Peptide-drug Conjugate Information
General Information of This Peptide-drug Conjugate (PDC)
| PDC ID |
PDC_00029
|
|||||
|---|---|---|---|---|---|---|
| PDC Name |
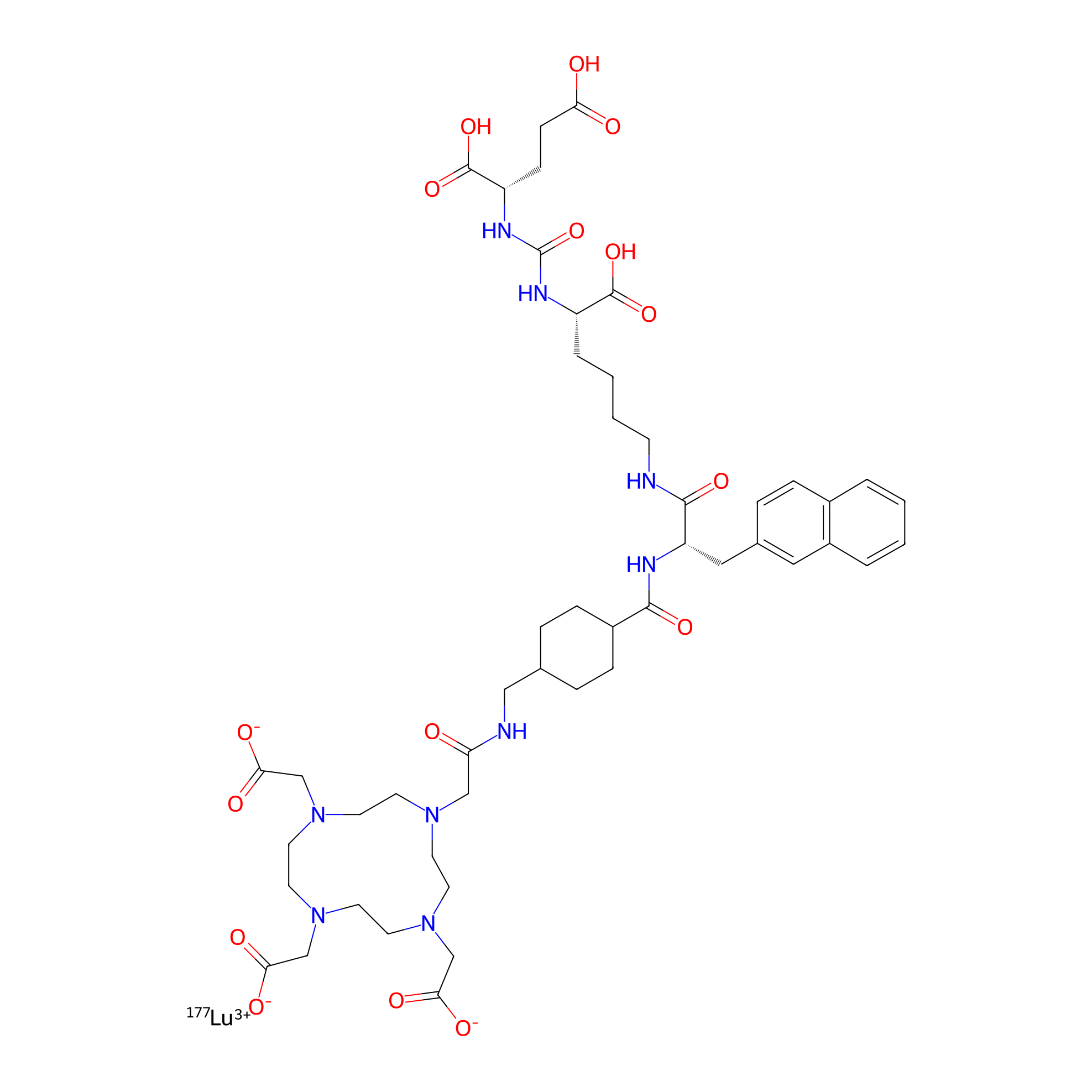
177Lu-PSMA-617
|
|||||
| Synonyms |
Vipivotide tetraxetan Lu-177; 177Lu-Psma-617; G6UF363ECX; Lutetium Lu-177 vipivotide tetraxetan; 177Lu-Labeled PSMA-617; PSMA-617 Lu-177; UNII-G6UF363ECX; Vipivotide tetraxetan lutetium Lu-177; Lutetium (177Lu) vipivotide tetraxetan; lutetium lu 177 vipivotide tetraxetan [USAN]; WHO 11429; 1703749-62-5; PLUVICTO; lutetium ((1)Lu) vipivotide tetraxetan [INN]; Lutetium (177Lu) vipivotide tetraxetan [INN]; LUTETIUM (177LU) VIPIVOTIDE TETRAXETAN [WHO-DD]; LUTETATE(3-)-177LU, (N-((((1S)-1-CARBOXY-5-(((2S)-3-(2-NAPHTHALENYL)-1-OXO-2-(((TRANS-4-(((2-(4,7,10-TRIS((CARBOXY-.KAPPA.O)METHYL)-1,4,7,10-TETRAAZACYCLODODEC-1-YL-.KAPPA.N1,.KAPPA.N4,.KAPPA.N7,.KAPPA.N10)ACETYL-.KAPPA.O)AMINO)METHYL)CYCLOHEXYL)CARBONYL)AMINO)PROPYL)AMINO)PENTYL)AMINO)CARBONYL)-L-GLUTAMATO(6-))-, HYDROGEN (1:3); LUTETATE(3-)-177LU, (N2-((((1S)-1,3-DICARBOXYPROPYL)AMINO)CARBONYL)-N6-(3-(2-NAPHTHALENYL)-N-((TRANS-4-(((2-(4,7,10-TRIS((CARBOXY-.KAPPA.O)METHYL)-1,4,7,10-TETRAAZACYCLODODEC-1-YL-.KAPPA.N1,.KAPPA.N4,.KAPPA.N7,.KAPPA.N10)ACETYL-.KAPPA.O)AMINO)METHYL)CYCLOHEXYL)CARBONYL)-L-ALANYL)-L-LYSINATO(6-))-, HYDROGEN (1:3
Click to Show/Hide
|
|||||
| PDC Status |
Approved
|
|||||
| Indication |
In total 6 Indication(s)
|
|||||
| Structure |
|
|||||
| Peptide Name |
PSMA-617
|
Peptide Info | ||||
| Receptor Name |
Glutamate carboxypeptidase 2 (FOLH1)
|
Receptor Info | ||||
| Drug Name |
Lutetium-177
|
Drug Info | ||||
| Therapeutic Target |
Human Deoxyribonucleic acid (hDNA)
|
Target Info | ||||
| Linker Name |
(S)-2-(4-(aminomethyl)cyclohexane-1-carboxamido)-3-(naphthalen-2-yl)propanoic acid
|
Linker Info | ||||
| Peptide Modified Type |
The modification of binding with chemical molecules
|
|||||
| Modified Segment |
Urea
|
|||||
| Absorption |
Following intravenous injection, Ga-68 PSMA-11 uptake occurs in the adrenal and prostate glands, with high uptake in PSMA-expressing tissues. Uptake of the drug is very minimal in the cerebral cortex, heart, and lungs. Mean maximum standardized uptake value (SUVmax) at later acquisition times is about 15.3.
|
|||||
| Distribution |
Ga-68 PSMA-11 accumulates in the liver (15%), kidneys (7%), spleen (2%), and salivary glands (0.5%). Ga-68 PSMA-11 accumulation increases at later acquisition times.
|
|||||
| Metabolism |
Ga-68 PSMA-11 decays to stable zinc-68.
|
|||||
| Excretion |
About 14% of the total injected dose is excreted in the urine within two hours following intravenous administration.
|
|||||
| Drugbank ID | ||||||
| ChEBI ID | ||||||
| Formula |
C49H68LuN9O16
|
|||||
| #Ro5 Violations (Lipinski): 4 | Molecular Weight (mw) | 1216.1 | ||||
| Lipid-water partition coefficient (xlogp) | Not Available | |||||
| Hydrogen Bond Donor Count (hbonddonor) | 8 | |||||
| Hydrogen Bond Acceptor Count (hbondacc) | 20 | |||||
| Rotatable Bond Count (rotbonds) | 24 | |||||
Full List of Activity Data of This Peptide-drug Conjugate
Identified from the Human Clinical Data
| Experiment 1 Reporting the Activity Data of This PDC | [1] | ||||
| Indication | ATM-mutated metastatic castration resistant prostate cancer | ||||
| Efficacy Data | α-fetoprotein increase rate |
61.89%
|
|||
| Administration Time | 1 month | ||||
| Administration Dosage | 7.5 GBq | ||||
| Description |
177Lu-PSMA 7.5 GBq was given to the patient (-fetoprotein: 38,669 ng/mL), and posttherapy imaging was performed 48 hours after the intravenous administration of 177Lu-PSMA. Adequate uptakes were detected in metastatic lesions on whole-body posttherapy images (A, B) similar to pretreatment 68Ga-PSMA PET/CT. The patient well tolerated the treatment without any adverse effects. However, in follow-up at month 1, -fetoprotein level progressed to 62,600 ng/mL, and 68Ga-PSMA PET/CT was planned.
Click to Show/Hide
|
||||
| In Vivo Model | A 46-year-old man who had progressive metastatic testicular mixed germ cell tumor. | ||||
| Experiment 2 Reporting the Activity Data of This PDC | [2] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | ≥10% PSA decline |
58%
|
|||
| Patients Enrolled |
Patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | At least one course of [177lu]-psma-617 | ||||
| Administration Dosage | 6-7 GBq | ||||
| MOA of PDC |
[177Lu]-PSMA-617 is a novel treatment modality for prostate cancer, utilizing the tumors expression of PSMA as a target to allow for the administration of mixed beta-gamma radiation directly to the site of active metastases.
|
||||
| Description |
A subjective clinical benefit, based on the clinical evaluation by the treating oncologist, was observed in 28 patients (52%). The first PSA was measured following a median of 1.2 months from the start of treatment (range 0.4-3.7 months). PSA nadir was achieved within a median of 1.4 months (range 0.4-13.4). A maximal PSA decline of at least 20% was observed in 26 patients (50%), a maximal PSA decline of at least 50% was observed in 18 patients (35%), and a maximal PSA decline of at least 90% was observed in 7 patients (16%). Thirty patients (58%) had any PSA decline (PSA decline greater than 10%) upon their first PSA assessment.
Click to Show/Hide
|
||||
| Experiment 3 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | 18-month overall survival (OS) |
63.80%
|
|||
| Patients Enrolled |
68 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 3 cycles every six weeks | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
Another study retrospectively examined outcomes in 68 patients with a mean of 71 years of age (range 46-89) who were treated with a mean of three cycles of 177Lu-PSMA-617 (median of 3, range 1-7 cycles) every six weeks. The 18-month overall survival was 63.8%. Those with a baseline PSA <20 ug/L had a higher 18-month survival estimate (79.9%) versus those with PSA levels greater than 20 ug/L (53.8%, p = < 0.05). Those with an SUVmax greater than 15 had a higher 18-month survival rate of 56% compared to those with SUVmax less than 15 (p = < 0.05). Their study found any decrease in PSA levels after two cycles of treatment was indicative of greater chance of overall survival (p = < 0.01).
Click to Show/Hide
|
||||
| Experiment 4 Reporting the Activity Data of This PDC | [2] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >20% PSA decline |
50.00%
|
|||
| Patients Enrolled |
Patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | At least one course of [177lu]-psma-617 | ||||
| Administration Dosage | 6-7 GBq | ||||
| MOA of PDC |
[177Lu]-PSMA-617 is a novel treatment modality for prostate cancer, utilizing the tumors expression of PSMA as a target to allow for the administration of mixed beta-gamma radiation directly to the site of active metastases.
|
||||
| Description |
A subjective clinical benefit, based on the clinical evaluation by the treating oncologist, was observed in 28 patients (52%). The first PSA was measured following a median of 1.2 months from the start of treatment (range 0.4-3.7 months). PSA nadir was achieved within a median of 1.4 months (range 0.4-13.4). A maximal PSA decline of at least 20% was observed in 26 patients (50%), a maximal PSA decline of at least 50% was observed in 18 patients (35%), and a maximal PSA decline of at least 90% was observed in 7 patients (16%). Thirty patients (58%) had any PSA decline (PSA decline greater than 10%) upon their first PSA assessment.
Click to Show/Hide
|
||||
| Experiment 5 Reporting the Activity Data of This PDC | [4] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >20% PSA decline |
63.00%
|
|||
| Patients Enrolled |
19 patients with metastatic castration-resistant prostate cancer, median age 68.8 years (range: 56.9 - 83.3).
|
||||
| Administration Time | Every 6-8 weeks | ||||
| Administration Dosage | 7.64 MBq per cycle | ||||
| Description |
Patients presented with bone, lymph node, and visceral metastases (89%, 68%, and 21%, respectively). All patients were pretreated with docetaxel, either abiraterone or enzalutamide, or both. Biochemical response in terms of PSA decline ≥50 or ≥30% was observed in 42% and 63%, respectively. There were significant correlations between PSA and PSMA mRNA expression, as well as tumor volumes (both MTV and TTV), AR-FL and AR-V7 mRNA expression. However, there was no correlation with response to PSMA treatment.
Click to Show/Hide
|
||||
| Experiment 6 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >25% PSA decline |
60.00%
|
|||
| Patients Enrolled |
30 patients with PSMA-positive prostate tumor.
|
||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
177Lu-PSMA-617 was offered to thirty patients with PSMA-positive prostate tumor. Treatment efficacy was retrospectively assessed by PSA levels with 70% of patients demonstrating a decrease in PSA levels. 18 patients were noted to have PSA decline greater than 25%, while 13 patients had a decline greater than 50%. Six of these patients were restaged using PSMA PET/CT (positron emission tomography/computed tomography), and all six patients had a response rate of more than 50% in SUVmax (maximum standardized uptake value) of the tumor.
Click to Show/Hide
|
||||
| Experiment 7 Reporting the Activity Data of This PDC | [5] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >25% PSA increase |
44.00%
|
|||
| Patients Enrolled |
45 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 164 cycles of rnt, every 6-8 weeks | ||||
| Description |
Forty-five patients were treated with total of 164 cycles of RNT. Fifteen patients (33%) had PSA decline of ≥50%, 23 patients (51%) showed any PSA decline and 20 patients (44%) showed PSA increase of ≥25%. Median OS and PFS were 17,1 months and 7,4 months. Patients had any or ≥50% PSA response after the first cycle, lower initial ALP (<120U/L) had longer OS and PFS. Patients had normal Hb showed longer OS and patients had lower initial PSA (<51ng/mL) had longer PFS. Patients had PSA progression of ≥25% had shorter OS and PFS.
Click to Show/Hide
|
||||
| Experiment 8 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >30% PSA decline |
60.00%
|
|||
| Patients Enrolled |
10 patients with metastatic castration-resistant prostate cancer.
|
||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
A small two center study was conducted in 2015, which followed ten mCRPC patients treated with 177Lu-PSMA-617. Response was evaluated by change in PSA. Eight weeks after therapy, seven out of the 10 study subjects, experienced a decline in PSA. Six out of ten patients had a decline more than 30%, while five patients had a decline of more than 50% in their PSA levels. Three patients showed an increase in PSA indicative of progression of disease. Post-treatment PSA levels declined significantly in this study, indicating positive treatment response.
Click to Show/Hide
|
||||
| Experiment 9 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
44.00%
|
|||
| Patients Enrolled |
50 patients with progressive, PSMA-positive, symptomatic metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 4 cycles every 6 weeks | ||||
| Administration Dosage | 7.5 GBq (range 4-8.9 GBq) | ||||
| MOA of PDC |
Lutetium Lu 177 vipivotide tetraxetan is a PSMA-binding ligand bound to a DOTA chelator (i.e., tetraxetan) radiolabeled with lutetium-177. Once lutetium Lu 177 vipivotide tetraxetan is bound to PSMA-expressing cells, the beta-minus emission from lutetium-177 delivers radiation to PSMA-expressing and surrounding cells, inducing DNA damage that leads to cell death. The exposure-efficacy relationships of lutetium Lu 177 vipivotide tetraxetan and the time course of the pharmacodynamic response are not fully characterized [9]. Lutetium-177 decays to a stable hafnium-177 with a physical half-life of 6.647 days by emitting beta-minus radiation with a maximum energy of 0.498 MeV (79%) and photonic radiation (γ) of 0.208 MeV (11%) and 0.113 MeV (6.4%).
Click to Show/Hide
|
||||
| Description |
A PSA response (PSA reduction of ≥ 50% from baseline) was seen in 32 of 50 patients (64%) with progressive, PSMA-positive, symptomatic mCRPC who received up to 4 cycles of lutetium Lu 177 vipivotide tetraxetan every 6 weeks in the LuPSMA study (ACTRN12615000912583). 22 of 50 patients (44%) had a ≥ 80% decrease in PSA. At a median follow-up of 31.4 months, median OS was 13.3 months in the overall population and 18.4 months in those achieving a PSA response.
Click to Show/Hide
|
||||
| Half life period | 41.6 h | ||||
| Related Clinical Trial | |||||
| NCT Number | ACTRN12615000912583 | Clinical Status | Phase 2 | ||
| Clinical Description | Background: Lutetium-177 (177Lu)-PSMA-617 (LuPSMA) is a radiolabelled small molecule that binds with high affinity to prostate specific membrane antigen (PSMA) enabling targeted delivery of beta-radiation. We have previously reported favourable activity with low toxicity in a 30 patient study in men with metastatic castrate-resistant prostate cancer (mCRPC) and now report updated results including a twenty patient extension cohort. Methods: In this phase II trial, 50 patients with PSMA-avid mCRPC who had progressed after standard therapies received up to 4 cycles of LuPSMA every 6 weeks. The primary endpoints were PSA response (PCWG2) and toxicity (CTCAE v4). Other endpoints included imaging response, PSA PFS and OS. Cut-off for analysis 5 Oct 2018. Results: 76 men were screened to identify 50 patients eligible for treatment. Median PSA doubling time was 2.6 months. The majority of patients had received prior docetaxel (84%), cabazitaxel (48%), and abiraterone and/or enzalutamide (90%). The mean administered radioactivity was 7.5 GBq/cycle. PSA decline 50% was achieved in 32 of 50 patients (64%, 95% CI 50-77%), including 22 patients (44%, 95% CI 30-59%) with a PSA decline 80%. 27 patients had measurable soft tissue at baseline and 56% of these patients had a partial or complete response by RECIST 1.1. The most common toxicities attributed to LuPSMA were transient G1-2 dry mouth in 68%, G1-2 nausea in 48%, and G1-2 fatigue in 36%. G3-4 toxicities attributed to LuPSMA were infrequent with thrombocytopenia in 10% and anaemia in 10%. Median PSA PFS was 6.9 months (95% CI 6.0-8.7) and median OS was 13.3 months (95% CI 10.5-18.0). Upon subsequent progression, further LuPSMA was administered to 14 patients (median 2 cycles commencing 359 days from enrolment); PSA 50% response occurred in 9 patients (64%). Conclusions: This expanded 50 patient cohort confirms high response rates and low toxicity with LuPSMA in men who had progressed after standard therapies. In patients who subsequently progressed and were administered further LuPSMA, high response rates were also observed. These results have provided the basis for randomised controlled trials currently underway. | ||||
| Experiment 10 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
52.00%
|
|||
| Patients Enrolled |
254 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 3 median number cycles, delivered at a median interval of 5.7 weeks | ||||
| Administration Dosage | 6.5 GBq/cycle (median cumulative dose 21.2 GBq) | ||||
| MOA of PDC |
Lutetium Lu 177 vipivotide tetraxetan is a PSMA-binding ligand bound to a DOTA chelator (i.e., tetraxetan) radiolabeled with lutetium-177. Once lutetium Lu 177 vipivotide tetraxetan is bound to PSMA-expressing cells, the beta-minus emission from lutetium-177 delivers radiation to PSMA-expressing and surrounding cells, inducing DNA damage that leads to cell death. The exposure-efficacy relationships of lutetium Lu 177 vipivotide tetraxetan and the time course of the pharmacodynamic response are not fully characterized [9]. Lutetium-177 decays to a stable hafnium-177 with a physical half-life of 6.647 days by emitting beta-minus radiation with a maximum energy of 0.498 MeV (79%) and photonic radiation (γ) of 0.208 MeV (11%) and 0.113 MeV (6.4%).
Click to Show/Hide
|
||||
| Description |
A ≥ 50% reduction in PSA was seen in 52.0% of patients (132/254); at a median follow-up of 14.5 months, median PSA PFS was 5.5 months and median OS was 14.5 months. The median dose of lutetium Lu 177 vipivotide tetraxetan was 6.5 GBq/cycle (median cumulative dose 21.2 GBq), the median number cycles was 3, delivered at a median interval of 5.7 weeks.
Click to Show/Hide
|
||||
| Half life period | 41.6 h | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT04833517 | Clinical Status | Phase 2 | ||
| Clinical Description | This prospective registry aims to assess outcome and toxicity of targeted radionuclide therapies in patients with advanced prostate cancer in clinical routine. While the major investigated treatment modality is prostate-specific membrane antigen (PSMA)-targeted radioligand therapy, also other radionuclide therapies such as Ra223 and liver-directed radioembolization are included. The investigators believe that prospectively assessed long-term outcome data on implementation of radionuclide therapy, especially in the palliative setting of advanced mCRPC, help to better define the real benefits and risks of the respective treatment modalities for patients regarding survival and quality-of-life. | ||||
| Experiment 11 Reporting the Activity Data of This PDC | [7], [8] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
57.00%
|
|||
| Patients Enrolled |
Between Aug 26, 2015, and Dec 8, 2016, 43 men were screened to identify 30 patients eligible for treatment. 26 (87%) had received at least one line of previous chemotherapy (80% docetaxel and 47% cabazitaxel) and 25 (83%) received prior abiraterone acetate, enzalutamide, or both.
|
||||
| Administration Time | Every 6 weeks for up to six doses | ||||
| Administration Dosage | 7.4 GBq | ||||
| MOA of PDC |
After binding to the PSMA receptor, [177Lu]Lu-PSMA-617 is internalized into the PSMA positive cells, resulting in a long retention within these cells; the high energy electrons emitted during the decay can selectively induce tissue and DNA damage, leading to cell death.
|
||||
| Description |
The authors reported that 57% of patients enrolled in the study had PSA reductions of greater than 50%, and significant improvements in quality of life were reported, which rapidly manifested after initiation of the therapy.
|
||||
| Half life period | 41.1 ± 9.3 h | ||||
| Related Clinical Trial | |||||
| NCT Number | ACTRN12615000912583 | Clinical Status | Phase 2 | ||
| Experiment 12 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
60.00%
|
|||
| Patients Enrolled |
15 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | Every 8weeks, up to 4 cycles | ||||
| Administration Dosage | 6.0-7.4 GBq/cycle | ||||
| MOA of PDC |
Lutetium Lu 177 vipivotide tetraxetan is a PSMA-binding ligand bound to a DOTA chelator (i.e., tetraxetan) radiolabeled with lutetium-177. Once lutetium Lu 177 vipivotide tetraxetan is bound to PSMA-expressing cells, the beta-minus emission from lutetium-177 delivers radiation to PSMA-expressing and surrounding cells, inducing DNA damage that leads to cell death. The exposure-efficacy relationships of lutetium Lu 177 vipivotide tetraxetan and the time course of the pharmacodynamic response are not fully characterized [9]. Lutetium-177 decays to a stable hafnium-177 with a physical half-life of 6.647 days by emitting beta-minus radiation with a maximum energy of 0.498 MeV (79%) and photonic radiation (γ) of 0.208 MeV (11%) and 0.113 MeV (6.4%).
Click to Show/Hide
|
||||
| Description |
60% of patients (9/15) in the lutetium Lu 177 vipivotide tetraxetan arm and 40% (8/20) in the docetaxel arm achieved a ≥ 50% decline in PSA from baseline [between-group difference 20%; 95% CI -12 to 47 (noninferiority margin of -15 in per protocol analysis achieved)]. Patients were administered lutetium Lu 177 vipivotide tetraxetan (6.0-7.4 GBq/cycle, every 8 weeks, up to 4 cycles) or docetaxel (75 mg/m2/cycle, every 3 weeks, up to 10 cycles).
Click to Show/Hide
|
||||
| Half life period | 41.6 h | ||||
| Related Clinical Trial | |||||
| NCT Number | CTRI/2019/12/022282 | Clinical Status | Phase 2 | ||
| Clinical Description | This was an investigator-initiated, randomized, parallel group, open-label, and phase 2 non-inferiority trial conducted at a tertiary care institution. Between December 2019 and March 2021, patients with biopsy-proven adenocarcinoma prostate and castration-resistant disease were recruited. Patients were considered eligible if they had metastatic disease on 68 Ga-PSMA-11 PET/CT with significant PSMA expression. Significant PSMA expression was defined as tracer avidity of at least 80% of the lesions being significantly (1.5 times) greater than that of normal liver with none of the lesions having uptake less than that of liver. Only chemotherapy-nave patients were considered for inclusion in this trial; however, patients with prior treatment of NAADs were also included. The patients were required to have Eastern Cooperative Oncology Group (ECOG) performance score2, and adequate haematological, renal, and liver function reserve (Supplementary Table 1). Patients with histological evidence of sarcomatous, spindle-cell or small-cell differentiation, and Sjogren syndrome were excluded. Informed written consent was obtained from the patients prior to inclusion in the study. The study was approved by the Institute Ethics Committee (INT/IEC/2019/001972) and was conducted in accordance with the guidelines enshrined in the Declaration of Helsinki. The trial was also prospectively registered at the Clinical Trials Registry-India (CTRI/2019/12/022282). | ||||
| Experiment 13 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
64.00%
|
|||
| Patients Enrolled |
50 patients with progressive, PSMA-positive, symptomatic metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 4 cycles every 6 weeks | ||||
| Administration Dosage | 7.5 GBq (range 4-8.9 GBq) | ||||
| MOA of PDC |
Lutetium Lu 177 vipivotide tetraxetan is a PSMA-binding ligand bound to a DOTA chelator (i.e., tetraxetan) radiolabeled with lutetium-177. Once lutetium Lu 177 vipivotide tetraxetan is bound to PSMA-expressing cells, the beta-minus emission from lutetium-177 delivers radiation to PSMA-expressing and surrounding cells, inducing DNA damage that leads to cell death. The exposure-efficacy relationships of lutetium Lu 177 vipivotide tetraxetan and the time course of the pharmacodynamic response are not fully characterized [9]. Lutetium-177 decays to a stable hafnium-177 with a physical half-life of 6.647 days by emitting beta-minus radiation with a maximum energy of 0.498 MeV (79%) and photonic radiation (γ) of 0.208 MeV (11%) and 0.113 MeV (6.4%).
