoc analysis from the HORIZON study. Among 110 patients with triple-class refractory disease who had received ≥3 prior lines of therapy, 77 (70%) had received a previous ASCT and 58 (53%) had TTP <36 months post-ASCT (Suppl. Table S3). In patients with a TTP >36 months post-ASCT or no ASCT versus patients with a TTP <36 months post-ASCT, ORR was higher (29% vs 22%; Suppl. Table S4) and median DOR (7.6 months vs 3.9 months) and median PFS (4.2 months vs 3.4 months) were longer. Since pomalidomide and lenalidomide both belong to the immunomodulatory drugs, we analyzed if the duration of previous treatment with lenalidomide could have impacted the results. The median duration of lenalidomide was 14.4 months in patients with ASCT and TTP < 36 months, 38.3 months in patients with ASCT and TTP > 36 months, and 14.6 months in patients with no previous ASCT. However, the median PFS for patients treated with pomalidomide did not differ substantially between these groups of patients. The safety profile of melflufen and dexamethasone was generally consistent between patients with a TTP >36 months post-ASCT or no ASCT and patients with a TTP <36 months post-ASCT. In OCEAN among the melflufen group, the frequency of grade 3/4 TEAEs (88% and 92%), serious TEAEs (44% and 38%), and fatal adverse events (AEs; 11% and 13%) was similar in patients with a TTP >36 months post-ASCT or no ASCT and patients with TTP <36 months. However, patients with a TTP >36 months post-ASCT or no ASCT had lower rates of TEAEs leading to treatment discontinuation (23% and 31%), the longer median duration of study treatment (35.1 weeks vs 15.1 weeks), and longer median time to experiencing grade 3/4 thrombocytopenia (11.2 weeks vs 4.1 weeks) and grade 3/4 neutropenia (4.8 weeks vs 2.1 weeks) than patients with a TTP <36 months post-ASCT. In HORIZON, patients with a TTP >36 months post-ASCT or no ASCT had lower rates of grade 3/4 TEAEs (88% and 98%), but higher rates of serious TEAEs (64% and 53%) and similar rates of TEAEs leading to treatment discontinuation (29% and 33%) than patients with a TTP <36 months post-ASCT.
Click to Show/Hide
|
||||
| Experiment 401 Reporting the Activity Data of This PDC | [2] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Treatment-emergent adverse event rate |
82%
|
|||
| MOA of PDC |
Melphalan flufenamide (melflufen), a first-in-class alkylating peptide-drug conjugate, plus dexamethasone was approved in Europe for use in patients with triple-class refractory relapsed/refractory multiple myeloma (RRMM) with 3 prior lines of therapy and without prior autologous stem cell transplantation (ASCT) or with a time to progression >36 months after prior ASCT. The randomized LIGHTHOUSE study (NCT04649060) assessed melflufen plus daratumumab and dexamethasone (melflufen group) versus daratumumab in patients with RRMM with disease refractory to an immunomodulatory agent and a proteasome inhibitor or who had received 3 prior lines of therapy including an immunomodulatory agent and a proteasome inhibitor. A partial clinical hold issued by the US Food and Drug Administration for all melflufen studies led to financial constraints and premature study closure on February 23rd 2022 (data cut-off date). In total, 54 of 240 planned patients were randomized (melflufen group, N=27; daratumumab group, N=27). Median progression-free survival (PFS) was not reached in the melflufen group versus 4.9 months in the daratumumab group (Hazard Ratio: 0.18 [95% Confidence Interval, 0.05-0.65]; P=0.0032) at a median follow-up time of 7.1 and 6.6 months, respectively. Overall response rate (ORR) was 59% in the melflufen group versus 30% in the daratumumab group (P=0.0300). The most common grade 3 treatment-emergent adverse events in the melflufen group versus daratumumab group were neutropenia (50% vs. 12%), thrombocytopenia (50% vs. 8%), and anemia (32% vs. 19%). Melflufen plus daratumumab and dexamethasone demonstrated superior PFS and ORR versus daratumumab in RRMM and a safety profile comparable to previously published melflufen studies.
Click to Show/Hide
|
||||
| Description |
The safety population included patients who received ≥1 dose of melflufen, daratumumab, or dexamethasone (melflufen group) and 26 patients who received daratumumab monotherapy. In the safety population, ≥1 TEAE was reported in 21 patients (96%) with melflufen, daratumumab, and dexamethasone and 22 patients (85%) with daratumumab. Overall, grade ≥3 TEAE occurred in 18 patients (82%) with melflufen, daratumumab, and dexamethasone and 14 patients (54%) with daratumumab. The most common hematologic grade ≥3 TEAE were neutropenia (melflufen group, 11 patients [50%]; daratumumab group, 3 patients [12%]), thrombocytopenia (melflufen group, 11 patients [50%]; daratumumab group, 2 patients [8%]), and anemia (melflufen group, 7 patients [32%]; daratumumab group, 5 patients [19%]). The most common non-hematologic grade ≥3 TEAE were pneumonia (melflufen group, 2 patients [9%]; daratumumab group, 2 patients [8%]) and femur fracture (melflufen group, 0 patients [0%]; daratumumab group, 2 patients [8%]); of these, 1 event (5%) of pneumonia in the melflufen group and 1 event (4%) of femur fracture in the daratumumab group were considered treatment-related TEAE by the investigator. Serious AE occurred in 6 patients (27%) with melflufen, daratumumab, and dexamethasone, and 12 patients (46%) with daratumumab. The most common serious AE (occurring in ≥4 patients overall) were anemia (melflufen group, 2 patients [9%]; daratumumab group, 3 patients [12%]) and pneumonia (melflufen group, 2 patients [9%]; daratumumab group, 2 patients [8%]). TEAE leading to treatment discontinuation occurred in 2 patients (9%) in the melflufen group (neutropenia and thrombocytopenia, N=1 each) and 4 patients (15%) in the daratumumab group (anemia, disease progression, hypercalcemia, and renal failure, N=1 each). Overall, 5 patients died on study before the crossover: 2 patients who received melflufen, daratumumab, and dexamethasone (1 due to disease progression and 1 due to unknown reasons, both >30 days after the last dose of study treatment) and 3 patients who received daratumumab (1 due to disease progression and 1 due to unknown reasons, both ≤30 days after the last dose of study treatment and 1 due to an AE [COVID-19 pneumonia], >30 days after the last dose of study treatment). In addition, one patient who crossed over to receive melflufen, daratumumab, and dexamethasone after progression on daratumumab died.
Click to Show/Hide
|
||||
| In Vivo Model | 22 relapsed/refractory multiple myeloma. | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT04649060 | Clinical Status | Phase 3 | ||
| Clinical Description | This was a randomized, controlled, open-label, Phase 3 multicenter study which enrolled patients with Relapsed-Refractory Multiple Myeloma (RRMM) who were either double refractory to an Immunomodulatory Drug (IMiD) and a Proteasome Inhibitor (PI) (regardless of the number of prior lines of therapy), or had received at least 3 prior lines of therapy including an IMiD and a PI. Patients received treatment with melflufen+dexamethasone+daratumumab or daratumumab until documented progressive disease, unacceptable toxicity, or patient/treating physician decision. Patients in the daratumumab treatment arm had the option to receive treatment with melflufen+dexamethasone+daratumumab after confirmed progressive disease. | ||||
| Experiment 402 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Relapsed/Refractory multiple myeloma | ||||
| Efficacy Data | Treatment-emergent adverse event rate |
85.70%
|
|||
| Patients Enrolled |
14 patients with relapsed refractory multiple myeloma.
|
||||
| Administration Time | 28-day cycle | ||||
| Administration Dosage | 40 mg | ||||
| MOA of PDC |
Melphalan flufenamide (melflufen) is a first-in-class peptide-drug conjugate that utilizes increased peptidase expression to selectively release potent alkylating agents inside tumor cells. Melflufen is hydrolyzed by peptidases and esterases to melphalan either directly or through an intermediate metabolite, desethyl-melflufen. The high lipophilicity of melflufen facilitates passive diffusion across cell membranes. The activity and tolerability of melflufen in relapsed/refractory multiple myeloma (RRMM) were demonstrated in the O-12-M1 (NCT01897714), OCEAN (NCT03151811), and HORIZON (NCT02963493) trials.
Click to Show/Hide
|
||||
| Description |
Overall, at least one TEAE was reported in 13 (92.9%) and 13 (100.0%) patients in Arms A and B, respectively (Table 3). During cycle 1, 9 patients (64.3%) and 12 patients (92.3%), respectively, had at least one TEAE. Cumulatively, grade 3 or 4 AEs occurred in 12 (85.7%) and 12 (92.3%) patients, respectively, and serious AEs were reported in 5 (35.7%) and 9 (69.2%) patients, respectively. The most common any-grade AEs in Arms A and B, respectively, were thrombocytopenia (10 [71.4%]; 10 [76.9%]), neutropenia (9 [64.3%]; 9 [69.2%]), and anemia (9 [64.3%]; 7 [53.8%]). No phlebitis or local-infusion-related reactions were reported based on pre- and post-infusion inspection of the IV site, and there were no extravasations observed in Arm A or B. Similarly, VIP scores collected on Day 1 post-infusion and on Day 8 indicated that patients had healthy IV sites (VIP score of 0) with no signs of phlebitis following PVC administration of melflufen. The most common non-hematological AE was positive SARS-CoV-2 test (Arm A: 2 [14.3%]; Arm B: 4 [30.8%]). Pneumonia was the most common serious AE (Arm A: 2 [14.3%]; Arm B: 2 [15.4%]). The most common AE considered related to melflufen and/or dexamethasone by investigators was thrombocytopenia (Arm A: 10 [71.4%]; Arm B: 10 [76.9%]). AEs led to treatment discontinuation in 3 (21.4%) and 6 (46.2%) patients in Arms A and B, respectively.
Click to Show/Hide
|
||||
| Half life period | 75.6 h | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT04412707 | Clinical Status | Phase 2 | ||
| Clinical Description | This is a randomized, two-period, cross-over Phase 2 study, comparing PK, and assessing safety and tolerability and efficacy of peripheral and central intravenous administration of melflufen in patients with RRMM. It is an international study, enrolling patients in US and Europe. The study will enroll patients following at least 2 lines of prior therapy. | ||||
Revealed Based on the Cell Line Data
| Experiment 1 Reporting the Activity Data of This PDC | [11] | ||||
| Indication | Breast cancer | ||||
| Efficacy Data | Cell viability |
20%
|
|||
| Administration Time | 48 h | ||||
| Administration Dosage | 100 μM | ||||
| MOA of PDC |
Melphalan is a wellknown cancer drug used for decades for the treatment of various cancer types, and it is still widely used for hematological cancers today. It is an alkylating agent that works by adding an alkyl group to the guanine base of the DNA, resulting in an aberrant linkage between DNA strands, DNA breakage, and inhibition of DNA synthesis. Melphalan is a hydrophilic drug, and as such, it does not penetrate cell membranes easily, which is limiting to its anticancer potential. In contrast, melflufen (melphalan flufenamide), a new peptideconjugated alkylator, is highly lipophilic and therefore penetrates the cell membrane easily. Inside the cell, melflufen is rapidly hydrolyzed into less lipophilic metabolites that retain high alkylating potential, leading to their entrapment and accumulation. Aminopeptidases belong to a large family of enzymes that catalyze the cleavage of amino acids from the amino terminus of proteins or peptides and are shown to facilitate intracellular hydrolysis of melflufen. Aminopeptidases are involved in multiple cellular processes, and their expression and activity are frequently deregulated in cancer cells. For this reason, aminopeptidase inhibitors bestatin and tosedostat have been investigated in the clinical settings. Exploiting aminopeptidase activity to convert a lipophilic drug such as melflufen to an intracellular hydrophilic metabolite with high alkylating potential may offer an effective alternative therapeutic approach. Previously it has been shown that aminopeptidase N (ANPEP or CD13) can hydrolyze melflufen, but it is largely unknown whether melflufen can be a substrate for other aminopeptidases. Application of melflufen has mainly been focused on multiple myeloma, where it has shown promising results in phase 3 clinical trial in relapse and refractory patient population. 13 Yet it is unexplored whether melflufen can be effective in other cancer types such as breast cancer. Here, we demonstrate the efficacy of melflufen in D492HER2 breast epithelial cells overexpressing the HER2 oncogene and the triplenegative cell line MDAMB231.
Click to Show/Hide
|
||||
| Description |
D492HER2 cells showed increased sensitivity to melphalan compared to the progenitor cell line D492. However, concentration as high as 100 μmol/L was insufficient to kill the whole cell population. In both cell lines, around 40% of D492 cells and at least 20% of D492HER2 cells were still viable after incubation with 100 μmol/L melphalan. On the contrary, melflufen decreased viability of both D492 and D492HER2 cells at much lower doses.
Click to Show/Hide
|
||||
| In Vitro Model | Normal | D492 cell | CVCL_D1HJ | ||
| Experiment 2 Reporting the Activity Data of This PDC | [11] | ||||
| Indication | Breast cancer | ||||
| Efficacy Data | Cell viability |
20%
|
|||
| Administration Time | 48 h | ||||
| Administration Dosage | 10 μM | ||||
| MOA of PDC |
Melphalan is a wellknown cancer drug used for decades for the treatment of various cancer types, and it is still widely used for hematological cancers today. It is an alkylating agent that works by adding an alkyl group to the guanine base of the DNA, resulting in an aberrant linkage between DNA strands, DNA breakage, and inhibition of DNA synthesis. Melphalan is a hydrophilic drug, and as such, it does not penetrate cell membranes easily, which is limiting to its anticancer potential. In contrast, melflufen (melphalan flufenamide), a new peptideconjugated alkylator, is highly lipophilic and therefore penetrates the cell membrane easily. Inside the cell, melflufen is rapidly hydrolyzed into less lipophilic metabolites that retain high alkylating potential, leading to their entrapment and accumulation. Aminopeptidases belong to a large family of enzymes that catalyze the cleavage of amino acids from the amino terminus of proteins or peptides and are shown to facilitate intracellular hydrolysis of melflufen. Aminopeptidases are involved in multiple cellular processes, and their expression and activity are frequently deregulated in cancer cells. For this reason, aminopeptidase inhibitors bestatin and tosedostat have been investigated in the clinical settings. Exploiting aminopeptidase activity to convert a lipophilic drug such as melflufen to an intracellular hydrophilic metabolite with high alkylating potential may offer an effective alternative therapeutic approach. Previously it has been shown that aminopeptidase N (ANPEP or CD13) can hydrolyze melflufen, but it is largely unknown whether melflufen can be a substrate for other aminopeptidases. Application of melflufen has mainly been focused on multiple myeloma, where it has shown promising results in phase 3 clinical trial in relapse and refractory patient population. 13 Yet it is unexplored whether melflufen can be effective in other cancer types such as breast cancer. Here, we demonstrate the efficacy of melflufen in D492HER2 breast epithelial cells overexpressing the HER2 oncogene and the triplenegative cell line MDAMB231.
Click to Show/Hide
|
||||
| Description |
While these cells tolerated higher drug concentrations for both drugs compared to our D492 cell lines, melflufen was significantly more efficient than doxorubicin in killing the MDAMB231 cells (Figure 3C).
|
||||
| In Vitro Model | Breast adenocarcinoma | MDA-MB-231 cell | CVCL_0062 | ||
| Experiment 3 Reporting the Activity Data of This PDC | [11] | ||||
| Indication | Breast cancer | ||||
| Efficacy Data | Cell viability |
22%
|
|||
| Administration Time | 48 h | ||||
| Administration Dosage | 2.0 μM; with bestatin (10 μmol/L) | ||||
| MOA of PDC |
Melphalan is a wellknown cancer drug used for decades for the treatment of various cancer types, and it is still widely used for hematological cancers today. It is an alkylating agent that works by adding an alkyl group to the guanine base of the DNA, resulting in an aberrant linkage between DNA strands, DNA breakage, and inhibition of DNA synthesis. Melphalan is a hydrophilic drug, and as such, it does not penetrate cell membranes easily, which is limiting to its anticancer potential. In contrast, melflufen (melphalan flufenamide), a new peptideconjugated alkylator, is highly lipophilic and therefore penetrates the cell membrane easily. Inside the cell, melflufen is rapidly hydrolyzed into less lipophilic metabolites that retain high alkylating potential, leading to their entrapment and accumulation. Aminopeptidases belong to a large family of enzymes that catalyze the cleavage of amino acids from the amino terminus of proteins or peptides and are shown to facilitate intracellular hydrolysis of melflufen. Aminopeptidases are involved in multiple cellular processes, and their expression and activity are frequently deregulated in cancer cells. For this reason, aminopeptidase inhibitors bestatin and tosedostat have been investigated in the clinical settings. Exploiting aminopeptidase activity to convert a lipophilic drug such as melflufen to an intracellular hydrophilic metabolite with high alkylating potential may offer an effective alternative therapeutic approach. Previously it has been shown that aminopeptidase N (ANPEP or CD13) can hydrolyze melflufen, but it is largely unknown whether melflufen can be a substrate for other aminopeptidases. Application of melflufen has mainly been focused on multiple myeloma, where it has shown promising results in phase 3 clinical trial in relapse and refractory patient population. 13 Yet it is unexplored whether melflufen can be effective in other cancer types such as breast cancer. Here, we demonstrate the efficacy of melflufen in D492HER2 breast epithelial cells overexpressing the HER2 oncogene and the triplenegative cell line MDAMB231.