Click to Show/Hide
|
||||
| Description |
A PSA response (PSA reduction of ≥ 50% from baseline) was seen in 32 of 50 patients (64%) with progressive, PSMA-positive, symptomatic mCRPC who received up to 4 cycles of lutetium Lu 177 vipivotide tetraxetan every 6 weeks in the LuPSMA study (ACTRN12615000912583). 22 of 50 patients (44%) had a ≥ 80% decrease in PSA. At a median follow-up of 31.4 months, median OS was 13.3 months in the overall population and 18.4 months in those achieving a PSA response.
Click to Show/Hide
|
||||
| Half life period | 41.6 h | ||||
| Related Clinical Trial | |||||
| NCT Number | ACTRN12615000912583 | Clinical Status | Phase 2 | ||
| Clinical Description | Background: Lutetium-177 (177Lu)-PSMA-617 (LuPSMA) is a radiolabelled small molecule that binds with high affinity to prostate specific membrane antigen (PSMA) enabling targeted delivery of beta-radiation. We have previously reported favourable activity with low toxicity in a 30 patient study in men with metastatic castrate-resistant prostate cancer (mCRPC) and now report updated results including a twenty patient extension cohort. Methods: In this phase II trial, 50 patients with PSMA-avid mCRPC who had progressed after standard therapies received up to 4 cycles of LuPSMA every 6 weeks. The primary endpoints were PSA response (PCWG2) and toxicity (CTCAE v4). Other endpoints included imaging response, PSA PFS and OS. Cut-off for analysis 5 Oct 2018. Results: 76 men were screened to identify 50 patients eligible for treatment. Median PSA doubling time was 2.6 months. The majority of patients had received prior docetaxel (84%), cabazitaxel (48%), and abiraterone and/or enzalutamide (90%). The mean administered radioactivity was 7.5 GBq/cycle. PSA decline 50% was achieved in 32 of 50 patients (64%, 95% CI 50-77%), including 22 patients (44%, 95% CI 30-59%) with a PSA decline 80%. 27 patients had measurable soft tissue at baseline and 56% of these patients had a partial or complete response by RECIST 1.1. The most common toxicities attributed to LuPSMA were transient G1-2 dry mouth in 68%, G1-2 nausea in 48%, and G1-2 fatigue in 36%. G3-4 toxicities attributed to LuPSMA were infrequent with thrombocytopenia in 10% and anaemia in 10%. Median PSA PFS was 6.9 months (95% CI 6.0-8.7) and median OS was 13.3 months (95% CI 10.5-18.0). Upon subsequent progression, further LuPSMA was administered to 14 patients (median 2 cycles commencing 359 days from enrolment); PSA 50% response occurred in 9 patients (64%). Conclusions: This expanded 50 patient cohort confirms high response rates and low toxicity with LuPSMA in men who had progressed after standard therapies. In patients who subsequently progressed and were administered further LuPSMA, high response rates were also observed. These results have provided the basis for randomised controlled trials currently underway. | ||||
| Experiment 14 Reporting the Activity Data of This PDC | [7], [9] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
64.00%
|
|||
| Patients Enrolled |
Seventy-five patients were screened to identify 50 evaluable patients. Sixteen patients were excluded because of either low PSMA expression (n = 8) or discordant sites of 18F-FDG-positive PSMA-negative disease. Fifty patients with PSMA-avid metastatic castration-resistant prostate cancer who had progressed after standard therapies received up to 4 cycles of <sup>177</sup>Lu-PSMA every 6 wk.
Click to Show/Hide
|
||||
| Administration Time | Every 6 weeks for up to six doses | ||||
| Administration Dosage | 7.4 GBq | ||||
| MOA of PDC |
After binding to the PSMA receptor, [177Lu]Lu-PSMA-617 is internalized into the PSMA positive cells, resulting in a long retention within these cells; the high energy electrons emitted during the decay can selectively induce tissue and DNA damage, leading to cell death.
|
||||
| Description |
The overall results of this study are in good agreement with those reported in previous retrospective studies. In an extension of this study, the group around Hofman reported even higher efficacy, with PSA response rates of at least 50% in 64% of all cases, whereas toxicity was similar to the first results.
|
||||
| Half life period | 41.1 ± 9.3 h | ||||
| Related Clinical Trial | |||||
| NCT Number | ACTRN12615000912583 | Clinical Status | Phase 2 | ||
| Experiment 15 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
66.00%
|
|||
| Patients Enrolled |
65 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | ≤6 cycles every 6 weeks | ||||
| Administration Dosage | 6.0-8.5 GBq | ||||
| MOA of PDC |
Lutetium Lu 177 vipivotide tetraxetan is a PSMA-binding ligand bound to a DOTA chelator (i.e., tetraxetan) radiolabeled with lutetium-177. Once lutetium Lu 177 vipivotide tetraxetan is bound to PSMA-expressing cells, the beta-minus emission from lutetium-177 delivers radiation to PSMA-expressing and surrounding cells, inducing DNA damage that leads to cell death. The exposure-efficacy relationships of lutetium Lu 177 vipivotide tetraxetan and the time course of the pharmacodynamic response are not fully characterized [9]. Lutetium-177 decays to a stable hafnium-177 with a physical half-life of 6.647 days by emitting beta-minus radiation with a maximum energy of 0.498 MeV (79%) and photonic radiation (γ) of 0.208 MeV (11%) and 0.113 MeV (6.4%).
Click to Show/Hide
|
||||
| Description |
65 of 99 patients treated with lutetium Lu 177 vipivotide tetraxetan 6.0-8.5 GBq every 6 weeks for up to 6 cycles (n = 99) compared with 37 of 101 patients receiving cabazitaxel 20 mg/m2 every 3 weeks for up to 10 cycles achieved a PSA reduction of ≥ 50% from baseline [66% vs 37%; treatment difference 29% (95% CI 16-42); p < 0.0001 (ITT analysis)]. Lutetium Lu 177 vipivotide tetraxetan also delayed disease progression [HR 0.63 (95% CI 0.46-0.86;) p = 0.0028], radiographic progression [0.64 (95% CI 0.46-0.88); p = 0.0070] and PSA PFS [0.60 (95% CI 0.44-0.83); p = 0.0017] compared with cabazitaxel.
Click to Show/Hide
|
||||
| Half life period | 41.6 h | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT03392428 | Clinical Status | Phase 2 | ||
| Clinical Description | This open label, randomised, stratified, 2-arm, multicentre, phase 2 trial aims to determine the activity and safety of Lu-PSMA vs cabazitaxel in men with progressive metastatic castration resistant prostate cancer | ||||
| Experiment 16 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
50.00%
|
|||
| Administration Time | 2 cycles | ||||
| Administration Dosage | A first cycle of 3 GBq, followed by a second cycle with 3-6 GBq after 7-9 weeks | ||||
| MOA of PDC |
Lutetium Lu 177 vipivotide tetraxetan is a PSMA-binding ligand bound to a DOTA chelator (i.e., tetraxetan) radiolabeled with lutetium-177. Once lutetium Lu 177 vipivotide tetraxetan is bound to PSMA-expressing cells, the beta-minus emission from lutetium-177 delivers radiation to PSMA-expressing and surrounding cells, inducing DNA damage that leads to cell death. The exposure-efficacy relationships of lutetium Lu 177 vipivotide tetraxetan and the time course of the pharmacodynamic response are not fully characterized [9]. Lutetium-177 decays to a stable hafnium-177 with a physical half-life of 6.647 days by emitting beta-minus radiation with a maximum energy of 0.498 MeV (79%) and photonic radiation (γ) of 0.208 MeV (11%) and 0.113 MeV (6.4%).
Click to Show/Hide
|
||||
| Description |
A pilot study (NCT03828838) showed that treatment with lutetium Lu 177 vipivotide tetraxetan was effective in patients with PSMA-expressing, low volume (≥ 1 but ≤ 10 positive lesions on PSMA-PET) metastatic hormone-sensitive prostate cancer (mHSPC). After 2 cycles of lutetium Lu 177 vipivotide tetraxetan (a first cycle of 3 GBq, followed by a second cycle with 3-6 GBq after 7-9 weeks), 5 of 10 patients showed a > 50% PSA reduction and in one patient, PSA was undetectable.
Click to Show/Hide
|
||||
| In Vivo Model | PSMA-expressing, low volume (≥ 1 but ≤ 1010 positive lesions on PSMA-PET) metastatic hormone-sensitive prostate cancer (mHSPC). | ||||
| Half life period | 41.6 h | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT03828838 | Clinical Status | Phase 1/2 | ||
| Clinical Description | Radioligand therapy (RLT) using Lu-177 labelled PSMA is a promising new therapeutic approach to treat metastatic prostate cancer. This tumor-specific treatment is directed against prostate-specific membrane antigen (PSMA), which is overexpressed in prostate cancer cells. In the last few years, several lutetium-177 (177Lu, emitter) labeled PSMA ligands have been developed and are currently applied to treat metastatic castrate resistant prostate cancer (mCRPC) patients. However, there are no prospective studies published so far using this treatment approach in hormone sensitive setting. In this pilot study patients with hormone sensitive prostate cancer who did not undergo hormonal treatment will be treated with Lu-177 PSMA-617. | ||||
| Experiment 17 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
50.00%
|
|||
| Patients Enrolled |
10 patients with low volume (≥ 1 but ≤ 10 positive lesions on PSMA-PET) metastatic hormone-sensitive prostate cancer.
|
||||
| Administration Time | 2 cycles | ||||
| Administration Dosage | A first cycle of 3 GBq, followed by a second cycle with 3-6 GBq after 7-9 weeks | ||||
| MOA of PDC |
Lutetium Lu 177 vipivotide tetraxetan is a PSMA-binding ligand bound to a DOTA chelator (i.e., tetraxetan) radiolabeled with lutetium-177. Once lutetium Lu 177 vipivotide tetraxetan is bound to PSMA-expressing cells, the beta-minus emission from lutetium-177 delivers radiation to PSMA-expressing and surrounding cells, inducing DNA damage that leads to cell death. The exposure-efficacy relationships of lutetium Lu 177 vipivotide tetraxetan and the time course of the pharmacodynamic response are not fully characterized [9]. Lutetium-177 decays to a stable hafnium-177 with a physical half-life of 6.647 days by emitting beta-minus radiation with a maximum energy of 0.498 MeV (79%) and photonic radiation (γ) of 0.208 MeV (11%) and 0.113 MeV (6.4%).
Click to Show/Hide
|
||||
| Description |
After 2 cycles of lutetium Lu 177 vipivotide tetraxetan (a first cycle of 3 GBq, followed by a second cycle with 3-6 GBq after 7-9 weeks), 5 of 10 patients showed a > 50% PSA reduction and in one patient, PSA was undetectable.
|
||||
| Half life period | 41.6 h | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT03828838 | Clinical Status | Phase 1/2 | ||
| Clinical Description | Radioligand therapy (RLT) using Lu-177 labelled PSMA is a promising new therapeutic approach to treat metastatic prostate cancer. This tumor-specific treatment is directed against prostate-specific membrane antigen (PSMA), which is overexpressed in prostate cancer cells. In the last few years, several lutetium-177 (177Lu, emitter) labeled PSMA ligands have been developed and are currently applied to treat metastatic castrate resistant prostate cancer (mCRPC) patients. However, there are no prospective studies published so far using this treatment approach in hormone sensitive setting. In this pilot study patients with hormone sensitive prostate cancer who did not undergo hormonal treatment will be treated with Lu-177 PSMA-617. | ||||
| Experiment 18 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
54.00%
|
|||
| Patients Enrolled |
27 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 7.4-22 gbq on days 1 and 15 in the p hase 1 dose-escalation co hort (n = 29); 22gbq on days 1 and 15 in the p hase 2 co hort (n = 21) | ||||
| Administration Dosage | 22 GBq | ||||
| MOA of PDC |
Lutetium Lu 177 vipivotide tetraxetan is a PSMA-binding ligand bound to a DOTA chelator (i.e., tetraxetan) radiolabeled with lutetium-177. Once lutetium Lu 177 vipivotide tetraxetan is bound to PSMA-expressing cells, the beta-minus emission from lutetium-177 delivers radiation to PSMA-expressing and surrounding cells, inducing DNA damage that leads to cell death. The exposure-efficacy relationships of lutetium Lu 177 vipivotide tetraxetan and the time course of the pharmacodynamic response are not fully characterized [9]. Lutetium-177 decays to a stable hafnium-177 with a physical half-life of 6.647 days by emitting beta-minus radiation with a maximum energy of 0.498 MeV (79%) and photonic radiation (γ) of 0.208 MeV (11%) and 0.113 MeV (6.4%).
Click to Show/Hide
|
||||
| Description |
A phase 1/2 study (NCT03042468) found that a single cycle of fractionated-dose of lutetium Lu 177 vipivotide tetraxetan [7.4-22 GBq on days 1 and 15 in the phase 1 dose-escalation cohort (n = 29); 22GBq on days 1 and 15 in the phase 2 cohort (n = 21); 27 patients treated at 22 GBq] was effective in patients with progressive mCRPC. A >50% PSA reduction was seen in 27 of 50 patients (54%); median PSA PFS was 5.6 months and median OS was 15.2 months.
Click to Show/Hide
|
||||
| Half life period | 41.6 h | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT03042468 | Clinical Status | Phase 1/2 | ||
| Clinical Description | The purpose of this study is to find the highest dose level of the study drug, 177Lu-PSMA-617 that can be given without severe side effects for advanced prostate cancer. | ||||
| Experiment 19 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
61.00%
|
|||
| Patients Enrolled |
56 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | On day 1 of each 6-week cycle | ||||
| Administration Dosage | 7.5 GBq | ||||
| MOA of PDC |
Lutetium Lu 177 vipivotide tetraxetan is a PSMA-binding ligand bound to a DOTA chelator (i.e., tetraxetan) radiolabeled with lutetium-177. Once lutetium Lu 177 vipivotide tetraxetan is bound to PSMA-expressing cells, the beta-minus emission from lutetium-177 delivers radiation to PSMA-expressing and surrounding cells, inducing DNA damage that leads to cell death. The exposure-efficacy relationships of lutetium Lu 177 vipivotide tetraxetan and the time course of the pharmacodynamic response are not fully characterized [9]. Lutetium-177 decays to a stable hafnium-177 with a physical half-life of 6.647 days by emitting beta-minus radiation with a maximum energy of 0.498 MeV (79%) and photonic radiation (γ) of 0.208 MeV (11%) and 0.113 MeV (6.4%).
Click to Show/Hide
|
||||
| Description |
A > 50% reduction in PSA after administration of up to 6 cycles of lutetium Lu 177 vipivotide tetraxetan plus idronoxil (a synthetic flavonoid derivative with radiosensitising properties) was seen in 34 of 56 (61%) patients with progressive mCRPC previously treated with AR pathway inhibition and taxanes in the phase 1/2 LuPin trial (ACTRN12618001073291). The median PSA PFS was 7.5 months and median OS was 19.7 months. Patients received lutetium Lu 177 vipivotide tetraxetan 7.5 GBq on day 1 of each 6-week cycle, with escalating doses of NOX66 on days 1-10 of a 6-week cycle.
Click to Show/Hide
|
||||
| Half life period | 41.6 h | ||||
| Related Clinical Trial | |||||
| NCT Number | ACTRN12618001073291 | Clinical Status | Phase 1/2 | ||
| Clinical Description | Background: Trials of lutetium prostate specific membrane antigen (PSMA) in men with metastatic castration-resistant prostate cancer (mCRPC) have demonstrated good safety and efficacy, but combination strategies may improve outcomes. Idronoxil is a synthetic flavonoid derivative with radiosensitising properties. 2. Objective: To evaluate the safety and activity of 177Lu PSMA 617 (LuPSMA-617) in combination with idronoxil suppositories (NOX66) in patients with end-stage mCRPC. 3. Design, setting, and participants: Thirty-two men with progressive mCRPC previously treated with taxane-based chemotherapy (91% treated with both docetaxel and cabazitaxel) and abiraterone and/or enzalutamide were enrolled in this phase I dose escalation study with phase II dose expansion. 4. Intervention: Screening with 68Ga PSMA and 18F-fludeoxyglucose positron emission tomography (PET)/computed tomography (CT) was performed. Men received up to six cycles of LuPSMA-617 (7.5 GBq) on day 1, with escalating doses of NOX66 on days 110 of a 6-wk cycle. Cohort 1 (n = 8) received 400 mg and cohort 2 (n = 24) 800 mg of NOX66. 5. Outcome measurements and statistical analysis: Adverse events (AEs), pain inventory scores, prostate-specific antigen (PSA) response, progression-free survival, and overall survival were evaluated. | ||||
| Experiment 20 Reporting the Activity Data of This PDC | [10] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
75.00%
|
|||
| Patients Enrolled |
37 patients with metastatic castration-resistant prostate cancer.
|
||||
| Description |
To interrogate potential synergy between 177Lu-PSMA-617 and pembrolizumab, the phase Ib/II PRINCE trial (NCT03658447) was initiated. Although the study is ongoing, an interim report details a ≥ 50% PSA decline rate of near 75% among 37 patients.
|
||||
| Related Clinical Trial | |||||
| NCT Number | NCT03658447 | Clinical Status | Phase 1/2 | ||
| Clinical Description | This investigator driven study will examine the safety, tolerability and efficacy of the combination of 177Lutetium-PSMA (177Lu-PSMA) and pembrolizumab in patients with metastatic Castration Resistant Prostate Cancer (mCRPC). 177Lu-PSMA is a compound that binds to the extra-cellular domain of the prostate-specific membrane antigen. Pembrolizumab is an antibody targeted against anti-programmed cell death 1 (PD-1).This is a single arm study where all patients will be treated with 177Lu-PSMA for upto 6 doses and pembrolizumab for upto 35 cycles. | ||||
| Experiment 21 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
46.00%
|
|||
| Patients Enrolled |
581 patients with metastatic castration-resistant prostate cancer.
|
||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
The VISION trial was an international open-label phase 3 trial that assigned 581 mCRPC patients who previously received a novel hormonal agent and chemotherapy to either the treatment group (receiving 177Lu-PSMA-617 and standard of care) or control group (standard of care alone). Primary end points were progression-free survival, median overall survival, and median follow-up. Median progression-free survival was 8.7 months in the 177Lu-PSMA-617 group, as compared with 3.4 months in the control group (HR for progression or death, 0.40; 99.2% confidence interval, 0.29 to 0.57; P < 0.001). Median overall survival was 15.3 months in the 177Lu-PSMA-617 group, as compared with 11.3 months in the control group (hazard ratio for death, 0.62; 95% CI, 0.52 to 0.74; P < 0.001). The median follow-up was 20.3 months (95% CI, 19.8 to 21.0) in the 177Lu-PSMA-617 group and 19.8 months (95% CI, 18.3 to 20.8) in the control group. Secondary end points included median time to the first symptomatic skeletal event or death and PSA level. The median time to the first symptomatic skeletal event or death was 11.5 months in the 177Lu-PSMA-617 group, as compared with 6.8 months in the control group (P < 0.001). The proportions of patients with confirmed decreases in the PSA level of at least 50% and 80% from baseline were higher in the 177Lu-PSMA-617 group than in the control group.
Click to Show/Hide
|
||||
| Experiment 22 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
37.50%
|
|||
| Patients Enrolled |
40 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | Up to 4 cycles (median number of 3 cycles, range 2-5) every eight to twelve weeks | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
A phase II study followed forty patients with PET/CT-68Ga-PSMA positive mCRPC treated with 177Lu PSMA-617. 177Lu PSMA-617 was given for up to four cycles (median number of three cycles, range 2-5) every eight to twelve weeks. With a median follow-up of 15.5 months (range 6-22 ), 37.5% of patients had a greater than 50% PSA decline and 50% had a PSA decline greater than 30%. The median PFS was 7.5 months (95% CI: 4.8-10.5) and median OS was 12.4 months (95% CI 7.4-20.3 months).
Click to Show/Hide
|
||||
| Experiment 23 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
50.00%
|
|||
| Patients Enrolled |
35 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | Up to 4 cycles every 8 weeks | ||||
| Administration Dosage | 6.0-7.4 GBq/cycle | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
A randomized, parallel group, open label, and non-inferiority phase II trial conducted between 2019 and 2021 studied a group of thirty five chemo-naive patients with mCPRC and high expressing PSMA lesions on 68Ga-PSMA-11 on PET/CT. Patients were randomized in 1:1 ratio to either 177Lu PSMA-617 (6.0-7.4 GBq/cycle, every 8 weeks, up to 4 cycles) or docetaxel (75 mg/m2/cycle, every 3 weeks, for up to 10 cycles), with fifteen and twenty patients in each group, respectively. The primary endpoint was best PSA response rate (PSA-RR), which is defined as a ≥ 50% decline in PSA from baseline. The 177Lu PSMA-617 arm PSA-RR was 60% versus 40% in docetaxel group with a difference in PSA-RR of 20% (95% CI: 1-47, p = 0.025) and met the pre-specified criterion for non-inferiority which was defined as margin of 15% decline in PSA-RR. The PFS rate for 177Lu PSMA-617 was 30% versus 20% for docetaxel (95% CI: 18-38, p = 0.5). The number of treatment-related adverse events grade 3 or higher occurred less in the 177Lu PSMA-617 arm than the docetaxel arm (30% versus 50% respectively, p = 0.2).
Click to Show/Hide
|
||||
| Experiment 24 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
57.00%
|
|||
| Patients Enrolled |
30 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 4 cycles | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
Another single-arm, single-center, phase 2 trial recruited thirty men with mCRPC and progressive disease after receiving standard treatments including taxane-based chemotherapy and second-generation anti-androgen treatment (abiraterone, enzalutamide, or both). They were administered four cycles of 177Lu-PSMA-617. The primary end points included PSA level, imaging response using bone scan, and PET/CT and quality of life. The PSA decline of greater than or equal to 50% was achieved in 57% of patients. Imaging response using PSMA PET showed a complete response in 10% of patients, a partial response in 30% of patients, and progressive disease in 27% of patients. Cognitive functioning, insomnia, and pain, which were measured using the EORTC-QLQ30 (European Organization for the Research and Treatment of Cancer Quality of Life Questionnaire) and BPI (brief pain inventory) scoring tools showed improvement during treatment compared to baseline, thus indicating improved quality of life.
Click to Show/Hide
|
||||
| Experiment 25 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
64.00%
|
|||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
The Thera-P trial was a phase II prospective multicenter trial looking at those with mCPRC who progressed after docetaxel chemotherapy and were randomly assigned to 177Lu PSMA-617 or cabazitaxel. Initial reported results found that those who were treated with 177Lu PSMA-617 treatment led to improvement in PSA response rate (66% vs 37%), RECIST response rate (49% vs 24%), PFS (HR 0.63), less G3-G4 toxicities (33% vs 53%), and overall better patient reported outcomes.
Click to Show/Hide
|
||||
| Experiment 26 Reporting the Activity Data of This PDC | [11] | ||||
| Indication | ATM-mutated metastatic castration resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
10.60-69.00%
|
|||
| Patients Enrolled |
Metastatic castration-resistant prostate cancer patients.
|
||||
| Administration Time | 4-6 cycles at 6-12 weekly intervals | ||||
| Administration Dosage | 2-8 GBq | ||||
| MOA of PDC |
177Lu-PSMA therapy is a promising treatment alternative in patients with mCRPC, with good clinical efficacy, even in heavily pretreated patients with multiple lines of systemic therapy. Additionally, the available data regarding 177Lu-PSMA therapy revealed that this type of therapy is safe, with a low toxicity profile. There is also some preliminary evidence that 177Lu-PSMA therapy is more effective, if used prior to other systemic therapies, earlier during the disease course. Consequently, this treatment alternative may shift its place from the last treatment step of mCRPC to one of the initial therapy steps for PCa, probably combined with other systemic treatment options in the future.
Click to Show/Hide
|
||||
| Description |
Although there are some different approaches regarding the use of 177Lu-PSMA therapy in different countries, this type of therapy is generally safe, with a low toxicity profile. From the oncological point of view, a PSA (prostate specific antigen) decline of ≥50% was seen in 10.6-69% of patients with mCRPC; whereas progression-free survival (PFS) was reported to be 3-13.7 months in different studies.
Click to Show/Hide
|
||||
| Experiment 27 Reporting the Activity Data of This PDC | [12] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
20.00%
|
|||
| Patients Enrolled |
61 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | Median 4 (iqr: 2-6) cycles | ||||
| Administration Dosage | Median 800 (IQR: 470-1150) mCi | ||||
| MOA of PDC |
In conclusion, the current study was the first to demonstrate that pretreatment NLR, MLR, PLR and SII are powerful independent prognostic indices predicting survival in patients with mCRPC receiving 177Lu-PSMA-617 therapy. A large-scale prospective study is warranted to confirm the preliminary results obtained in this study.
|
||||
| Description |
Mean follow-up time was 53.2±24 months. While there were 61 patients at the baseline, 46 (75%) patients were able to complete the fourth cycle, and 18 (30%) patients were able to complete the eighth cycle. Median 4 (IQR: 2-6) cycles and 800 (IQR: 470-1150) mCi 177Lu-PSMA-617 were applied. During the 177Lu-PSMA-617 therapy period, androgen receptor signaling inhibitor was continued in 8 (13%) patients and chemotherapy was continued in 3 (5%) patients. According to the PCWG3 PSA response patterns, 18 (30%) patients had fitted into pattern 1 (PSA reduction of 50% or more from baseline and sustained), 12 (20%) patients into pattern 2 (PSA decrease of more than 50% followed by a modest rise), and 31 (51%) patients into pattern 3 (PSA progression of more than 25%). No significant difference was found between PSA patterns according to baseline inflammation indices (P values for NLR, dNLR, MLR, PLR, SII, PIV were.298,.105,.137,.774,.727,.944, respectively).
Click to Show/Hide
|
||||
| Experiment 28 Reporting the Activity Data of This PDC | [12] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
30.00%
|
|||
| Patients Enrolled |
61 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | Median 4 (iqr: 2-6) cycles | ||||
| Administration Dosage | Median 800 (IQR: 470-1150) mCi | ||||
| MOA of PDC |
In conclusion, the current study was the first to demonstrate that pretreatment NLR, MLR, PLR and SII are powerful independent prognostic indices predicting survival in patients with mCRPC receiving 177Lu-PSMA-617 therapy. A large-scale prospective study is warranted to confirm the preliminary results obtained in this study.
|
||||
| Description |
Mean follow-up time was 53.2±24 months. While there were 61 patients at the baseline, 46 (75%) patients were able to complete the fourth cycle, and 18 (30%) patients were able to complete the eighth cycle. Median 4 (IQR: 2-6) cycles and 800 (IQR: 470-1150) mCi 177Lu-PSMA-617 were applied. During the 177Lu-PSMA-617 therapy period, androgen receptor signaling inhibitor was continued in 8 (13%) patients and chemotherapy was continued in 3 (5%) patients. According to the PCWG3 PSA response patterns, 18 (30%) patients had fitted into pattern 1 (PSA reduction of 50% or more from baseline and sustained), 12 (20%) patients into pattern 2 (PSA decrease of more than 50% followed by a modest rise), and 31 (51%) patients into pattern 3 (PSA progression of more than 25%). No significant difference was found between PSA patterns according to baseline inflammation indices (P values for NLR, dNLR, MLR, PLR, SII, PIV were.298,.105,.137,.774,.727,.944, respectively).
Click to Show/Hide
|
||||
| Experiment 29 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
31.00%
|
|||
| Patients Enrolled |
82 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 1 dose | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
One study retrospectively analyzed 82 mCRPC patients who received a single dose of Lu-PSMA. Tolerability and response to treatment were assessed using hematologic parameters, renal scintigraphy, clinical data, and prostate-specific antigen (PSA) levels. A PSA decline from baseline was noted in 64% patients with 31% of patients having a greater than 50% decline, while 47% patients had stable disease with a 25-50% decrease in PSA levels. Only 25% of patients showed an increase in PSA levels indicating disease progression, and 7% of patients died due to extensive disease.
Click to Show/Hide
|
||||
| Experiment 30 Reporting the Activity Data of This PDC | [13] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
32.00%
|
|||
| Patients Enrolled |
22 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | First treatment cycle | ||||
| Description |
After the first treatment cycle, only 58% of the patients (n = 19) showed a decrease in serum PSA, and only 32% showed a decrease of more than 50%. After all treatment cycles were completed, 65% of the patients responded with a PSA drop greater than 50%. An even higher group of 84% responded with a general decrease in PSA levels. The highest reduction of PSA levels was observed from 139.1 to 0.24 ug/L (99.83%). Before PSMA RLT treatment, the mean serum PSA level was 258.12 ug/L (range, 0.42-3305.00 ug/L) and after 2 to 9 treatment cycles, it decreased to 79.61 ug/L (range, 0.24-869.10 ug/L).
Click to Show/Hide
|
||||
| Experiment 31 Reporting the Activity Data of This PDC | [14] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
32.00%
|
|||
| Patients Enrolled |
28 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 1 dose | ||||
| MOA of PDC |
Radiopharmaceuticals have been used in prostate cancer for decades with known efficacy in palliation of bone metastasis. The FDA approval of the most recent radiopharmaceutical, 177Lu-PSMA-617, shows a clear overall survival benefit compared to the best SOC. Current studies are ongoing to evaluate the effectiveness of 177Lu-PSMA-617 in earlier lines of therapy, such as after only 1 line of therapy with an ARPI as in the PSMAfore study, or in mCSPC in combination with ADT and an ARPI as in the PSMAddition study. Studies are also ongoing with 177Lu-PSMA-617 in combination with other treatments which may produce a synergistic effect. As described, there are many clinical trials ongoing that are modifying the 177Lu-PSMA-617 to possibly achieve improved results. Studies are also ongoing looking at swapping the 177Lu for another radioactive agent, such as 225Ac (an alpha emitter) which may have benefits over the beta-emitting 177Lu. Other studies are looking at J591, a monoclonal antibody to PSMA which has unique differences compared to small-molecule PSMA binders. Overall, PSMA-based radioligand therapy has been shown to be an effective and life-prolonging therapy and should be considered a treatment option for selected men with mCRPC. As described, there are many ongoing studies further evaluating PSMA radioligand therapy in Australia, South Africa, Europe, and the United States, representing a truly global effort to improve prostate cancer care.
Click to Show/Hide
|
||||
| Description |
A subsequent retrospective study, the first evaluating multiple administrations of 177Lu-PSMA-617, was reported by the same group. The authors reviewed 28 consecutive patients who received 50 infusions of 177Lu-PSMA-617 between 2014 and 2015. In their report, a PSA decline was noted in 59% and 75% of patients after 1 and 2 therapies, respectively, and a PSA decline of 50% or greater occurred in 32% and 50%, respectively. The estimated median survival was 29.4 weeks compared to 19.7 weeks in the historical best supportive care group which was statistically significant (HR 44; 95% CI 0.20-0.95; P=.031). Authors of the study also noted no significant changes in hematologic or renal parameters
Click to Show/Hide
|
||||
| Experiment 32 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
32.00%
|
|||
| Patients Enrolled |
28 patients with metastatic castration-resistant prostate cancer.
|
||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
A retrospective analysis studied 28 patients with mCRPC who were treated with 177Lu-PSMA-617 [Citation47]. The estimated median survival was 29.4 weeks, significantly longer than survival in the supportive care group (HR, 0.44; 95% confidence interval, 0.20-0.95]; P = 0.031). Results of the study noted any PSA decline in 59% of patients after one cycle and 75% of patients after two cycles of treatment, while there was a noted PSA decline of 50% or greater in 32% of patients after one cycle of treatment and in 50% of patients after two cycles of treatment. Although this study found a 50% or greater PSA decline in majority of treated patients, 83% of patients reported a stable or improved quality of life after treatment.
Click to Show/Hide
|
||||
| Experiment 33 Reporting the Activity Data of This PDC | [15] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
33.00%
|
|||
| Patients Enrolled |
Patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 351 cycles | ||||
| Description |
Any PSA decline occurred in 70 (67%) and a PSA decline ≥50% in 34 (33%) of patients after the first cycle.
|
||||
| Experiment 34 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
33.00%
|
|||
| Patients Enrolled |
104 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | A median of 3 cycles (1-8 cycles) | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
A total of 104 patients with mCRPC who were previously treated with one line of chemotherapy (docetaxel and/or cabazitaxel) and at least one of antihormonal therapies (enzalutamide and/or abiraterone) were retrospectively studied after being treated with 177Lu-PSMA-617 RLT. A median of three cycles were administered (1-8 cycles). Results of the study noted a median overall survival of 56.0 weeks (95% CI: 50.5-61.5) and PSA decline >50% in 33% patients after receiving first cycle of treatment.
Click to Show/Hide
|
||||
| Experiment 35 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
33.00%
|
|||
| Patients Enrolled |
30 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 1 cycles | ||||
| Administration Dosage | 180 mCi | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
A study sought to analyze the prognostic significance of monitoring PSA levels during 177Lu-PSMA-617 treatment. The study included thirty mCPRC patients who had baseline Ga-68 PSMA PET/CT prior to undergoing 177Lu-PSMA-617 treatment. Patients were treated with a fixed dose of 180 mCi of 177Lu-PSMA-617 every six to eight weeks. A total of 171 cycles of treatment were administered with a median of four cycles per patients (range 3-7). A PSA decline greater than 50% was seen in 33% of patients after one cycle of treatment and increased to 43% of patients at the conclusion of the last cycle of treatment. Of the 20 patients who did not have a 50% reduction in PSA levels after the first cycle, four of these patients eventually had a PSA decline of greater than 50% after the conclusion of the last cycle of treatment. The median OS was statistically significant in those who had a greater than 50% decline in PSA level 21 ± 10 (95% CI: 1.2-40.7) compared to those who did not 8.0 ± 2.6 (95% CI: 2.7-13.2) months (p = 0.012). Any PSA decline was seen in 50% of patients after just one cycle of treatment and remained stable at 46% of patients at the conclusion of treatment, but did not have a statistically significant impact on median OS; however it was significant for any PSA decline after the last cycle of treatment (13 ± 1, 95% CI: 10.9-15 months for responders versus 6.0 ± 1.9, 95% CI: 2.2-9.7 months for non-responders).
Click to Show/Hide
|
||||
| Experiment 36 Reporting the Activity Data of This PDC | [16] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
35.00%
|
|||
| Patients Enrolled |
Patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | Every 6weeks | ||||
| Administration Dosage | 7.5 GBq | ||||
| Description |
There was no significant difference comparing the rate of > 50% PSA decline or best PSA response between the 6.0 GBq and 7.5 GBq group (35% vs. 54%, p = 0.065; and - 40.2% vs. - 57.8%, p = 0.329). The median estimated survival and PSA-PFS did not significantly differ between the 6.0 GBq and 7.5 GBq groups as well (11.3 vs. 12.7 months, p = 0.384; and 9.5 vs. 12.3 months, p = 0.258).
Click to Show/Hide
|
||||
| Experiment 37 Reporting the Activity Data of This PDC | [2] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
35.00%
|
|||
| Patients Enrolled |
Patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | At least one course of [177lu]-psma-617 | ||||
| Administration Dosage | 6-7 GBq | ||||
| MOA of PDC |
[177Lu]-PSMA-617 is a novel treatment modality for prostate cancer, utilizing the tumors expression of PSMA as a target to allow for the administration of mixed beta-gamma radiation directly to the site of active metastases.
|
||||
| Description |
A subjective clinical benefit, based on the clinical evaluation by the treating oncologist, was observed in 28 patients (52%). The first PSA was measured following a median of 1.2 months from the start of treatment (range 0.4-3.7 months). PSA nadir was achieved within a median of 1.4 months (range 0.4-13.4). A maximal PSA decline of at least 20% was observed in 26 patients (50%), a maximal PSA decline of at least 50% was observed in 18 patients (35%), and a maximal PSA decline of at least 90% was observed in 7 patients (16%). Thirty patients (58%) had any PSA decline (PSA decline greater than 10%) upon their first PSA assessment.
Click to Show/Hide
|
||||
| Experiment 38 Reporting the Activity Data of This PDC | [17] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
35.90%
|
|||
| Patients Enrolled |
508 patients with metastatic castration-resistant prostate cancer.
|
||||
| Description |
A total of 12 studies involving 508 cases of mCRPC were included in this analysis. After the first cycle of treatment, the pooled rate of PSA decline was 69.30% (95% CI: 65.40%73.30%), and that of >50% PSA decline was 35.90% (95% CI: 31.80%40.00%). No significant adverse events were reported in any of the studies.
|
||||
| Experiment 39 Reporting the Activity Data of This PDC | [18] | ||||
| Indication | ATM-mutated metastatic castration resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
36.00%
|
|||
| Patients Enrolled |
14 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 4 cycles | ||||
| Administration Dosage | Mean 7.0 GBq | ||||
| MOA of PDC |
PSMA TRT involves conjugating radionuclides to antibodies and small molecule-ligands directed against PSMA. The most common radionuclide utilized to date is Lutetium-177, a beta-emitter with a mean path-length of 0.7 mm and maximum of 1.8 mm. Gamma-ray emission allows for concurrent single photon emission computed tomography (SPECT). Actinium-225 has been the most common alpha-emitter utilized. Alpha-emitters are thousands of times more potent and can induce double-stranded DNA breaks more difficult to repair, but mean path-length is much shorter than beta-emitters (under 0.01 mm).
Click to Show/Hide
|
||||
| Experiment 40 Reporting the Activity Data of This PDC | [19] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
36.00%
|
|||
| Patients Enrolled |
25 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | A median of four (iqr: 2-6) cycles every 6-8 weeks | ||||
| Administration Dosage | Mean of 7.7 ± 1.4 GBq/cycle | ||||
| MOA of PDC |
The response to radioligand therapy with 177Lu-PSMA-617 seems to be independent of the presence of early-onset prostate cancer (EOPC); however, the less favorable survival outcome observed in our study may indicate a more aggressive disease course. Expectedly, the safety of LuPSMA-RLT does not seem to be compromised in metastasized castration-resistant EOPC patients. Comparative studies on age at diagnosis of prostate cancer and the patients outcome after LuPSMA-RLT are needed.
Click to Show/Hide
|
||||
| Description |
An initial PSA reduction (≥ 50%) was observed in 9/25 (36%) of patients without being significantly associated with OS (p = 0.601). PSA response (PSA decline ≥50% at 12 weeks) was observed in 12/25 (48%) of patients and significantly associated with longer OS (16.0 months, 95% CI 7.4-24.6 vs. 4.0 months, 95% CI 1.1-6.9, p = 0.002).
|
||||
| Experiment 41 Reporting the Activity Data of This PDC | [20] | ||||
| Indication | Advanced prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
37.50%
|
|||
| Patients Enrolled |
Patients with advanced prostate cancer.
|
||||
| Administration Time | 2 cycles | ||||
| Description |
A maximum PSA decrease of 50% was achieved in 3 patients (37.5%).
|
||||
| Experiment 42 Reporting the Activity Data of This PDC | [18] | ||||
| Indication | ATM-mutated metastatic castration resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
38.00%
|
|||
| Patients Enrolled |
64 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 4 cycles | ||||
| Administration Dosage | 6.0/7.4 GBq | ||||
| MOA of PDC |
PSMA TRT involves conjugating radionuclides to antibodies and small molecule-ligands directed against PSMA. The most common radionuclide utilized to date is Lutetium-177, a beta-emitter with a mean path-length of 0.7 mm and maximum of 1.8 mm. Gamma-ray emission allows for concurrent single photon emission computed tomography (SPECT). Actinium-225 has been the most common alpha-emitter utilized. Alpha-emitters are thousands of times more potent and can induce double-stranded DNA breaks more difficult to repair, but mean path-length is much shorter than beta-emitters (under 0.01 mm).
Click to Show/Hide
|
||||
| Experiment 43 Reporting the Activity Data of This PDC | [21] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
40.00%
|
|||
| Patients Enrolled |
Patients with metastatic castration-resistant prostate cancer; taxane chemotherapy pretreated.
|
||||
| Experiment 44 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
40.00%
|
|||
| Patients Enrolled |
145 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 1 cycles | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
A 2014-2015 retrospective multi-institutional study looked to evaluate the efficacy and safety of 177Lu-PSMA-617 in a larger population of patients. 145 patients with a median age of 73 years (range 43-88) with mCRPC were treated with a range of 1-4 cycles of treatment. Median follow-up time was sixteen weeks (range 2-30). The primary endpoint of the study was biochemical response, which was defined as a decline in PSA greater than 50% from baseline and secondary endpoints included toxicity. A total of 248 cycles of treatment were carried out in 145 patients with the overall biochemical response rate of 45% after conclusion of all treatment and 40% of patients becoming responders after only one cycle of treatment.
Click to Show/Hide
|
||||
| Experiment 45 Reporting the Activity Data of This PDC | [22] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
41.50%
|
|||
| Patients Enrolled |
416 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 3 cycles | ||||
| MOA of PDC |
The PSMA molecule acts as a target for theranostics in detecting and treating prostatic lesions. This ultimately promotes the concept of precision and personalized medicine. Several published articles showed favorable outcomes of Lu-PSMA-PRLT in mCRPC patients, which quickly translated into routine clinical practices with real effectiveness, a low toxicity profile, and documentation of the risk-benefit of PRLT. Nevertheless, many questions related to PRLT remain unresolved such as the sequencing of PRLT with ARTA or taxane-based chemotherapy, re-challenge therapy, combined therapy, alpha therapy in mCRPC patients, and early treatment of PRLT in mHNPC patients. To solve these questions, several clinical trials are currently under way, and the results of these trials will be helpful in deciding treatment strategies for prostate cancer patients.
Click to Show/Hide
|
||||
| Description |
Since initial retrospective studies had a limited number of patients and a heterogeneous population, the WARMTH (World Association of Radiopharmaceutical and Molecular Therapy) planned a multi-center retrospective study to evaluate response rate, OS, and the impact of prior therapies on OS in more than 300 mCRPC patients treated with 177Lu-PSMA-617. The study included 416 mCRPC patients who received a total of 1493 cycles of 177Lu-PSMA-617, with a median of 3 cycles per patient. Post-177Lu-PSMA-617, serum PSA decline was seen in 282 (71.8%) patients, of whom 163 (41.5%) showed a serum PSA decline of ≥50%, whereas 111 patients (28.2%) showed an increase in serum PSA levels. A median OS of 11.1 months (95% CI 9.7-12.5 months) was observed. Prior chemotherapy, the presence of bone and liver metastases, and poor ECOG status were significant adverse prognosticators for survival in both univariate and multivariate analyses. No imaging response evaluation and no determination of PFS after 177Lu-PSMA-617 were major limitations for this study.
Click to Show/Hide
|
||||
| Experiment 46 Reporting the Activity Data of This PDC | [4] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
42.00%
|
|||
| Patients Enrolled |
19 patients with metastatic castration-resistant prostate cancer, median age 68.8 years (range: 56.9 - 83.3).
|
||||
| Administration Time | Every 6-8 weeks | ||||
| Administration Dosage | 7.64 MBq per cycle | ||||
| Description |
Patients presented with bone, lymph node, and visceral metastases (89%, 68%, and 21%, respectively). All patients were pretreated with docetaxel, either abiraterone or enzalutamide, or both. Biochemical response in terms of PSA decline ≥50 or ≥30% was observed in 42% and 63%, respectively. There were significant correlations between PSA and PSMA mRNA expression, as well as tumor volumes (both MTV and TTV), AR-FL and AR-V7 mRNA expression. However, there was no correlation with response to PSMA treatment.
Click to Show/Hide
|
||||
| Experiment 47 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
43.00%
|
|||
| Patients Enrolled |
30 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Dosage | 180 mCi | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
A study sought to analyze the prognostic significance of monitoring PSA levels during 177Lu-PSMA-617 treatment. The study included thirty mCPRC patients who had baseline Ga-68 PSMA PET/CT prior to undergoing 177Lu-PSMA-617 treatment. Patients were treated with a fixed dose of 180 mCi of 177Lu-PSMA-617 every six to eight weeks. A total of 171 cycles of treatment were administered with a median of four cycles per patients (range 3-7). A PSA decline greater than 50% was seen in 33% of patients after one cycle of treatment and increased to 43% of patients at the conclusion of the last cycle of treatment. Of the 20 patients who did not have a 50% reduction in PSA levels after the first cycle, four of these patients eventually had a PSA decline of greater than 50% after the conclusion of the last cycle of treatment. The median OS was statistically significant in those who had a greater than 50% decline in PSA level 21 ± 10 (95% CI: 1.2-40.7) compared to those who did not 8.0 ± 2.6 (95% CI: 2.7-13.2) months (p = 0.012). Any PSA decline was seen in 50% of patients after just one cycle of treatment and remained stable at 46% of patients at the conclusion of treatment, but did not have a statistically significant impact on median OS; however it was significant for any PSA decline after the last cycle of treatment (13 ± 1, 95% CI: 10.9-15 months for responders versus 6.0 ± 1.9, 95% CI: 2.2-9.7 months for non-responders).
Click to Show/Hide
|
||||
| Experiment 48 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
43.33%
|
|||
| Patients Enrolled |
30 patients with PSMA-positive prostate tumor.
|
||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
177Lu-PSMA-617 was offered to thirty patients with PSMA-positive prostate tumor. Treatment efficacy was retrospectively assessed by PSA levels with 70% of patients demonstrating a decrease in PSA levels. 18 patients were noted to have PSA decline greater than 25%, while 13 patients had a decline greater than 50%. Six of these patients were restaged using PSMA PET/CT (positron emission tomography/computed tomography), and all six patients had a response rate of more than 50% in SUVmax (maximum standardized uptake value) of the tumor.
Click to Show/Hide
|
||||
| Experiment 49 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
44.00%
|
|||
| Patients Enrolled |
52 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 1 cycles | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
An additional retrospective study of 52 mCRPC patients (mean age of 70, range 48-87 years) evaluated the PSA response of those treated with 177Lu-PSMA-617 after one to three cycles of radioligand therapy (RLT) every eight weeks. A total of 190 cycles of RLT (3-6 cycles per patient) were given and 80% of patients showed a decline after the first cycle with 44% of patients showing a PSA response of more than 50%. After the third cycle, 73% of patients showed any PSA decline. The median OS was 60 weeks for all patients and median OS was statistically longer for those who responded with decline in PSA after first cycle compared to those without (68 vs 33 weeks).
Click to Show/Hide
|
||||
| Experiment 50 Reporting the Activity Data of This PDC | [22], [23] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
44.00%
|
|||
| Patients Enrolled |
Twelve studies including 669 metastatic castration-resistant prostate cancer patients reported <sup>177</sup>Lu-PSMA radioligand therapy(RLT). <sup>177</sup>Lu-PSMA RLT caused a best decline of PSA ≥50% twice as often as the third-line treatment (mean frequency 44% versus 22%, p=0.0002, t-test).
|
||||
| MOA of PDC |
The PSMA molecule acts as a target for theranostics in detecting and treating prostatic lesions. This ultimately promotes the concept of precision and personalized medicine. Several published articles showed favorable outcomes of Lu-PSMA-PRLT in mCRPC patients, which quickly translated into routine clinical practices with real effectiveness, a low toxicity profile, and documentation of the risk-benefit of PRLT. Nevertheless, many questions related to PRLT remain unresolved such as the sequencing of PRLT with ARTA or taxane-based chemotherapy, re-challenge therapy, combined therapy, alpha therapy in mCRPC patients, and early treatment of PRLT in mHNPC patients. To solve these questions, several clinical trials are currently under way, and the results of these trials will be helpful in deciding treatment strategies for prostate cancer patients.
Click to Show/Hide
|
||||
| Description |
A systematic review on the comparison of 177Lu-PSMA-PRLT with third-line treatments such as abiraterone, enzalutamide, and cabazitaxel was published by Von Eyben et al. A significant difference of PSA response was seen between the two groups (a PSA decline of ≥50% in 44% of patients in Lu-PSMA-PRLT group versus only 22% of patients in third-line treatment group). The authors mentioned that, despite variations in doses and number of cycles, 177Lu-PSMA-PRLT group showed a favorable response rate as compared to the third-line treatment group, and they also mentioned more side effects and discontinuation of third-line treatment as compared to 177Lu-PSMA- PRLT group.
Click to Show/Hide
|
||||
| Experiment 51 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
44.90%
|
|||
| Patients Enrolled |
50 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | A median of 3 cycles | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
Fifty patients were studied prospectively with PSMA-avid prostate cancer metastases who underwent a median of three cycles (range 1-4) of 177Lu PSMA-617 therapy. Nine were deemed 177Lu PSMA-617 refractory prior to death with a total of twelve deaths in the study. A PSA decline was noted in 23 patients, with 11 patients having a PSA decline of ≥50% after the first cycle of treatment. 12 patients had a PSA decline of <50% ranging from 11.3 to 43.5%. The remaining 23 patients experienced a PSA increase after the first 177Lu PSMA-617 cycle (range 19.7-100%).
Click to Show/Hide
|
||||
| Experiment 52 Reporting the Activity Data of This PDC | [24] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
45.00%
|
|||
| Patients Enrolled |
Patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 2-cycles of 177lu-psma-rlt | ||||
| Administration Dosage | 3.5-7.5 GBq | ||||
| MOA of PDC |
Entwickelt im Deutschen Krebsforschungszentrum in Heidelberg, ist PSMA-617 der weltweit weiterhin am hufigsten eingesetzte Ligand zur Behandlung von Patienten mit metastasiertem Prostatakarzinom. (Developed at the German Cancer Research Center in Heidelberg, PSMA-617 remains the most commonly used ligand worldwide for treating patients with metastatic prostate cancer.)
Click to Show/Hide
|
||||
| Description |
Im Median erhielten die Patienten 2 Zyklen der 177Lu-PSMA-RLT. Die Mehrheit der Patienten erhielt 3,5-7,5 GBq (im Median 6,0 GBq) Aktivitt pro Zyklus. ber den gesamten Beobachtungszeitraum zeigten 45 % der Patienten eine PSA50. Irgendein PSA-Abfall trat bei 60 % der Patienten auf. (The patients received a median of 2 cycles of 177Lu-PSMA-RLT. The majority of the patients received 3.5-7.5 GBq (a median of 6.0 GBq) of activity per cycle. Throughout the entire observation period, 45% of the patients exhibited a PSA50. Some decrease in PSA levels occurred in 60% of the patients.)
Click to Show/Hide
|
||||
| Half life period | 6.7 day | ||||
| Experiment 53 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
45.00%
|
|||
| Patients Enrolled |
145 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 1-4 cycles | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
A 2014-2015 retrospective multi-institutional study looked to evaluate the efficacy and safety of 177Lu-PSMA-617 in a larger population of patients. 145 patients with a median age of 73 years (range 43-88) with mCRPC were treated with a range of 1-4 cycles of treatment. Median follow-up time was sixteen weeks (range 2-30). The primary endpoint of the study was biochemical response, which was defined as a decline in PSA greater than 50% from baseline and secondary endpoints included toxicity. A total of 248 cycles of treatment were carried out in 145 patients with the overall biochemical response rate of 45% after conclusion of all treatment and 40% of patients becoming responders after only one cycle of treatment.
Click to Show/Hide
|
||||
| Experiment 54 Reporting the Activity Data of This PDC | [22] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
45.00%
|
|||
| Patients Enrolled |
145 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 1-4 cycles | ||||
| Administration Dosage | 2-8 GBq/cycle | ||||
| MOA of PDC |
The PSMA molecule acts as a target for theranostics in detecting and treating prostatic lesions. This ultimately promotes the concept of precision and personalized medicine. Several published articles showed favorable outcomes of Lu-PSMA-PRLT in mCRPC patients, which quickly translated into routine clinical practices with real effectiveness, a low toxicity profile, and documentation of the risk-benefit of PRLT. Nevertheless, many questions related to PRLT remain unresolved such as the sequencing of PRLT with ARTA or taxane-based chemotherapy, re-challenge therapy, combined therapy, alpha therapy in mCRPC patients, and early treatment of PRLT in mHNPC patients. To solve these questions, several clinical trials are currently under way, and the results of these trials will be helpful in deciding treatment strategies for prostate cancer patients.