Click to Show/Hide
|
||||
| Description |
Aminopeptidases are thought to be responsible for the cleavage of melflufen, and indeed, in our model, the aminopeptidase inhibitor bestatin attenuated the activity of melflufen in D492HER2 cells. Interestingly, in D492 cells, preincubation with bestatin showed no effect on melflufen activity.
|
||||
| In Vitro Model | Normal | D492 cell | CVCL_D1HJ | ||
| Experiment 4 Reporting the Activity Data of This PDC | [11] | ||||
| Indication | Breast cancer | ||||
| Efficacy Data | Cell viability |
25%
|
|||
| Administration Time | 48 h | ||||
| Administration Dosage | 10 μM | ||||
| MOA of PDC |
Melphalan is a wellknown cancer drug used for decades for the treatment of various cancer types, and it is still widely used for hematological cancers today. It is an alkylating agent that works by adding an alkyl group to the guanine base of the DNA, resulting in an aberrant linkage between DNA strands, DNA breakage, and inhibition of DNA synthesis. Melphalan is a hydrophilic drug, and as such, it does not penetrate cell membranes easily, which is limiting to its anticancer potential. In contrast, melflufen (melphalan flufenamide), a new peptideconjugated alkylator, is highly lipophilic and therefore penetrates the cell membrane easily. Inside the cell, melflufen is rapidly hydrolyzed into less lipophilic metabolites that retain high alkylating potential, leading to their entrapment and accumulation. Aminopeptidases belong to a large family of enzymes that catalyze the cleavage of amino acids from the amino terminus of proteins or peptides and are shown to facilitate intracellular hydrolysis of melflufen. Aminopeptidases are involved in multiple cellular processes, and their expression and activity are frequently deregulated in cancer cells. For this reason, aminopeptidase inhibitors bestatin and tosedostat have been investigated in the clinical settings. Exploiting aminopeptidase activity to convert a lipophilic drug such as melflufen to an intracellular hydrophilic metabolite with high alkylating potential may offer an effective alternative therapeutic approach. Previously it has been shown that aminopeptidase N (ANPEP or CD13) can hydrolyze melflufen, but it is largely unknown whether melflufen can be a substrate for other aminopeptidases. Application of melflufen has mainly been focused on multiple myeloma, where it has shown promising results in phase 3 clinical trial in relapse and refractory patient population. 13 Yet it is unexplored whether melflufen can be effective in other cancer types such as breast cancer. Here, we demonstrate the efficacy of melflufen in D492HER2 breast epithelial cells overexpressing the HER2 oncogene and the triplenegative cell line MDAMB231.
Click to Show/Hide
|
||||
| Description |
D492HER2 cells showed increased sensitivity to melphalan compared to the progenitor cell line D492. However, concentration as high as 100 μmol/L was insufficient to kill the whole cell population. In both cell lines, around 40% of D492 cells and at least 20% of D492HER2 cells were still viable after incubation with 100 μmol/L melphalan. On the contrary, melflufen decreased viability of both D492 and D492HER2 cells at much lower doses.
Click to Show/Hide
|
||||
| In Vitro Model | Normal | D492 cell | CVCL_D1HJ | ||
| Experiment 5 Reporting the Activity Data of This PDC | [11] | ||||
| Indication | Breast cancer | ||||
| Efficacy Data | Cell viability |
25%
|
|||
| Administration Time | 48 h | ||||
| Administration Dosage | 75 μM | ||||
| MOA of PDC |
Melphalan is a wellknown cancer drug used for decades for the treatment of various cancer types, and it is still widely used for hematological cancers today. It is an alkylating agent that works by adding an alkyl group to the guanine base of the DNA, resulting in an aberrant linkage between DNA strands, DNA breakage, and inhibition of DNA synthesis. Melphalan is a hydrophilic drug, and as such, it does not penetrate cell membranes easily, which is limiting to its anticancer potential. In contrast, melflufen (melphalan flufenamide), a new peptideconjugated alkylator, is highly lipophilic and therefore penetrates the cell membrane easily. Inside the cell, melflufen is rapidly hydrolyzed into less lipophilic metabolites that retain high alkylating potential, leading to their entrapment and accumulation. Aminopeptidases belong to a large family of enzymes that catalyze the cleavage of amino acids from the amino terminus of proteins or peptides and are shown to facilitate intracellular hydrolysis of melflufen. Aminopeptidases are involved in multiple cellular processes, and their expression and activity are frequently deregulated in cancer cells. For this reason, aminopeptidase inhibitors bestatin and tosedostat have been investigated in the clinical settings. Exploiting aminopeptidase activity to convert a lipophilic drug such as melflufen to an intracellular hydrophilic metabolite with high alkylating potential may offer an effective alternative therapeutic approach. Previously it has been shown that aminopeptidase N (ANPEP or CD13) can hydrolyze melflufen, but it is largely unknown whether melflufen can be a substrate for other aminopeptidases. Application of melflufen has mainly been focused on multiple myeloma, where it has shown promising results in phase 3 clinical trial in relapse and refractory patient population. 13 Yet it is unexplored whether melflufen can be effective in other cancer types such as breast cancer. Here, we demonstrate the efficacy of melflufen in D492HER2 breast epithelial cells overexpressing the HER2 oncogene and the triplenegative cell line MDAMB231.
Click to Show/Hide
|
||||
| Description |
D492HER2 cells showed increased sensitivity to melphalan compared to the progenitor cell line D492. However, concentration as high as 100 μmol/L was insufficient to kill the whole cell population. In both cell lines, around 40% of D492 cells and at least 20% of D492HER2 cells were still viable after incubation with 100 μmol/L melphalan. On the contrary, melflufen decreased viability of both D492 and D492HER2 cells at much lower doses.
Click to Show/Hide
|
||||
| In Vitro Model | Normal | D492 cell | CVCL_D1HJ | ||
| Experiment 6 Reporting the Activity Data of This PDC | [11] | ||||
| Indication | Breast cancer | ||||
| Efficacy Data | Cell viability |
25%
|
|||
| Administration Time | 48 h | ||||
| Administration Dosage | 2.0 μM | ||||
| MOA of PDC |
Melphalan is a wellknown cancer drug used for decades for the treatment of various cancer types, and it is still widely used for hematological cancers today. It is an alkylating agent that works by adding an alkyl group to the guanine base of the DNA, resulting in an aberrant linkage between DNA strands, DNA breakage, and inhibition of DNA synthesis. Melphalan is a hydrophilic drug, and as such, it does not penetrate cell membranes easily, which is limiting to its anticancer potential. In contrast, melflufen (melphalan flufenamide), a new peptideconjugated alkylator, is highly lipophilic and therefore penetrates the cell membrane easily. Inside the cell, melflufen is rapidly hydrolyzed into less lipophilic metabolites that retain high alkylating potential, leading to their entrapment and accumulation. Aminopeptidases belong to a large family of enzymes that catalyze the cleavage of amino acids from the amino terminus of proteins or peptides and are shown to facilitate intracellular hydrolysis of melflufen. Aminopeptidases are involved in multiple cellular processes, and their expression and activity are frequently deregulated in cancer cells. For this reason, aminopeptidase inhibitors bestatin and tosedostat have been investigated in the clinical settings. Exploiting aminopeptidase activity to convert a lipophilic drug such as melflufen to an intracellular hydrophilic metabolite with high alkylating potential may offer an effective alternative therapeutic approach. Previously it has been shown that aminopeptidase N (ANPEP or CD13) can hydrolyze melflufen, but it is largely unknown whether melflufen can be a substrate for other aminopeptidases. Application of melflufen has mainly been focused on multiple myeloma, where it has shown promising results in phase 3 clinical trial in relapse and refractory patient population. 13 Yet it is unexplored whether melflufen can be effective in other cancer types such as breast cancer. Here, we demonstrate the efficacy of melflufen in D492HER2 breast epithelial cells overexpressing the HER2 oncogene and the triplenegative cell line MDAMB231.
Click to Show/Hide
|
||||
| Description |
Aminopeptidases are thought to be responsible for the cleavage of melflufen, and indeed, in our model, the aminopeptidase inhibitor bestatin attenuated the activity of melflufen in D492HER2 cells. Interestingly, in D492 cells, preincubation with bestatin showed no effect on melflufen activity.
|
||||
| In Vitro Model | Normal | D492 cell | CVCL_D1HJ | ||
| Experiment 7 Reporting the Activity Data of This PDC | [11] | ||||
| Indication | Breast cancer | ||||
| Efficacy Data | Cell viability |
25%
|
|||
| Administration Time | 48 h | ||||
| Administration Dosage | 2.0 μM | ||||
| MOA of PDC |
Melphalan is a wellknown cancer drug used for decades for the treatment of various cancer types, and it is still widely used for hematological cancers today. It is an alkylating agent that works by adding an alkyl group to the guanine base of the DNA, resulting in an aberrant linkage between DNA strands, DNA breakage, and inhibition of DNA synthesis. Melphalan is a hydrophilic drug, and as such, it does not penetrate cell membranes easily, which is limiting to its anticancer potential. In contrast, melflufen (melphalan flufenamide), a new peptideconjugated alkylator, is highly lipophilic and therefore penetrates the cell membrane easily. Inside the cell, melflufen is rapidly hydrolyzed into less lipophilic metabolites that retain high alkylating potential, leading to their entrapment and accumulation. Aminopeptidases belong to a large family of enzymes that catalyze the cleavage of amino acids from the amino terminus of proteins or peptides and are shown to facilitate intracellular hydrolysis of melflufen. Aminopeptidases are involved in multiple cellular processes, and their expression and activity are frequently deregulated in cancer cells. For this reason, aminopeptidase inhibitors bestatin and tosedostat have been investigated in the clinical settings. Exploiting aminopeptidase activity to convert a lipophilic drug such as melflufen to an intracellular hydrophilic metabolite with high alkylating potential may offer an effective alternative therapeutic approach. Previously it has been shown that aminopeptidase N (ANPEP or CD13) can hydrolyze melflufen, but it is largely unknown whether melflufen can be a substrate for other aminopeptidases. Application of melflufen has mainly been focused on multiple myeloma, where it has shown promising results in phase 3 clinical trial in relapse and refractory patient population. 13 Yet it is unexplored whether melflufen can be effective in other cancer types such as breast cancer. Here, we demonstrate the efficacy of melflufen in D492HER2 breast epithelial cells overexpressing the HER2 oncogene and the triplenegative cell line MDAMB231.
Click to Show/Hide
|
||||
| Description |
Aminopeptidases are thought to be responsible for the cleavage of melflufen, and indeed, in our model, the aminopeptidase inhibitor bestatin attenuated the activity of melflufen in D492HER2 cells. Interestingly, in D492 cells, preincubation with bestatin showed no effect on melflufen activity.
|
||||
| In Vitro Model | Normal | D492 cell | CVCL_D1HJ | ||
| Experiment 8 Reporting the Activity Data of This PDC | [11] | ||||
| Indication | Breast cancer | ||||
| Efficacy Data | Cell viability |
25%
|
|||
| Administration Time | 48 h | ||||
| Administration Dosage | 5 μM | ||||
| MOA of PDC |
Melphalan is a wellknown cancer drug used for decades for the treatment of various cancer types, and it is still widely used for hematological cancers today. It is an alkylating agent that works by adding an alkyl group to the guanine base of the DNA, resulting in an aberrant linkage between DNA strands, DNA breakage, and inhibition of DNA synthesis. Melphalan is a hydrophilic drug, and as such, it does not penetrate cell membranes easily, which is limiting to its anticancer potential. In contrast, melflufen (melphalan flufenamide), a new peptideconjugated alkylator, is highly lipophilic and therefore penetrates the cell membrane easily. Inside the cell, melflufen is rapidly hydrolyzed into less lipophilic metabolites that retain high alkylating potential, leading to their entrapment and accumulation. Aminopeptidases belong to a large family of enzymes that catalyze the cleavage of amino acids from the amino terminus of proteins or peptides and are shown to facilitate intracellular hydrolysis of melflufen. Aminopeptidases are involved in multiple cellular processes, and their expression and activity are frequently deregulated in cancer cells. For this reason, aminopeptidase inhibitors bestatin and tosedostat have been investigated in the clinical settings. Exploiting aminopeptidase activity to convert a lipophilic drug such as melflufen to an intracellular hydrophilic metabolite with high alkylating potential may offer an effective alternative therapeutic approach. Previously it has been shown that aminopeptidase N (ANPEP or CD13) can hydrolyze melflufen, but it is largely unknown whether melflufen can be a substrate for other aminopeptidases. Application of melflufen has mainly been focused on multiple myeloma, where it has shown promising results in phase 3 clinical trial in relapse and refractory patient population. 13 Yet it is unexplored whether melflufen can be effective in other cancer types such as breast cancer. Here, we demonstrate the efficacy of melflufen in D492HER2 breast epithelial cells overexpressing the HER2 oncogene and the triplenegative cell line MDAMB231.
Click to Show/Hide
|
||||
| Description |
While these cells tolerated higher drug concentrations for both drugs compared to our D492 cell lines, melflufen was significantly more efficient than doxorubicin in killing the MDAMB231 cells (Figure 3C).
|
||||
| In Vitro Model | Breast adenocarcinoma | MDA-MB-231 cell | CVCL_0062 | ||
| Experiment 9 Reporting the Activity Data of This PDC | [11] | ||||
| Indication | Breast cancer | ||||
| Efficacy Data | Cell viability |
30%
|
|||
| Administration Time | 48 h | ||||
| Administration Dosage | 50 μM | ||||
| MOA of PDC |
Melphalan is a wellknown cancer drug used for decades for the treatment of various cancer types, and it is still widely used for hematological cancers today. It is an alkylating agent that works by adding an alkyl group to the guanine base of the DNA, resulting in an aberrant linkage between DNA strands, DNA breakage, and inhibition of DNA synthesis. Melphalan is a hydrophilic drug, and as such, it does not penetrate cell membranes easily, which is limiting to its anticancer potential. In contrast, melflufen (melphalan flufenamide), a new peptideconjugated alkylator, is highly lipophilic and therefore penetrates the cell membrane easily. Inside the cell, melflufen is rapidly hydrolyzed into less lipophilic metabolites that retain high alkylating potential, leading to their entrapment and accumulation. Aminopeptidases belong to a large family of enzymes that catalyze the cleavage of amino acids from the amino terminus of proteins or peptides and are shown to facilitate intracellular hydrolysis of melflufen. Aminopeptidases are involved in multiple cellular processes, and their expression and activity are frequently deregulated in cancer cells. For this reason, aminopeptidase inhibitors bestatin and tosedostat have been investigated in the clinical settings. Exploiting aminopeptidase activity to convert a lipophilic drug such as melflufen to an intracellular hydrophilic metabolite with high alkylating potential may offer an effective alternative therapeutic approach. Previously it has been shown that aminopeptidase N (ANPEP or CD13) can hydrolyze melflufen, but it is largely unknown whether melflufen can be a substrate for other aminopeptidases. Application of melflufen has mainly been focused on multiple myeloma, where it has shown promising results in phase 3 clinical trial in relapse and refractory patient population. 13 Yet it is unexplored whether melflufen can be effective in other cancer types such as breast cancer. Here, we demonstrate the efficacy of melflufen in D492HER2 breast epithelial cells overexpressing the HER2 oncogene and the triplenegative cell line MDAMB231.
Click to Show/Hide
|
||||
| Description |
D492HER2 cells showed increased sensitivity to melphalan compared to the progenitor cell line D492. However, concentration as high as 100 μmol/L was insufficient to kill the whole cell population. In both cell lines, around 40% of D492 cells and at least 20% of D492HER2 cells were still viable after incubation with 100 μmol/L melphalan. On the contrary, melflufen decreased viability of both D492 and D492HER2 cells at much lower doses.
Click to Show/Hide
|
||||
| In Vitro Model | Normal | D492 cell | CVCL_D1HJ | ||
| Experiment 10 Reporting the Activity Data of This PDC | [11] | ||||
| Indication | Breast cancer | ||||
| Efficacy Data | Cell viability |
30%
|
|||
| Administration Time | 48 h | ||||
| Administration Dosage | 1.5 μM; with bestatin (10 μmol/L) | ||||
| MOA of PDC |
Melphalan is a wellknown cancer drug used for decades for the treatment of various cancer types, and it is still widely used for hematological cancers today. It is an alkylating agent that works by adding an alkyl group to the guanine base of the DNA, resulting in an aberrant linkage between DNA strands, DNA breakage, and inhibition of DNA synthesis. Melphalan is a hydrophilic drug, and as such, it does not penetrate cell membranes easily, which is limiting to its anticancer potential. In contrast, melflufen (melphalan flufenamide), a new peptideconjugated alkylator, is highly lipophilic and therefore penetrates the cell membrane easily. Inside the cell, melflufen is rapidly hydrolyzed into less lipophilic metabolites that retain high alkylating potential, leading to their entrapment and accumulation. Aminopeptidases belong to a large family of enzymes that catalyze the cleavage of amino acids from the amino terminus of proteins or peptides and are shown to facilitate intracellular hydrolysis of melflufen. Aminopeptidases are involved in multiple cellular processes, and their expression and activity are frequently deregulated in cancer cells. For this reason, aminopeptidase inhibitors bestatin and tosedostat have been investigated in the clinical settings. Exploiting aminopeptidase activity to convert a lipophilic drug such as melflufen to an intracellular hydrophilic metabolite with high alkylating potential may offer an effective alternative therapeutic approach. Previously it has been shown that aminopeptidase N (ANPEP or CD13) can hydrolyze melflufen, but it is largely unknown whether melflufen can be a substrate for other aminopeptidases. Application of melflufen has mainly been focused on multiple myeloma, where it has shown promising results in phase 3 clinical trial in relapse and refractory patient population. 13 Yet it is unexplored whether melflufen can be effective in other cancer types such as breast cancer. Here, we demonstrate the efficacy of melflufen in D492HER2 breast epithelial cells overexpressing the HER2 oncogene and the triplenegative cell line MDAMB231.