Click to Show/Hide
|
||||
| Description |
The first major multi-center retrospective study on 177Lu-PSMA-617 was published by Rahbar et al., reporting 145 patients with mCRPC who progressed after second-line systemic therapies. The overall response rate in terms of serum PSA decline >50% was seen in 45% of patients after all 177Lu-PSMA-617 cycles. On imaging, 21 (45%) patients and 13 (28%) patients had PR and SD, respectively. There was grade 3-4 toxicity in 18 patients (13%), which included severe anemia, thrombocytopenia, and leukopenia. They found elevated alkaline phosphatase and visceral metastases as negative predictors of response to 177Lu-PSMA-617. A major drawback of this study was the variable cycles and doses of 177Lu-PSMA-617 given to patients
Click to Show/Hide
|
||||
| Experiment 55 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
45.40%
|
|||
| Patients Enrolled |
14 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 2 or more cycles | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
A prospective trial investigated the efficacy and toxicity of 177Lu-PSMA-617 in fourteen patients with mCRPC. Biochemical response using PSA level and clinical symptoms were evaluated after two or more cycles of treatment. PSA levels declined in 11 out of 14 (78.6%) patients, with greater than 50% decline in 45.4% patients over a period of 8 weeks. Progressive disease, defined by a PSA increase of 25% or greater occurred in 21.4% patients. The mean serum alkaline phosphatase level declined from 569.5 U/L to 498.4 U/L, but this was not statistically significant (P = 0.17). At baseline, nine patients with bone metastases reported skeletal bone pain. Eight of these patients showed improvement in pain after treatment.
Click to Show/Hide
|
||||
| Experiment 56 Reporting the Activity Data of This PDC | [22] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
45.50%
|
|||
| Patients Enrolled |
90 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 1-7 cycles | ||||
| Administration Dosage | 3.7-8 GBq/cycle | ||||
| MOA of PDC |
The PSMA molecule acts as a target for theranostics in detecting and treating prostatic lesions. This ultimately promotes the concept of precision and personalized medicine. Several published articles showed favorable outcomes of Lu-PSMA-PRLT in mCRPC patients, which quickly translated into routine clinical practices with real effectiveness, a low toxicity profile, and documentation of the risk-benefit of PRLT. Nevertheless, many questions related to PRLT remain unresolved such as the sequencing of PRLT with ARTA or taxane-based chemotherapy, re-challenge therapy, combined therapy, alpha therapy in mCRPC patients, and early treatment of PRLT in mHNPC patients. To solve these questions, several clinical trials are currently under way, and the results of these trials will be helpful in deciding treatment strategies for prostate cancer patients.
Click to Show/Hide
|
||||
| Description |
A favorable response rate (PSA and objective response) and safe profile of 177Lu-PSMA-617 were demonstrated in this study, leading to greater use of Lu-PSMA-PRLT in clinical practices. Similarly, Yadav et al. reported favorable outcomes of 177Lu-PSMA-617 in a prospective, single-arm, single-center study in 90 mCRPC patients.
|
||||
| Experiment 57 Reporting the Activity Data of This PDC | [25] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
46.00%
|
|||
| Patients Enrolled |
Patients with metastatic castration-resistant prostate cance treated with LuPSMA between December 2014 and October 2018.
|
||||
| Administration Time | 3 cycles | ||||
| Administration Dosage | 19.3 GBq (cumulated activity) | ||||
| Experiment 58 Reporting the Activity Data of This PDC | [22], [26] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
46.00%
|
|||
| Patients Enrolled |
175 metastatic castration-resistant prostate cancer (mCRPC) patient were included in this meta-analysis. 46% of patients had greater than 50% PSA decline after <sup>177</sup>Lu-PSMA RLT, and a higher proportion (75%) had any PSA decline after therapy.
|
||||
| Administration Dosage | 3.7-8.7 GBq/cycle | ||||
| MOA of PDC |
The PSMA molecule acts as a target for theranostics in detecting and treating prostatic lesions. This ultimately promotes the concept of precision and personalized medicine. Several published articles showed favorable outcomes of Lu-PSMA-PRLT in mCRPC patients, which quickly translated into routine clinical practices with real effectiveness, a low toxicity profile, and documentation of the risk-benefit of PRLT. Nevertheless, many questions related to PRLT remain unresolved such as the sequencing of PRLT with ARTA or taxane-based chemotherapy, re-challenge therapy, combined therapy, alpha therapy in mCRPC patients, and early treatment of PRLT in mHNPC patients. To solve these questions, several clinical trials are currently under way, and the results of these trials will be helpful in deciding treatment strategies for prostate cancer patients.
Click to Show/Hide
|
||||
| Description |
Yadav et al. provided a meta-analysis of 177Lu-PSMA-PRLT for treating mCRPC patients. They analyzed 16 articles (13 articles used 177Lu-PSMA-617, 2 articles used 177Lu-PSMA-I&T, and 1 article used both radioligands). The authors showed >50% PSA decline after 177Lu-PSMA-PRLT in 46% of patients. Anatomical imaging response as per the RECIST criteria was reported by eight studies, with a proportion of 37.2% of patients had PR, SD in 38.3% of patients and PD in 24.5% of patients, whereas molecular imaging response as per the PERCIST criteria demonstrated PR in 74 patients (44.3%), SD in 39 patients (23.4%), and PD in 54 patients (32.3%). Common clinical toxicities were grades 1-2, which included anemia (23%), leukopenia (14.2%), thrombocytopenia (15%), nephrotoxicity (9.5%), and xerostomia (14.5%). The authors observed significant heterogeneity in several studies while analyzing this meta-analysis. They concluded that 177Lu-PSMA-PRLT is a promising treatment modality in mCRPC patients who showed PD after standard care treatments.
Click to Show/Hide
|
||||
| Experiment 59 Reporting the Activity Data of This PDC | [19] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
48.00%
|
|||
| Patients Enrolled |
25 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | A median of four (iqr: 2-6) cycles every 6-8 weeks | ||||
| Administration Dosage | Mean of 7.7 ± 1.4 GBq/cycle | ||||
| MOA of PDC |
The response to radioligand therapy with 177Lu-PSMA-617 seems to be independent of the presence of early-onset prostate cancer (EOPC); however, the less favorable survival outcome observed in our study may indicate a more aggressive disease course. Expectedly, the safety of LuPSMA-RLT does not seem to be compromised in metastasized castration-resistant EOPC patients. Comparative studies on age at diagnosis of prostate cancer and the patients outcome after LuPSMA-RLT are needed.
Click to Show/Hide
|
||||
| Description |
An initial PSA reduction (≥ 50%) was observed in 9/25 (36%) of patients without being significantly associated with OS (p = 0.601). PSA response (PSA decline ≥50% at 12 weeks) was observed in 12/25 (48%) of patients and significantly associated with longer OS (16.0 months, 95% CI 7.4-24.6 vs. 4.0 months, 95% CI 1.1-6.9, p = 0.002).
|
||||
| Experiment 60 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
48.00%
|
|||
| Patients Enrolled |
24 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 1-4 cycles | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
A retrospective study reviewed 24 mCPRC patients with a median age of 81.7 (range 75.1-91.9 years old) and median of four prior lines of treatments who were treated with 177Lu-PSMA-617. 54% of patients had bone and lymph node metastasis. Primary endpoints were response, which was defined as a decrease in PSA level over 50% from baseline and toxicity. Patients were treated with one to four cycles. A PSA decline over 50% was seen in 48% (n = 11) of patients.
Click to Show/Hide
|
||||
| Experiment 61 Reporting the Activity Data of This PDC | [27] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
50.00%
|
|||
| Patients Enrolled |
10 patients with low-volume metastatic hormone-sensitive prostate cancer.
|
||||
| Administration Time | 2 cycles | ||||
| Administration Dosage | 9.0 GBq (range 8.0-9.2 GBq) | ||||
| Evaluation Method | 68Ga-PSMA-11 PET/CT assay | ||||
| MOA of PDC |
We successfully performed small lesion dosimetry and showed that the tumor sink effect in mHSPC patients is of less concern than was expected. Tumor-to-organ ratio of absorbed dose was high and tumor uptake correlates with PSA response. Additional treatment cycles are legitimate in terms of organ toxicity and could lead to better tumor response.
|
||||
| Experiment 62 Reporting the Activity Data of This PDC | [14] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
50.00%
|
|||
| Patients Enrolled |
10 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 8 weeks | ||||
| MOA of PDC |
Radiopharmaceuticals have been used in prostate cancer for decades with known efficacy in palliation of bone metastasis. The FDA approval of the most recent radiopharmaceutical, 177Lu-PSMA-617, shows a clear overall survival benefit compared to the best SOC. Current studies are ongoing to evaluate the effectiveness of 177Lu-PSMA-617 in earlier lines of therapy, such as after only 1 line of therapy with an ARPI as in the PSMAfore study, or in mCSPC in combination with ADT and an ARPI as in the PSMAddition study. Studies are also ongoing with 177Lu-PSMA-617 in combination with other treatments which may produce a synergistic effect. As described, there are many clinical trials ongoing that are modifying the 177Lu-PSMA-617 to possibly achieve improved results. Studies are also ongoing looking at swapping the 177Lu for another radioactive agent, such as 225Ac (an alpha emitter) which may have benefits over the beta-emitting 177Lu. Other studies are looking at J591, a monoclonal antibody to PSMA which has unique differences compared to small-molecule PSMA binders. Overall, PSMA-based radioligand therapy has been shown to be an effective and life-prolonging therapy and should be considered a treatment option for selected men with mCRPC. As described, there are many ongoing studies further evaluating PSMA radioligand therapy in Australia, South Africa, Europe, and the United States, representing a truly global effort to improve prostate cancer care.
Click to Show/Hide
|
||||
| Description |
Though the first experience with PSMA-targeted 177Lu dates to 2013 at Bad Burka, this experience was not reported until later. The first report on safety and efficacy came from investigators at University Hospital Bonn and University Hospital Muenster. The authors retrospectively evaluated the results of 10 consecutive patients with mCRPC who were treated with a single dose of 177Lu-DKFZ-617 (later called simply PSMA-617) PSMA between 2013 and 2014. They showed that after 8 weeks, 7 patients (70%) showed a PSA decline with 5 patients (50%) having more than a 50% decline in PSA. Grade 3 or higher hematotoxicity was seen in only one patient and there was no relevant nephrotoxicity or hepatotoxicity.
Click to Show/Hide
|
||||
| Experiment 63 Reporting the Activity Data of This PDC | [14] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
50.00%
|
|||
| Patients Enrolled |
28 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 2 doses | ||||
| MOA of PDC |
Radiopharmaceuticals have been used in prostate cancer for decades with known efficacy in palliation of bone metastasis. The FDA approval of the most recent radiopharmaceutical, 177Lu-PSMA-617, shows a clear overall survival benefit compared to the best SOC. Current studies are ongoing to evaluate the effectiveness of 177Lu-PSMA-617 in earlier lines of therapy, such as after only 1 line of therapy with an ARPI as in the PSMAfore study, or in mCSPC in combination with ADT and an ARPI as in the PSMAddition study. Studies are also ongoing with 177Lu-PSMA-617 in combination with other treatments which may produce a synergistic effect. As described, there are many clinical trials ongoing that are modifying the 177Lu-PSMA-617 to possibly achieve improved results. Studies are also ongoing looking at swapping the 177Lu for another radioactive agent, such as 225Ac (an alpha emitter) which may have benefits over the beta-emitting 177Lu. Other studies are looking at J591, a monoclonal antibody to PSMA which has unique differences compared to small-molecule PSMA binders. Overall, PSMA-based radioligand therapy has been shown to be an effective and life-prolonging therapy and should be considered a treatment option for selected men with mCRPC. As described, there are many ongoing studies further evaluating PSMA radioligand therapy in Australia, South Africa, Europe, and the United States, representing a truly global effort to improve prostate cancer care.
Click to Show/Hide
|
||||
| Description |
A subsequent retrospective study, the first evaluating multiple administrations of 177Lu-PSMA-617, was reported by the same group. The authors reviewed 28 consecutive patients who received 50 infusions of 177Lu-PSMA-617 between 2014 and 2015. In their report, a PSA decline was noted in 59% and 75% of patients after 1 and 2 therapies, respectively, and a PSA decline of 50% or greater occurred in 32% and 50%, respectively. The estimated median survival was 29.4 weeks compared to 19.7 weeks in the historical best supportive care group which was statistically significant (HR 44; 95% CI 0.20-0.95; P=.031). Authors of the study also noted no significant changes in hematologic or renal parameters
Click to Show/Hide
|
||||
| Experiment 64 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
50.00%
|
|||
| Patients Enrolled |
28 patients with metastatic castration-resistant prostate cancer.
|
||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
A retrospective analysis studied 28 patients with mCRPC who were treated with 177Lu-PSMA-617 [Citation47]. The estimated median survival was 29.4 weeks, significantly longer than survival in the supportive care group (HR, 0.44; 95% confidence interval, 0.20-0.95]; P = 0.031). Results of the study noted any PSA decline in 59% of patients after one cycle and 75% of patients after two cycles of treatment, while there was a noted PSA decline of 50% or greater in 32% of patients after one cycle of treatment and in 50% of patients after two cycles of treatment. Although this study found a 50% or greater PSA decline in majority of treated patients, 83% of patients reported a stable or improved quality of life after treatment.
Click to Show/Hide
|
||||
| Experiment 65 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
50.00%
|
|||
| Patients Enrolled |
10 patients with metastatic castration-resistant prostate cancer.
|
||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
A small two center study was conducted in 2015, which followed ten mCRPC patients treated with 177Lu-PSMA-617. Response was evaluated by change in PSA. Eight weeks after therapy, seven out of the 10 study subjects, experienced a decline in PSA. Six out of ten patients had a decline more than 30%, while five patients had a decline of more than 50% in their PSA levels. Three patients showed an increase in PSA indicative of progression of disease. Post-treatment PSA levels declined significantly in this study, indicating positive treatment response.
Click to Show/Hide
|
||||
| Experiment 66 Reporting the Activity Data of This PDC | [22] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
50.00%
|
|||
| Patients Enrolled |
2346 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Dosage | 6 GBq/cycle | ||||
| MOA of PDC |
The PSMA molecule acts as a target for theranostics in detecting and treating prostatic lesions. This ultimately promotes the concept of precision and personalized medicine. Several published articles showed favorable outcomes of Lu-PSMA-PRLT in mCRPC patients, which quickly translated into routine clinical practices with real effectiveness, a low toxicity profile, and documentation of the risk-benefit of PRLT. Nevertheless, many questions related to PRLT remain unresolved such as the sequencing of PRLT with ARTA or taxane-based chemotherapy, re-challenge therapy, combined therapy, alpha therapy in mCRPC patients, and early treatment of PRLT in mHNPC patients. To solve these questions, several clinical trials are currently under way, and the results of these trials will be helpful in deciding treatment strategies for prostate cancer patients.
Click to Show/Hide
|
||||
| Description |
Von Eyben et al. published a review and meta-analysis on 177Lu-PSMA-PRLT with the inclusion of 2346 patients. They found a median OS of 16 months after PRLT and longer survival in asymptomatic patients and those with only lymph node metastatic disease as compared to symptomatic patients and those with extensive disease. They also demonstrated ≥50% PSA decline in 50% of patients with longer survival as compared to those with <50% PSA decline. Hematologic toxicity was observed in approximately 10% of the patients with anemia of grade 3 as the most severe adverse effect of 177Lu-PSMA-PRLT. The authors mentioned that the intensified schedule of 177Lu-PSMA-PRLT (increased dose activity up to 9 GBq per cycle with a shortened time interval between cycles) increases the survival and efficacy of PRLT without increasing hematological toxicity.
Click to Show/Hide
|
||||
| Experiment 67 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
52.00%
|
|||
| Patients Enrolled |
254 patients with metastatic castration-resistant prostate cancer.
|
||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
The REALITY (REgistry to Assess Outcome and Toxicity of Targeted RadionucLIde TherapY) study was a prospective real world cohort of 254 patients with mCRPC who received 177Lu-PSMA-617 as experimental salvage therapy after conventional treatments had failed. The primary end points were efficacy, reflected by PSA-PFS, (prostate specific antigen-progression-free survival) OS, (overall survival) and safety which was reflected by the incidence of treatment-related (AEs). Over the entire course of 177Lu-PSMA-617 RLT (radioligand therapy), 52.0% patients had a greater than 50% decline in their PSA response. At a median (minimum - maximum) follow-up of 14.9 (5.0-64.4) months, the median PSA-PFS was 5.5 (4.4-6.6) months, while the median OS was 14.5 (11.5-17.5) months.
Click to Show/Hide
|
||||
| Experiment 68 Reporting the Activity Data of This PDC | [22] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
52.50%
|
|||
| Patients Enrolled |
40 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 2-5 cycles | ||||
| Administration Dosage | 4.44-5.55 GBq/cycle | ||||
| MOA of PDC |
The PSMA molecule acts as a target for theranostics in detecting and treating prostatic lesions. This ultimately promotes the concept of precision and personalized medicine. Several published articles showed favorable outcomes of Lu-PSMA-PRLT in mCRPC patients, which quickly translated into routine clinical practices with real effectiveness, a low toxicity profile, and documentation of the risk-benefit of PRLT. Nevertheless, many questions related to PRLT remain unresolved such as the sequencing of PRLT with ARTA or taxane-based chemotherapy, re-challenge therapy, combined therapy, alpha therapy in mCRPC patients, and early treatment of PRLT in mHNPC patients. To solve these questions, several clinical trials are currently under way, and the results of these trials will be helpful in deciding treatment strategies for prostate cancer patients.
Click to Show/Hide
|
||||
| Description |
Suman et al. evaluated the efficacy of 177Lu-PSMA-617 in heavily pre-treated mCRPC patients. A total of 40 mCRPC patients who received at least 2 cycles of 177Lu-PSMA-617 were included in this study. Twenty-one (52.5%) patients were responders (CR, PR, and SD) and 19 (47.5%) patients were non-responders (PD) on both symptomatic and biochemical scales. As per PET response criteria in solid tumor (PERCIST) criteria, 16 patients (43%) and 21 patients (57%) were responders and non-responders, respectively, on 68Ga-PSMA-11 PET/CT imaging. Metastatic nodal lesions responded better compared to liver and bony lesions. The median OS of 12 months and the median PFS of 7 months were registered without any grade 3/4 toxicity. The authors concluded that 177Lu-PSMA-617 controlled disease with good symptomatic and biochemical response rates without any high-grade clinical toxicity.
Click to Show/Hide
|
||||
| Experiment 69 Reporting the Activity Data of This PDC | [28] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
53.00%
|
|||
| Patients Enrolled |
Patients with metastatic castration-resistant prostate cance, who had been treated with at least one next-generation antihormonal drug as well as chemotherapy.
|
||||
| Administration Time | 159 cycle | ||||
| Administration Dosage | Median dose 6.11 GBq | ||||
| Description |
A decline in prostate-specific antigen (PSA) of ≥50% occurred in 53%, and a decline in PSA of any amount in 91% of patients. The estimated median OS was 32 weeks.
|
||||
| Experiment 70 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
53.00%
|
|||
| Patients Enrolled |
59 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | A median of 3 cycles | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
Another study retrospectively studied fifty-nine mCRPC patients after receiving at least one antihormonal drug as well as chemotherapy. These patients were treated with a median of three cycles of 177Lu-PSMA-61. The primary end point was overall survival, and secondary end point was decrease in PSA level. Follow-up data was available for forty-five patients with 91% showing a PSA decline. A decline in PSA levels of greater than or equal to 50% occurred in 53% of the patients. The median overall survival was 32 weeks. An initial alkaline phosphatase (ALP) level less than 220 U/L and a PSA decline after the first cycle were associated with a longer overall survival (56 vs. 28 weeks, p < 0.01, and 56 vs. 29 weeks, p = 0.04, respectively). Toxicity overview showed grade 3 leukopenia and thrombocytopenia in 3% patients and grade 3 anemia in 19%. No grade 3 or 4 nephrotoxicity or grade 4 blood toxicity was observed. This study showed a statistically significant decline in ALP levels after the first cycle of 177Lu-PSMA-617.
Click to Show/Hide
|
||||
| Experiment 71 Reporting the Activity Data of This PDC | [16] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
54.00%
|
|||
| Patients Enrolled |
Patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | Every 8weeks | ||||
| Administration Dosage | 6.0 GBq | ||||
| Description |
There was no significant difference comparing the rate of > 50% PSA decline or best PSA response between the 6.0 GBq and 7.5 GBq group (35% vs. 54%, p = 0.065; and - 40.2% vs. - 57.8%, p = 0.329). The median estimated survival and PSA-PFS did not significantly differ between the 6.0 GBq and 7.5 GBq groups as well (11.3 vs. 12.7 months, p = 0.384; and 9.5 vs. 12.3 months, p = 0.258).
Click to Show/Hide
|
||||
| Experiment 72 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
54.00%
|
|||
| Patients Enrolled |
56 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 1-4 cycles | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
Another retrospective study evaluated 56 mCPRC patients with a median age of 69.5 (range 55-84) who received one to four cycles of 177Lu-PSMA-617. Biochemical response was defined using Prostate Cancer Working Group Criteria 3 (PCWG3). A total of 139 cycles of treatment were performed with a decline of greater than 50% in 54% of patients and any PSA decline in 65% of patients. Estimated median overall survival was 16 months versus 14 months in the chemotherapy alone group. Longer OS was observed in patients with a PSA decline of >50%, a baseline ALP level <220 U/l, more than two cycles of treatment, and cumulative activity of greater than 15 GBq.
Click to Show/Hide
|
||||
| Experiment 73 Reporting the Activity Data of This PDC | [29] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
56.00%
|
|||
| Patients Enrolled |
Patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | Total of 213 cycles; 3 cycles with every 8 weeks | ||||
| Administration Dosage | 6.016 ± 0.543 GBq | ||||
| Description |
A PSA decline ≥50% and some PSA decline occurred in 56% and 66% of the patients.
|
||||
| Experiment 74 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
56.00%
|
|||
| Patients Enrolled |
191 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 1-5 cycles | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
A real-world study evaluated 191 patients with mCPRC treated with 177Lu-PSMA-617. Patients had confirmation of PSMA expressing lesions by 68Ga-PSMA-ligand PET/CT. The majority of individuals (90%) had first- and second-line systemic treatment prior to being treated with 177Lu-PSMA-617. Patients received one to five cycles of treatment and specific endpoints included biochemical response, radiologic response, PSA PFS, and OS. A PSA RR (defined as a decline of ≥50% in PSA) was found in 56% of patients, and any PSA decline occurred in 75% of patients. The median radiographic progression-free survival was found to be six months (range 3-10), PSA PFS (n = 132) was 4 months (range 3-8), and the overall survival (n = 191) was 12 months (range 5-18).
Click to Show/Hide
|
||||
| Experiment 75 Reporting the Activity Data of This PDC | [30] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
56.70%
|
|||
| Patients Enrolled |
30 patients with metastatic castration-resistant prostate cancer who underwent 4 cycles of mean 7.5 GBq Lu-PSMA 617 at 6weeks interval.
|
||||
| Administration Time | 4 cycles at 6-week intervals | ||||
| Administration Dosage | 7.5 GBq | ||||
| Description |
The first prospective study published by the Australian group (LuPSMA trial) was a single-center, single-arm phase 2 study in 30 mCRPC patients who underwent 4 cycles of mean 7.5 GBq Lu-PSMA 617 at 6 weeks interval. Seventeen (56.7%) of the patients reported ≥50% decline in PSA. Four patients (13%) reported relevant grade 3-4 thrombocytopenia.
|
||||
| Experiment 76 Reporting the Activity Data of This PDC | [31] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
57.00%
|
|||
| Patients Enrolled |
Patients with advanced metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 1 cycle | ||||
| Administration Dosage | 6 GBq | ||||
| Description |
During treatment, maximum prostate-specific antigen decrease was 50% or greater and 90% or greater in 57% and 24% of the patients, respectively.
|
||||
| Experiment 77 Reporting the Activity Data of This PDC | [21] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
57.00%
|
|||
| Patients Enrolled |
Patients with metastatic castration-resistant prostate cancer; naive (T-naive).
|
||||
| Experiment 78 Reporting the Activity Data of This PDC | [14] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
57.00%
|
|||
| Patients Enrolled |
30 patients with metastatic castration-resistant prostate cancer who underwent 4 cycles of mean 7.5 GBq Lu-PSMA 617 at 6weeks interval.
|
||||
| Administration Time | 4 cycles at 6-week intervals | ||||
| MOA of PDC |
Radiopharmaceuticals have been used in prostate cancer for decades with known efficacy in palliation of bone metastasis. The FDA approval of the most recent radiopharmaceutical, 177Lu-PSMA-617, shows a clear overall survival benefit compared to the best SOC. Current studies are ongoing to evaluate the effectiveness of 177Lu-PSMA-617 in earlier lines of therapy, such as after only 1 line of therapy with an ARPI as in the PSMAfore study, or in mCSPC in combination with ADT and an ARPI as in the PSMAddition study. Studies are also ongoing with 177Lu-PSMA-617 in combination with other treatments which may produce a synergistic effect. As described, there are many clinical trials ongoing that are modifying the 177Lu-PSMA-617 to possibly achieve improved results. Studies are also ongoing looking at swapping the 177Lu for another radioactive agent, such as 225Ac (an alpha emitter) which may have benefits over the beta-emitting 177Lu. Other studies are looking at J591, a monoclonal antibody to PSMA which has unique differences compared to small-molecule PSMA binders. Overall, PSMA-based radioligand therapy has been shown to be an effective and life-prolonging therapy and should be considered a treatment option for selected men with mCRPC. As described, there are many ongoing studies further evaluating PSMA radioligand therapy in Australia, South Africa, Europe, and the United States, representing a truly global effort to improve prostate cancer care.
Click to Show/Hide
|
||||
| Description |
Thirty patients received treatment in this study out of 43 screened patients, thus only 70% of patients were treated. A PSA response was seen in 17 patients (57%). There were no treatment-related deaths in the study and the most common AEs were grade 1 dry mouth in 26 patients (87%), grade 1-2 nausea in 15 patients (50%), and grade 1-2 fatigue in 15 patients (50%).
Click to Show/Hide
|
||||
| Experiment 79 Reporting the Activity Data of This PDC | [22] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
57.00%
|
|||
| Patients Enrolled |
30 patients with metastatic castration-resistant prostate cancer who underwent 4 cycles of mean 7.5 GBq Lu-PSMA 617 at 6weeks interval.
|
||||
| Administration Time | 1-4 cycles | ||||
| Administration Dosage | 4.4-8.7 GBq/cycle | ||||
| MOA of PDC |
The PSMA molecule acts as a target for theranostics in detecting and treating prostatic lesions. This ultimately promotes the concept of precision and personalized medicine. Several published articles showed favorable outcomes of Lu-PSMA-PRLT in mCRPC patients, which quickly translated into routine clinical practices with real effectiveness, a low toxicity profile, and documentation of the risk-benefit of PRLT. Nevertheless, many questions related to PRLT remain unresolved such as the sequencing of PRLT with ARTA or taxane-based chemotherapy, re-challenge therapy, combined therapy, alpha therapy in mCRPC patients, and early treatment of PRLT in mHNPC patients. To solve these questions, several clinical trials are currently under way, and the results of these trials will be helpful in deciding treatment strategies for prostate cancer patients.
Click to Show/Hide
|
||||
| Description |
In 2018, a phase II trial on 177Lu-PSMA-617 (LuPSMA trial) was published by Hofman et al. In this study, they included a total of 30 mCRPC patients who showed PD on standard therapies and received 1-4 cycles with 7.5 GBq of 177Lu-PSMA-617 (range: 4.4-8.7 GBq). They found >50% PSA decline in 17 patients (57%) and an objective response rate of 40%, 37%, and 37% of patients on 68Ga PSMA-11, FDG-PET/CT, and bone imaging, respectively. The median PFS was 7.6 months, and the median OS was 13.5 months after 177Lu-PSMA-617. Improvement in pain level was noted in 27 patients (90%), which significantly contributed to a better quality of life. 177Lu-PSMA-617 was well tolerated with minimal side effects. Commonly seen side effects were grade 1 dryness of mouth (87%), grade 1-2 transient nausea (50%) and fatigue (50%). Uncommonly seen side effects included grade 3-4 thrombocytopenia (13%), grade 3 anemia (13%), and neutropenia (7%). This was the first prospective single-arm, single-center, phase II study on the use of 177Lu-PSMA-617 in mCRPC patients.
Click to Show/Hide
|
||||
| Experiment 80 Reporting the Activity Data of This PDC | [32] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
58.00%
|
|||
| Patients Enrolled |
Metastatic castration-resistant prostate cancer patients.
|
||||
| Description |
One of the earliest experiences with 177Lu-PSMA-617 radioligand therapy (RLT) was described by Ahmadzadehfar et al. in 2015. Ten patients with mCRPC were recruited to undergo 177Lu-PSMA-617 RLT and received one cycle of therapy (dose 6 GBq). At eight-week follow-up, 70% (7/10) experienced PSA decline, and 50% (5/10) experienced >50% decline in PSA levels. After those initial encouraging results, in a follow-up study with an expanded cohort, 24 patients with progressive mCRPC underwent 177Lu-PSMA-617 RLT. After one cycle, 79.1% (19/24) showed a decline in PSA levels; 41.7% (10/24) showed >50% decline. Twenty-two out of the 24 patients were selected for a second cycle, and 68.2% (15/22) had a PSA decline, with 13 (59%) experiencing >50% decline. Since then, numerous retrospective studies with larger groups of patients have been published by the same group. In 2017, Ahmadzadehfar et al. reported a cohort of 52 patients who each received between three and six cycles of therapy (mean: 3.6 cycles, mean dose: 6 GBq). Dosing was administered in eight-week intervals and the median cumulative dose was 18.5 GBq. Of note, 80.8% (42/52) experienced a PSA decline eight weeks after the first cycle. Median overall survival was 60 weeks, with patients who had PSA responses having significantly longer survival compared to those who did not (68 vs. 33 weeks). In a cohort of 99 patients who received between one to four cycles of therapy (mean: 1.7 cycles) with 8-12 week intervals, 65.6% (45/99) had PSA response after the first cycle. In a cohort of 104 patients, described in 2018, 67.3% (70/104) experienced a PSA decline after one cycle of therapy. Patients underwent an average of 3.4 cycles of therapy, with eight-week intervals. The average dose was 6.1 GBq per cycle and 18.8 GBq cumulatively. The median overall survival was 56 weeks; again, those who responded had longer survival (62.9 vs. 47 weeks).
Click to Show/Hide
|
||||
| Experiment 81 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
58.70%
|
|||
| Patients Enrolled |
62 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | A median of 3 cycles (2-5) | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
A single center retrospective analysis studied 62 men with mCRPC who were treated with 177Lu-PSMA-617. A median of 3 treatment cycles (2-5) were administered over 4 weeks. Progression-free survival and overall survival were 4.9 months (2.4-9.6) and 17.2 months (6-26.4) respectively. Greater than 50% PSA response was found in 58.7% of patients (p < 0.004).
Click to Show/Hide
|
||||
| Experiment 82 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
58.90%
|
|||
| Patients Enrolled |
56 patients with metastatic castration-resistant prostate cancer.
|
||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
Another prospective trial studied 56 patients with progressive mCRPC and rising PSA levels who then received 177Lu-PSMA. Clinical efficacy was assessed using the visual analogue scale for pain, PSA levels, median overall survival, and Gallium-68-labeled prostate-specific membrane antigen (68Ga-PSMA PET/CT) for objective response. There was a decline in PSA of greater than 80% in 23.2% of patients, a decline of greater than 50% in 58.9%, and a decline of greater than 30% in 66.1% of patients. Progressive disease was noted in 10.7% of patients with a rise in PSA level greater than 25%. 68Ga-PSMA PET/CT prior to PSMA radioligand therapy showed the median SUVmax of the target lesion to be 37.5, which decreased to 15.7 after PSMA RLT. Ga-PSMA PET/CT was used to measure response rates which included a partial remission in 56%, stable disease in 8%, and progressive disease in 36% of patients. The median progression-free survival was 13.7 months, and median overall survival was not reached. PET/CT results showing a decrease in SUV max of the target lesion are indicative of a favorable objective response to Lu-PSMA therapy.
Click to Show/Hide
|
||||
| Experiment 83 Reporting the Activity Data of This PDC | [18] | ||||
| Indication | ATM-mutated metastatic castration resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
61.00%
|
|||
| Patients Enrolled |
44 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 1 cycle | ||||
| Administration Dosage | 7.4-22.2 GBq x 2 | ||||
| MOA of PDC |
PSMA TRT involves conjugating radionuclides to antibodies and small molecule-ligands directed against PSMA. The most common radionuclide utilized to date is Lutetium-177, a beta-emitter with a mean path-length of 0.7 mm and maximum of 1.8 mm. Gamma-ray emission allows for concurrent single photon emission computed tomography (SPECT). Actinium-225 has been the most common alpha-emitter utilized. Alpha-emitters are thousands of times more potent and can induce double-stranded DNA breaks more difficult to repair, but mean path-length is much shorter than beta-emitters (under 0.01 mm).
Click to Show/Hide
|
||||
| Experiment 84 Reporting the Activity Data of This PDC | [33] | ||||
| Indication | ATM-mutated metastatic castration resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
61.00%
|
|||
| Patients Enrolled |
121 metastatic castration-resistant prostate cancer patients.
|
||||
| Administration Dosage | Median administered cumulative activity: 20 GBq | ||||
| MOA of PDC |
177Lu-PSMA-617 RLT is an effective form of therapy in mCRPC patients and confirms the findings of the short-term studies. 177Lu-PSMA-617 prolongs the overall survival in mCRPC patients heavily pre-treated with chemotherapy, first and second-line anti-androgens, and androgen inhibitor therapies. The delayed toxicity is low and acceptable by most of these patients. Patients who were treated with various other mCRPC-approved compounds before 177Lu-PSMA-RLT were associated with a significantly shorter OS than that of the patients who received 177Lu-PSMA RLT at the earlier stages of mCRPC. An aggressive treatment approach, either sequential or in combination with second-generation anti-androgens, chemotherapies, or with investigational 225Ac-PSMA-617 alpha therapies, might prolong the survival of mCRPC patients in the future.
Click to Show/Hide
|
||||
| Description |
The median administered cumulative activity was 20 GBq (3.7-37 GBq). The median follow-up duration was 36 months (6-72 months). The estimated median PFS and OS were 12 months (mo) (95% CI: 10.3-13 mo) and 16 mo (95% CI: 13-17 mo), respectively. Any PSA decline and PSA decline >50% was achieved in 73% and 61% of the patients, respectively. Multivariate analysis revealed only failure to achieve >50% PSA decline as a significant factor associated with a poor PFS. Prognostic factors associated with reduced OS included, failure to experience >50% PSA decline, heavily pre-treated patient cohort who received >2 lines of prior treatment options, and patient sub-group treated with ≥2 lines of chemotherapy. Patients re-treated with additional treatment options after attaining 177Lu-PSMA refractory disease showed a remarkably prolonged OS. A significant clinical benefit was achieved post 177Lu-PSMA-617 RLT. The most common toxicities observed were fatigue (34.7%), followed by nausea (33%), and dry mouth (24.7%).
Click to Show/Hide
|
||||
| Experiment 85 Reporting the Activity Data of This PDC | [34] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
61.00%
|
|||
| Patients Enrolled |
99 patients with metastatic castration-resistant prostate cancer.
|
||||
| MOA of PDC |
At our center, patients who did not meet the TheraP PSMA imaging criteria or the VISION laboratory criteria benefited from 177Lu-PSMA-617 radioligand therapy.
|
||||
| Description |
Ninety-nine patients were included. Sixty patients achieved a PSA50. Seven of 18 (39%) patients who did not meet the TheraP PSMA imaging criteria achieved a PSA50. Nineteen of 31 (61%) patients who did not meet the VISION laboratory criteria achieved a PSA50. Sixty-three patients had a delay or stoppage in therapy, which was due to a good response in 19 patients and progressive disease in 14 patients. Of 10 patients with a good response who restarted treatment, 9 subsequently achieved a PSA50 on retreatment. The most common toxicities were anemia (33%) and thrombocytopenia (21%).
Click to Show/Hide
|
||||
| Experiment 86 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
62.00%
|
|||
| Patients Enrolled |
21 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | Every 8 weeks | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
Another real-world prospective cohort study included twenty-one treatments refractory mCRPC patients at Bushehr Department of Nuclear Medicine between December 2016 to December 2018 treated with 177Lu-PSMA-617 every 8 weeks. Patients had to have PSMA secreting lesions detected by PSMA imaging with 68Ga-PSMA PET or 177Lu/99Tc-PSMA before to undergoing treatment. The mean age of patients was 70.3 ± 9.6 (range 54-88) with a median of two cycles of treatment (range 1-4). The primary endpoint of the study was to assess biochemical response (BCR), which was defined as a drop in the PSA of more than 50. Additional secondary endpoints included response by ECOG and overall survival. A BCR was seen in 62% of patients. The estimated overall survival was seen to be 62.69 weeks (95% confidence interval: 42.06-83.33) with a median follow-up period of 9 months (range 1-25 months).
Click to Show/Hide
|
||||
| Experiment 87 Reporting the Activity Data of This PDC | [30] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
64.00%
|
|||
| Patients Enrolled |
50 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 4 cycles at 6-week intervals | ||||
| Administration Dosage | 7.5 GBq | ||||
| Description |
A further extension of this study with 50 patients recently reported ≥50% decrease in PSA in 64% of patients and grade 3-4 thrombocytopenia or anemia in 10% of the patients. Median progression-free survival (PFS) and overall survival (OS) was 6.9 months and 13.3 months, respectively.
|
||||
| Experiment 88 Reporting the Activity Data of This PDC | [18] | ||||
| Indication | ATM-mutated metastatic castration resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
64.00%
|
|||
| Patients Enrolled |
50 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 4 cycles | ||||
| Administration Dosage | Median 7.4 GBq | ||||
| MOA of PDC |
PSMA TRT involves conjugating radionuclides to antibodies and small molecule-ligands directed against PSMA. The most common radionuclide utilized to date is Lutetium-177, a beta-emitter with a mean path-length of 0.7 mm and maximum of 1.8 mm. Gamma-ray emission allows for concurrent single photon emission computed tomography (SPECT). Actinium-225 has been the most common alpha-emitter utilized. Alpha-emitters are thousands of times more potent and can induce double-stranded DNA breaks more difficult to repair, but mean path-length is much shorter than beta-emitters (under 0.01 mm).
Click to Show/Hide
|
||||
| Experiment 89 Reporting the Activity Data of This PDC | [35] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
64.30%
|
|||
| Administration Time | 12 weeks after the first cycle | ||||
| Administration Dosage | 6.5 ± 1.2 GBq | ||||
| MOA of PDC |
RLT with 177Lu-PSMA-617 can be effectively and safely initiated as early as 8 weeks after failure of 223Ra in patients with progressive bone-metastatic mCRPC refractory to 223Ra. Objective response can be achieved even in patients with more advanced disease and disseminated/diffuse bone metastases, albeit with increasing incidence of significant hematotoxicity.
Click to Show/Hide
|
||||
| Description |
A PSA response (≥50% PSA decline 12 weeks after the first177Lu-PSMA-617 cycle) was observed in 18/28 (64.3%) patients and imaging-based partial remission (PR) was observed in 11/28 (39.3%) patients.
|
||||
| In Vivo Model | 28 men with progressive metastatic castration-resistant prostate cancer who median age 73 years, range 63-89 years). | ||||
| Experiment 90 Reporting the Activity Data of This PDC | [13] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
65.00%
|
|||
| Patients Enrolled |
22 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | All treatment cycles | ||||
| Description |
After the first treatment cycle, only 58% of the patients (n = 19) showed a decrease in serum PSA, and only 32% showed a decrease of more than 50%. After all treatment cycles were completed, 65% of the patients responded with a PSA drop greater than 50%. An even higher group of 84% responded with a general decrease in PSA levels. The highest reduction of PSA levels was observed from 139.1 to 0.24 ug/L (99.83%). Before PSMA RLT treatment, the mean serum PSA level was 258.12 ug/L (range, 0.42-3305.00 ug/L) and after 2 to 9 treatment cycles, it decreased to 79.61 ug/L (range, 0.24-869.10 ug/L).
Click to Show/Hide
|
||||
| Experiment 91 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
65.00%
|
|||
| Patients Enrolled |
43 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | Every six to twelve weeks | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
A single center retrospective study reviewed 43 mCRPC patients with a median age of 71 (range 51-88) and 177Lu-PSMA-617 treatments every six to twelve weeks. A total of 112 cycles of RLT were conducted with a median of three cycles (range 1-6). Endpoints included PSA response, toxicity, median OS, and median PSA PFS. A PSA decline of greater than 90% was seen in 23% of patients, while a decline of greater than 50% was seen in 65% of patients. A median OS was 52 weeks, while a PSA PFS was found to be 20 weeks.
Click to Show/Hide
|
||||
| Experiment 92 Reporting the Activity Data of This PDC | [18] | ||||
| Indication | ATM-mutated metastatic castration resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
66.00%
|
|||
| Patients Enrolled |
200 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 6 cycles | ||||
| Administration Dosage | 6-8 GBq | ||||
| MOA of PDC |
PSMA TRT involves conjugating radionuclides to antibodies and small molecule-ligands directed against PSMA. The most common radionuclide utilized to date is Lutetium-177, a beta-emitter with a mean path-length of 0.7 mm and maximum of 1.8 mm. Gamma-ray emission allows for concurrent single photon emission computed tomography (SPECT). Actinium-225 has been the most common alpha-emitter utilized. Alpha-emitters are thousands of times more potent and can induce double-stranded DNA breaks more difficult to repair, but mean path-length is much shorter than beta-emitters (under 0.01 mm).
Click to Show/Hide
|
||||
| Experiment 93 Reporting the Activity Data of This PDC | [36] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
66.00%
|
|||
| Patients Enrolled |
200 patients with metastatic castration-resistant prostate cancer.
|
||||
| Evaluation Method | 68Ga-PSMA-11 PET/CT assay | ||||
| Description |
The phase II TheraP trial, compared 177Lu PSMA-617 to cabazitaxel in 200 men with mCRPC. The primary endpoint was PSA response defined by a reduction of PSA ≥ 50% from baseline. In contrast to the VISION trial, TheraP set PSMA SUVmax requirements of at least one lesion on 68Ga-PSMA-11 PET with SUVmax > 20, and the remaining metastatic lesions SUVmax > 10, and no discordant hypermetabolic disease. PSA responses were more frequent among men in the 177Lu PSMA-617 group versus the cabazitaxel group (66% vs. 37%, respectively).
Click to Show/Hide
|
||||
| Experiment 94 Reporting the Activity Data of This PDC | [14] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
66.00%
|
|||
| Patients Enrolled |
200 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | Every 6 weeks (up to 6 cycles) | ||||
| Evaluation Method | 68Ga-PSMA PET assay | ||||
| MOA of PDC |
Radiopharmaceuticals have been used in prostate cancer for decades with known efficacy in palliation of bone metastasis. The FDA approval of the most recent radiopharmaceutical, 177Lu-PSMA-617, shows a clear overall survival benefit compared to the best SOC. Current studies are ongoing to evaluate the effectiveness of 177Lu-PSMA-617 in earlier lines of therapy, such as after only 1 line of therapy with an ARPI as in the PSMAfore study, or in mCSPC in combination with ADT and an ARPI as in the PSMAddition study. Studies are also ongoing with 177Lu-PSMA-617 in combination with other treatments which may produce a synergistic effect. As described, there are many clinical trials ongoing that are modifying the 177Lu-PSMA-617 to possibly achieve improved results. Studies are also ongoing looking at swapping the 177Lu for another radioactive agent, such as 225Ac (an alpha emitter) which may have benefits over the beta-emitting 177Lu. Other studies are looking at J591, a monoclonal antibody to PSMA which has unique differences compared to small-molecule PSMA binders. Overall, PSMA-based radioligand therapy has been shown to be an effective and life-prolonging therapy and should be considered a treatment option for selected men with mCRPC. As described, there are many ongoing studies further evaluating PSMA radioligand therapy in Australia, South Africa, Europe, and the United States, representing a truly global effort to improve prostate cancer care.
Click to Show/Hide
|
||||
| Description |
Of the patients with PET screening in TheraP, approximately 27% were excluded from treatment. Investigators found that patients who received 177Lu-PSMA-617 were more likely to receive a PSA response (66% vs. 37% in the intent-to-treat group, P<.0001). Updated survival analysis was presented at a 2022 meeting, and overall survival was similar between 177Lu-PSMA-617 and cabazitaxel at 19.1 months versus 19.6 months was not significantly different between the 2 arms. The finding of survival equivalence in a PSMA-selected patient population was surprising to some but it is well known that cabazitaxel is an important life-prolonging therapy in mCRPC.
Click to Show/Hide
|
||||
| Experiment 95 Reporting the Activity Data of This PDC | [37] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >50% PSA decline |
73.00%
|
|||
| Patients Enrolled |
30 patients undergoing <sup>177</sup>Lu-PSMA-617 therapy from 2014 to 2016 (age range 50-87 years, median 73.5 years).
|
||||
| Description |
Most patients underwent three treatment cycles (n=12); at least 2 cycles (n=6) or at most 8 cycles (n=1) were performed. Out of 30 cases, PSA response after the first cycle was observed in 73% (n=22). Compared to baseline, QoL was significantly improved at 2-month follow-up revealing increase in global health status (p=0.025), role functioning (p=0.017) and emotional functioning (0.010), and decrease in pain (p=0.033). Global health status variation can be explained up to 20.5% by response in PSA (p=0.012), this improved with PSA reduction.
Click to Show/Hide
|
||||
| Experiment 96 Reporting the Activity Data of This PDC | [38] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >90% PSA decline |
58.00%
|
|||
| Patients Enrolled |
Patients with metastatic castration-resistant prostate cancer treated with LuPSMA between December 2014 and July 2019.
|
||||
| Description |
Median baseline PSA was 1000 (interquartile range 431-2151) ng/ml. PSA decline of at least 50% at 12 wk was achieved in 22 (58%) patients, while median time to pain progression was 8.3 (95% confidence interval [CI] 4.1-12.6) mouth. Median overall survival was 11.6 (95% CI 8.8-14.3) mouth.
|
||||
| Related Clinical Trial | |||||
| NCT Number | NCT03511664 | Clinical Status | Phase 3 | ||
| Clinical Description | The primary objective of this study was to compare the two alternate primary endpoints of radiographic progression-free survival (rPFS) and overall survival (OS) in patients with progressive prostate-specific membrane antigen (PSMA)-positive metastatic castration-resistant prostate cancer (mCRPC) who received 177Lu-PSMA-617 in addition to best supportive/best standard of care (BSC/BSoC) versus patients treated with best supportive/best standard of care alone. | ||||
| Experiment 97 Reporting the Activity Data of This PDC | [30] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >90% PSA decline |
38.00%
|
|||
| Patients Enrolled |
64 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | Up to 4 cycles at every 8 ± 1 weeks | ||||
| Administration Dosage | 6.0/7.4 GBq | ||||
| Description |
An investigator-initiated prospective open-label bi-centric single-arm phase 2 trial RESIST-PC (NCT03042312) randomized 64 mCRPC patients in two Lu-177 PSMA-617 activity groups (6.0 or 7.4 GBq) with up to 4 cycles at every 8 ± 1 weeks. PSA decline of ≥50% was seen in 38% of the patients, and the best PSA response occurred after 3 cycles.
|
||||
| Related Clinical Trial | |||||
| NCT Number | NCT03042312 | Clinical Status | Phase 2 | ||
| Clinical Description | This was an open-label, multicenter, prospective trial to assess safety and efficacy of 177Lu-PSMA-617 in patients with metastatic castration resistant prostate cancer. | ||||
| Experiment 98 Reporting the Activity Data of This PDC | [2] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >90% PSA decline |
16.00%
|
|||
| Patients Enrolled |
Patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | At least one course of [177lu]-psma-617 | ||||
| Administration Dosage | 6-7 GBq | ||||
| MOA of PDC |
[177Lu]-PSMA-617 is a novel treatment modality for prostate cancer, utilizing the tumors expression of PSMA as a target to allow for the administration of mixed beta-gamma radiation directly to the site of active metastases.
|
||||
| Description |
A subjective clinical benefit, based on the clinical evaluation by the treating oncologist, was observed in 28 patients (52%). The first PSA was measured following a median of 1.2 months from the start of treatment (range 0.4-3.7 months). PSA nadir was achieved within a median of 1.4 months (range 0.4-13.4). A maximal PSA decline of at least 20% was observed in 26 patients (50%), a maximal PSA decline of at least 50% was observed in 18 patients (35%), and a maximal PSA decline of at least 90% was observed in 7 patients (16%). Thirty patients (58%) had any PSA decline (PSA decline greater than 10%) upon their first PSA assessment.
Click to Show/Hide
|
||||
| Experiment 99 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >90% PSA decline |
23.00%
|
|||
| Patients Enrolled |
43 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | Every six to twelve weeks | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
A single center retrospective study reviewed 43 mCRPC patients with a median age of 71 (range 51-88) and 177Lu-PSMA-617 treatments every six to twelve weeks. A total of 112 cycles of RLT were conducted with a median of three cycles (range 1-6). Endpoints included PSA response, toxicity, median OS, and median PSA PFS. A PSA decline of greater than 90% was seen in 23% of patients, while a decline of greater than 50% was seen in 65% of patients. A median OS was 52 weeks, while a PSA PFS was found to be 20 weeks.
Click to Show/Hide
|
||||
| Experiment 100 Reporting the Activity Data of This PDC | [5] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >90% PSA decline |
33.00%
|
|||
| Patients Enrolled |
45 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 164 cycles of rnt, every 6-8 weeks | ||||
| Description |
Forty-five patients were treated with total of 164 cycles of RNT. Fifteen patients (33%) had PSA decline of ≥50%, 23 patients (51%) showed any PSA decline and 20 patients (44%) showed PSA increase of ≥25%. Median OS and PFS were 17,1 months and 7,4 months. Patients had any or ≥50% PSA response after the first cycle, lower initial ALP (<120U/L) had longer OS and PFS. Patients had normal Hb showed longer OS and patients had lower initial PSA (<51ng/mL) had longer PFS. Patients had PSA progression of ≥25% had shorter OS and PFS.
Click to Show/Hide
|
||||
| Experiment 101 Reporting the Activity Data of This PDC | [9] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | >90% PSA decline |
64.00%
|
|||
| Patients Enrolled |
Patients with PSMA-avid metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 4 cycles; every 6 wk | ||||
| Administration Dosage | 7.5 GBq/cycle | ||||
| Description |
A PSA decline of at least 50% was achieved in 32 of 50 patients (64%; 95% confidence interval [CI], 50%-77%), including 22 patients (44%; 95% CI, 30%-59%) with at least an 80% decrease.
|
||||
| Experiment 102 Reporting the Activity Data of This PDC | [39] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | ALP level hazard ratio |
1.1
|
|||
| Administration Time | After receiving 177lu-psma-617 treatment | ||||
| Description |
This analysis identified FDG-positive tumour volume (FDGvol; HR 2.6; 95% CI, 1.4-4.8), mean intensity of PSMA-avid tumour uptake (PSMAmean; HR 0.89; 95% CI, 0.8-0.98), bone scan index (BSI; HR 2.3; 95% CI, 1.2-4.4), ALP (HR 1.1; 95% CI, 1-1.2) and LDH (HR 1.2; 95% CI, 1-1.8) as biomarkers prognostic of overall survival.
|
||||
| In Vivo Model | Men with metastatic castrate-resistant prostate cancer. | ||||
| Experiment 103 Reporting the Activity Data of This PDC | [40] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Anemia |
7.10%
|
|||
| Patients Enrolled |
14 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 140 patients receiving a total of 497 cycles | ||||
| Administration Dosage | 6.9 GBq/cycle | ||||
| MOA of PDC |
Hematologic adverse events after RLT have an acceptable overall incidence and are frequently reversible. High bone tumor burden, previous taxane-based chemotherapy and pretreatment grade 2 cytopenia may be considered as risk factors for developing clinically relevant myelosuppression, whereas cumulative RLT activity and previous 223Ra-dichloride treatment show no significant contribution to incidence rates.