Click to Show/Hide
|
||||
| Description |
Aminopeptidases are thought to be responsible for the cleavage of melflufen, and indeed, in our model, the aminopeptidase inhibitor bestatin attenuated the activity of melflufen in D492HER2 cells. Interestingly, in D492 cells, preincubation with bestatin showed no effect on melflufen activity.
|
||||
| In Vitro Model | Normal | D492 cell | CVCL_D1HJ | ||
| Experiment 11 Reporting the Activity Data of This PDC | [11] | ||||
| Indication | Breast cancer | ||||
| Efficacy Data | Cell viability |
30%
|
|||
| Administration Time | 48 h | ||||
| Administration Dosage | 1.5 μM | ||||
| MOA of PDC |
Melphalan is a wellknown cancer drug used for decades for the treatment of various cancer types, and it is still widely used for hematological cancers today. It is an alkylating agent that works by adding an alkyl group to the guanine base of the DNA, resulting in an aberrant linkage between DNA strands, DNA breakage, and inhibition of DNA synthesis. Melphalan is a hydrophilic drug, and as such, it does not penetrate cell membranes easily, which is limiting to its anticancer potential. In contrast, melflufen (melphalan flufenamide), a new peptideconjugated alkylator, is highly lipophilic and therefore penetrates the cell membrane easily. Inside the cell, melflufen is rapidly hydrolyzed into less lipophilic metabolites that retain high alkylating potential, leading to their entrapment and accumulation. Aminopeptidases belong to a large family of enzymes that catalyze the cleavage of amino acids from the amino terminus of proteins or peptides and are shown to facilitate intracellular hydrolysis of melflufen. Aminopeptidases are involved in multiple cellular processes, and their expression and activity are frequently deregulated in cancer cells. For this reason, aminopeptidase inhibitors bestatin and tosedostat have been investigated in the clinical settings. Exploiting aminopeptidase activity to convert a lipophilic drug such as melflufen to an intracellular hydrophilic metabolite with high alkylating potential may offer an effective alternative therapeutic approach. Previously it has been shown that aminopeptidase N (ANPEP or CD13) can hydrolyze melflufen, but it is largely unknown whether melflufen can be a substrate for other aminopeptidases. Application of melflufen has mainly been focused on multiple myeloma, where it has shown promising results in phase 3 clinical trial in relapse and refractory patient population. 13 Yet it is unexplored whether melflufen can be effective in other cancer types such as breast cancer. Here, we demonstrate the efficacy of melflufen in D492HER2 breast epithelial cells overexpressing the HER2 oncogene and the triplenegative cell line MDAMB231.
Click to Show/Hide
|
||||
| Description |
Aminopeptidases are thought to be responsible for the cleavage of melflufen, and indeed, in our model, the aminopeptidase inhibitor bestatin attenuated the activity of melflufen in D492HER2 cells. Interestingly, in D492 cells, preincubation with bestatin showed no effect on melflufen activity.
|
||||
| In Vitro Model | Normal | D492 cell | CVCL_D1HJ | ||
| Experiment 12 Reporting the Activity Data of This PDC | [11] | ||||
| Indication | Breast cancer | ||||
| Efficacy Data | Cell viability |
35%
|
|||
| Administration Time | 48 h | ||||
| Administration Dosage | 1.0 μM | ||||
| MOA of PDC |
Melphalan is a wellknown cancer drug used for decades for the treatment of various cancer types, and it is still widely used for hematological cancers today. It is an alkylating agent that works by adding an alkyl group to the guanine base of the DNA, resulting in an aberrant linkage between DNA strands, DNA breakage, and inhibition of DNA synthesis. Melphalan is a hydrophilic drug, and as such, it does not penetrate cell membranes easily, which is limiting to its anticancer potential. In contrast, melflufen (melphalan flufenamide), a new peptideconjugated alkylator, is highly lipophilic and therefore penetrates the cell membrane easily. Inside the cell, melflufen is rapidly hydrolyzed into less lipophilic metabolites that retain high alkylating potential, leading to their entrapment and accumulation. Aminopeptidases belong to a large family of enzymes that catalyze the cleavage of amino acids from the amino terminus of proteins or peptides and are shown to facilitate intracellular hydrolysis of melflufen. Aminopeptidases are involved in multiple cellular processes, and their expression and activity are frequently deregulated in cancer cells. For this reason, aminopeptidase inhibitors bestatin and tosedostat have been investigated in the clinical settings. Exploiting aminopeptidase activity to convert a lipophilic drug such as melflufen to an intracellular hydrophilic metabolite with high alkylating potential may offer an effective alternative therapeutic approach. Previously it has been shown that aminopeptidase N (ANPEP or CD13) can hydrolyze melflufen, but it is largely unknown whether melflufen can be a substrate for other aminopeptidases. Application of melflufen has mainly been focused on multiple myeloma, where it has shown promising results in phase 3 clinical trial in relapse and refractory patient population. 13 Yet it is unexplored whether melflufen can be effective in other cancer types such as breast cancer. Here, we demonstrate the efficacy of melflufen in D492HER2 breast epithelial cells overexpressing the HER2 oncogene and the triplenegative cell line MDAMB231.
Click to Show/Hide
|
||||
| Description |
D492HER2 cells showed increased sensitivity to melphalan compared to the progenitor cell line D492. However, concentration as high as 100 μmol/L was insufficient to kill the whole cell population. In both cell lines, around 40% of D492 cells and at least 20% of D492HER2 cells were still viable after incubation with 100 μmol/L melphalan. On the contrary, melflufen decreased viability of both D492 and D492HER2 cells at much lower doses.
Click to Show/Hide
|
||||
| In Vitro Model | Normal | D492 cell | CVCL_D1HJ | ||
| Experiment 13 Reporting the Activity Data of This PDC | [11] | ||||
| Indication | Breast cancer | ||||
| Efficacy Data | Cell viability |
40%
|
|||
| Administration Time | 48 h | ||||
| Administration Dosage | 100 μM | ||||
| MOA of PDC |
Melphalan is a wellknown cancer drug used for decades for the treatment of various cancer types, and it is still widely used for hematological cancers today. It is an alkylating agent that works by adding an alkyl group to the guanine base of the DNA, resulting in an aberrant linkage between DNA strands, DNA breakage, and inhibition of DNA synthesis. Melphalan is a hydrophilic drug, and as such, it does not penetrate cell membranes easily, which is limiting to its anticancer potential. In contrast, melflufen (melphalan flufenamide), a new peptideconjugated alkylator, is highly lipophilic and therefore penetrates the cell membrane easily. Inside the cell, melflufen is rapidly hydrolyzed into less lipophilic metabolites that retain high alkylating potential, leading to their entrapment and accumulation. Aminopeptidases belong to a large family of enzymes that catalyze the cleavage of amino acids from the amino terminus of proteins or peptides and are shown to facilitate intracellular hydrolysis of melflufen. Aminopeptidases are involved in multiple cellular processes, and their expression and activity are frequently deregulated in cancer cells. For this reason, aminopeptidase inhibitors bestatin and tosedostat have been investigated in the clinical settings. Exploiting aminopeptidase activity to convert a lipophilic drug such as melflufen to an intracellular hydrophilic metabolite with high alkylating potential may offer an effective alternative therapeutic approach. Previously it has been shown that aminopeptidase N (ANPEP or CD13) can hydrolyze melflufen, but it is largely unknown whether melflufen can be a substrate for other aminopeptidases. Application of melflufen has mainly been focused on multiple myeloma, where it has shown promising results in phase 3 clinical trial in relapse and refractory patient population. 13 Yet it is unexplored whether melflufen can be effective in other cancer types such as breast cancer. Here, we demonstrate the efficacy of melflufen in D492HER2 breast epithelial cells overexpressing the HER2 oncogene and the triplenegative cell line MDAMB231.
Click to Show/Hide
|
||||
| Description |
D492HER2 cells showed increased sensitivity to melphalan compared to the progenitor cell line D492. However, concentration as high as 100 μmol/L was insufficient to kill the whole cell population. In both cell lines, around 40% of D492 cells and at least 20% of D492HER2 cells were still viable after incubation with 100 μmol/L melphalan. On the contrary, melflufen decreased viability of both D492 and D492HER2 cells at much lower doses.
Click to Show/Hide
|
||||
| In Vitro Model | Normal | D492 cell | CVCL_D1HJ | ||
| Experiment 14 Reporting the Activity Data of This PDC | [11] | ||||
| Indication | Breast cancer | ||||
| Efficacy Data | Cell viability |
40%
|
|||
| Administration Time | 48 h | ||||
| Administration Dosage | 2 μM | ||||
| MOA of PDC |
Melphalan is a wellknown cancer drug used for decades for the treatment of various cancer types, and it is still widely used for hematological cancers today. It is an alkylating agent that works by adding an alkyl group to the guanine base of the DNA, resulting in an aberrant linkage between DNA strands, DNA breakage, and inhibition of DNA synthesis. Melphalan is a hydrophilic drug, and as such, it does not penetrate cell membranes easily, which is limiting to its anticancer potential. In contrast, melflufen (melphalan flufenamide), a new peptideconjugated alkylator, is highly lipophilic and therefore penetrates the cell membrane easily. Inside the cell, melflufen is rapidly hydrolyzed into less lipophilic metabolites that retain high alkylating potential, leading to their entrapment and accumulation. Aminopeptidases belong to a large family of enzymes that catalyze the cleavage of amino acids from the amino terminus of proteins or peptides and are shown to facilitate intracellular hydrolysis of melflufen. Aminopeptidases are involved in multiple cellular processes, and their expression and activity are frequently deregulated in cancer cells. For this reason, aminopeptidase inhibitors bestatin and tosedostat have been investigated in the clinical settings. Exploiting aminopeptidase activity to convert a lipophilic drug such as melflufen to an intracellular hydrophilic metabolite with high alkylating potential may offer an effective alternative therapeutic approach. Previously it has been shown that aminopeptidase N (ANPEP or CD13) can hydrolyze melflufen, but it is largely unknown whether melflufen can be a substrate for other aminopeptidases. Application of melflufen has mainly been focused on multiple myeloma, where it has shown promising results in phase 3 clinical trial in relapse and refractory patient population. 13 Yet it is unexplored whether melflufen can be effective in other cancer types such as breast cancer. Here, we demonstrate the efficacy of melflufen in D492HER2 breast epithelial cells overexpressing the HER2 oncogene and the triplenegative cell line MDAMB231.
Click to Show/Hide
|
||||
| Description |
While these cells tolerated higher drug concentrations for both drugs compared to our D492 cell lines, melflufen was significantly more efficient than doxorubicin in killing the MDAMB231 cells (Figure 3C).
|
||||
| In Vitro Model | Breast adenocarcinoma | MDA-MB-231 cell | CVCL_0062 | ||
| Experiment 15 Reporting the Activity Data of This PDC | [11] | ||||
| Indication | Breast cancer | ||||
| Efficacy Data | Cell viability |
45%
|
|||
| Administration Time | 48 h | ||||
| Administration Dosage | 2.0 μM; with bestatin (10 μmol/L) | ||||
| MOA of PDC |
Melphalan is a wellknown cancer drug used for decades for the treatment of various cancer types, and it is still widely used for hematological cancers today. It is an alkylating agent that works by adding an alkyl group to the guanine base of the DNA, resulting in an aberrant linkage between DNA strands, DNA breakage, and inhibition of DNA synthesis. Melphalan is a hydrophilic drug, and as such, it does not penetrate cell membranes easily, which is limiting to its anticancer potential. In contrast, melflufen (melphalan flufenamide), a new peptideconjugated alkylator, is highly lipophilic and therefore penetrates the cell membrane easily. Inside the cell, melflufen is rapidly hydrolyzed into less lipophilic metabolites that retain high alkylating potential, leading to their entrapment and accumulation. Aminopeptidases belong to a large family of enzymes that catalyze the cleavage of amino acids from the amino terminus of proteins or peptides and are shown to facilitate intracellular hydrolysis of melflufen. Aminopeptidases are involved in multiple cellular processes, and their expression and activity are frequently deregulated in cancer cells. For this reason, aminopeptidase inhibitors bestatin and tosedostat have been investigated in the clinical settings. Exploiting aminopeptidase activity to convert a lipophilic drug such as melflufen to an intracellular hydrophilic metabolite with high alkylating potential may offer an effective alternative therapeutic approach. Previously it has been shown that aminopeptidase N (ANPEP or CD13) can hydrolyze melflufen, but it is largely unknown whether melflufen can be a substrate for other aminopeptidases. Application of melflufen has mainly been focused on multiple myeloma, where it has shown promising results in phase 3 clinical trial in relapse and refractory patient population. 13 Yet it is unexplored whether melflufen can be effective in other cancer types such as breast cancer. Here, we demonstrate the efficacy of melflufen in D492HER2 breast epithelial cells overexpressing the HER2 oncogene and the triplenegative cell line MDAMB231.
Click to Show/Hide
|
||||
| Description |
Aminopeptidases are thought to be responsible for the cleavage of melflufen, and indeed, in our model, the aminopeptidase inhibitor bestatin attenuated the activity of melflufen in D492HER2 cells. Interestingly, in D492 cells, preincubation with bestatin showed no effect on melflufen activity.
|
||||
| In Vitro Model | Normal | D492 cell | CVCL_D1HJ | ||
| Experiment 16 Reporting the Activity Data of This PDC | [11] | ||||
| Indication | Breast cancer | ||||
| Efficacy Data | Cell viability |
48%
|
|||
| Administration Time | 48 h | ||||
| Administration Dosage | 1.5 μM | ||||
| MOA of PDC |
Melphalan is a wellknown cancer drug used for decades for the treatment of various cancer types, and it is still widely used for hematological cancers today. It is an alkylating agent that works by adding an alkyl group to the guanine base of the DNA, resulting in an aberrant linkage between DNA strands, DNA breakage, and inhibition of DNA synthesis. Melphalan is a hydrophilic drug, and as such, it does not penetrate cell membranes easily, which is limiting to its anticancer potential. In contrast, melflufen (melphalan flufenamide), a new peptideconjugated alkylator, is highly lipophilic and therefore penetrates the cell membrane easily. Inside the cell, melflufen is rapidly hydrolyzed into less lipophilic metabolites that retain high alkylating potential, leading to their entrapment and accumulation. Aminopeptidases belong to a large family of enzymes that catalyze the cleavage of amino acids from the amino terminus of proteins or peptides and are shown to facilitate intracellular hydrolysis of melflufen. Aminopeptidases are involved in multiple cellular processes, and their expression and activity are frequently deregulated in cancer cells. For this reason, aminopeptidase inhibitors bestatin and tosedostat have been investigated in the clinical settings. Exploiting aminopeptidase activity to convert a lipophilic drug such as melflufen to an intracellular hydrophilic metabolite with high alkylating potential may offer an effective alternative therapeutic approach. Previously it has been shown that aminopeptidase N (ANPEP or CD13) can hydrolyze melflufen, but it is largely unknown whether melflufen can be a substrate for other aminopeptidases. Application of melflufen has mainly been focused on multiple myeloma, where it has shown promising results in phase 3 clinical trial in relapse and refractory patient population. 13 Yet it is unexplored whether melflufen can be effective in other cancer types such as breast cancer. Here, we demonstrate the efficacy of melflufen in D492HER2 breast epithelial cells overexpressing the HER2 oncogene and the triplenegative cell line MDAMB231.
Click to Show/Hide
|
||||
| Description |
Aminopeptidases are thought to be responsible for the cleavage of melflufen, and indeed, in our model, the aminopeptidase inhibitor bestatin attenuated the activity of melflufen in D492HER2 cells. Interestingly, in D492 cells, preincubation with bestatin showed no effect on melflufen activity.
|
||||
| In Vitro Model | Normal | D492 cell | CVCL_D1HJ | ||
| Experiment 17 Reporting the Activity Data of This PDC | [11] | ||||
| Indication | Breast cancer | ||||
| Efficacy Data | Cell viability |
50%
|
|||
| Administration Time | 48 h | ||||
| Administration Dosage | 75 μM | ||||
| MOA of PDC |
Melphalan is a wellknown cancer drug used for decades for the treatment of various cancer types, and it is still widely used for hematological cancers today. It is an alkylating agent that works by adding an alkyl group to the guanine base of the DNA, resulting in an aberrant linkage between DNA strands, DNA breakage, and inhibition of DNA synthesis. Melphalan is a hydrophilic drug, and as such, it does not penetrate cell membranes easily, which is limiting to its anticancer potential. In contrast, melflufen (melphalan flufenamide), a new peptideconjugated alkylator, is highly lipophilic and therefore penetrates the cell membrane easily. Inside the cell, melflufen is rapidly hydrolyzed into less lipophilic metabolites that retain high alkylating potential, leading to their entrapment and accumulation. Aminopeptidases belong to a large family of enzymes that catalyze the cleavage of amino acids from the amino terminus of proteins or peptides and are shown to facilitate intracellular hydrolysis of melflufen. Aminopeptidases are involved in multiple cellular processes, and their expression and activity are frequently deregulated in cancer cells. For this reason, aminopeptidase inhibitors bestatin and tosedostat have been investigated in the clinical settings. Exploiting aminopeptidase activity to convert a lipophilic drug such as melflufen to an intracellular hydrophilic metabolite with high alkylating potential may offer an effective alternative therapeutic approach. Previously it has been shown that aminopeptidase N (ANPEP or CD13) can hydrolyze melflufen, but it is largely unknown whether melflufen can be a substrate for other aminopeptidases. Application of melflufen has mainly been focused on multiple myeloma, where it has shown promising results in phase 3 clinical trial in relapse and refractory patient population. 13 Yet it is unexplored whether melflufen can be effective in other cancer types such as breast cancer. Here, we demonstrate the efficacy of melflufen in D492HER2 breast epithelial cells overexpressing the HER2 oncogene and the triplenegative cell line MDAMB231.
Click to Show/Hide
|
||||
| Description |
D492HER2 cells showed increased sensitivity to melphalan compared to the progenitor cell line D492. However, concentration as high as 100 μmol/L was insufficient to kill the whole cell population. In both cell lines, around 40% of D492 cells and at least 20% of D492HER2 cells were still viable after incubation with 100 μmol/L melphalan. On the contrary, melflufen decreased viability of both D492 and D492HER2 cells at much lower doses.