Click to Show/Hide
|
||||
| Description |
Significant (grade ≥ 3) hematologic adverse events occurred in 13 (9.3%) patients, with anemia in 10 (7.1%), leukopenia in 5 (3.6%) and thrombocytopenia in 6 (4.3%). Hematotoxicity was reversible to grade ≤ 2 through a median follow-up of 8 (IQR 9) months in all but two patients who died from disease progression within less than 3 months after RLT.
Click to Show/Hide
|
||||
| Experiment 104 Reporting the Activity Data of This PDC | [36] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Anemia |
12.90%
|
|||
| Patients Enrolled |
1192 patients with metastatic castration-resistant prostate cancer.
|
||||
| Description |
177Lu PSMA-617 has been shown to have a low, but significant, rate of adverse events (AE) in several clinical studies. In the phase III VISION study, 52.7% of patients experienced a grade 3 or higher AE, as compared to 38.0% of patients with similar events in the control group. Anemia was the most common grade ≥3 AE, observed in 12.9% of subjects
Click to Show/Hide
|
||||
| Experiment 105 Reporting the Activity Data of This PDC | [35] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Anemia |
17.90%
|
|||
| Administration Time | Median of 4 (iqr: 2-7) cycles | ||||
| Administration Dosage | Mean cumulative activity of 30.7 ± 23.4 GBq | ||||
| MOA of PDC |
RLT with 177Lu-PSMA-617 can be effectively and safely initiated as early as 8 weeks after failure of 223Ra in patients with progressive bone-metastatic mCRPC refractory to 223Ra. Objective response can be achieved even in patients with more advanced disease and disseminated/diffuse bone metastases, albeit with increasing incidence of significant hematotoxicity.
Click to Show/Hide
|
||||
| Description |
Grade ≥ 3 hematological toxicity was observed in six patients after their last treatment cycle with anemia, leukopenia and thrombocytopenia in 5/28 (17.9%), 4/28 (14.3%) and 6/28 (21.4%) patients, respectively.
|
||||
| In Vivo Model | 28 men with progressive metastatic castration-resistant prostate cancer who median age 73 years, range 63-89 years). | ||||
| Experiment 106 Reporting the Activity Data of This PDC | [36] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Anemia |
19.00%
|
|||
| Patients Enrolled |
1192 patients with metastatic castration-resistant prostate cancer.
|
||||
| Description |
Additionally, a recently published meta-analysis of 250 studies with a total of 1192 patients similarly found that while grade 3 and 4 toxicities were uncommon, anemia was the highest reported adverse event for both 177Lu PSMA-617 (0.19 [0.06-0.15]) and 177Lu PSMAI&T (0.09 [0.05-0.16]). Greater than 35% of patients in the treatment group of the VISION trial experienced fatigue, dry mouth, or nausea, though almost entirely grade ≤ 2 AE.
Click to Show/Hide
|
||||
| Experiment 107 Reporting the Activity Data of This PDC | [41] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Anemia | ≥ 20% | |||
| Patients Enrolled |
734 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 5 doses (range: 1 to 6) | ||||
| Administration Dosage | Median cumulative dose 37.5 GBq (range, 7.0 to 48.3) | ||||
| MOA of PDC |
On March 23, 2022, the FDA approved 177Lu-PSMA-617 for the treatment of adult patients with PSMA-positive mCRPC who have been treated with androgen receptor pathway inhibition and taxane-based chemotherapy. The approval was based on a meaningful advantage in overall survival supported by a delay in tumor progression and higher objective response rate. The decision took into account several important factors unique to this applications context. Metastatic castration-resistant prostate cancer (mCRPC) is a life-threatening condition that lacks curative treatment, creating an unmet need. This product provides a novel mechanism of action as the first radioligand therapeutic agent for mCRPC providing anti-tumor effects in both bone and non-bone sites and may provide an opportunity to be combined with other available therapies with different toxicity profiles across mechanistic classes. Finally, 177Lu-PSMA-617 offers a different safety profile than other available systemic therapies which was determined to be acceptable for the indicated patient population, expanding treatment options that can be individualized to a patients preferences and comorbidities.
Click to Show/Hide
|
||||
| Description |
Serious adverse reactions occurred in 36% of patients who received 177Lu-PSMA-617 plus BSoC. Fatal adverse reactions occurred in 2.8% of patients who received 177Lu-PSMA-617 plus BSoC, including sepsis (0.9%), pancytopenia (0.6%), hepatic failure (0.4%), intracranial hemorrhage (0.2%), subdural hematoma (0.2%), ischemic stroke (0.2%), COVID-19 (0.2%), and aspiration pneumonia (0.2%). The 2 fatal adverse reactions of intracranial hemorrhage and subdural hematoma occurred in patients who had concurrent treatment-related thrombocytopenia. The most common adverse reactions (≥ 20%) occurring at a higher incidence in patients who received 177Lu-PSMA-617 plus BSoC were fatigue, dry mouth, nausea, anemia, decreased appetite, and constipation. The most common laboratory abnormalities that worsened from baseline in ≥ 30% of patients who received 177Lu-PSMA-617 plus BSoC were decreased lymphocytes, decreased hemoglobin, decreased leukocytes, decreased platelets, decreased calcium, and decreased sodium.
Click to Show/Hide
|
||||
| Experiment 108 Reporting the Activity Data of This PDC | [42] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Anemia |
33%
|
|||
| Patients Enrolled |
45 patients with progressive metastatic castration-resistant prostate cancer and diffuse bone marrow involvement.
|
||||
| Administration Time | 4 cycles | ||||
| Administration Dosage | 7.4 ± 1.4 GBq | ||||
| Evaluation Method | 68Ga-PSMA-11 PET/CT assay | ||||
| MOA of PDC |
Our findings suggest that repeated cycles of RLT with 177Lu-PSMA-617 can be carried out at an acceptable safety profile in mCRPC patients with diffuse bone marrow involvement. RLT may provide a suitable strategy for prolonged disease control with substantial clinical benefit. After a minimum of two cycles, treatment response translated into significantly longer median OS. Further studies should be carried out to investigate the role of individualized RLT concepts in this advanced stage setting.
Click to Show/Hide
|
||||
| Description |
Patients with PR on interim imaging after two cycles had a longer median OS compared to patients with stable or progressive disease (15.5 vs. 7.1 mo, p < 0.001). Previous taxane-based chemotherapy (HR 3.21, 95%CI 1.18-8.70, p = 0.02) and baseline LDH levels (HR 1.001, 95%CI 1.000-1.001, p = 0.04) were inversely associated with OS on a Cox-regression analysis. Grade ≥ 3 hematological decline was observed after 22/201 (11%) cycles with anemia, leukopenia and thrombocytopenia in 15/45 (33%), 6/45 (13%) and 8/45 (18%) patients, respectively.
Click to Show/Hide
|
||||
| Experiment 109 Reporting the Activity Data of This PDC | [34] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Anemia |
33%
|
|||
| Patients Enrolled |
99 patients with metastatic castration-resistant prostate cancer.
|
||||
| MOA of PDC |
At our center, patients who did not meet the TheraP PSMA imaging criteria or the VISION laboratory criteria benefited from 177Lu-PSMA-617 radioligand therapy.
|
||||
| Description |
Ninety-nine patients were included. Sixty patients achieved a PSA50. Seven of 18 (39%) patients who did not meet the TheraP PSMA imaging criteria achieved a PSA50. Nineteen of 31 (61%) patients who did not meet the VISION laboratory criteria achieved a PSA50. Sixty-three patients had a delay or stoppage in therapy, which was due to a good response in 19 patients and progressive disease in 14 patients. Of 10 patients with a good response who restarted treatment, 9 subsequently achieved a PSA50 on retreatment. The most common toxicities were anemia (33%) and thrombocytopenia (21%).
Click to Show/Hide
|
||||
| Experiment 110 Reporting the Activity Data of This PDC | [41] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Appetite decrease rate | ≥ 20% | |||
| Patients Enrolled |
734 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 5 doses (range: 1 to 6) | ||||
| Administration Dosage | Median cumulative dose 37.5 GBq (range, 7.0 to 48.3) | ||||
| MOA of PDC |
On March 23, 2022, the FDA approved 177Lu-PSMA-617 for the treatment of adult patients with PSMA-positive mCRPC who have been treated with androgen receptor pathway inhibition and taxane-based chemotherapy. The approval was based on a meaningful advantage in overall survival supported by a delay in tumor progression and higher objective response rate. The decision took into account several important factors unique to this applications context. Metastatic castration-resistant prostate cancer (mCRPC) is a life-threatening condition that lacks curative treatment, creating an unmet need. This product provides a novel mechanism of action as the first radioligand therapeutic agent for mCRPC providing anti-tumor effects in both bone and non-bone sites and may provide an opportunity to be combined with other available therapies with different toxicity profiles across mechanistic classes. Finally, 177Lu-PSMA-617 offers a different safety profile than other available systemic therapies which was determined to be acceptable for the indicated patient population, expanding treatment options that can be individualized to a patients preferences and comorbidities.
Click to Show/Hide
|
||||
| Description |
Serious adverse reactions occurred in 36% of patients who received 177Lu-PSMA-617 plus BSoC. Fatal adverse reactions occurred in 2.8% of patients who received 177Lu-PSMA-617 plus BSoC, including sepsis (0.9%), pancytopenia (0.6%), hepatic failure (0.4%), intracranial hemorrhage (0.2%), subdural hematoma (0.2%), ischemic stroke (0.2%), COVID-19 (0.2%), and aspiration pneumonia (0.2%). The 2 fatal adverse reactions of intracranial hemorrhage and subdural hematoma occurred in patients who had concurrent treatment-related thrombocytopenia. The most common adverse reactions (≥ 20%) occurring at a higher incidence in patients who received 177Lu-PSMA-617 plus BSoC were fatigue, dry mouth, nausea, anemia, decreased appetite, and constipation. The most common laboratory abnormalities that worsened from baseline in ≥ 30% of patients who received 177Lu-PSMA-617 plus BSoC were decreased lymphocytes, decreased hemoglobin, decreased leukocytes, decreased platelets, decreased calcium, and decreased sodium.
Click to Show/Hide
|
||||
| Experiment 111 Reporting the Activity Data of This PDC | [41] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Aspiration pneumonia |
0.20%
|
|||
| Patients Enrolled |
734 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 5 doses (range: 1 to 6) | ||||
| Administration Dosage | Median cumulative dose 37.5 GBq (range, 7.0 to 48.3) | ||||
| MOA of PDC |
On March 23, 2022, the FDA approved 177Lu-PSMA-617 for the treatment of adult patients with PSMA-positive mCRPC who have been treated with androgen receptor pathway inhibition and taxane-based chemotherapy. The approval was based on a meaningful advantage in overall survival supported by a delay in tumor progression and higher objective response rate. The decision took into account several important factors unique to this applications context. Metastatic castration-resistant prostate cancer (mCRPC) is a life-threatening condition that lacks curative treatment, creating an unmet need. This product provides a novel mechanism of action as the first radioligand therapeutic agent for mCRPC providing anti-tumor effects in both bone and non-bone sites and may provide an opportunity to be combined with other available therapies with different toxicity profiles across mechanistic classes. Finally, 177Lu-PSMA-617 offers a different safety profile than other available systemic therapies which was determined to be acceptable for the indicated patient population, expanding treatment options that can be individualized to a patients preferences and comorbidities.
Click to Show/Hide
|
||||
| Description |
Serious adverse reactions occurred in 36% of patients who received 177Lu-PSMA-617 plus BSoC. Fatal adverse reactions occurred in 2.8% of patients who received 177Lu-PSMA-617 plus BSoC, including sepsis (0.9%), pancytopenia (0.6%), hepatic failure (0.4%), intracranial hemorrhage (0.2%), subdural hematoma (0.2%), ischemic stroke (0.2%), COVID-19 (0.2%), and aspiration pneumonia (0.2%). The 2 fatal adverse reactions of intracranial hemorrhage and subdural hematoma occurred in patients who had concurrent treatment-related thrombocytopenia. The most common adverse reactions (≥ 20%) occurring at a higher incidence in patients who received 177Lu-PSMA-617 plus BSoC were fatigue, dry mouth, nausea, anemia, decreased appetite, and constipation. The most common laboratory abnormalities that worsened from baseline in ≥ 30% of patients who received 177Lu-PSMA-617 plus BSoC were decreased lymphocytes, decreased hemoglobin, decreased leukocytes, decreased platelets, decreased calcium, and decreased sodium.
Click to Show/Hide
|
||||
| Experiment 112 Reporting the Activity Data of This PDC | [16] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Best PSA response |
-57.80%
|
|||
| Patients Enrolled |
Patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | Every 8weeks | ||||
| Administration Dosage | 6.0 GBq | ||||
| Description |
There was no significant difference comparing the rate of > 50% PSA decline or best PSA response between the 6.0 GBq and 7.5 GBq group (35% vs. 54%, p = 0.065; and - 40.2% vs. - 57.8%, p = 0.329). The median estimated survival and PSA-PFS did not significantly differ between the 6.0 GBq and 7.5 GBq groups as well (11.3 vs. 12.7 months, p = 0.384; and 9.5 vs. 12.3 months, p = 0.258).
Click to Show/Hide
|
||||
| Experiment 113 Reporting the Activity Data of This PDC | [16] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Best PSA response |
-40.20%
|
|||
| Patients Enrolled |
Patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | Every 6weeks | ||||
| Administration Dosage | 7.5 GBq | ||||
| Description |
There was no significant difference comparing the rate of > 50% PSA decline or best PSA response between the 6.0 GBq and 7.5 GBq group (35% vs. 54%, p = 0.065; and - 40.2% vs. - 57.8%, p = 0.329). The median estimated survival and PSA-PFS did not significantly differ between the 6.0 GBq and 7.5 GBq groups as well (11.3 vs. 12.7 months, p = 0.384; and 9.5 vs. 12.3 months, p = 0.258).
Click to Show/Hide
|
||||
| Experiment 114 Reporting the Activity Data of This PDC | [43] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Best PSA response rate |
60%
|
|||
| Patients Enrolled |
40 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 4 cycles every 8 weeks | ||||
| Administration Dosage | 6.0-7.4 GBq/cycle | ||||
| MOA of PDC |
177Lu-PSMA-617 was demonstrated to be safe and non-inferior to docetaxel in the treatment of mCRPC and could, thus, be potentially employed earlier in the disease course rather than being solely reserved for advanced end-stage disease.
|
||||
| Description |
Of these, best PSA-RR in the 177Lu-PSMA-617 arm was 60% (9/15) versus 40% (8/20) in the docetaxel arm.
|
||||
| Experiment 115 Reporting the Activity Data of This PDC | [44] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Biochemical non-response according to PCWG3 criteria |
64%
|
|||
| Patients Enrolled |
64 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 2 cycles | ||||
| Administration Dosage | Cumulative mean activity of 11.5 (8.1-14.9) GBq | ||||
| MOA of PDC |
In general, the first two cycles of PSMA-RLT were well tolerated haematologically. Qualitative and quantitative bone marrow impairment appears closely associated with osseous tumour burden as only patients with advanced bone involvement and non-response to therapy exhibited high-grade haematological adverse events as well as a significant mean decline of haematological parameters. This implies that in patients with already advanced mCRPC, non-response to PSMA-RLT may be a major cause of bone marrow impairment during early treatment cycles.
Click to Show/Hide
|
||||
| Description |
At restaging, 23 (36%) patients achieved a biochemical response according to PCWG3 criteria, while 41 patients (64%) patients were biochemical non-responders, 56% of which with a biochemical progression (n = 23). There were no therapy-related deaths documented in the observation period.
|
||||
| Experiment 116 Reporting the Activity Data of This PDC | [44] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Biochemical progression according to PCWG3 criteria |
56%
|
|||
| Patients Enrolled |
64 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 2 cycles | ||||
| Administration Dosage | Cumulative mean activity of 11.5 (8.1-14.9) GBq | ||||
| MOA of PDC |
In general, the first two cycles of PSMA-RLT were well tolerated haematologically. Qualitative and quantitative bone marrow impairment appears closely associated with osseous tumour burden as only patients with advanced bone involvement and non-response to therapy exhibited high-grade haematological adverse events as well as a significant mean decline of haematological parameters. This implies that in patients with already advanced mCRPC, non-response to PSMA-RLT may be a major cause of bone marrow impairment during early treatment cycles.
Click to Show/Hide
|
||||
| Description |
At restaging, 23 (36%) patients achieved a biochemical response according to PCWG3 criteria, while 41 patients (64%) patients were biochemical non-responders, 56% of which with a biochemical progression (n = 23). There were no therapy-related deaths documented in the observation period.
|
||||
| Experiment 117 Reporting the Activity Data of This PDC | [45] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Biochemical response according to PCWG3 criteria |
13%
|
|||
| Patients Enrolled |
23 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 16 week | ||||
| Administration Dosage | 6 GBq (162.16 mCi) | ||||
| MOA of PDC |
This study shows that PSA changes in patients with mCRPC as early as four weeks after the first administration of PSMA-RLT are predictive of both long-term biochemical and PET imaging responses, as well as overall survival. At this early stage, a PSA decrease of at least 30% was found to be more suitable to detect future responders, as well as a longer overall survival compared to the threshold of 50% proposed by the PCWG for long-term biochemical evaluation. An early increase in PSA (+25%) is a strong predictor for biochemical progression and shorter overall survival. Larger prospective studies are warranted to validate these findings and provide criteria for the early assessment of PSMA-RLT, including even more lenient thresholds, as suggested by our explorative retrospective ROC analysis.
Click to Show/Hide
|
||||
| Description |
At w16, 16 patients (59%) achieved a biochemical response according to the PCWG3 criteria (mean %PSAw16 -77 ± 13). Four patients (15%) displayed PSA progression (mean %PSAw16 103 ± 62), and three patients were biochemically stable (mean %PSAw16 -19 ± 22). In all patients, the biochemical response status was confirmed in the PSA follow-up. %PSAw16 had no correlation to previous treatments or other relevant pretherapeutic parameters (p ≥ 0.15)
Click to Show/Hide
|
||||
| Experiment 118 Reporting the Activity Data of This PDC | [44] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Biochemical response according to PCWG3 criteria |
36%
|
|||
| Patients Enrolled |
64 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 2 cycles | ||||
| Administration Dosage | Cumulative mean activity of 11.5 (8.1-14.9) GBq | ||||
| MOA of PDC |
In general, the first two cycles of PSMA-RLT were well tolerated haematologically. Qualitative and quantitative bone marrow impairment appears closely associated with osseous tumour burden as only patients with advanced bone involvement and non-response to therapy exhibited high-grade haematological adverse events as well as a significant mean decline of haematological parameters. This implies that in patients with already advanced mCRPC, non-response to PSMA-RLT may be a major cause of bone marrow impairment during early treatment cycles.
Click to Show/Hide
|
||||
| Description |
At restaging, 23 (36%) patients achieved a biochemical response according to PCWG3 criteria, while 41 patients (64%) patients were biochemical non-responders, 56% of which with a biochemical progression (n = 23). There were no therapy-related deaths documented in the observation period.
|
||||
| Experiment 119 Reporting the Activity Data of This PDC | [45] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Biochemical response according to PCWG3 criteria |
59%
|
|||
| Patients Enrolled |
23 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 16 week | ||||
| Administration Dosage | 6 GBq (162.16 mCi) | ||||
| MOA of PDC |
This study shows that PSA changes in patients with mCRPC as early as four weeks after the first administration of PSMA-RLT are predictive of both long-term biochemical and PET imaging responses, as well as overall survival. At this early stage, a PSA decrease of at least 30% was found to be more suitable to detect future responders, as well as a longer overall survival compared to the threshold of 50% proposed by the PCWG for long-term biochemical evaluation. An early increase in PSA (+25%) is a strong predictor for biochemical progression and shorter overall survival. Larger prospective studies are warranted to validate these findings and provide criteria for the early assessment of PSMA-RLT, including even more lenient thresholds, as suggested by our explorative retrospective ROC analysis.
Click to Show/Hide
|
||||
| Description |
At w16, 16 patients (59%) achieved a biochemical response according to the PCWG3 criteria (mean %PSAw16 -77 ± 13). Four patients (15%) displayed PSA progression (mean %PSAw16 103 ± 62), and three patients were biochemically stable (mean %PSAw16 -19 ± 22). In all patients, the biochemical response status was confirmed in the PSA follow-up. %PSAw16 had no correlation to previous treatments or other relevant pretherapeutic parameters (p ≥ 0.15)
Click to Show/Hide
|
||||
| Experiment 120 Reporting the Activity Data of This PDC | [46] | ||||
| Indication | Adenocarcinoma prostate | ||||
| Efficacy Data | Bone lesions decrease rate |
90%
|
|||
| Administration Time | 2 cycles | ||||
| Administration Dosage | 4 GBq | ||||
| MOA of PDC |
Prostate-specific membrane antigen (PSMA)-targeted radioligand therapy with 177Lu-PSMA-617 has shown promising results in patients with metastasized castration-resistant prostate cancer. We report a case of a 74-year-old man with metastatic prostate cancer with comorbidities of diabetes mellitus, hypertension, and chronic kidney disease. In order to minimize radiation burden to kidneys, a lower dose of 4 GBq of 177Lu-PSMA-617 was prescribed instead of the usual 6 to 7 GBq. There was significant decrease in prostate-specific antigen levels and symptoms. Renal profile remained stable. This case highlights that compromised renal function is not a definite contraindication to radionuclide therapy, and doses can be modified based on risk versus benefits.
Click to Show/Hide
|
||||
| Description |
Posttherapy 68Ga-PSMA scan after 2 cycles showed significant decrease in metastatic bone lesions with 90% drop in prostate-specific antigen level from 169 to 16.9 ng/mL.
|
||||
| In Vivo Model | A 74-year-old man with metastatic prostate cancer. | ||||
| Experiment 121 Reporting the Activity Data of This PDC | [15] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Bone metastases |
97%
|
|||
| Patients Enrolled |
Patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 351 cycles | ||||
| Description |
A total of 51 patients (49%) died during the observation period. The majority of patients (97%) presented with bone metastases, 77% with lymph node metastases and 32% with visceral metastases.
|
||||
| Experiment 122 Reporting the Activity Data of This PDC | [39] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Bone scan index hazard ratio |
2.3
|
|||
| Administration Time | After receiving 177lu-psma-617 treatment | ||||
| Description |
This analysis identified FDG-positive tumour volume (FDGvol; HR 2.6; 95% CI, 1.4-4.8), mean intensity of PSMA-avid tumour uptake (PSMAmean; HR 0.89; 95% CI, 0.8-0.98), bone scan index (BSI; HR 2.3; 95% CI, 1.2-4.4), ALP (HR 1.1; 95% CI, 1-1.2) and LDH (HR 1.2; 95% CI, 1-1.7) as biomarkers prognostic of overall survival.
|
||||
| In Vivo Model | Men with metastatic castrate-resistant prostate cancer. | ||||
| Experiment 123 Reporting the Activity Data of This PDC | [47] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | C-index |
0.71
|
|||
| Patients Enrolled |
40 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | Once every 6-8 weeks, for a maximum of four to six cycles | ||||
| Administration Dosage | 6.0-8.5 GBq | ||||
| Evaluation Method | 68Ga-PSMA-11 PET/CT assay | ||||
| MOA of PDC |
Also, previously identified risk factors in mCRPC, such as lactate dehydrogenase or albumin, were not available or were not collected systematically and consequently not tested in the models. Similarly, 2-[18F]FDG-PET was available only in a minority of patients in this study and thus could not be tested in the models. Dual-tracer PET imaging with [68Ga]Ga-PSMA-11 and 2-[18F]FDG-PET can improve patient selection for 177Lu-PSMA therapy; however, several steps are required to establish 2-[18F]FDG-PET as a screening tool for 177Lu-PSMA in practice (ie, confirmation of its prognostic value in a multicentre setting, standardisation of image interpretation, inclusion in drug label and guidelines, and insurance coverage).
Click to Show/Hide
|
||||
| Description |
The C-index of the overall survival model was 071 (95% CI 069-073). Similar C-indices were achieved at internal validation (071 [069-073]) and external validation (072 [068-076]). The C-index of the PSA-progression-free survival model was 070 (95% CI 068-072). Similar C-indices were achieved at internal validation (070 [068-072]) and external validation (071 [068-074]). Both models were adequately calibrated and their predictions correlated with the observed outcome. Compared with high-risk patients, low-risk patients had significantly longer overall survival in the validation cohort (249 months [95% CI 168-273] vs 74 months [40-108]; p<00001) and PSA-progression-free survival (66 months [60-71] vs 25 months [12-38]; p=0022).
Click to Show/Hide
|
||||
| Related Clinical Trial | |||||
| NCT Number | NCT03042312 | Clinical Status | Phase 2 | ||
| Clinical Description | This was an open-label, multicenter, prospective trial to assess safety and efficacy of 177Lu-PSMA-617 in patients with metastatic castration resistant prostate cancer. | ||||
| Experiment 124 Reporting the Activity Data of This PDC | [47] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | C-index |
0.71
|
|||
| Patients Enrolled |
40 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | Once every 6-8 weeks, for a maximum of four to six cycles | ||||
| Administration Dosage | 6.0-8.5 GBq | ||||
| Evaluation Method | 68Ga-PSMA-11 PET/CT assay | ||||
| MOA of PDC |
Also, previously identified risk factors in mCRPC, such as lactate dehydrogenase or albumin, were not available or were not collected systematically and consequently not tested in the models. Similarly, 2-[18F]FDG-PET was available only in a minority of patients in this study and thus could not be tested in the models. Dual-tracer PET imaging with [68Ga]Ga-PSMA-11 and 2-[18F]FDG-PET can improve patient selection for 177Lu-PSMA therapy; however, several steps are required to establish 2-[18F]FDG-PET as a screening tool for 177Lu-PSMA in practice (ie, confirmation of its prognostic value in a multicentre setting, standardisation of image interpretation, inclusion in drug label and guidelines, and insurance coverage).