Click to Show/Hide
|
||||
| In Vitro Model | Normal | D492 cell | CVCL_D1HJ | ||
| Experiment 18 Reporting the Activity Data of This PDC | [11] | ||||
| Indication | Breast cancer | ||||
| Efficacy Data | Cell viability |
50%
|
|||
| Administration Time | 48 h | ||||
| Administration Dosage | 1.0 μM; with bestatin (10 μmol/L) | ||||
| MOA of PDC |
Melphalan is a wellknown cancer drug used for decades for the treatment of various cancer types, and it is still widely used for hematological cancers today. It is an alkylating agent that works by adding an alkyl group to the guanine base of the DNA, resulting in an aberrant linkage between DNA strands, DNA breakage, and inhibition of DNA synthesis. Melphalan is a hydrophilic drug, and as such, it does not penetrate cell membranes easily, which is limiting to its anticancer potential. In contrast, melflufen (melphalan flufenamide), a new peptideconjugated alkylator, is highly lipophilic and therefore penetrates the cell membrane easily. Inside the cell, melflufen is rapidly hydrolyzed into less lipophilic metabolites that retain high alkylating potential, leading to their entrapment and accumulation. Aminopeptidases belong to a large family of enzymes that catalyze the cleavage of amino acids from the amino terminus of proteins or peptides and are shown to facilitate intracellular hydrolysis of melflufen. Aminopeptidases are involved in multiple cellular processes, and their expression and activity are frequently deregulated in cancer cells. For this reason, aminopeptidase inhibitors bestatin and tosedostat have been investigated in the clinical settings. Exploiting aminopeptidase activity to convert a lipophilic drug such as melflufen to an intracellular hydrophilic metabolite with high alkylating potential may offer an effective alternative therapeutic approach. Previously it has been shown that aminopeptidase N (ANPEP or CD13) can hydrolyze melflufen, but it is largely unknown whether melflufen can be a substrate for other aminopeptidases. Application of melflufen has mainly been focused on multiple myeloma, where it has shown promising results in phase 3 clinical trial in relapse and refractory patient population. 13 Yet it is unexplored whether melflufen can be effective in other cancer types such as breast cancer. Here, we demonstrate the efficacy of melflufen in D492HER2 breast epithelial cells overexpressing the HER2 oncogene and the triplenegative cell line MDAMB231.
Click to Show/Hide
|
||||
| Description |
Aminopeptidases are thought to be responsible for the cleavage of melflufen, and indeed, in our model, the aminopeptidase inhibitor bestatin attenuated the activity of melflufen in D492HER2 cells. Interestingly, in D492 cells, preincubation with bestatin showed no effect on melflufen activity.
|
||||
| In Vitro Model | Normal | D492 cell | CVCL_D1HJ | ||
| Experiment 19 Reporting the Activity Data of This PDC | [11] | ||||
| Indication | Breast cancer | ||||
| Efficacy Data | Cell viability |
55%
|
|||
| Administration Time | 48 h | ||||
| Administration Dosage | 0.1 μM | ||||
| MOA of PDC |
Melphalan is a wellknown cancer drug used for decades for the treatment of various cancer types, and it is still widely used for hematological cancers today. It is an alkylating agent that works by adding an alkyl group to the guanine base of the DNA, resulting in an aberrant linkage between DNA strands, DNA breakage, and inhibition of DNA synthesis. Melphalan is a hydrophilic drug, and as such, it does not penetrate cell membranes easily, which is limiting to its anticancer potential. In contrast, melflufen (melphalan flufenamide), a new peptideconjugated alkylator, is highly lipophilic and therefore penetrates the cell membrane easily. Inside the cell, melflufen is rapidly hydrolyzed into less lipophilic metabolites that retain high alkylating potential, leading to their entrapment and accumulation. Aminopeptidases belong to a large family of enzymes that catalyze the cleavage of amino acids from the amino terminus of proteins or peptides and are shown to facilitate intracellular hydrolysis of melflufen. Aminopeptidases are involved in multiple cellular processes, and their expression and activity are frequently deregulated in cancer cells. For this reason, aminopeptidase inhibitors bestatin and tosedostat have been investigated in the clinical settings. Exploiting aminopeptidase activity to convert a lipophilic drug such as melflufen to an intracellular hydrophilic metabolite with high alkylating potential may offer an effective alternative therapeutic approach. Previously it has been shown that aminopeptidase N (ANPEP or CD13) can hydrolyze melflufen, but it is largely unknown whether melflufen can be a substrate for other aminopeptidases. Application of melflufen has mainly been focused on multiple myeloma, where it has shown promising results in phase 3 clinical trial in relapse and refractory patient population. 13 Yet it is unexplored whether melflufen can be effective in other cancer types such as breast cancer. Here, we demonstrate the efficacy of melflufen in D492HER2 breast epithelial cells overexpressing the HER2 oncogene and the triplenegative cell line MDAMB231.
Click to Show/Hide
|
||||
| Description |
D492HER2 cells showed increased sensitivity to melphalan compared to the progenitor cell line D492. However, concentration as high as 100 μmol/L was insufficient to kill the whole cell population. In both cell lines, around 40% of D492 cells and at least 20% of D492HER2 cells were still viable after incubation with 100 μmol/L melphalan. On the contrary, melflufen decreased viability of both D492 and D492HER2 cells at much lower doses.
Click to Show/Hide
|
||||
| In Vitro Model | Normal | D492 cell | CVCL_D1HJ | ||
| Experiment 20 Reporting the Activity Data of This PDC | [11] | ||||
| Indication | Breast cancer | ||||
| Efficacy Data | Cell viability |
55%
|
|||
| Administration Time | 48 h | ||||
| Administration Dosage | 1.0 μM | ||||
| MOA of PDC |
Melphalan is a wellknown cancer drug used for decades for the treatment of various cancer types, and it is still widely used for hematological cancers today. It is an alkylating agent that works by adding an alkyl group to the guanine base of the DNA, resulting in an aberrant linkage between DNA strands, DNA breakage, and inhibition of DNA synthesis. Melphalan is a hydrophilic drug, and as such, it does not penetrate cell membranes easily, which is limiting to its anticancer potential. In contrast, melflufen (melphalan flufenamide), a new peptideconjugated alkylator, is highly lipophilic and therefore penetrates the cell membrane easily. Inside the cell, melflufen is rapidly hydrolyzed into less lipophilic metabolites that retain high alkylating potential, leading to their entrapment and accumulation. Aminopeptidases belong to a large family of enzymes that catalyze the cleavage of amino acids from the amino terminus of proteins or peptides and are shown to facilitate intracellular hydrolysis of melflufen. Aminopeptidases are involved in multiple cellular processes, and their expression and activity are frequently deregulated in cancer cells. For this reason, aminopeptidase inhibitors bestatin and tosedostat have been investigated in the clinical settings. Exploiting aminopeptidase activity to convert a lipophilic drug such as melflufen to an intracellular hydrophilic metabolite with high alkylating potential may offer an effective alternative therapeutic approach. Previously it has been shown that aminopeptidase N (ANPEP or CD13) can hydrolyze melflufen, but it is largely unknown whether melflufen can be a substrate for other aminopeptidases. Application of melflufen has mainly been focused on multiple myeloma, where it has shown promising results in phase 3 clinical trial in relapse and refractory patient population. 13 Yet it is unexplored whether melflufen can be effective in other cancer types such as breast cancer. Here, we demonstrate the efficacy of melflufen in D492HER2 breast epithelial cells overexpressing the HER2 oncogene and the triplenegative cell line MDAMB231.
Click to Show/Hide
|
||||
| Description |
Aminopeptidases are thought to be responsible for the cleavage of melflufen, and indeed, in our model, the aminopeptidase inhibitor bestatin attenuated the activity of melflufen in D492HER2 cells. Interestingly, in D492 cells, preincubation with bestatin showed no effect on melflufen activity.
|
||||
| In Vitro Model | Normal | D492 cell | CVCL_D1HJ | ||
| Experiment 21 Reporting the Activity Data of This PDC | [11] | ||||
| Indication | Breast cancer | ||||
| Efficacy Data | Cell viability |
60%
|
|||
| Administration Time | 48 h | ||||
| Administration Dosage | 0.7 μM; with bestatin (10 μmol/L) | ||||
| MOA of PDC |
Melphalan is a wellknown cancer drug used for decades for the treatment of various cancer types, and it is still widely used for hematological cancers today. It is an alkylating agent that works by adding an alkyl group to the guanine base of the DNA, resulting in an aberrant linkage between DNA strands, DNA breakage, and inhibition of DNA synthesis. Melphalan is a hydrophilic drug, and as such, it does not penetrate cell membranes easily, which is limiting to its anticancer potential. In contrast, melflufen (melphalan flufenamide), a new peptideconjugated alkylator, is highly lipophilic and therefore penetrates the cell membrane easily. Inside the cell, melflufen is rapidly hydrolyzed into less lipophilic metabolites that retain high alkylating potential, leading to their entrapment and accumulation. Aminopeptidases belong to a large family of enzymes that catalyze the cleavage of amino acids from the amino terminus of proteins or peptides and are shown to facilitate intracellular hydrolysis of melflufen. Aminopeptidases are involved in multiple cellular processes, and their expression and activity are frequently deregulated in cancer cells. For this reason, aminopeptidase inhibitors bestatin and tosedostat have been investigated in the clinical settings. Exploiting aminopeptidase activity to convert a lipophilic drug such as melflufen to an intracellular hydrophilic metabolite with high alkylating potential may offer an effective alternative therapeutic approach. Previously it has been shown that aminopeptidase N (ANPEP or CD13) can hydrolyze melflufen, but it is largely unknown whether melflufen can be a substrate for other aminopeptidases. Application of melflufen has mainly been focused on multiple myeloma, where it has shown promising results in phase 3 clinical trial in relapse and refractory patient population. 13 Yet it is unexplored whether melflufen can be effective in other cancer types such as breast cancer. Here, we demonstrate the efficacy of melflufen in D492HER2 breast epithelial cells overexpressing the HER2 oncogene and the triplenegative cell line MDAMB231.
Click to Show/Hide
|
||||
| Description |
Aminopeptidases are thought to be responsible for the cleavage of melflufen, and indeed, in our model, the aminopeptidase inhibitor bestatin attenuated the activity of melflufen in D492HER2 cells. Interestingly, in D492 cells, preincubation with bestatin showed no effect on melflufen activity.
|
||||
| In Vitro Model | Normal | D492 cell | CVCL_D1HJ | ||
| Experiment 22 Reporting the Activity Data of This PDC | [11] | ||||
| Indication | Breast cancer | ||||
| Efficacy Data | Cell viability |
65%
|
|||
| Administration Time | 48 h | ||||
| Administration Dosage | 1.0 μM | ||||
| MOA of PDC |
Melphalan is a wellknown cancer drug used for decades for the treatment of various cancer types, and it is still widely used for hematological cancers today. It is an alkylating agent that works by adding an alkyl group to the guanine base of the DNA, resulting in an aberrant linkage between DNA strands, DNA breakage, and inhibition of DNA synthesis. Melphalan is a hydrophilic drug, and as such, it does not penetrate cell membranes easily, which is limiting to its anticancer potential. In contrast, melflufen (melphalan flufenamide), a new peptideconjugated alkylator, is highly lipophilic and therefore penetrates the cell membrane easily. Inside the cell, melflufen is rapidly hydrolyzed into less lipophilic metabolites that retain high alkylating potential, leading to their entrapment and accumulation. Aminopeptidases belong to a large family of enzymes that catalyze the cleavage of amino acids from the amino terminus of proteins or peptides and are shown to facilitate intracellular hydrolysis of melflufen. Aminopeptidases are involved in multiple cellular processes, and their expression and activity are frequently deregulated in cancer cells. For this reason, aminopeptidase inhibitors bestatin and tosedostat have been investigated in the clinical settings. Exploiting aminopeptidase activity to convert a lipophilic drug such as melflufen to an intracellular hydrophilic metabolite with high alkylating potential may offer an effective alternative therapeutic approach. Previously it has been shown that aminopeptidase N (ANPEP or CD13) can hydrolyze melflufen, but it is largely unknown whether melflufen can be a substrate for other aminopeptidases. Application of melflufen has mainly been focused on multiple myeloma, where it has shown promising results in phase 3 clinical trial in relapse and refractory patient population. 13 Yet it is unexplored whether melflufen can be effective in other cancer types such as breast cancer. Here, we demonstrate the efficacy of melflufen in D492HER2 breast epithelial cells overexpressing the HER2 oncogene and the triplenegative cell line MDAMB231.
Click to Show/Hide
|
||||
| Description |
D492HER2 cells showed increased sensitivity to melphalan compared to the progenitor cell line D492. However, concentration as high as 100 μmol/L was insufficient to kill the whole cell population. In both cell lines, around 40% of D492 cells and at least 20% of D492HER2 cells were still viable after incubation with 100 μmol/L melphalan. On the contrary, melflufen decreased viability of both D492 and D492HER2 cells at much lower doses.
Click to Show/Hide
|
||||
| In Vitro Model | Normal | D492 cell | CVCL_D1HJ | ||
| Experiment 23 Reporting the Activity Data of This PDC | [11] | ||||
| Indication | Breast cancer | ||||
| Efficacy Data | Cell viability |
65%
|
|||
| Administration Time | 48 h | ||||
| Administration Dosage | 0.7 μM | ||||
| MOA of PDC |
Melphalan is a wellknown cancer drug used for decades for the treatment of various cancer types, and it is still widely used for hematological cancers today. It is an alkylating agent that works by adding an alkyl group to the guanine base of the DNA, resulting in an aberrant linkage between DNA strands, DNA breakage, and inhibition of DNA synthesis. Melphalan is a hydrophilic drug, and as such, it does not penetrate cell membranes easily, which is limiting to its anticancer potential. In contrast, melflufen (melphalan flufenamide), a new peptideconjugated alkylator, is highly lipophilic and therefore penetrates the cell membrane easily. Inside the cell, melflufen is rapidly hydrolyzed into less lipophilic metabolites that retain high alkylating potential, leading to their entrapment and accumulation. Aminopeptidases belong to a large family of enzymes that catalyze the cleavage of amino acids from the amino terminus of proteins or peptides and are shown to facilitate intracellular hydrolysis of melflufen. Aminopeptidases are involved in multiple cellular processes, and their expression and activity are frequently deregulated in cancer cells. For this reason, aminopeptidase inhibitors bestatin and tosedostat have been investigated in the clinical settings. Exploiting aminopeptidase activity to convert a lipophilic drug such as melflufen to an intracellular hydrophilic metabolite with high alkylating potential may offer an effective alternative therapeutic approach. Previously it has been shown that aminopeptidase N (ANPEP or CD13) can hydrolyze melflufen, but it is largely unknown whether melflufen can be a substrate for other aminopeptidases. Application of melflufen has mainly been focused on multiple myeloma, where it has shown promising results in phase 3 clinical trial in relapse and refractory patient population. 13 Yet it is unexplored whether melflufen can be effective in other cancer types such as breast cancer. Here, we demonstrate the efficacy of melflufen in D492HER2 breast epithelial cells overexpressing the HER2 oncogene and the triplenegative cell line MDAMB231.
Click to Show/Hide
|
||||
| Description |
Aminopeptidases are thought to be responsible for the cleavage of melflufen, and indeed, in our model, the aminopeptidase inhibitor bestatin attenuated the activity of melflufen in D492HER2 cells. Interestingly, in D492 cells, preincubation with bestatin showed no effect on melflufen activity.
|
||||
| In Vitro Model | Normal | D492 cell | CVCL_D1HJ | ||
| Experiment 24 Reporting the Activity Data of This PDC | [11] | ||||
| Indication | Breast cancer | ||||
| Efficacy Data | Cell viability |
70%
|
|||
| Administration Time | 48 h | ||||
| Administration Dosage | 1.0 μM | ||||
| MOA of PDC |
Melphalan is a wellknown cancer drug used for decades for the treatment of various cancer types, and it is still widely used for hematological cancers today. It is an alkylating agent that works by adding an alkyl group to the guanine base of the DNA, resulting in an aberrant linkage between DNA strands, DNA breakage, and inhibition of DNA synthesis. Melphalan is a hydrophilic drug, and as such, it does not penetrate cell membranes easily, which is limiting to its anticancer potential. In contrast, melflufen (melphalan flufenamide), a new peptideconjugated alkylator, is highly lipophilic and therefore penetrates the cell membrane easily. Inside the cell, melflufen is rapidly hydrolyzed into less lipophilic metabolites that retain high alkylating potential, leading to their entrapment and accumulation. Aminopeptidases belong to a large family of enzymes that catalyze the cleavage of amino acids from the amino terminus of proteins or peptides and are shown to facilitate intracellular hydrolysis of melflufen. Aminopeptidases are involved in multiple cellular processes, and their expression and activity are frequently deregulated in cancer cells. For this reason, aminopeptidase inhibitors bestatin and tosedostat have been investigated in the clinical settings. Exploiting aminopeptidase activity to convert a lipophilic drug such as melflufen to an intracellular hydrophilic metabolite with high alkylating potential may offer an effective alternative therapeutic approach. Previously it has been shown that aminopeptidase N (ANPEP or CD13) can hydrolyze melflufen, but it is largely unknown whether melflufen can be a substrate for other aminopeptidases. Application of melflufen has mainly been focused on multiple myeloma, where it has shown promising results in phase 3 clinical trial in relapse and refractory patient population. 13 Yet it is unexplored whether melflufen can be effective in other cancer types such as breast cancer. Here, we demonstrate the efficacy of melflufen in D492HER2 breast epithelial cells overexpressing the HER2 oncogene and the triplenegative cell line MDAMB231.