Click to Show/Hide
|
||||
| Description |
The C-index of the overall survival model was 071 (95% CI 069-073). Similar C-indices were achieved at internal validation (071 [069-073]) and external validation (072 [068-076]). The C-index of the PSA-progression-free survival model was 070 (95% CI 068-072). Similar C-indices were achieved at internal validation (070 [068-072]) and external validation (071 [068-074]). Both models were adequately calibrated and their predictions correlated with the observed outcome. Compared with high-risk patients, low-risk patients had significantly longer overall survival in the validation cohort (249 months [95% CI 168-273] vs 74 months [40-108]; p<00001) and PSA-progression-free survival (66 months [60-71] vs 25 months [12-38]; p=0022).
Click to Show/Hide
|
||||
| Related Clinical Trial | |||||
| NCT Number | NCT03042312 | Clinical Status | Phase 2 | ||
| Clinical Description | This was an open-label, multicenter, prospective trial to assess safety and efficacy of 177Lu-PSMA-617 in patients with metastatic castration resistant prostate cancer. | ||||
| Experiment 125 Reporting the Activity Data of This PDC | [47] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | C-index |
0.72
|
|||
| Patients Enrolled |
40 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | Once every 6-8 weeks, for a maximum of four to six cycles | ||||
| Administration Dosage | 6.0-8.5 GBq | ||||
| Evaluation Method | 68Ga-PSMA-11 PET/CT assay | ||||
| MOA of PDC |
Also, previously identified risk factors in mCRPC, such as lactate dehydrogenase or albumin, were not available or were not collected systematically and consequently not tested in the models. Similarly, 2-[18F]FDG-PET was available only in a minority of patients in this study and thus could not be tested in the models. Dual-tracer PET imaging with [68Ga]Ga-PSMA-11 and 2-[18F]FDG-PET can improve patient selection for 177Lu-PSMA therapy; however, several steps are required to establish 2-[18F]FDG-PET as a screening tool for 177Lu-PSMA in practice (ie, confirmation of its prognostic value in a multicentre setting, standardisation of image interpretation, inclusion in drug label and guidelines, and insurance coverage).
Click to Show/Hide
|
||||
| Description |
The C-index of the overall survival model was 071 (95% CI 069-073). Similar C-indices were achieved at internal validation (071 [069-073]) and external validation (072 [068-076]). The C-index of the PSA-progression-free survival model was 070 (95% CI 068-072). Similar C-indices were achieved at internal validation (070 [068-072]) and external validation (071 [068-074]). Both models were adequately calibrated and their predictions correlated with the observed outcome. Compared with high-risk patients, low-risk patients had significantly longer overall survival in the validation cohort (249 months [95% CI 168-273] vs 74 months [40-108]; p<00001) and PSA-progression-free survival (66 months [60-71] vs 25 months [12-38]; p=0022).
Click to Show/Hide
|
||||
| Related Clinical Trial | |||||
| NCT Number | NCT03042312 | Clinical Status | Phase 2 | ||
| Clinical Description | This was an open-label, multicenter, prospective trial to assess safety and efficacy of 177Lu-PSMA-617 in patients with metastatic castration resistant prostate cancer. | ||||
| Experiment 126 Reporting the Activity Data of This PDC | [41] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Calcium decrease rate | ≥ 30% | |||
| Patients Enrolled |
734 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 5 doses (range: 1 to 6) | ||||
| Administration Dosage | Median cumulative dose 37.5 GBq (range, 7.0 to 48.3) | ||||
| MOA of PDC |
On March 23, 2022, the FDA approved 177Lu-PSMA-617 for the treatment of adult patients with PSMA-positive mCRPC who have been treated with androgen receptor pathway inhibition and taxane-based chemotherapy. The approval was based on a meaningful advantage in overall survival supported by a delay in tumor progression and higher objective response rate. The decision took into account several important factors unique to this applications context. Metastatic castration-resistant prostate cancer (mCRPC) is a life-threatening condition that lacks curative treatment, creating an unmet need. This product provides a novel mechanism of action as the first radioligand therapeutic agent for mCRPC providing anti-tumor effects in both bone and non-bone sites and may provide an opportunity to be combined with other available therapies with different toxicity profiles across mechanistic classes. Finally, 177Lu-PSMA-617 offers a different safety profile than other available systemic therapies which was determined to be acceptable for the indicated patient population, expanding treatment options that can be individualized to a patients preferences and comorbidities.
Click to Show/Hide
|
||||
| Description |
Serious adverse reactions occurred in 36% of patients who received 177Lu-PSMA-617 plus BSoC. Fatal adverse reactions occurred in 2.8% of patients who received 177Lu-PSMA-617 plus BSoC, including sepsis (0.9%), pancytopenia (0.6%), hepatic failure (0.4%), intracranial hemorrhage (0.2%), subdural hematoma (0.2%), ischemic stroke (0.2%), COVID-19 (0.2%), and aspiration pneumonia (0.2%). The 2 fatal adverse reactions of intracranial hemorrhage and subdural hematoma occurred in patients who had concurrent treatment-related thrombocytopenia. The most common adverse reactions (≥ 20%) occurring at a higher incidence in patients who received 177Lu-PSMA-617 plus BSoC were fatigue, dry mouth, nausea, anemia, decreased appetite, and constipation. The most common laboratory abnormalities that worsened from baseline in ≥ 30% of patients who received 177Lu-PSMA-617 plus BSoC were decreased lymphocytes, decreased hemoglobin, decreased leukocytes, decreased platelets, decreased calcium, and decreased sodium.
Click to Show/Hide
|
||||
| Experiment 127 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Complete response (CR) |
9.20%
|
|||
| Patients Enrolled |
581 patients with metastatic castration-resistant prostate cancer.
|
||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
The VISION trial was an international open-label phase 3 trial that assigned 581 mCRPC patients who previously received a novel hormonal agent and chemotherapy to either the treatment group (receiving 177Lu-PSMA-617 and standard of care) or control group (standard of care alone). Primary end points were progression-free survival, median overall survival, and median follow-up. Median progression-free survival was 8.7 months in the 177Lu-PSMA-617 group, as compared with 3.4 months in the control group (HR for progression or death, 0.40;99.2% confidence interval, 0.29 to 0.57;P < 0.001). Median overall survival was 15.3 months in the 177Lu-PSMA-617 group, as compared with 11.3 months in the control group (hazard ratio for death, 0.62;95% CI, 0.52 to 0.74;P < 0.001). The median follow-up was 20.3 months (95% CI, 19.8 to 21.0) in the 177Lu-PSMA-617 group and 19.8 months (95% CI, 18.3 to 20.8) in the control group. Secondary end points included median time to the first symptomatic skeletal event or death and PSA level. The median time to the first symptomatic skeletal event or death was 11.5 months in the 177Lu-PSMA-617 group, as compared with 6.8 months in the control group (P < 0.001). The proportions of patients with confirmed decreases in the PSA level of at least 50% and 80% from baseline were higher in the 177Lu-PSMA-617 group than in the control group.
Click to Show/Hide
|
||||
| Experiment 128 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Complete response (CR) |
10%
|
|||
| Patients Enrolled |
30 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 4 cycles | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
Another single-arm, single-center, phase 2 trial recruited thirty men with mCRPC and progressive disease after receiving standard treatments including taxane-based chemotherapy and second-generation anti-androgen treatment (abiraterone, enzalutamide, or both). They were administered four cycles of 177Lu-PSMA-617. The primary end points included PSA level, imaging response using bone scan, and PET/CT and quality of life. The PSA decline of greater than or equal to 50% was achieved in 57% of patients. Imaging response using PSMA PET showed a complete response in 10% of patients, a partial response in 30% of patients, and progressive disease in 27% of patients. Cognitive functioning, insomnia, and pain, which were measured using the EORTC-QLQ30 (European Organization for the Research and Treatment of Cancer Quality of Life Questionnaire) and BPI (brief pain inventory) scoring tools showed improvement during treatment compared to baseline, thus indicating improved quality of life.
Click to Show/Hide
|
||||
| Experiment 129 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Complete response (CR) |
29%
|
|||
| Patients Enrolled |
30 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 4 cycles | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
Another single-arm, single-center, phase 2 trial recruited thirty men with mCRPC and progressive disease after receiving standard treatments including taxane-based chemotherapy and second-generation anti-androgen treatment (abiraterone, enzalutamide, or both). They were administered four cycles of 177Lu-PSMA-617. The primary end points included PSA level, imaging response using bone scan, and PET/CT and quality of life. The PSA decline of greater than or equal to 50% was achieved in 57% of patients. Imaging response using PSMA PET showed a complete response in 10% of patients, a partial response in 30% of patients, and progressive disease in 27% of patients. Cognitive functioning, insomnia, and pain, which were measured using the EORTC-QLQ30 (European Organization for the Research and Treatment of Cancer Quality of Life Questionnaire) and BPI (brief pain inventory) scoring tools showed improvement during treatment compared to baseline, thus indicating improved quality of life.
Click to Show/Hide
|
||||
| Experiment 130 Reporting the Activity Data of This PDC | [48] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Complete response (CR) |
0%
|
|||
| Patients Enrolled |
Patients with metastatic castration-resistant prostate cancer who underwent 68Ga-PSMA and FDG PET-CT scans.
|
||||
| Evaluation Method | 68Ga-PSMA/18F-FDG PET-CT assay | ||||
| Description |
In the period between 2016 and 2018, 58 patients were referred for [177Lu]-PSMA PRLT to the center, of which 51 patients underwent both [68Ga]-PSMA and FDG PET-CT scans and provisionally qualified for the analysis; out of these complete information of four patients was not available and hence were excluded. Thus, 47 patients were retrospectively recruited and categorized according to the proposed Pro-PET scoring scheme and were analyzed as discussed above. The cohort comprised of heavily pretreated patients with 2 (4.3%) underwent radical prostatectomy; surgical castration was performed in 45 (95.7%) patients; first-line hormonal therapy (with estrogen analogues, leutinizing hormone releasing hormone agonists and antagonists and antiandrogens) in 44 (93.6%) patients, second-line hormonal therapy (with CYP17 blockers and newer anti-androgens) in 34 (72.4%) patients; first-line chemotherapy (with docetaxel) in 33 (70.2%) patients, second-line chemotherapy (with cabazitaxel, oral metronomic chemotherapy, etc.) in 22 (46.8%) and radiotherapy in 26 (55.3%) patients.
Click to Show/Hide
|
||||
| Experiment 131 Reporting the Activity Data of This PDC | [48] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Complete response (CR) |
2.10%
|
|||
| Patients Enrolled |
Patients with metastatic castration-resistant prostate cancer who underwent 68Ga-PSMA and FDG PET-CT scans.
|
||||
| Evaluation Method | 68Ga-PSMA/18F-FDG PET-CT assay | ||||
| Description |
In the period between 2016 and 2018, 58 patients were referred for [177Lu]-PSMA PRLT to the center, of which 51 patients underwent both [68Ga]-PSMA and FDG PET-CT scans and provisionally qualified for the analysis; out of these complete information of four patients was not available and hence were excluded. Thus, 47 patients were retrospectively recruited and categorized according to the proposed Pro-PET scoring scheme and were analyzed as discussed above. The cohort comprised of heavily pretreated patients with 2 (4.3%) underwent radical prostatectomy; surgical castration was performed in 45 (95.7%) patients; first-line hormonal therapy (with estrogen analogues, leutinizing hormone releasing hormone agonists and antagonists and antiandrogens) in 44 (93.6%) patients, second-line hormonal therapy (with CYP17 blockers and newer anti-androgens) in 34 (72.4%) patients; first-line chemotherapy (with docetaxel) in 33 (70.2%) patients, second-line chemotherapy (with cabazitaxel, oral metronomic chemotherapy, etc.) in 22 (46.8%) and radiotherapy in 26 (55.3%) patients.
Click to Show/Hide
|
||||
| Experiment 132 Reporting the Activity Data of This PDC | [48] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Complete response (CR) |
4.30%
|
|||
| Patients Enrolled |
Patients with metastatic castration-resistant prostate cancer who underwent 68Ga-PSMA and FDG PET-CT scans.
|
||||
| Evaluation Method | 68Ga-PSMA/18F-FDG PET-CT assay | ||||
| Description |
In the period between 2016 and 2018, 58 patients were referred for [177Lu]-PSMA PRLT to the center, of which 51 patients underwent both [68Ga]-PSMA and FDG PET-CT scans and provisionally qualified for the analysis; out of these complete information of four patients was not available and hence were excluded. Thus, 47 patients were retrospectively recruited and categorized according to the proposed Pro-PET scoring scheme and were analyzed as discussed above. The cohort comprised of heavily pretreated patients with 2 (4.3%) underwent radical prostatectomy; surgical castration was performed in 45 (95.7%) patients; first-line hormonal therapy (with estrogen analogues, leutinizing hormone releasing hormone agonists and antagonists and antiandrogens) in 44 (93.6%) patients, second-line hormonal therapy (with CYP17 blockers and newer anti-androgens) in 34 (72.4%) patients; first-line chemotherapy (with docetaxel) in 33 (70.2%) patients, second-line chemotherapy (with cabazitaxel, oral metronomic chemotherapy, etc.) in 22 (46.8%) and radiotherapy in 26 (55.3%) patients.
Click to Show/Hide
|
||||
| Experiment 133 Reporting the Activity Data of This PDC | [41] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Complete response (CR) |
6%
|
|||
| Patients Enrolled |
319 patients with metastatic castration-resistant prostate cancer who underwent 4 cycles of mean 7.5 GBq Lu-PSMA 617 at 6weeks interval.
|
||||
| Administration Time | Every 6 weeks for up to a total of 6 doses | ||||
| Administration Dosage | 7.4 GBq (200 mCi) | ||||
| MOA of PDC |
On March 23, 2022, the FDA approved 177Lu-PSMA-617 for the treatment of adult patients with PSMA-positive mCRPC who have been treated with androgen receptor pathway inhibition and taxane-based chemotherapy. The approval was based on a meaningful advantage in overall survival supported by a delay in tumor progression and higher objective response rate. The decision took into account several important factors unique to this applications context. Metastatic castration-resistant prostate cancer (mCRPC) is a life-threatening condition that lacks curative treatment, creating an unmet need. This product provides a novel mechanism of action as the first radioligand therapeutic agent for mCRPC providing anti-tumor effects in both bone and non-bone sites and may provide an opportunity to be combined with other available therapies with different toxicity profiles across mechanistic classes. Finally, 177Lu-PSMA-617 offers a different safety profile than other available systemic therapies which was determined to be acceptable for the indicated patient population, expanding treatment options that can be individualized to a patients preferences and comorbidities.
Click to Show/Hide
|
||||
| Description |
The co-primary endpoint of OS was statistically significant, with patients randomized to receive 177Lu-PSMA-617 plus BSoC having prolonged OS (median estimate 15.3 months) compared to BSoC alone (median estimate 11.3 months), hazard ratio (HR) 0.62 (95% CI: 0.52, 0.74, p<0.001). The planned interim OS analysis was not necessary as the targeted number of OS events were observed before the targeted number of rPFS events. Therefore, the final OS analysis was evaluated at the time of rPFS analysis.
Click to Show/Hide
|
||||
| Experiment 134 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Complete response (CR) |
8.70%
|
|||
| Patients Enrolled |
36 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 2 cycles | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
A retrospective single center study looked at therapeutic outcomes of 177Lu-PSMA-617 in mCRPC based on post-treatment imaging findings. 36 patients (aged 67 ± 8.8 years) were included out of which 23 received 2 cycles of treatment. Eleven patients (47.8%) were considered responsive in the post-therapeutic scans by 177Lu-PSMA-617, two of which experienced complete response. Nine (39.1%) patients had stable disease while three (13%) experienced disease progression.
Click to Show/Hide
|
||||
| Experiment 135 Reporting the Activity Data of This PDC | [48] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Complete response (CR) |
12.80%
|
|||
| Patients Enrolled |
Patients with metastatic castration-resistant prostate cancer who underwent 68Ga-PSMA and FDG PET-CT scans.
|
||||
| Evaluation Method | 68Ga-PSMA/18F-FDG PET-CT assay | ||||
| Description |
In the period between 2016 and 2018, 58 patients were referred for [177Lu]-PSMA PRLT to the center, of which 51 patients underwent both [68Ga]-PSMA and FDG PET-CT scans and provisionally qualified for the analysis; out of these complete information of four patients was not available and hence were excluded. Thus, 47 patients were retrospectively recruited and categorized according to the proposed Pro-PET scoring scheme and were analyzed as discussed above. The cohort comprised of heavily pretreated patients with 2 (4.3%) underwent radical prostatectomy; surgical castration was performed in 45 (95.7%) patients; first-line hormonal therapy (with estrogen analogues, leutinizing hormone releasing hormone agonists and antagonists and antiandrogens) in 44 (93.6%) patients, second-line hormonal therapy (with CYP17 blockers and newer anti-androgens) in 34 (72.4%) patients; first-line chemotherapy (with docetaxel) in 33 (70.2%) patients, second-line chemotherapy (with cabazitaxel, oral metronomic chemotherapy, etc.) in 22 (46.8%) and radiotherapy in 26 (55.3%) patients.
Click to Show/Hide
|
||||
| Experiment 136 Reporting the Activity Data of This PDC | [41] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Constipation | ≥ 20% | |||
| Patients Enrolled |
734 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 5 doses (range: 1 to 6) | ||||
| Administration Dosage | Median cumulative dose 37.5 GBq (range, 7.0 to 48.3) | ||||
| MOA of PDC |
On March 23, 2022, the FDA approved 177Lu-PSMA-617 for the treatment of adult patients with PSMA-positive mCRPC who have been treated with androgen receptor pathway inhibition and taxane-based chemotherapy. The approval was based on a meaningful advantage in overall survival supported by a delay in tumor progression and higher objective response rate. The decision took into account several important factors unique to this applications context. Metastatic castration-resistant prostate cancer (mCRPC) is a life-threatening condition that lacks curative treatment, creating an unmet need. This product provides a novel mechanism of action as the first radioligand therapeutic agent for mCRPC providing anti-tumor effects in both bone and non-bone sites and may provide an opportunity to be combined with other available therapies with different toxicity profiles across mechanistic classes. Finally, 177Lu-PSMA-617 offers a different safety profile than other available systemic therapies which was determined to be acceptable for the indicated patient population, expanding treatment options that can be individualized to a patients preferences and comorbidities.
Click to Show/Hide
|
||||
| Description |
Serious adverse reactions occurred in 36% of patients who received 177Lu-PSMA-617 plus BSoC. Fatal adverse reactions occurred in 2.8% of patients who received 177Lu-PSMA-617 plus BSoC, including sepsis (0.9%), pancytopenia (0.6%), hepatic failure (0.4%), intracranial hemorrhage (0.2%), subdural hematoma (0.2%), ischemic stroke (0.2%), COVID-19 (0.2%), and aspiration pneumonia (0.2%). The 2 fatal adverse reactions of intracranial hemorrhage and subdural hematoma occurred in patients who had concurrent treatment-related thrombocytopenia. The most common adverse reactions (≥ 20%) occurring at a higher incidence in patients who received 177Lu-PSMA-617 plus BSoC were fatigue, dry mouth, nausea, anemia, decreased appetite, and constipation. The most common laboratory abnormalities that worsened from baseline in ≥ 30% of patients who received 177Lu-PSMA-617 plus BSoC were decreased lymphocytes, decreased hemoglobin, decreased leukocytes, decreased platelets, decreased calcium, and decreased sodium.
Click to Show/Hide
|
||||
| Experiment 137 Reporting the Activity Data of This PDC | [48] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Death rate |
44.70%
|
|||
| Patients Enrolled |
Patients with metastatic castration-resistant prostate cancer who underwent 68Ga-PSMA and FDG PET-CT scans.
|
||||
| Evaluation Method | 68Ga-PSMA/18F-FDG PET-CT assay | ||||
| Description |
In the period between 2016 and 2018, 58 patients were referred for [177Lu]-PSMA PRLT to the center, of which 51 patients underwent both [68Ga]-PSMA and FDG PET-CT scans and provisionally qualified for the analysis; out of these complete information of four patients was not available and hence were excluded. Thus, 47 patients were retrospectively recruited and categorized according to the proposed Pro-PET scoring scheme and were analyzed as discussed above. The cohort comprised of heavily pretreated patients with 2 (4.3%) underwent radical prostatectomy; surgical castration was performed in 45 (95.7%) patients; first-line hormonal therapy (with estrogen analogues, leutinizing hormone releasing hormone agonists and antagonists and antiandrogens) in 44 (93.6%) patients, second-line hormonal therapy (with CYP17 blockers and newer anti-androgens) in 34 (72.4%) patients; first-line chemotherapy (with docetaxel) in 33 (70.2%) patients, second-line chemotherapy (with cabazitaxel, oral metronomic chemotherapy, etc.) in 22 (46.8%) and radiotherapy in 26 (55.3%) patients.
Click to Show/Hide
|
||||
| Experiment 138 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Delayed disease progression hazard ratio |
0.63
|
|||
| Patients Enrolled |
65 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | ≤6 cycles every 6 weeks | ||||
| Administration Dosage | 6.0-8.5 GBq | ||||
| MOA of PDC |
Lutetium Lu 177 vipivotide tetraxetan is a PSMA-binding ligand bound to a DOTA chelator (i.e., tetraxetan) radiolabeled with lutetium-177. Once lutetium Lu 177 vipivotide tetraxetan is bound to PSMA-expressing cells, the beta-minus emission from lutetium-177 delivers radiation to PSMA-expressing and surrounding cells, inducing DNA damage that leads to cell death. The exposure-efficacy relationships of lutetium Lu 177 vipivotide tetraxetan and the time course of the pharmacodynamic response are not fully characterized [9]. Lutetium-177 decays to a stable hafnium-177 with a physical half-life of 6.647 days by emitting beta-minus radiation with a maximum energy of 0.498 MeV (79%) and photonic radiation (γ) of 0.208 MeV (11%) and 0.113 MeV (6.4%).
Click to Show/Hide
|
||||
| Description |
65 of 99 patients treated with lutetium Lu 177 vipivotide tetraxetan 6.0-8.5 GBq every 6 weeks for up to 6 cycles (n = 99) compared with 37 of 101 patients receiving cabazitaxel 20 mg/m2 every 3 weeks for up to 10 cycles achieved a PSA reduction of ≥ 50% from baseline [66% vs 37%; treatment difference 29% (95% CI 16-42); p < 0.0001 (ITT analysis)]. Lutetium Lu 177 vipivotide tetraxetan also delayed disease progression [HR 0.63 (95% CI 0.46-0.86;) p = 0.0028], radiographic progression [0.64 (95% CI 0.46-0.88); p = 0.0070] and PSA PFS [0.60 (95% CI 0.44-0.83); p = 0.0017] compared with cabazitaxel.
Click to Show/Hide
|
||||
| Half life period | 41.6 h | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT03392428 | Clinical Status | Phase 2 | ||
| Clinical Description | This open label, randomised, stratified, 2-arm, multicentre, phase 2 trial aims to determine the activity and safety of Lu-PSMA vs cabazitaxel in men with progressive metastatic castration resistant prostate cancer | ||||
| Experiment 139 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Delayed progression-free survival |
60%
|
|||
| Patients Enrolled |
65 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | ≤6 cycles every 6 weeks | ||||
| Administration Dosage | 6.0-8.5 GBq | ||||
| MOA of PDC |
Lutetium Lu 177 vipivotide tetraxetan is a PSMA-binding ligand bound to a DOTA chelator (i.e., tetraxetan) radiolabeled with lutetium-177. Once lutetium Lu 177 vipivotide tetraxetan is bound to PSMA-expressing cells, the beta-minus emission from lutetium-177 delivers radiation to PSMA-expressing and surrounding cells, inducing DNA damage that leads to cell death. The exposure-efficacy relationships of lutetium Lu 177 vipivotide tetraxetan and the time course of the pharmacodynamic response are not fully characterized [9]. Lutetium-177 decays to a stable hafnium-177 with a physical half-life of 6.647 days by emitting beta-minus radiation with a maximum energy of 0.498 MeV (79%) and photonic radiation (γ) of 0.208 MeV (11%) and 0.113 MeV (6.4%).
Click to Show/Hide
|
||||
| Description |
65 of 99 patients treated with lutetium Lu 177 vipivotide tetraxetan 6.0-8.5 GBq every 6 weeks for up to 6 cycles (n = 99) compared with 37 of 101 patients receiving cabazitaxel 20 mg/m2 every 3 weeks for up to 10 cycles achieved a PSA reduction of ≥ 50% from baseline [66% vs 37%; treatment difference 29% (95% CI 16-42); p < 0.0001 (ITT analysis)]. Lutetium Lu 177 vipivotide tetraxetan also delayed disease progression [HR 0.63 (95% CI 0.46-0.86;) p = 0.0028], radiographic progression [0.64 (95% CI 0.46-0.88); p = 0.0070] and PSA PFS [0.60 (95% CI 0.44-0.83); p = 0.0017] compared with cabazitaxel.
Click to Show/Hide
|
||||
| Half life period | 41.6 h | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT03392428 | Clinical Status | Phase 2 | ||
| Clinical Description | This open label, randomised, stratified, 2-arm, multicentre, phase 2 trial aims to determine the activity and safety of Lu-PSMA vs cabazitaxel in men with progressive metastatic castration resistant prostate cancer | ||||
| Experiment 140 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Delayed radiographic progression |
64%
|
|||
| Patients Enrolled |
65 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | ≤6 cycles every 6 weeks | ||||
| Administration Dosage | 6.0-8.5 GBq | ||||
| MOA of PDC |
Lutetium Lu 177 vipivotide tetraxetan is a PSMA-binding ligand bound to a DOTA chelator (i.e., tetraxetan) radiolabeled with lutetium-177. Once lutetium Lu 177 vipivotide tetraxetan is bound to PSMA-expressing cells, the beta-minus emission from lutetium-177 delivers radiation to PSMA-expressing and surrounding cells, inducing DNA damage that leads to cell death. The exposure-efficacy relationships of lutetium Lu 177 vipivotide tetraxetan and the time course of the pharmacodynamic response are not fully characterized [9]. Lutetium-177 decays to a stable hafnium-177 with a physical half-life of 6.647 days by emitting beta-minus radiation with a maximum energy of 0.498 MeV (79%) and photonic radiation (γ) of 0.208 MeV (11%) and 0.113 MeV (6.4%).