Click to Show/Hide
|
||||
| Description |
Aminopeptidases are thought to be responsible for the cleavage of melflufen, and indeed, in our model, the aminopeptidase inhibitor bestatin attenuated the activity of melflufen in D492HER2 cells. Interestingly, in D492 cells, preincubation with bestatin showed no effect on melflufen activity.
|
||||
| In Vitro Model | Normal | D492 cell | CVCL_D1HJ | ||
| Experiment 25 Reporting the Activity Data of This PDC | [11] | ||||
| Indication | Breast cancer | ||||
| Efficacy Data | Cell viability |
70%
|
|||
| Administration Time | 48 h | ||||
| Administration Dosage | 0.5 μM | ||||
| MOA of PDC |
Melphalan is a wellknown cancer drug used for decades for the treatment of various cancer types, and it is still widely used for hematological cancers today. It is an alkylating agent that works by adding an alkyl group to the guanine base of the DNA, resulting in an aberrant linkage between DNA strands, DNA breakage, and inhibition of DNA synthesis. Melphalan is a hydrophilic drug, and as such, it does not penetrate cell membranes easily, which is limiting to its anticancer potential. In contrast, melflufen (melphalan flufenamide), a new peptideconjugated alkylator, is highly lipophilic and therefore penetrates the cell membrane easily. Inside the cell, melflufen is rapidly hydrolyzed into less lipophilic metabolites that retain high alkylating potential, leading to their entrapment and accumulation. Aminopeptidases belong to a large family of enzymes that catalyze the cleavage of amino acids from the amino terminus of proteins or peptides and are shown to facilitate intracellular hydrolysis of melflufen. Aminopeptidases are involved in multiple cellular processes, and their expression and activity are frequently deregulated in cancer cells. For this reason, aminopeptidase inhibitors bestatin and tosedostat have been investigated in the clinical settings. Exploiting aminopeptidase activity to convert a lipophilic drug such as melflufen to an intracellular hydrophilic metabolite with high alkylating potential may offer an effective alternative therapeutic approach. Previously it has been shown that aminopeptidase N (ANPEP or CD13) can hydrolyze melflufen, but it is largely unknown whether melflufen can be a substrate for other aminopeptidases. Application of melflufen has mainly been focused on multiple myeloma, where it has shown promising results in phase 3 clinical trial in relapse and refractory patient population. 13 Yet it is unexplored whether melflufen can be effective in other cancer types such as breast cancer. Here, we demonstrate the efficacy of melflufen in D492HER2 breast epithelial cells overexpressing the HER2 oncogene and the triplenegative cell line MDAMB231.
Click to Show/Hide
|
||||
| Description |
Aminopeptidases are thought to be responsible for the cleavage of melflufen, and indeed, in our model, the aminopeptidase inhibitor bestatin attenuated the activity of melflufen in D492HER2 cells. Interestingly, in D492 cells, preincubation with bestatin showed no effect on melflufen activity.
|
||||
| In Vitro Model | Normal | D492 cell | CVCL_D1HJ | ||
| Experiment 26 Reporting the Activity Data of This PDC | [11] | ||||
| Indication | Breast cancer | ||||
| Efficacy Data | Cell viability |
73%
|
|||
| Administration Time | 48 h | ||||
| Administration Dosage | 1 μM | ||||
| MOA of PDC |
Melphalan is a wellknown cancer drug used for decades for the treatment of various cancer types, and it is still widely used for hematological cancers today. It is an alkylating agent that works by adding an alkyl group to the guanine base of the DNA, resulting in an aberrant linkage between DNA strands, DNA breakage, and inhibition of DNA synthesis. Melphalan is a hydrophilic drug, and as such, it does not penetrate cell membranes easily, which is limiting to its anticancer potential. In contrast, melflufen (melphalan flufenamide), a new peptideconjugated alkylator, is highly lipophilic and therefore penetrates the cell membrane easily. Inside the cell, melflufen is rapidly hydrolyzed into less lipophilic metabolites that retain high alkylating potential, leading to their entrapment and accumulation. Aminopeptidases belong to a large family of enzymes that catalyze the cleavage of amino acids from the amino terminus of proteins or peptides and are shown to facilitate intracellular hydrolysis of melflufen. Aminopeptidases are involved in multiple cellular processes, and their expression and activity are frequently deregulated in cancer cells. For this reason, aminopeptidase inhibitors bestatin and tosedostat have been investigated in the clinical settings. Exploiting aminopeptidase activity to convert a lipophilic drug such as melflufen to an intracellular hydrophilic metabolite with high alkylating potential may offer an effective alternative therapeutic approach. Previously it has been shown that aminopeptidase N (ANPEP or CD13) can hydrolyze melflufen, but it is largely unknown whether melflufen can be a substrate for other aminopeptidases. Application of melflufen has mainly been focused on multiple myeloma, where it has shown promising results in phase 3 clinical trial in relapse and refractory patient population. 13 Yet it is unexplored whether melflufen can be effective in other cancer types such as breast cancer. Here, we demonstrate the efficacy of melflufen in D492HER2 breast epithelial cells overexpressing the HER2 oncogene and the triplenegative cell line MDAMB231.
Click to Show/Hide
|
||||
| Description |
While these cells tolerated higher drug concentrations for both drugs compared to our D492 cell lines, melflufen was significantly more efficient than doxorubicin in killing the MDAMB231 cells (Figure 3C).
|
||||
| In Vitro Model | Breast adenocarcinoma | MDA-MB-231 cell | CVCL_0062 | ||
| Experiment 27 Reporting the Activity Data of This PDC | [11] | ||||
| Indication | Breast cancer | ||||
| Efficacy Data | Cell viability |
74%
|
|||
| Administration Time | 48 h | ||||
| Administration Dosage | 0.5 μM | ||||
| MOA of PDC |
Melphalan is a wellknown cancer drug used for decades for the treatment of various cancer types, and it is still widely used for hematological cancers today. It is an alkylating agent that works by adding an alkyl group to the guanine base of the DNA, resulting in an aberrant linkage between DNA strands, DNA breakage, and inhibition of DNA synthesis. Melphalan is a hydrophilic drug, and as such, it does not penetrate cell membranes easily, which is limiting to its anticancer potential. In contrast, melflufen (melphalan flufenamide), a new peptideconjugated alkylator, is highly lipophilic and therefore penetrates the cell membrane easily. Inside the cell, melflufen is rapidly hydrolyzed into less lipophilic metabolites that retain high alkylating potential, leading to their entrapment and accumulation. Aminopeptidases belong to a large family of enzymes that catalyze the cleavage of amino acids from the amino terminus of proteins or peptides and are shown to facilitate intracellular hydrolysis of melflufen. Aminopeptidases are involved in multiple cellular processes, and their expression and activity are frequently deregulated in cancer cells. For this reason, aminopeptidase inhibitors bestatin and tosedostat have been investigated in the clinical settings. Exploiting aminopeptidase activity to convert a lipophilic drug such as melflufen to an intracellular hydrophilic metabolite with high alkylating potential may offer an effective alternative therapeutic approach. Previously it has been shown that aminopeptidase N (ANPEP or CD13) can hydrolyze melflufen, but it is largely unknown whether melflufen can be a substrate for other aminopeptidases. Application of melflufen has mainly been focused on multiple myeloma, where it has shown promising results in phase 3 clinical trial in relapse and refractory patient population. 13 Yet it is unexplored whether melflufen can be effective in other cancer types such as breast cancer. Here, we demonstrate the efficacy of melflufen in D492HER2 breast epithelial cells overexpressing the HER2 oncogene and the triplenegative cell line MDAMB231.
Click to Show/Hide
|
||||
| Description |
While these cells tolerated higher drug concentrations for both drugs compared to our D492 cell lines, melflufen was significantly more efficient than doxorubicin in killing the MDAMB231 cells (Figure 3C).
|
||||
| In Vitro Model | Breast adenocarcinoma | MDA-MB-231 cell | CVCL_0062 | ||
| Experiment 28 Reporting the Activity Data of This PDC | [11] | ||||
| Indication | Breast cancer | ||||
| Efficacy Data | Cell viability |
75%
|
|||
| Administration Time | 48 h | ||||
| Administration Dosage | 50 μM | ||||
| MOA of PDC |
Melphalan is a wellknown cancer drug used for decades for the treatment of various cancer types, and it is still widely used for hematological cancers today. It is an alkylating agent that works by adding an alkyl group to the guanine base of the DNA, resulting in an aberrant linkage between DNA strands, DNA breakage, and inhibition of DNA synthesis. Melphalan is a hydrophilic drug, and as such, it does not penetrate cell membranes easily, which is limiting to its anticancer potential. In contrast, melflufen (melphalan flufenamide), a new peptideconjugated alkylator, is highly lipophilic and therefore penetrates the cell membrane easily. Inside the cell, melflufen is rapidly hydrolyzed into less lipophilic metabolites that retain high alkylating potential, leading to their entrapment and accumulation. Aminopeptidases belong to a large family of enzymes that catalyze the cleavage of amino acids from the amino terminus of proteins or peptides and are shown to facilitate intracellular hydrolysis of melflufen. Aminopeptidases are involved in multiple cellular processes, and their expression and activity are frequently deregulated in cancer cells. For this reason, aminopeptidase inhibitors bestatin and tosedostat have been investigated in the clinical settings. Exploiting aminopeptidase activity to convert a lipophilic drug such as melflufen to an intracellular hydrophilic metabolite with high alkylating potential may offer an effective alternative therapeutic approach. Previously it has been shown that aminopeptidase N (ANPEP or CD13) can hydrolyze melflufen, but it is largely unknown whether melflufen can be a substrate for other aminopeptidases. Application of melflufen has mainly been focused on multiple myeloma, where it has shown promising results in phase 3 clinical trial in relapse and refractory patient population. 13 Yet it is unexplored whether melflufen can be effective in other cancer types such as breast cancer. Here, we demonstrate the efficacy of melflufen in D492HER2 breast epithelial cells overexpressing the HER2 oncogene and the triplenegative cell line MDAMB231.
Click to Show/Hide
|
||||
| Description |
D492HER2 cells showed increased sensitivity to melphalan compared to the progenitor cell line D492. However, concentration as high as 100 μmol/L was insufficient to kill the whole cell population. In both cell lines, around 40% of D492 cells and at least 20% of D492HER2 cells were still viable after incubation with 100 μmol/L melphalan. On the contrary, melflufen decreased viability of both D492 and D492HER2 cells at much lower doses.
Click to Show/Hide
|
||||
| In Vitro Model | Normal | D492 cell | CVCL_D1HJ | ||
| Experiment 29 Reporting the Activity Data of This PDC | [11] | ||||
| Indication | Breast cancer | ||||
| Efficacy Data | Cell viability |
75%
|
|||
| Administration Time | 48 h | ||||
| Administration Dosage | 0.5 μM | ||||
| MOA of PDC |
Melphalan is a wellknown cancer drug used for decades for the treatment of various cancer types, and it is still widely used for hematological cancers today. It is an alkylating agent that works by adding an alkyl group to the guanine base of the DNA, resulting in an aberrant linkage between DNA strands, DNA breakage, and inhibition of DNA synthesis. Melphalan is a hydrophilic drug, and as such, it does not penetrate cell membranes easily, which is limiting to its anticancer potential. In contrast, melflufen (melphalan flufenamide), a new peptideconjugated alkylator, is highly lipophilic and therefore penetrates the cell membrane easily. Inside the cell, melflufen is rapidly hydrolyzed into less lipophilic metabolites that retain high alkylating potential, leading to their entrapment and accumulation. Aminopeptidases belong to a large family of enzymes that catalyze the cleavage of amino acids from the amino terminus of proteins or peptides and are shown to facilitate intracellular hydrolysis of melflufen. Aminopeptidases are involved in multiple cellular processes, and their expression and activity are frequently deregulated in cancer cells. For this reason, aminopeptidase inhibitors bestatin and tosedostat have been investigated in the clinical settings. Exploiting aminopeptidase activity to convert a lipophilic drug such as melflufen to an intracellular hydrophilic metabolite with high alkylating potential may offer an effective alternative therapeutic approach. Previously it has been shown that aminopeptidase N (ANPEP or CD13) can hydrolyze melflufen, but it is largely unknown whether melflufen can be a substrate for other aminopeptidases. Application of melflufen has mainly been focused on multiple myeloma, where it has shown promising results in phase 3 clinical trial in relapse and refractory patient population. 13 Yet it is unexplored whether melflufen can be effective in other cancer types such as breast cancer. Here, we demonstrate the efficacy of melflufen in D492HER2 breast epithelial cells overexpressing the HER2 oncogene and the triplenegative cell line MDAMB231.
Click to Show/Hide
|
||||
| Description |
D492HER2 cells showed increased sensitivity to melphalan compared to the progenitor cell line D492. However, concentration as high as 100 μmol/L was insufficient to kill the whole cell population. In both cell lines, around 40% of D492 cells and at least 20% of D492HER2 cells were still viable after incubation with 100 μmol/L melphalan. On the contrary, melflufen decreased viability of both D492 and D492HER2 cells at much lower doses.
Click to Show/Hide
|
||||
| In Vitro Model | Normal | D492 cell | CVCL_D1HJ | ||
| Experiment 30 Reporting the Activity Data of This PDC | [11] | ||||
| Indication | Breast cancer | ||||
| Efficacy Data | Cell viability |
75%
|
|||
| Administration Time | 48 h | ||||
| Administration Dosage | 0.1 μM | ||||
| MOA of PDC |
Melphalan is a wellknown cancer drug used for decades for the treatment of various cancer types, and it is still widely used for hematological cancers today. It is an alkylating agent that works by adding an alkyl group to the guanine base of the DNA, resulting in an aberrant linkage between DNA strands, DNA breakage, and inhibition of DNA synthesis. Melphalan is a hydrophilic drug, and as such, it does not penetrate cell membranes easily, which is limiting to its anticancer potential. In contrast, melflufen (melphalan flufenamide), a new peptideconjugated alkylator, is highly lipophilic and therefore penetrates the cell membrane easily. Inside the cell, melflufen is rapidly hydrolyzed into less lipophilic metabolites that retain high alkylating potential, leading to their entrapment and accumulation. Aminopeptidases belong to a large family of enzymes that catalyze the cleavage of amino acids from the amino terminus of proteins or peptides and are shown to facilitate intracellular hydrolysis of melflufen. Aminopeptidases are involved in multiple cellular processes, and their expression and activity are frequently deregulated in cancer cells. For this reason, aminopeptidase inhibitors bestatin and tosedostat have been investigated in the clinical settings. Exploiting aminopeptidase activity to convert a lipophilic drug such as melflufen to an intracellular hydrophilic metabolite with high alkylating potential may offer an effective alternative therapeutic approach. Previously it has been shown that aminopeptidase N (ANPEP or CD13) can hydrolyze melflufen, but it is largely unknown whether melflufen can be a substrate for other aminopeptidases. Application of melflufen has mainly been focused on multiple myeloma, where it has shown promising results in phase 3 clinical trial in relapse and refractory patient population. 13 Yet it is unexplored whether melflufen can be effective in other cancer types such as breast cancer. Here, we demonstrate the efficacy of melflufen in D492HER2 breast epithelial cells overexpressing the HER2 oncogene and the triplenegative cell line MDAMB231.
Click to Show/Hide
|
||||
| Description |
While these cells tolerated higher drug concentrations for both drugs compared to our D492 cell lines, melflufen was significantly more efficient than doxorubicin in killing the MDAMB231 cells (Figure 3C).
|
||||
| In Vitro Model | Breast adenocarcinoma | MDA-MB-231 cell | CVCL_0062 | ||
| Experiment 31 Reporting the Activity Data of This PDC | [11] | ||||
| Indication | Breast cancer | ||||
| Efficacy Data | Cell viability |
80%
|
|||
| Administration Time | 48 h | ||||
| Administration Dosage | 0.1 μM | ||||
| MOA of PDC |
Melphalan is a wellknown cancer drug used for decades for the treatment of various cancer types, and it is still widely used for hematological cancers today. It is an alkylating agent that works by adding an alkyl group to the guanine base of the DNA, resulting in an aberrant linkage between DNA strands, DNA breakage, and inhibition of DNA synthesis. Melphalan is a hydrophilic drug, and as such, it does not penetrate cell membranes easily, which is limiting to its anticancer potential. In contrast, melflufen (melphalan flufenamide), a new peptideconjugated alkylator, is highly lipophilic and therefore penetrates the cell membrane easily. Inside the cell, melflufen is rapidly hydrolyzed into less lipophilic metabolites that retain high alkylating potential, leading to their entrapment and accumulation. Aminopeptidases belong to a large family of enzymes that catalyze the cleavage of amino acids from the amino terminus of proteins or peptides and are shown to facilitate intracellular hydrolysis of melflufen. Aminopeptidases are involved in multiple cellular processes, and their expression and activity are frequently deregulated in cancer cells. For this reason, aminopeptidase inhibitors bestatin and tosedostat have been investigated in the clinical settings. Exploiting aminopeptidase activity to convert a lipophilic drug such as melflufen to an intracellular hydrophilic metabolite with high alkylating potential may offer an effective alternative therapeutic approach. Previously it has been shown that aminopeptidase N (ANPEP or CD13) can hydrolyze melflufen, but it is largely unknown whether melflufen can be a substrate for other aminopeptidases. Application of melflufen has mainly been focused on multiple myeloma, where it has shown promising results in phase 3 clinical trial in relapse and refractory patient population. 13 Yet it is unexplored whether melflufen can be effective in other cancer types such as breast cancer. Here, we demonstrate the efficacy of melflufen in D492HER2 breast epithelial cells overexpressing the HER2 oncogene and the triplenegative cell line MDAMB231.
Click to Show/Hide
|
||||
| Description |
Aminopeptidases are thought to be responsible for the cleavage of melflufen, and indeed, in our model, the aminopeptidase inhibitor bestatin attenuated the activity of melflufen in D492HER2 cells. Interestingly, in D492 cells, preincubation with bestatin showed no effect on melflufen activity.
|
||||
| In Vitro Model | Normal | D492 cell | CVCL_D1HJ | ||
| Experiment 32 Reporting the Activity Data of This PDC | [11] | ||||
| Indication | Breast cancer | ||||
| Efficacy Data | Cell viability |
80%
|
|||
| Administration Time | 48 h | ||||
| Administration Dosage | 1.5 μM; with bestatin (10 μmol/L) | ||||
| MOA of PDC |
Melphalan is a wellknown cancer drug used for decades for the treatment of various cancer types, and it is still widely used for hematological cancers today. It is an alkylating agent that works by adding an alkyl group to the guanine base of the DNA, resulting in an aberrant linkage between DNA strands, DNA breakage, and inhibition of DNA synthesis. Melphalan is a hydrophilic drug, and as such, it does not penetrate cell membranes easily, which is limiting to its anticancer potential. In contrast, melflufen (melphalan flufenamide), a new peptideconjugated alkylator, is highly lipophilic and therefore penetrates the cell membrane easily. Inside the cell, melflufen is rapidly hydrolyzed into less lipophilic metabolites that retain high alkylating potential, leading to their entrapment and accumulation. Aminopeptidases belong to a large family of enzymes that catalyze the cleavage of amino acids from the amino terminus of proteins or peptides and are shown to facilitate intracellular hydrolysis of melflufen. Aminopeptidases are involved in multiple cellular processes, and their expression and activity are frequently deregulated in cancer cells. For this reason, aminopeptidase inhibitors bestatin and tosedostat have been investigated in the clinical settings. Exploiting aminopeptidase activity to convert a lipophilic drug such as melflufen to an intracellular hydrophilic metabolite with high alkylating potential may offer an effective alternative therapeutic approach. Previously it has been shown that aminopeptidase N (ANPEP or CD13) can hydrolyze melflufen, but it is largely unknown whether melflufen can be a substrate for other aminopeptidases. Application of melflufen has mainly been focused on multiple myeloma, where it has shown promising results in phase 3 clinical trial in relapse and refractory patient population. 13 Yet it is unexplored whether melflufen can be effective in other cancer types such as breast cancer. Here, we demonstrate the efficacy of melflufen in D492HER2 breast epithelial cells overexpressing the HER2 oncogene and the triplenegative cell line MDAMB231.
Click to Show/Hide
|
||||
| Description |
Aminopeptidases are thought to be responsible for the cleavage of melflufen, and indeed, in our model, the aminopeptidase inhibitor bestatin attenuated the activity of melflufen in D492HER2 cells. Interestingly, in D492 cells, preincubation with bestatin showed no effect on melflufen activity.
|
||||
| In Vitro Model | Normal | D492 cell | CVCL_D1HJ | ||
| Experiment 33 Reporting the Activity Data of This PDC | [11] | ||||
| Indication | Breast cancer | ||||
| Efficacy Data | Cell viability |
82%
|
|||
| Administration Time | 48 h | ||||
| Administration Dosage | 0.5 μM; with bestatin (10 μmol/L) | ||||
| MOA of PDC |
Melphalan is a wellknown cancer drug used for decades for the treatment of various cancer types, and it is still widely used for hematological cancers today. It is an alkylating agent that works by adding an alkyl group to the guanine base of the DNA, resulting in an aberrant linkage between DNA strands, DNA breakage, and inhibition of DNA synthesis. Melphalan is a hydrophilic drug, and as such, it does not penetrate cell membranes easily, which is limiting to its anticancer potential. In contrast, melflufen (melphalan flufenamide), a new peptideconjugated alkylator, is highly lipophilic and therefore penetrates the cell membrane easily. Inside the cell, melflufen is rapidly hydrolyzed into less lipophilic metabolites that retain high alkylating potential, leading to their entrapment and accumulation. Aminopeptidases belong to a large family of enzymes that catalyze the cleavage of amino acids from the amino terminus of proteins or peptides and are shown to facilitate intracellular hydrolysis of melflufen. Aminopeptidases are involved in multiple cellular processes, and their expression and activity are frequently deregulated in cancer cells. For this reason, aminopeptidase inhibitors bestatin and tosedostat have been investigated in the clinical settings. Exploiting aminopeptidase activity to convert a lipophilic drug such as melflufen to an intracellular hydrophilic metabolite with high alkylating potential may offer an effective alternative therapeutic approach. Previously it has been shown that aminopeptidase N (ANPEP or CD13) can hydrolyze melflufen, but it is largely unknown whether melflufen can be a substrate for other aminopeptidases. Application of melflufen has mainly been focused on multiple myeloma, where it has shown promising results in phase 3 clinical trial in relapse and refractory patient population. 13 Yet it is unexplored whether melflufen can be effective in other cancer types such as breast cancer. Here, we demonstrate the efficacy of melflufen in D492HER2 breast epithelial cells overexpressing the HER2 oncogene and the triplenegative cell line MDAMB231.
Click to Show/Hide
|
||||
| Description |
Aminopeptidases are thought to be responsible for the cleavage of melflufen, and indeed, in our model, the aminopeptidase inhibitor bestatin attenuated the activity of melflufen in D492HER2 cells. Interestingly, in D492 cells, preincubation with bestatin showed no effect on melflufen activity.
|
||||
| In Vitro Model | Normal | D492 cell | CVCL_D1HJ | ||
| Experiment 34 Reporting the Activity Data of This PDC | [11] | ||||
| Indication | Breast cancer | ||||
| Efficacy Data | Cell viability |
84%
|
|||
| Administration Time | 48 h | ||||
| Administration Dosage | 0.5 μM | ||||
| MOA of PDC |
Melphalan is a wellknown cancer drug used for decades for the treatment of various cancer types, and it is still widely used for hematological cancers today. It is an alkylating agent that works by adding an alkyl group to the guanine base of the DNA, resulting in an aberrant linkage between DNA strands, DNA breakage, and inhibition of DNA synthesis. Melphalan is a hydrophilic drug, and as such, it does not penetrate cell membranes easily, which is limiting to its anticancer potential. In contrast, melflufen (melphalan flufenamide), a new peptideconjugated alkylator, is highly lipophilic and therefore penetrates the cell membrane easily. Inside the cell, melflufen is rapidly hydrolyzed into less lipophilic metabolites that retain high alkylating potential, leading to their entrapment and accumulation. Aminopeptidases belong to a large family of enzymes that catalyze the cleavage of amino acids from the amino terminus of proteins or peptides and are shown to facilitate intracellular hydrolysis of melflufen. Aminopeptidases are involved in multiple cellular processes, and their expression and activity are frequently deregulated in cancer cells. For this reason, aminopeptidase inhibitors bestatin and tosedostat have been investigated in the clinical settings. Exploiting aminopeptidase activity to convert a lipophilic drug such as melflufen to an intracellular hydrophilic metabolite with high alkylating potential may offer an effective alternative therapeutic approach. Previously it has been shown that aminopeptidase N (ANPEP or CD13) can hydrolyze melflufen, but it is largely unknown whether melflufen can be a substrate for other aminopeptidases. Application of melflufen has mainly been focused on multiple myeloma, where it has shown promising results in phase 3 clinical trial in relapse and refractory patient population. 13 Yet it is unexplored whether melflufen can be effective in other cancer types such as breast cancer. Here, we demonstrate the efficacy of melflufen in D492HER2 breast epithelial cells overexpressing the HER2 oncogene and the triplenegative cell line MDAMB231.
Click to Show/Hide
|
||||
| Description |
Aminopeptidases are thought to be responsible for the cleavage of melflufen, and indeed, in our model, the aminopeptidase inhibitor bestatin attenuated the activity of melflufen in D492HER2 cells. Interestingly, in D492 cells, preincubation with bestatin showed no effect on melflufen activity.
|
||||
| In Vitro Model | Normal | D492 cell | CVCL_D1HJ | ||
| Experiment 35 Reporting the Activity Data of This PDC | [11] | ||||
| Indication | Breast cancer | ||||
| Efficacy Data | Cell viability |
86%
|
|||
| Administration Time | 48 h | ||||
| Administration Dosage | 0.1 μM; with bestatin (10 μmol/L) | ||||
| MOA of PDC |
Melphalan is a wellknown cancer drug used for decades for the treatment of various cancer types, and it is still widely used for hematological cancers today. It is an alkylating agent that works by adding an alkyl group to the guanine base of the DNA, resulting in an aberrant linkage between DNA strands, DNA breakage, and inhibition of DNA synthesis. Melphalan is a hydrophilic drug, and as such, it does not penetrate cell membranes easily, which is limiting to its anticancer potential. In contrast, melflufen (melphalan flufenamide), a new peptideconjugated alkylator, is highly lipophilic and therefore penetrates the cell membrane easily. Inside the cell, melflufen is rapidly hydrolyzed into less lipophilic metabolites that retain high alkylating potential, leading to their entrapment and accumulation. Aminopeptidases belong to a large family of enzymes that catalyze the cleavage of amino acids from the amino terminus of proteins or peptides and are shown to facilitate intracellular hydrolysis of melflufen. Aminopeptidases are involved in multiple cellular processes, and their expression and activity are frequently deregulated in cancer cells. For this reason, aminopeptidase inhibitors bestatin and tosedostat have been investigated in the clinical settings. Exploiting aminopeptidase activity to convert a lipophilic drug such as melflufen to an intracellular hydrophilic metabolite with high alkylating potential may offer an effective alternative therapeutic approach. Previously it has been shown that aminopeptidase N (ANPEP or CD13) can hydrolyze melflufen, but it is largely unknown whether melflufen can be a substrate for other aminopeptidases. Application of melflufen has mainly been focused on multiple myeloma, where it has shown promising results in phase 3 clinical trial in relapse and refractory patient population. 13 Yet it is unexplored whether melflufen can be effective in other cancer types such as breast cancer. Here, we demonstrate the efficacy of melflufen in D492HER2 breast epithelial cells overexpressing the HER2 oncogene and the triplenegative cell line MDAMB231.
Click to Show/Hide
|
||||
| Description |
Aminopeptidases are thought to be responsible for the cleavage of melflufen, and indeed, in our model, the aminopeptidase inhibitor bestatin attenuated the activity of melflufen in D492HER2 cells. Interestingly, in D492 cells, preincubation with bestatin showed no effect on melflufen activity.
|
||||
| In Vitro Model | Normal | D492 cell | CVCL_D1HJ | ||
| Experiment 36 Reporting the Activity Data of This PDC | [11] | ||||
| Indication | Breast cancer | ||||
| Efficacy Data | Cell viability |
90%
|
|||
| Administration Time | 48 h | ||||
| Administration Dosage | 1.0 μM; with bestatin (10 μmol/L) | ||||
| MOA of PDC |
Melphalan is a wellknown cancer drug used for decades for the treatment of various cancer types, and it is still widely used for hematological cancers today. It is an alkylating agent that works by adding an alkyl group to the guanine base of the DNA, resulting in an aberrant linkage between DNA strands, DNA breakage, and inhibition of DNA synthesis. Melphalan is a hydrophilic drug, and as such, it does not penetrate cell membranes easily, which is limiting to its anticancer potential. In contrast, melflufen (melphalan flufenamide), a new peptideconjugated alkylator, is highly lipophilic and therefore penetrates the cell membrane easily. Inside the cell, melflufen is rapidly hydrolyzed into less lipophilic metabolites that retain high alkylating potential, leading to their entrapment and accumulation. Aminopeptidases belong to a large family of enzymes that catalyze the cleavage of amino acids from the amino terminus of proteins or peptides and are shown to facilitate intracellular hydrolysis of melflufen. Aminopeptidases are involved in multiple cellular processes, and their expression and activity are frequently deregulated in cancer cells. For this reason, aminopeptidase inhibitors bestatin and tosedostat have been investigated in the clinical settings. Exploiting aminopeptidase activity to convert a lipophilic drug such as melflufen to an intracellular hydrophilic metabolite with high alkylating potential may offer an effective alternative therapeutic approach. Previously it has been shown that aminopeptidase N (ANPEP or CD13) can hydrolyze melflufen, but it is largely unknown whether melflufen can be a substrate for other aminopeptidases. Application of melflufen has mainly been focused on multiple myeloma, where it has shown promising results in phase 3 clinical trial in relapse and refractory patient population. 13 Yet it is unexplored whether melflufen can be effective in other cancer types such as breast cancer. Here, we demonstrate the efficacy of melflufen in D492HER2 breast epithelial cells overexpressing the HER2 oncogene and the triplenegative cell line MDAMB231.
Click to Show/Hide
|
||||
| Description |
Aminopeptidases are thought to be responsible for the cleavage of melflufen, and indeed, in our model, the aminopeptidase inhibitor bestatin attenuated the activity of melflufen in D492HER2 cells. Interestingly, in D492 cells, preincubation with bestatin showed no effect on melflufen activity.
|
||||
| In Vitro Model | Normal | D492 cell | CVCL_D1HJ | ||
| Experiment 37 Reporting the Activity Data of This PDC | [11] | ||||
| Indication | Breast cancer | ||||
| Efficacy Data | Cell viability |
95%
|
|||
| Administration Time | 48 h | ||||
| Administration Dosage | 0.7 μM | ||||
| MOA of PDC |
Melphalan is a wellknown cancer drug used for decades for the treatment of various cancer types, and it is still widely used for hematological cancers today. It is an alkylating agent that works by adding an alkyl group to the guanine base of the DNA, resulting in an aberrant linkage between DNA strands, DNA breakage, and inhibition of DNA synthesis. Melphalan is a hydrophilic drug, and as such, it does not penetrate cell membranes easily, which is limiting to its anticancer potential. In contrast, melflufen (melphalan flufenamide), a new peptideconjugated alkylator, is highly lipophilic and therefore penetrates the cell membrane easily. Inside the cell, melflufen is rapidly hydrolyzed into less lipophilic metabolites that retain high alkylating potential, leading to their entrapment and accumulation. Aminopeptidases belong to a large family of enzymes that catalyze the cleavage of amino acids from the amino terminus of proteins or peptides and are shown to facilitate intracellular hydrolysis of melflufen. Aminopeptidases are involved in multiple cellular processes, and their expression and activity are frequently deregulated in cancer cells. For this reason, aminopeptidase inhibitors bestatin and tosedostat have been investigated in the clinical settings. Exploiting aminopeptidase activity to convert a lipophilic drug such as melflufen to an intracellular hydrophilic metabolite with high alkylating potential may offer an effective alternative therapeutic approach. Previously it has been shown that aminopeptidase N (ANPEP or CD13) can hydrolyze melflufen, but it is largely unknown whether melflufen can be a substrate for other aminopeptidases. Application of melflufen has mainly been focused on multiple myeloma, where it has shown promising results in phase 3 clinical trial in relapse and refractory patient population. 13 Yet it is unexplored whether melflufen can be effective in other cancer types such as breast cancer. Here, we demonstrate the efficacy of melflufen in D492HER2 breast epithelial cells overexpressing the HER2 oncogene and the triplenegative cell line MDAMB231.
Click to Show/Hide
|
||||
| Description |
Aminopeptidases are thought to be responsible for the cleavage of melflufen, and indeed, in our model, the aminopeptidase inhibitor bestatin attenuated the activity of melflufen in D492HER2 cells. Interestingly, in D492 cells, preincubation with bestatin showed no effect on melflufen activity.
|
||||
| In Vitro Model | Normal | D492 cell | CVCL_D1HJ | ||
| Experiment 38 Reporting the Activity Data of This PDC | [11] | ||||
| Indication | Breast cancer | ||||
| Efficacy Data | Cell viability |
97%
|
|||
| Administration Time | 48 h | ||||
| Administration Dosage | 0.7 μM; with bestatin (10 μmol/L) | ||||
| MOA of PDC |
Melphalan is a wellknown cancer drug used for decades for the treatment of various cancer types, and it is still widely used for hematological cancers today. It is an alkylating agent that works by adding an alkyl group to the guanine base of the DNA, resulting in an aberrant linkage between DNA strands, DNA breakage, and inhibition of DNA synthesis. Melphalan is a hydrophilic drug, and as such, it does not penetrate cell membranes easily, which is limiting to its anticancer potential. In contrast, melflufen (melphalan flufenamide), a new peptideconjugated alkylator, is highly lipophilic and therefore penetrates the cell membrane easily. Inside the cell, melflufen is rapidly hydrolyzed into less lipophilic metabolites that retain high alkylating potential, leading to their entrapment and accumulation. Aminopeptidases belong to a large family of enzymes that catalyze the cleavage of amino acids from the amino terminus of proteins or peptides and are shown to facilitate intracellular hydrolysis of melflufen. Aminopeptidases are involved in multiple cellular processes, and their expression and activity are frequently deregulated in cancer cells. For this reason, aminopeptidase inhibitors bestatin and tosedostat have been investigated in the clinical settings. Exploiting aminopeptidase activity to convert a lipophilic drug such as melflufen to an intracellular hydrophilic metabolite with high alkylating potential may offer an effective alternative therapeutic approach. Previously it has been shown that aminopeptidase N (ANPEP or CD13) can hydrolyze melflufen, but it is largely unknown whether melflufen can be a substrate for other aminopeptidases. Application of melflufen has mainly been focused on multiple myeloma, where it has shown promising results in phase 3 clinical trial in relapse and refractory patient population. 13 Yet it is unexplored whether melflufen can be effective in other cancer types such as breast cancer. Here, we demonstrate the efficacy of melflufen in D492HER2 breast epithelial cells overexpressing the HER2 oncogene and the triplenegative cell line MDAMB231.
Click to Show/Hide
|
||||
| Description |
Aminopeptidases are thought to be responsible for the cleavage of melflufen, and indeed, in our model, the aminopeptidase inhibitor bestatin attenuated the activity of melflufen in D492HER2 cells. Interestingly, in D492 cells, preincubation with bestatin showed no effect on melflufen activity.
|
||||
| In Vitro Model | Normal | D492 cell | CVCL_D1HJ | ||
| Experiment 39 Reporting the Activity Data of This PDC | [11] | ||||
| Indication | Breast cancer | ||||
| Efficacy Data | Cell viability |
98%
|
|||
| Administration Time | 48 h | ||||
| Administration Dosage | 0.1 μM | ||||
| MOA of PDC |
Melphalan is a wellknown cancer drug used for decades for the treatment of various cancer types, and it is still widely used for hematological cancers today. It is an alkylating agent that works by adding an alkyl group to the guanine base of the DNA, resulting in an aberrant linkage between DNA strands, DNA breakage, and inhibition of DNA synthesis. Melphalan is a hydrophilic drug, and as such, it does not penetrate cell membranes easily, which is limiting to its anticancer potential. In contrast, melflufen (melphalan flufenamide), a new peptideconjugated alkylator, is highly lipophilic and therefore penetrates the cell membrane easily. Inside the cell, melflufen is rapidly hydrolyzed into less lipophilic metabolites that retain high alkylating potential, leading to their entrapment and accumulation. Aminopeptidases belong to a large family of enzymes that catalyze the cleavage of amino acids from the amino terminus of proteins or peptides and are shown to facilitate intracellular hydrolysis of melflufen. Aminopeptidases are involved in multiple cellular processes, and their expression and activity are frequently deregulated in cancer cells. For this reason, aminopeptidase inhibitors bestatin and tosedostat have been investigated in the clinical settings. Exploiting aminopeptidase activity to convert a lipophilic drug such as melflufen to an intracellular hydrophilic metabolite with high alkylating potential may offer an effective alternative therapeutic approach. Previously it has been shown that aminopeptidase N (ANPEP or CD13) can hydrolyze melflufen, but it is largely unknown whether melflufen can be a substrate for other aminopeptidases. Application of melflufen has mainly been focused on multiple myeloma, where it has shown promising results in phase 3 clinical trial in relapse and refractory patient population. 13 Yet it is unexplored whether melflufen can be effective in other cancer types such as breast cancer. Here, we demonstrate the efficacy of melflufen in D492HER2 breast epithelial cells overexpressing the HER2 oncogene and the triplenegative cell line MDAMB231.
Click to Show/Hide
|
||||
| Description |
Aminopeptidases are thought to be responsible for the cleavage of melflufen, and indeed, in our model, the aminopeptidase inhibitor bestatin attenuated the activity of melflufen in D492HER2 cells. Interestingly, in D492 cells, preincubation with bestatin showed no effect on melflufen activity.
|
||||
| In Vitro Model | Normal | D492 cell | CVCL_D1HJ | ||
| Experiment 40 Reporting the Activity Data of This PDC | [11] | ||||
| Indication | Breast cancer | ||||
| Efficacy Data | Cell viability |
99%
|
|||
| Administration Time | 48 h | ||||
| Administration Dosage | 0.1 μM; with bestatin (10 μmol/L) | ||||
| MOA of PDC |
Melphalan is a wellknown cancer drug used for decades for the treatment of various cancer types, and it is still widely used for hematological cancers today. It is an alkylating agent that works by adding an alkyl group to the guanine base of the DNA, resulting in an aberrant linkage between DNA strands, DNA breakage, and inhibition of DNA synthesis. Melphalan is a hydrophilic drug, and as such, it does not penetrate cell membranes easily, which is limiting to its anticancer potential. In contrast, melflufen (melphalan flufenamide), a new peptideconjugated alkylator, is highly lipophilic and therefore penetrates the cell membrane easily. Inside the cell, melflufen is rapidly hydrolyzed into less lipophilic metabolites that retain high alkylating potential, leading to their entrapment and accumulation. Aminopeptidases belong to a large family of enzymes that catalyze the cleavage of amino acids from the amino terminus of proteins or peptides and are shown to facilitate intracellular hydrolysis of melflufen. Aminopeptidases are involved in multiple cellular processes, and their expression and activity are frequently deregulated in cancer cells. For this reason, aminopeptidase inhibitors bestatin and tosedostat have been investigated in the clinical settings. Exploiting aminopeptidase activity to convert a lipophilic drug such as melflufen to an intracellular hydrophilic metabolite with high alkylating potential may offer an effective alternative therapeutic approach. Previously it has been shown that aminopeptidase N (ANPEP or CD13) can hydrolyze melflufen, but it is largely unknown whether melflufen can be a substrate for other aminopeptidases. Application of melflufen has mainly been focused on multiple myeloma, where it has shown promising results in phase 3 clinical trial in relapse and refractory patient population. 13 Yet it is unexplored whether melflufen can be effective in other cancer types such as breast cancer. Here, we demonstrate the efficacy of melflufen in D492HER2 breast epithelial cells overexpressing the HER2 oncogene and the triplenegative cell line MDAMB231.
Click to Show/Hide
|
||||
| Description |
Aminopeptidases are thought to be responsible for the cleavage of melflufen, and indeed, in our model, the aminopeptidase inhibitor bestatin attenuated the activity of melflufen in D492HER2 cells. Interestingly, in D492 cells, preincubation with bestatin showed no effect on melflufen activity.
|
||||
| In Vitro Model | Normal | D492 cell | CVCL_D1HJ | ||
| Experiment 41 Reporting the Activity Data of This PDC | [11] | ||||
| Indication | Breast cancer | ||||
| Efficacy Data | Cell viability |
100%
|
|||
| Administration Time | 48 h | ||||
| Administration Dosage | 0.5 μM | ||||
| MOA of PDC |
Melphalan is a wellknown cancer drug used for decades for the treatment of various cancer types, and it is still widely used for hematological cancers today. It is an alkylating agent that works by adding an alkyl group to the guanine base of the DNA, resulting in an aberrant linkage between DNA strands, DNA breakage, and inhibition of DNA synthesis. Melphalan is a hydrophilic drug, and as such, it does not penetrate cell membranes easily, which is limiting to its anticancer potential. In contrast, melflufen (melphalan flufenamide), a new peptideconjugated alkylator, is highly lipophilic and therefore penetrates the cell membrane easily. Inside the cell, melflufen is rapidly hydrolyzed into less lipophilic metabolites that retain high alkylating potential, leading to their entrapment and accumulation. Aminopeptidases belong to a large family of enzymes that catalyze the cleavage of amino acids from the amino terminus of proteins or peptides and are shown to facilitate intracellular hydrolysis of melflufen. Aminopeptidases are involved in multiple cellular processes, and their expression and activity are frequently deregulated in cancer cells. For this reason, aminopeptidase inhibitors bestatin and tosedostat have been investigated in the clinical settings. Exploiting aminopeptidase activity to convert a lipophilic drug such as melflufen to an intracellular hydrophilic metabolite with high alkylating potential may offer an effective alternative therapeutic approach. Previously it has been shown that aminopeptidase N (ANPEP or CD13) can hydrolyze melflufen, but it is largely unknown whether melflufen can be a substrate for other aminopeptidases. Application of melflufen has mainly been focused on multiple myeloma, where it has shown promising results in phase 3 clinical trial in relapse and refractory patient population. 13 Yet it is unexplored whether melflufen can be effective in other cancer types such as breast cancer. Here, we demonstrate the efficacy of melflufen in D492HER2 breast epithelial cells overexpressing the HER2 oncogene and the triplenegative cell line MDAMB231.
Click to Show/Hide
|
||||
| Description |
D492HER2 cells showed increased sensitivity to melphalan compared to the progenitor cell line D492. However, concentration as high as 100 μmol/L was insufficient to kill the whole cell population. In both cell lines, around 40% of D492 cells and at least 20% of D492HER2 cells were still viable after incubation with 100 μmol/L melphalan. On the contrary, melflufen decreased viability of both D492 and D492HER2 cells at much lower doses.
Click to Show/Hide
|
||||
| In Vitro Model | Normal | D492 cell | CVCL_D1HJ | ||
| Experiment 42 Reporting the Activity Data of This PDC | [11] | ||||
| Indication | Breast cancer | ||||
| Efficacy Data | Cell viability |
100%
|
|||
| Administration Time | 48 h | ||||
| Administration Dosage | 10 μM | ||||
| MOA of PDC |
Melphalan is a wellknown cancer drug used for decades for the treatment of various cancer types, and it is still widely used for hematological cancers today. It is an alkylating agent that works by adding an alkyl group to the guanine base of the DNA, resulting in an aberrant linkage between DNA strands, DNA breakage, and inhibition of DNA synthesis. Melphalan is a hydrophilic drug, and as such, it does not penetrate cell membranes easily, which is limiting to its anticancer potential. In contrast, melflufen (melphalan flufenamide), a new peptideconjugated alkylator, is highly lipophilic and therefore penetrates the cell membrane easily. Inside the cell, melflufen is rapidly hydrolyzed into less lipophilic metabolites that retain high alkylating potential, leading to their entrapment and accumulation. Aminopeptidases belong to a large family of enzymes that catalyze the cleavage of amino acids from the amino terminus of proteins or peptides and are shown to facilitate intracellular hydrolysis of melflufen. Aminopeptidases are involved in multiple cellular processes, and their expression and activity are frequently deregulated in cancer cells. For this reason, aminopeptidase inhibitors bestatin and tosedostat have been investigated in the clinical settings. Exploiting aminopeptidase activity to convert a lipophilic drug such as melflufen to an intracellular hydrophilic metabolite with high alkylating potential may offer an effective alternative therapeutic approach. Previously it has been shown that aminopeptidase N (ANPEP or CD13) can hydrolyze melflufen, but it is largely unknown whether melflufen can be a substrate for other aminopeptidases. Application of melflufen has mainly been focused on multiple myeloma, where it has shown promising results in phase 3 clinical trial in relapse and refractory patient population. 13 Yet it is unexplored whether melflufen can be effective in other cancer types such as breast cancer. Here, we demonstrate the efficacy of melflufen in D492HER2 breast epithelial cells overexpressing the HER2 oncogene and the triplenegative cell line MDAMB231.
Click to Show/Hide
|
||||
| Description |
D492HER2 cells showed increased sensitivity to melphalan compared to the progenitor cell line D492. However, concentration as high as 100 μmol/L was insufficient to kill the whole cell population. In both cell lines, around 40% of D492 cells and at least 20% of D492HER2 cells were still viable after incubation with 100 μmol/L melphalan. On the contrary, melflufen decreased viability of both D492 and D492HER2 cells at much lower doses.
Click to Show/Hide
|
||||
| In Vitro Model | Normal | D492 cell | CVCL_D1HJ | ||
| Experiment 43 Reporting the Activity Data of This PDC | [11] | ||||
| Indication | Breast cancer | ||||
| Efficacy Data | Cell viability |
101%
|
|||
| Administration Time | 48 h | ||||
| Administration Dosage | 0.1 μM | ||||
| MOA of PDC |
Melphalan is a wellknown cancer drug used for decades for the treatment of various cancer types, and it is still widely used for hematological cancers today. It is an alkylating agent that works by adding an alkyl group to the guanine base of the DNA, resulting in an aberrant linkage between DNA strands, DNA breakage, and inhibition of DNA synthesis. Melphalan is a hydrophilic drug, and as such, it does not penetrate cell membranes easily, which is limiting to its anticancer potential. In contrast, melflufen (melphalan flufenamide), a new peptideconjugated alkylator, is highly lipophilic and therefore penetrates the cell membrane easily. Inside the cell, melflufen is rapidly hydrolyzed into less lipophilic metabolites that retain high alkylating potential, leading to their entrapment and accumulation. Aminopeptidases belong to a large family of enzymes that catalyze the cleavage of amino acids from the amino terminus of proteins or peptides and are shown to facilitate intracellular hydrolysis of melflufen. Aminopeptidases are involved in multiple cellular processes, and their expression and activity are frequently deregulated in cancer cells. For this reason, aminopeptidase inhibitors bestatin and tosedostat have been investigated in the clinical settings. Exploiting aminopeptidase activity to convert a lipophilic drug such as melflufen to an intracellular hydrophilic metabolite with high alkylating potential may offer an effective alternative therapeutic approach. Previously it has been shown that aminopeptidase N (ANPEP or CD13) can hydrolyze melflufen, but it is largely unknown whether melflufen can be a substrate for other aminopeptidases. Application of melflufen has mainly been focused on multiple myeloma, where it has shown promising results in phase 3 clinical trial in relapse and refractory patient population. 13 Yet it is unexplored whether melflufen can be effective in other cancer types such as breast cancer. Here, we demonstrate the efficacy of melflufen in D492HER2 breast epithelial cells overexpressing the HER2 oncogene and the triplenegative cell line MDAMB231.
Click to Show/Hide
|
||||
| Description |
D492HER2 cells showed increased sensitivity to melphalan compared to the progenitor cell line D492. However, concentration as high as 100 μmol/L was insufficient to kill the whole cell population. In both cell lines, around 40% of D492 cells and at least 20% of D492HER2 cells were still viable after incubation with 100 μmol/L melphalan. On the contrary, melflufen decreased viability of both D492 and D492HER2 cells at much lower doses.
Click to Show/Hide
|
||||
| In Vitro Model | Normal | D492 cell | CVCL_D1HJ | ||
| Experiment 44 Reporting the Activity Data of This PDC | [11] | ||||
| Indication | Breast cancer | ||||
| Efficacy Data | Cell viability |
120%
|
|||
| Administration Time | 48 h | ||||
| Administration Dosage | 0.5 μM; with bestatin (10 μmol/L) | ||||
| MOA of PDC |
Melphalan is a wellknown cancer drug used for decades for the treatment of various cancer types, and it is still widely used for hematological cancers today. It is an alkylating agent that works by adding an alkyl group to the guanine base of the DNA, resulting in an aberrant linkage between DNA strands, DNA breakage, and inhibition of DNA synthesis. Melphalan is a hydrophilic drug, and as such, it does not penetrate cell membranes easily, which is limiting to its anticancer potential. In contrast, melflufen (melphalan flufenamide), a new peptideconjugated alkylator, is highly lipophilic and therefore penetrates the cell membrane easily. Inside the cell, melflufen is rapidly hydrolyzed into less lipophilic metabolites that retain high alkylating potential, leading to their entrapment and accumulation. Aminopeptidases belong to a large family of enzymes that catalyze the cleavage of amino acids from the amino terminus of proteins or peptides and are shown to facilitate intracellular hydrolysis of melflufen. Aminopeptidases are involved in multiple cellular processes, and their expression and activity are frequently deregulated in cancer cells. For this reason, aminopeptidase inhibitors bestatin and tosedostat have been investigated in the clinical settings. Exploiting aminopeptidase activity to convert a lipophilic drug such as melflufen to an intracellular hydrophilic metabolite with high alkylating potential may offer an effective alternative therapeutic approach. Previously it has been shown that aminopeptidase N (ANPEP or CD13) can hydrolyze melflufen, but it is largely unknown whether melflufen can be a substrate for other aminopeptidases. Application of melflufen has mainly been focused on multiple myeloma, where it has shown promising results in phase 3 clinical trial in relapse and refractory patient population. 13 Yet it is unexplored whether melflufen can be effective in other cancer types such as breast cancer. Here, we demonstrate the efficacy of melflufen in D492HER2 breast epithelial cells overexpressing the HER2 oncogene and the triplenegative cell line MDAMB231.
Click to Show/Hide
|
||||
| Description |
Aminopeptidases are thought to be responsible for the cleavage of melflufen, and indeed, in our model, the aminopeptidase inhibitor bestatin attenuated the activity of melflufen in D492HER2 cells. Interestingly, in D492 cells, preincubation with bestatin showed no effect on melflufen activity.
|
||||
| In Vitro Model | Normal | D492 cell | CVCL_D1HJ | ||
| Experiment 45 Reporting the Activity Data of This PDC | [8] | ||||
| Indication | lymphoma | ||||
| Efficacy Data | Half Maximal Inhibitory Concentration (IC50) |
0.011 μM
|
|||
| Description |
Cell cycle distribution analyses were performed on melflufen treated (0.1, 0.2 and 0.4 uM) and control cells from the KM-H2 and SU-DHL-10 cell lines in which the cytotoxic activity of melflufen during the 72 h FMCA assay was calculated as 0.92, 0.22, and 0.71 uM respectively (see Table3). To minimize potential artifacts emanating from cells exiting the analyzed cell populations, e.g. due to early and/or extensive cell death, the cells were subjected to basal cell culture conditions for 40 h (preincubation) followed by 12, 24 and 48 h treatments with melflufen. Propidium iodide (PI) staining of DNA using Vindelovs technique was followed by quantitation with flow cytometry analysis. The percentage of cells in each cell cycle phase was determined with the ModFit LT software.
Click to Show/Hide
|
||||
| In Vitro Model | Diffuse large B-cell lymphoma | Diffuse large B-cell lymphoma cell Ly-3 | Homo sapiens | ||
| Experiment 46 Reporting the Activity Data of This PDC | [11] | ||||
| Indication | Breast cancer | ||||
| Efficacy Data | Half maximal inhibitory concentration (IC50) |
0.046 μmol/L
|
|||
| MOA of PDC |
Melphalan is a wellknown cancer drug used for decades for the treatment of various cancer types, and it is still widely used for hematological cancers today. It is an alkylating agent that works by adding an alkyl group to the guanine base of the DNA, resulting in an aberrant linkage between DNA strands, DNA breakage, and inhibition of DNA synthesis. Melphalan is a hydrophilic drug, and as such, it does not penetrate cell membranes easily, which is limiting to its anticancer potential. In contrast, melflufen (melphalan flufenamide), a new peptideconjugated alkylator, is highly lipophilic and therefore penetrates the cell membrane easily. Inside the cell, melflufen is rapidly hydrolyzed into less lipophilic metabolites that retain high alkylating potential, leading to their entrapment and accumulation. Aminopeptidases belong to a large family of enzymes that catalyze the cleavage of amino acids from the amino terminus of proteins or peptides and are shown to facilitate intracellular hydrolysis of melflufen. Aminopeptidases are involved in multiple cellular processes, and their expression and activity are frequently deregulated in cancer cells. For this reason, aminopeptidase inhibitors bestatin and tosedostat have been investigated in the clinical settings. Exploiting aminopeptidase activity to convert a lipophilic drug such as melflufen to an intracellular hydrophilic metabolite with high alkylating potential may offer an effective alternative therapeutic approach. Previously it has been shown that aminopeptidase N (ANPEP or CD13) can hydrolyze melflufen, but it is largely unknown whether melflufen can be a substrate for other aminopeptidases. Application of melflufen has mainly been focused on multiple myeloma, where it has shown promising results in phase 3 clinical trial in relapse and refractory patient population. 13 Yet it is unexplored whether melflufen can be effective in other cancer types such as breast cancer. Here, we demonstrate the efficacy of melflufen in D492HER2 breast epithelial cells overexpressing the HER2 oncogene and the triplenegative cell line MDAMB231.
Click to Show/Hide
|
||||
| Description |
IC50 values for melflufen of 0.046 μmol/L in D492HER2 cells and 0.52 μmol/L in D492 cells compared to doxorubicin values of 0.92 μmol/L for D492HER2 cells and 1.8 μmol/L for D492 underpin these findings (Figure 3B).
|
||||
| In Vitro Model | Normal | D492 cell | CVCL_D1HJ | ||
| Experiment 47 Reporting the Activity Data of This PDC | [1] | ||||
| Indication | Multiple myeloma | ||||
| Efficacy Data | Half maximal inhibitory concentration (IC50) |
0.05 μM
|
|||
| MOA of PDC |
Melflufen is highly lipophilic, which promotes its rapid uptake by cells. Once within the cell, melflufen releases its hydrophilic alkylator payloads via the hydrolytic activity of intracellular peptidases (e.g., aminopeptidases). Aminopeptidases are Zn2+-dependent metalloproteinases that remove amino acids at the N-terminal position from oligopeptides and have been associated with multiple tumorigenic processes such as proliferation, apoptosis, differentiation, angiogenesis, and motility. The dependence of melflufen on aminopeptidases was initially demonstrated by the reduced cytotoxic activity of melflufen-but not the alkylator melphalan-when cells were pretreated with bestatin, an antibiotic that is a potent aminopeptidase inhibitor. In addition, structure analogs designed to resist peptide hydrolysis (N-methyl derivative and derivative with D-amino acid) were shown to be almost 100-fold less potent than melflufen. Subsequent in vitro studies demonstrated that hydrolytic cleavage of melflufen by aminopeptidases releases alkylator payloads, including melphalan. In vitro, the activity of melflufen is multi-pronged, including induction of DNA damage, induction of apoptosis, inhibition of VEGF-dependent cell migration, and inhibition of tumor-associated angiogenesis, which have been further reviewed elsewhere. Downregulation of aminopeptidases resulted in reduced melflufen-mediated cytotoxic activity and apoptotic signaling in cultured cells.
Click to Show/Hide
|
||||
| Description |
Compared with the known alkylator melphalan, melflufen had a higher cytotoxic activity in this broad range of malignant human cells, with a mean IC50 value that was 35-fold lower with melflufen than melphalan.
|
||||
| In Vitro Model | Lung large cell carcinoma | U-1810 cell | CVCL_D054 | ||
| Experiment 48 Reporting the Activity Data of This PDC | [8] | ||||
| Indication | lymphoma | ||||
| Efficacy Data | Half Maximal Inhibitory Concentration (IC50) |
0.077 μM
|
|||
| Description |
Cell cycle distribution analyses were performed on melflufen treated (0.1, 0.2 and 0.4 uM) and control cells from the KM-H2 and SU-DHL-10 cell lines in which the cytotoxic activity of melflufen during the 72 h FMCA assay was calculated as 0.92, 0.22, and 0.71 uM respectively (see Table3). To minimize potential artifacts emanating from cells exiting the analyzed cell populations, e.g. due to early and/or extensive cell death, the cells were subjected to basal cell culture conditions for 40 h (preincubation) followed by 12, 24 and 48 h treatments with melflufen. Propidium iodide (PI) staining of DNA using Vindelovs technique was followed by quantitation with flow cytometry analysis. The percentage of cells in each cell cycle phase was determined with the ModFit LT software.
Click to Show/Hide
|
||||
| In Vitro Model | Diffuse large B-cell lymphoma | WSU-NHL cell | CVCL_1793 | ||
| Experiment 49 Reporting the Activity Data of This PDC | [8] | ||||
| Indication | lymphoma | ||||
| Efficacy Data | Half Maximal Inhibitory Concentration (IC50) |
0.088 μM
|
|||
| Description |
Cell cycle distribution analyses were performed on melflufen treated (0.1, 0.2 and 0.4 uM) and control cells from the KM-H2 and SU-DHL-10 cell lines in which the cytotoxic activity of melflufen during the 72 h FMCA assay was calculated as 0.92, 0.22, and 0.71 uM respectively (see Table3). To minimize potential artifacts emanating from cells exiting the analyzed cell populations, e.g. due to early and/or extensive cell death, the cells were subjected to basal cell culture conditions for 40 h (preincubation) followed by 12, 24 and 48 h treatments with melflufen. Propidium iodide (PI) staining of DNA using Vindelovs technique was followed by quantitation with flow cytometry analysis. The percentage of cells in each cell cycle phase was determined with the ModFit LT software.
Click to Show/Hide
|
||||
| In Vitro Model | Hodgkin lymphoma | HDLM-2 cell | CVCL_0009 | ||
| Experiment 50 Reporting the Activity Data of This PDC | [8] | ||||
| Indication | lymphoma | ||||
| Efficacy Data | Half Maximal Inhibitory Concentration (IC50) |
0.12 μM
|
|||
| Description |
Cell cycle distribution analyses were performed on melflufen treated (0.1, 0.2 and 0.4 uM) and control cells from the KM-H2 and SU-DHL-10 cell lines in which the cytotoxic activity of melflufen during the 72 h FMCA assay was calculated as 0.92, 0.22, and 0.71 uM respectively (see Table3). To minimize potential artifacts emanating from cells exiting the analyzed cell populations, e.g. due to early and/or extensive cell death, the cells were subjected to basal cell culture conditions for 40 h (preincubation) followed by 12, 24 and 48 h treatments with melflufen. Propidium iodide (PI) staining of DNA using Vindelovs technique was followed by quantitation with flow cytometry analysis. The percentage of cells in each cell cycle phase was determined with the ModFit LT software.
Click to Show/Hide
|
||||
| In Vitro Model | Diffuse large B-cell lymphoma | U-2940 cell | CVCL_1897 | ||
| Experiment 51 Reporting the Activity Data of This PDC | [8] | ||||
| Indication | lymphoma | ||||
| Efficacy Data | Half Maximal Inhibitory Concentration (IC50) |
0.22 μM
|
|||
| Description |
Cell cycle distribution analyses were performed on melflufen treated (0.1, 0.2 and 0.4 uM) and control cells from the KM-H2 and SU-DHL-10 cell lines in which the cytotoxic activity of melflufen during the 72 h FMCA assay was calculated as 0.92, 0.22, and 0.71 uM respectively (see Table3). To minimize potential artifacts emanating from cells exiting the analyzed cell populations, e.g. due to early and/or extensive cell death, the cells were subjected to basal cell culture conditions for 40 h (preincubation) followed by 12, 24 and 48 h treatments with melflufen. Propidium iodide (PI) staining of DNA using Vindelovs technique was followed by quantitation with flow cytometry analysis. The percentage of cells in each cell cycle phase was determined with the ModFit LT software.
Click to Show/Hide
|
||||
| In Vitro Model | Hodgkin lymphoma | KM-H2 cell | CVCL_1330 | ||
| Experiment 52 Reporting the Activity Data of This PDC | [8] | ||||
| Indication | lymphoma | ||||
| Efficacy Data | Half Maximal Inhibitory Concentration (IC50) |
0.39 μM
|
|||
| Description |
Cell cycle distribution analyses were performed on melflufen treated (0.1, 0.2 and 0.4 uM) and control cells from the KM-H2 and SU-DHL-10 cell lines in which the cytotoxic activity of melflufen during the 72 h FMCA assay was calculated as 0.92, 0.22, and 0.71 uM respectively (see Table3). To minimize potential artifacts emanating from cells exiting the analyzed cell populations, e.g. due to early and/or extensive cell death, the cells were subjected to basal cell culture conditions for 40 h (preincubation) followed by 12, 24 and 48 h treatments with melflufen. Propidium iodide (PI) staining of DNA using Vindelovs technique was followed by quantitation with flow cytometry analysis. The percentage of cells in each cell cycle phase was determined with the ModFit LT software.
Click to Show/Hide
|
||||
| In Vitro Model | Diffuse large B-cell lymphoma germinal center B-cell type | DoHH2 cell | CVCL_1179 | ||
| Experiment 53 Reporting the Activity Data of This PDC | [8] | ||||
| Indication | lymphoma | ||||
| Efficacy Data | Half Maximal Inhibitory Concentration (IC50) |
0.42 μM
|
|||
| Description |
Cell cycle distribution analyses were performed on melflufen treated (0.1, 0.2 and 0.4 uM) and control cells from the KM-H2 and SU-DHL-10 cell lines in which the cytotoxic activity of melflufen during the 72 h FMCA assay was calculated as 0.92, 0.22, and 0.71 uM respectively (see Table3). To minimize potential artifacts emanating from cells exiting the analyzed cell populations, e.g. due to early and/or extensive cell death, the cells were subjected to basal cell culture conditions for 40 h (preincubation) followed by 12, 24 and 48 h treatments with melflufen. Propidium iodide (PI) staining of DNA using Vindelovs technique was followed by quantitation with flow cytometry analysis. The percentage of cells in each cell cycle phase was determined with the ModFit LT software.
Click to Show/Hide
|
||||
| In Vitro Model | Diffuse large B-cell lymphoma | SU-DHL-6 cell | CVCL_2206 | ||
| Experiment 54 Reporting the Activity Data of This PDC | [8] | ||||
| Indication | lymphoma | ||||
| Efficacy Data | Half Maximal Inhibitory Concentration (IC50) |
0.45 μM
|
|||
| Description |
Cell cycle distribution analyses were performed on melflufen treated (0.1, 0.2 and 0.4 uM) and control cells from the KM-H2 and SU-DHL-10 cell lines in which the cytotoxic activity of melflufen during the 72 h FMCA assay was calculated as 0.92, 0.22, and 0.71 uM respectively (see Table3). To minimize potential artifacts emanating from cells exiting the analyzed cell populations, e.g. due to early and/or extensive cell death, the cells were subjected to basal cell culture conditions for 40 h (preincubation) followed by 12, 24 and 48 h treatments with melflufen. Propidium iodide (PI) staining of DNA using Vindelovs technique was followed by quantitation with flow cytometry analysis. The percentage of cells in each cell cycle phase was determined with the ModFit LT software.
Click to Show/Hide
|
||||
| In Vitro Model | Diffuse large B-cell lymphoma germinal center B-cell type | RC-K8 cell | CVCL_1883 | ||
| Experiment 55 Reporting the Activity Data of This PDC | [8] | ||||
| Indication | lymphoma | ||||
| Efficacy Data | Half Maximal Inhibitory Concentration (IC50) |
0.52 μM
|
|||
| Description |
Cell cycle distribution analyses were performed on melflufen treated (0.1, 0.2 and 0.4 uM) and control cells from the KM-H2 and SU-DHL-10 cell lines in which the cytotoxic activity of melflufen during the 72 h FMCA assay was calculated as 0.92, 0.22, and 0.71 uM respectively (see Table3). To minimize potential artifacts emanating from cells exiting the analyzed cell populations, e.g. due to early and/or extensive cell death, the cells were subjected to basal cell culture conditions for 40 h (preincubation) followed by 12, 24 and 48 h treatments with melflufen. Propidium iodide (PI) staining of DNA using Vindelovs technique was followed by quantitation with flow cytometry analysis. The percentage of cells in each cell cycle phase was determined with the ModFit LT software.
Click to Show/Hide
|
||||
| In Vitro Model | Diffuse large B-cell lymphoma | U-2932 cell | CVCL_1896 | ||
| Experiment 56 Reporting the Activity Data of This PDC | [11] | ||||
| Indication | Breast cancer | ||||
| Efficacy Data | Half maximal inhibitory concentration (IC50) |
0.52 μmol/L
|
|||
| MOA of PDC |
Melphalan is a wellknown cancer drug used for decades for the treatment of various cancer types, and it is still widely used for hematological cancers today. It is an alkylating agent that works by adding an alkyl group to the guanine base of the DNA, resulting in an aberrant linkage between DNA strands, DNA breakage, and inhibition of DNA synthesis. Melphalan is a hydrophilic drug, and as such, it does not penetrate cell membranes easily, which is limiting to its anticancer potential. In contrast, melflufen (melphalan flufenamide), a new peptideconjugated alkylator, is highly lipophilic and therefore penetrates the cell membrane easily. Inside the cell, melflufen is rapidly hydrolyzed into less lipophilic metabolites that retain high alkylating potential, leading to their entrapment and accumulation. Aminopeptidases belong to a large family of enzymes that catalyze the cleavage of amino acids from the amino terminus of proteins or peptides and are shown to facilitate intracellular hydrolysis of melflufen. Aminopeptidases are involved in multiple cellular processes, and their expression and activity are frequently deregulated in cancer cells. For this reason, aminopeptidase inhibitors bestatin and tosedostat have been investigated in the clinical settings. Exploiting aminopeptidase activity to convert a lipophilic drug such as melflufen to an intracellular hydrophilic metabolite with high alkylating potential may offer an effective alternative therapeutic approach. Previously it has been shown that aminopeptidase N (ANPEP or CD13) can hydrolyze melflufen, but it is largely unknown whether melflufen can be a substrate for other aminopeptidases. Application of melflufen has mainly been focused on multiple myeloma, where it has shown promising results in phase 3 clinical trial in relapse and refractory patient population. 13 Yet it is unexplored whether melflufen can be effective in other cancer types such as breast cancer. Here, we demonstrate the efficacy of melflufen in D492HER2 breast epithelial cells overexpressing the HER2 oncogene and the triplenegative cell line MDAMB231.
Click to Show/Hide
|
||||
| Description |
IC50 values for melflufen of 0.046 μmol/L in D492HER2 cells and 0.52 μmol/L in D492 cells compared to doxorubicin values of 0.92 μmol/L for D492HER2 cells and 1.8 μmol/L for D492 underpin these findings (Figure 4B).
|
||||
| In Vitro Model | Normal | D492 cell | CVCL_D1HJ | ||
| Experiment 57 Reporting the Activity Data of This PDC | [8] | ||||
| Indication | lymphoma | ||||
| Efficacy Data | Half Maximal Inhibitory Concentration (IC50) |
0.71 μM
|
|||
| Description |
Cell cycle distribution analyses were performed on melflufen treated (0.1, 0.2 and 0.4 uM) and control cells from the KM-H2 and SU-DHL-10 cell lines in which the cytotoxic activity of melflufen during the 72 h FMCA assay was calculated as 0.92, 0.22, and 0.71 uM respectively (see Table3). To minimize potential artifacts emanating from cells exiting the analyzed cell populations, e.g. due to early and/or extensive cell death, the cells were subjected to basal cell culture conditions for 40 h (preincubation) followed by 12, 24 and 48 h treatments with melflufen. Propidium iodide (PI) staining of DNA using Vindelovs technique was followed by quantitation with flow cytometry analysis. The percentage of cells in each cell cycle phase was determined with the ModFit LT software.
Click to Show/Hide
|
||||
| In Vitro Model | Diffuse large B-cell lymphoma | SU-DHL-10 cell | CVCL_1889 | ||
| Experiment 58 Reporting the Activity Data of This PDC | [8] | ||||
| Indication | lymphoma | ||||
| Efficacy Data | Half Maximal Inhibitory Concentration (IC50) |
0.73 μM
|
|||
| Description |
Cell cycle distribution analyses were performed on melflufen treated (0.1, 0.2 and 0.4 uM) and control cells from the KM-H2 and SU-DHL-10 cell lines in which the cytotoxic activity of melflufen during the 72 h FMCA assay was calculated as 0.92, 0.22, and 0.71 uM respectively (see Table3). To minimize potential artifacts emanating from cells exiting the analyzed cell populations, e.g. due to early and/or extensive cell death, the cells were subjected to basal cell culture conditions for 40 h (preincubation) followed by 12, 24 and 48 h treatments with melflufen. Propidium iodide (PI) staining of DNA using Vindelovs technique was followed by quantitation with flow cytometry analysis. The percentage of cells in each cell cycle phase was determined with the ModFit LT software.
Click to Show/Hide
|
||||
| In Vitro Model | Hodgkin lymphoma | L-428 cell | CVCL_1361 | ||
| Experiment 59 Reporting the Activity Data of This PDC | [8] | ||||
| Indication | lymphoma | ||||
| Efficacy Data | Half Maximal Inhibitory Concentration (IC50) |
0.92 μM
|
|||
| Description |
Cell cycle distribution analyses were performed on melflufen treated (0.1, 0.2 and 0.4 uM) and control cells from the KM-H2 and SU-DHL-10 cell lines in which the cytotoxic activity of melflufen during the 72 h FMCA assay was calculated as 0.92, 0.22, and 0.71 uM respectively (see Table3). To minimize potential artifacts emanating from cells exiting the analyzed cell populations, e.g. due to early and/or extensive cell death, the cells were subjected to basal cell culture conditions for 40 h (preincubation) followed by 12, 24 and 48 h treatments with melflufen. Propidium iodide (PI) staining of DNA using Vindelovs technique was followed by quantitation with flow cytometry analysis. The percentage of cells in each cell cycle phase was determined with the ModFit LT software.
Click to Show/Hide
|
||||
| In Vitro Model | Diffuse large B-cell lymphoma | DB cell | CVCL_1168 | ||
References