Click to Show/Hide
|
||||
| Description |
65 of 99 patients treated with lutetium Lu 177 vipivotide tetraxetan 6.0-8.5 GBq every 6 weeks for up to 6 cycles (n = 99) compared with 37 of 101 patients receiving cabazitaxel 20 mg/m2 every 3 weeks for up to 10 cycles achieved a PSA reduction of ≥ 50% from baseline [66% vs 37%; treatment difference 29% (95% CI 16-42); p < 0.0001 (ITT analysis)]. Lutetium Lu 177 vipivotide tetraxetan also delayed disease progression [HR 0.63 (95% CI 0.46-0.86;) p = 0.0028], radiographic progression [0.64 (95% CI 0.46-0.88); p = 0.0070] and PSA PFS [0.60 (95% CI 0.44-0.83); p = 0.0017] compared with cabazitaxel.
Click to Show/Hide
|
||||
| Half life period | 41.6 h | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT03392428 | Clinical Status | Phase 2 | ||
| Clinical Description | This open label, randomised, stratified, 2-arm, multicentre, phase 2 trial aims to determine the activity and safety of Lu-PSMA vs cabazitaxel in men with progressive metastatic castration resistant prostate cancer | ||||
| Experiment 141 Reporting the Activity Data of This PDC | [14] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Diarrhea |
52%
|
|||
| Patients Enrolled |
200 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | Every 6 weeks (up to 6 cycles) | ||||
| MOA of PDC |
Radiopharmaceuticals have been used in prostate cancer for decades with known efficacy in palliation of bone metastasis. The FDA approval of the most recent radiopharmaceutical, 177Lu-PSMA-617, shows a clear overall survival benefit compared to the best SOC. Current studies are ongoing to evaluate the effectiveness of 177Lu-PSMA-617 in earlier lines of therapy, such as after only 1 line of therapy with an ARPI as in the PSMAfore study, or in mCSPC in combination with ADT and an ARPI as in the PSMAddition study. Studies are also ongoing with 177Lu-PSMA-617 in combination with other treatments which may produce a synergistic effect. As described, there are many clinical trials ongoing that are modifying the 177Lu-PSMA-617 to possibly achieve improved results. Studies are also ongoing looking at swapping the 177Lu for another radioactive agent, such as 225Ac (an alpha emitter) which may have benefits over the beta-emitting 177Lu. Other studies are looking at J591, a monoclonal antibody to PSMA which has unique differences compared to small-molecule PSMA binders. Overall, PSMA-based radioligand therapy has been shown to be an effective and life-prolonging therapy and should be considered a treatment option for selected men with mCRPC. As described, there are many ongoing studies further evaluating PSMA radioligand therapy in Australia, South Africa, Europe, and the United States, representing a truly global effort to improve prostate cancer care.
Click to Show/Hide
|
||||
| Description |
Grade 3-4 AEs occurred in 32 (33%) of men who received 177Lu-PSMA-617 versus 45 (53%) of men in the cabazitaxel group. All-grade toxicities that were more common in the 177Lu-PSMA-617 were dry mouth (60% vs. 21%), dry eyes (30% vs. 4%), and thrombocytopenia (18% vs. 5%). All-grade toxicities that were more common with cabazitaxel were diarrhea (52% vs. 18%), neuropathy (26% vs. 10%), and dysgeusia (27% vs. 12%).
Click to Show/Hide
|
||||
| Experiment 142 Reporting the Activity Data of This PDC | [49] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Disease control rate (DCR) |
77%
|
|||
| Patients Enrolled |
Patients with progressive disease (PD) on second-line hormonal therapy and/or docetaxel chemotherapy.
|
||||
| Administration Time | 8- to 12-weekly intervals | ||||
| Administration Dosage | 3.7 to 8 GBq | ||||
| Description |
The disease control rates according to the radiographic and molecular response were 77% and 71%, respectively. The median overall survival and median progression-free survivals were 14 and 11.8 months, respectively.
|
||||
| Experiment 143 Reporting the Activity Data of This PDC | [14] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Dysgeusia |
27%
|
|||
| Patients Enrolled |
200 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | Every 6 weeks (up to 6 cycles) | ||||
| MOA of PDC |
Radiopharmaceuticals have been used in prostate cancer for decades with known efficacy in palliation of bone metastasis. The FDA approval of the most recent radiopharmaceutical, 177Lu-PSMA-617, shows a clear overall survival benefit compared to the best SOC. Current studies are ongoing to evaluate the effectiveness of 177Lu-PSMA-617 in earlier lines of therapy, such as after only 1 line of therapy with an ARPI as in the PSMAfore study, or in mCSPC in combination with ADT and an ARPI as in the PSMAddition study. Studies are also ongoing with 177Lu-PSMA-617 in combination with other treatments which may produce a synergistic effect. As described, there are many clinical trials ongoing that are modifying the 177Lu-PSMA-617 to possibly achieve improved results. Studies are also ongoing looking at swapping the 177Lu for another radioactive agent, such as 225Ac (an alpha emitter) which may have benefits over the beta-emitting 177Lu. Other studies are looking at J591, a monoclonal antibody to PSMA which has unique differences compared to small-molecule PSMA binders. Overall, PSMA-based radioligand therapy has been shown to be an effective and life-prolonging therapy and should be considered a treatment option for selected men with mCRPC. As described, there are many ongoing studies further evaluating PSMA radioligand therapy in Australia, South Africa, Europe, and the United States, representing a truly global effort to improve prostate cancer care.
Click to Show/Hide
|
||||
| Description |
Grade 3-4 AEs occurred in 32 (33%) of men who received 177Lu-PSMA-617 versus 45 (53%) of men in the cabazitaxel group. All-grade toxicities that were more common in the 177Lu-PSMA-617 were dry mouth (60% vs. 21%), dry eyes (30% vs. 4%), and thrombocytopenia (18% vs. 5%). All-grade toxicities that were more common with cabazitaxel were diarrhea (52% vs. 18%), neuropathy (26% vs. 10%), and dysgeusia (27% vs. 12%).
Click to Show/Hide
|
||||
| Experiment 144 Reporting the Activity Data of This PDC | [41] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Fatigue | ≥ 20% | |||
| Patients Enrolled |
734 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 5 doses (range: 1 to 6) | ||||
| Administration Dosage | Median cumulative dose 37.5 GBq (range, 7.0 to 48.3) | ||||
| MOA of PDC |
On March 23, 2022, the FDA approved 177Lu-PSMA-617 for the treatment of adult patients with PSMA-positive mCRPC who have been treated with androgen receptor pathway inhibition and taxane-based chemotherapy. The approval was based on a meaningful advantage in overall survival supported by a delay in tumor progression and higher objective response rate. The decision took into account several important factors unique to this applications context. Metastatic castration-resistant prostate cancer (mCRPC) is a life-threatening condition that lacks curative treatment, creating an unmet need. This product provides a novel mechanism of action as the first radioligand therapeutic agent for mCRPC providing anti-tumor effects in both bone and non-bone sites and may provide an opportunity to be combined with other available therapies with different toxicity profiles across mechanistic classes. Finally, 177Lu-PSMA-617 offers a different safety profile than other available systemic therapies which was determined to be acceptable for the indicated patient population, expanding treatment options that can be individualized to a patients preferences and comorbidities.
Click to Show/Hide
|
||||
| Description |
Serious adverse reactions occurred in 36% of patients who received 177Lu-PSMA-617 plus BSoC. Fatal adverse reactions occurred in 2.8% of patients who received 177Lu-PSMA-617 plus BSoC, including sepsis (0.9%), pancytopenia (0.6%), hepatic failure (0.4%), intracranial hemorrhage (0.2%), subdural hematoma (0.2%), ischemic stroke (0.2%), COVID-19 (0.2%), and aspiration pneumonia (0.2%). The 2 fatal adverse reactions of intracranial hemorrhage and subdural hematoma occurred in patients who had concurrent treatment-related thrombocytopenia. The most common adverse reactions (≥ 20%) occurring at a higher incidence in patients who received 177Lu-PSMA-617 plus BSoC were fatigue, dry mouth, nausea, anemia, decreased appetite, and constipation. The most common laboratory abnormalities that worsened from baseline in ≥ 30% of patients who received 177Lu-PSMA-617 plus BSoC were decreased lymphocytes, decreased hemoglobin, decreased leukocytes, decreased platelets, decreased calcium, and decreased sodium.
Click to Show/Hide
|
||||
| Experiment 145 Reporting the Activity Data of This PDC | [33] | ||||
| Indication | ATM-mutated metastatic castration resistant prostate cancer | ||||
| Efficacy Data | Fatigue |
34.70%
|
|||
| Patients Enrolled |
121 metastatic castration-resistant prostate cancer patients.
|
||||
| Administration Dosage | Median administered cumulative activity: 20 GBq | ||||
| MOA of PDC |
177Lu-PSMA-617 RLT is an effective form of therapy in mCRPC patients and confirms the findings of the short-term studies. 177Lu-PSMA-617 prolongs the overall survival in mCRPC patients heavily pre-treated with chemotherapy, first and second-line anti-androgens, and androgen inhibitor therapies. The delayed toxicity is low and acceptable by most of these patients. Patients who were treated with various other mCRPC-approved compounds before 177Lu-PSMA-RLT were associated with a significantly shorter OS than that of the patients who received 177Lu-PSMA RLT at the earlier stages of mCRPC. An aggressive treatment approach, either sequential or in combination with second-generation anti-androgens, chemotherapies, or with investigational 225Ac-PSMA-617 alpha therapies, might prolong the survival of mCRPC patients in the future.
Click to Show/Hide
|
||||
| Description |
The median administered cumulative activity was 20 GBq (3.7-37 GBq). The median follow-up duration was 36 months (6-72 months). The estimated median PFS and OS were 12 months (mo) (95% CI: 10.3-13 mo) and 16 mo (95% CI: 13-17 mo), respectively. Any PSA decline and PSA decline >50% was achieved in 73% and 61% of the patients, respectively. Multivariate analysis revealed only failure to achieve >50% PSA decline as a significant factor associated with a poor PFS. Prognostic factors associated with reduced OS included, failure to experience >50% PSA decline, heavily pre-treated patient cohort who received >2 lines of prior treatment options, and patient sub-group treated with ≥2 lines of chemotherapy. Patients re-treated with additional treatment options after attaining 177Lu-PSMA refractory disease showed a remarkably prolonged OS. A significant clinical benefit was achieved post 177Lu-PSMA-617 RLT. The most common toxicities observed were fatigue (34.7%), followed by nausea (33%), and dry mouth (24.7%).
Click to Show/Hide
|
||||
| Experiment 146 Reporting the Activity Data of This PDC | [14] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Fatigue |
43%
|
|||
| Patients Enrolled |
831 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | Every 6 weeks for 4-6 cycles | ||||
| MOA of PDC |
Radiopharmaceuticals have been used in prostate cancer for decades with known efficacy in palliation of bone metastasis. The FDA approval of the most recent radiopharmaceutical, 177Lu-PSMA-617, shows a clear overall survival benefit compared to the best SOC. Current studies are ongoing to evaluate the effectiveness of 177Lu-PSMA-617 in earlier lines of therapy, such as after only 1 line of therapy with an ARPI as in the PSMAfore study, or in mCSPC in combination with ADT and an ARPI as in the PSMAddition study. Studies are also ongoing with 177Lu-PSMA-617 in combination with other treatments which may produce a synergistic effect. As described, there are many clinical trials ongoing that are modifying the 177Lu-PSMA-617 to possibly achieve improved results. Studies are also ongoing looking at swapping the 177Lu for another radioactive agent, such as 225Ac (an alpha emitter) which may have benefits over the beta-emitting 177Lu. Other studies are looking at J591, a monoclonal antibody to PSMA which has unique differences compared to small-molecule PSMA binders. Overall, PSMA-based radioligand therapy has been shown to be an effective and life-prolonging therapy and should be considered a treatment option for selected men with mCRPC. As described, there are many ongoing studies further evaluating PSMA radioligand therapy in Australia, South Africa, Europe, and the United States, representing a truly global effort to improve prostate cancer care.
Click to Show/Hide
|
||||
| Description |
Toxicities of grade 3 or higher were experienced by 52.7% of patients. The most common all-grade toxicities with 177Lu-PSMA-617 were fatigue (43.1%), dry mouth (38.8%-0% grade 3 or higher), and nausea (35.3%). The most common grade 3 or higher toxicities included anemia (12.9%), thrombocytopenia (7.9%), and leucopenia (7.8%).
|
||||
| Experiment 147 Reporting the Activity Data of This PDC | [39] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | FDG-positive molecular tumour volume hazard ratio |
2.6
|
|||
| Administration Time | After receiving 177lu-psma-617 treatment | ||||
| Description |
This analysis identified FDG-positive tumour volume (FDGvol; HR 2.6; 95% CI, 1.4-4.8), mean intensity of PSMA-avid tumour uptake (PSMAmean; HR 0.89; 95% CI, 0.8-0.98), bone scan index (BSI; HR 2.3; 95% CI, 1.2-4.4), ALP (HR 1.1; 95% CI, 1-1.2) and LDH (HR 1.2; 95% CI, 1-1.5) as biomarkers prognostic of overall survival.
|
||||
| In Vivo Model | Men with metastatic castrate-resistant prostate cancer. | ||||
| Experiment 148 Reporting the Activity Data of This PDC | [50] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Glutathione increase rate |
0.016 mg/mL
|
|||
| Patients Enrolled |
Prostate cancer and neuroendocrine tumor patients referred to therapy with <sup>177</sup>Lu-PSMA and <sup>177</sup>Lu-DOTATATE, respectively.
|
||||
| Administration Time | 48 h | ||||
| Administration Dosage | 5.5 GBq | ||||
| MOA of PDC |
In biological systems, antioxidants such as catalase, superoxide dismutase, glutathione peroxidase, and glutathione reductase are responsible for the elimination or reduction of the adverse effects of ROS, that is, they prevent or reduce ROS generation. Dietary antioxidants, such as vitamins E, A, and C, and anthocyanins and polyphenols have a role in the protection of cells against ROS damage.
Click to Show/Hide
|
||||
| Description |
In total, 61 RNT cycles were evaluated in 34 patients with age of 65 ± 2.83 (median ± SE) years (range of 27-99); this total included 20 (59%) prostate cancer patients [35 cycles (57.4%)] and 14 patients (41%) with NET [26 cycles (42.6%)]. Of the 61 evaluated cycles, 27 cycles were given in the control group and 34 cycles were given in the intervention group. The serum level of MDA was significantly increased after treatment compared to before treatment (P = 0.02) in the control group, while no significant change in the serum level of MDA was observed in the intervention group (P = 0.52). The serum level of GSH was insignificantly decreased after treatment compared to before treatment in the control group and slightly increased after treatment in the intervention group (P > 0.05). The serum level of glutathione reductase was insignificantly increased in all groups of patients after treatment (P > 0.05).
Click to Show/Hide
|
||||
| Experiment 149 Reporting the Activity Data of This PDC | [50] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Glutathione reductase increase rate |
6.6 nmol/min/mg
|
|||
| Patients Enrolled |
Prostate cancer and neuroendocrine tumor patients referred to therapy with <sup>177</sup>Lu-PSMA and <sup>177</sup>Lu-DOTATATE, respectively.
|
||||
| Administration Time | 48 h | ||||
| Administration Dosage | 5.5 GBq | ||||
| MOA of PDC |
Vitamin C as a water-soluble vitamin is the reduced form of ascorbic acid. No significant adverse effect of taking high doses of vitamin C (over 2000 mg/day) has been reported due to the water-soluble feature of vitamin C. Vitamin C directly reacts with hydroxy, alkoxyl, and lipid peroxyl radicals and converts them to alcohol, water, and hydroperoxide lipid, respectively. It has been shown that taking vitamin C before radioiodine therapy can ameliorate the oxidative stress effect of radioiodine. The radioprotective effects of vitamin C are mainly due to its free radical scavenging activity.
Click to Show/Hide
|
||||
| Description |
In total, 61 RNT cycles were evaluated in 34 patients with age of 65 ± 2.83 (median ± SE) years (range of 27-99); this total included 20 (59%) prostate cancer patients [35 cycles (57.4%)] and 14 patients (41%) with NET [26 cycles (42.6%)]. Of the 61 evaluated cycles, 27 cycles were given in the control group and 34 cycles were given in the intervention group. The serum level of MDA was significantly increased after treatment compared to before treatment (P = 0.02) in the control group, while no significant change in the serum level of MDA was observed in the intervention group (P = 0.52). The serum level of GSH was insignificantly decreased after treatment compared to before treatment in the control group and slightly increased after treatment in the intervention group (P > 0.05). The serum level of glutathione reductase was insignificantly increased in all groups of patients after treatment (P > 0.05).
Click to Show/Hide
|
||||
| Experiment 150 Reporting the Activity Data of This PDC | [19] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Grade ≥ 3 anemia |
12%
|
|||
| Patients Enrolled |
25 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | A median of four (iqr: 2-6) cycles every 6-8 weeks | ||||
| Administration Dosage | Mean of 7.7 ± 1.4 GBq/cycle | ||||
| MOA of PDC |
The response to radioligand therapy with 177Lu-PSMA-617 seems to be independent of the presence of early-onset prostate cancer (EOPC); however, the less favorable survival outcome observed in our study may indicate a more aggressive disease course. Expectedly, the safety of LuPSMA-RLT does not seem to be compromised in metastasized castration-resistant EOPC patients. Comparative studies on age at diagnosis of prostate cancer and the patients outcome after LuPSMA-RLT are needed.
Click to Show/Hide
|
||||
| Description |
Intra- or post-therapeutic toxicity was graded according to the CTCAE v5.0 criteria. Newly developing grade ≥ 3 anemia, leukopenia, and thrombocytopenia occurred in three (12%), one (4%), and three (12%) patients, respectively. One patient showed renal toxicity (grade ≥ 3) during follow-up. Pain palliation (>2 level VAS decline) was achieved in 9/14 (64%) and performance status improvement (ECOG level decline ≥ 1) in 8/17 (47%) of patients.
Click to Show/Hide
|
||||
| Experiment 151 Reporting the Activity Data of This PDC | [40] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Grade ≥ 3 hematologic adverse events |
9.30%
|
|||
| Patients Enrolled |
14 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 140 patients receiving a total of 497 cycles | ||||
| Administration Dosage | 6.9 GBq/cycle | ||||
| MOA of PDC |
Hematologic adverse events after RLT have an acceptable overall incidence and are frequently reversible. High bone tumor burden, previous taxane-based chemotherapy and pretreatment grade 2 cytopenia may be considered as risk factors for developing clinically relevant myelosuppression, whereas cumulative RLT activity and previous 223Ra-dichloride treatment show no significant contribution to incidence rates.
Click to Show/Hide
|
||||
| Description |
Significant (grade ≥ 3) hematologic adverse events occurred in 13 (9.3%) patients, with anemia in 10 (7.1%), leukopenia in 5 (3.6%) and thrombocytopenia in 6 (4.3%). Hematotoxicity was reversible to grade ≤ 2 through a median follow-up of 8 (IQR 9) months in all but two patients who died from disease progression within less than 3 months after RLT.
Click to Show/Hide
|
||||
| Experiment 152 Reporting the Activity Data of This PDC | [42] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Grade ≥ 3 hematological decline |
11%
|
|||
| Patients Enrolled |
45 patients with progressive metastatic castration-resistant prostate cancer and diffuse bone marrow involvement.
|
||||
| Administration Time | 4 cycles | ||||
| Administration Dosage | 7.4 ± 1.4 GBq | ||||
| Evaluation Method | 68Ga-PSMA-11 PET/CT assay | ||||
| MOA of PDC |
Our findings suggest that repeated cycles of RLT with 177Lu-PSMA-617 can be carried out at an acceptable safety profile in mCRPC patients with diffuse bone marrow involvement. RLT may provide a suitable strategy for prolonged disease control with substantial clinical benefit. After a minimum of two cycles, treatment response translated into significantly longer median OS. Further studies should be carried out to investigate the role of individualized RLT concepts in this advanced stage setting.
Click to Show/Hide
|
||||
| Description |
Patients with PR on interim imaging after two cycles had a longer median OS compared to patients with stable or progressive disease (15.5 vs. 7.1 mo, p < 0.001). Previous taxane-based chemotherapy (HR 3.21, 95%CI 1.18-8.70, p = 0.02) and baseline LDH levels (HR 1.001, 95%CI 1.000-1.001, p = 0.04) were inversely associated with OS on a Cox-regression analysis. Grade ≥ 3 hematological decline was observed after 22/201 (11%) cycles with anemia, leukopenia and thrombocytopenia in 15/45 (33%), 6/45 (13%) and 8/45 (18%) patients, respectively.
Click to Show/Hide
|
||||
| Experiment 153 Reporting the Activity Data of This PDC | [35] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Grade ≥ 3 hematological toxicity |
21.40%
|
|||
| Administration Time | Median of 4 (iqr: 2-7) cycles | ||||
| Administration Dosage | Mean cumulative activity of 30.7 ± 23.4 GBq | ||||
| MOA of PDC |
RLT with 177Lu-PSMA-617 can be effectively and safely initiated as early as 8 weeks after failure of 223Ra in patients with progressive bone-metastatic mCRPC refractory to 223Ra. Objective response can be achieved even in patients with more advanced disease and disseminated/diffuse bone metastases, albeit with increasing incidence of significant hematotoxicity.
Click to Show/Hide
|
||||
| Description |
Grade ≥ 3 hematological toxicity was observed in six patients after their last treatment cycle with anemia, leukopenia and thrombocytopenia in 5/28 (17.9%), 4/28 (14.3%) and 6/28 (21.4%) patients, respectively.
|
||||
| In Vivo Model | 28 men with progressive metastatic castration-resistant prostate cancer who median age 73 years, range 63-89 years). | ||||
| Experiment 154 Reporting the Activity Data of This PDC | [14] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Grade ≥3 anemia |
13%
|
|||
| Patients Enrolled |
831 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | Every 6 weeks for 4-6 cycles | ||||
| MOA of PDC |
Radiopharmaceuticals have been used in prostate cancer for decades with known efficacy in palliation of bone metastasis. The FDA approval of the most recent radiopharmaceutical, 177Lu-PSMA-617, shows a clear overall survival benefit compared to the best SOC. Current studies are ongoing to evaluate the effectiveness of 177Lu-PSMA-617 in earlier lines of therapy, such as after only 1 line of therapy with an ARPI as in the PSMAfore study, or in mCSPC in combination with ADT and an ARPI as in the PSMAddition study. Studies are also ongoing with 177Lu-PSMA-617 in combination with other treatments which may produce a synergistic effect. As described, there are many clinical trials ongoing that are modifying the 177Lu-PSMA-617 to possibly achieve improved results. Studies are also ongoing looking at swapping the 177Lu for another radioactive agent, such as 225Ac (an alpha emitter) which may have benefits over the beta-emitting 177Lu. Other studies are looking at J591, a monoclonal antibody to PSMA which has unique differences compared to small-molecule PSMA binders. Overall, PSMA-based radioligand therapy has been shown to be an effective and life-prolonging therapy and should be considered a treatment option for selected men with mCRPC. As described, there are many ongoing studies further evaluating PSMA radioligand therapy in Australia, South Africa, Europe, and the United States, representing a truly global effort to improve prostate cancer care.
Click to Show/Hide
|
||||
| Description |
Toxicities of grade 3 or higher were experienced by 52.7% of patients. The most common all-grade toxicities with 177Lu-PSMA-617 were fatigue (43.1%), dry mouth (38.8%-0% grade 3 or higher), and nausea (35.3%). The most common grade 3 or higher toxicities included anemia (12.9%), thrombocytopenia (7.9%), and leucopenia (7.8%).
|
||||
| Experiment 155 Reporting the Activity Data of This PDC | [14] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Grade ≥3 hematotoxicity |
10%
|
|||
| Patients Enrolled |
10 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 8 weeks | ||||
| MOA of PDC |
Radiopharmaceuticals have been used in prostate cancer for decades with known efficacy in palliation of bone metastasis. The FDA approval of the most recent radiopharmaceutical, 177Lu-PSMA-617, shows a clear overall survival benefit compared to the best SOC. Current studies are ongoing to evaluate the effectiveness of 177Lu-PSMA-617 in earlier lines of therapy, such as after only 1 line of therapy with an ARPI as in the PSMAfore study, or in mCSPC in combination with ADT and an ARPI as in the PSMAddition study. Studies are also ongoing with 177Lu-PSMA-617 in combination with other treatments which may produce a synergistic effect. As described, there are many clinical trials ongoing that are modifying the 177Lu-PSMA-617 to possibly achieve improved results. Studies are also ongoing looking at swapping the 177Lu for another radioactive agent, such as 225Ac (an alpha emitter) which may have benefits over the beta-emitting 177Lu. Other studies are looking at J591, a monoclonal antibody to PSMA which has unique differences compared to small-molecule PSMA binders. Overall, PSMA-based radioligand therapy has been shown to be an effective and life-prolonging therapy and should be considered a treatment option for selected men with mCRPC. As described, there are many ongoing studies further evaluating PSMA radioligand therapy in Australia, South Africa, Europe, and the United States, representing a truly global effort to improve prostate cancer care.
Click to Show/Hide
|
||||
| Description |
Though the first experience with PSMA-targeted 177Lu dates to 2013 at Bad Burka, this experience was not reported until later. The first report on safety and efficacy came from investigators at University Hospital Bonn and University Hospital Muenster. The authors retrospectively evaluated the results of 10 consecutive patients with mCRPC who were treated with a single dose of 177Lu-DKFZ-617 (later called simply PSMA-617) PSMA between 2013 and 2014. They showed that after 8 weeks, 7 patients (70%) showed a PSA decline with 5 patients (50%) having more than a 50% decline in PSA. Grade 3 or higher hematotoxicity was seen in only one patient and there was no relevant nephrotoxicity or hepatotoxicity.
Click to Show/Hide
|
||||
| Experiment 156 Reporting the Activity Data of This PDC | [14] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Grade ≥3 leucopenia |
8%
|
|||
| Patients Enrolled |
831 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | Every 6 weeks for 4-6 cycles | ||||
| MOA of PDC |
Radiopharmaceuticals have been used in prostate cancer for decades with known efficacy in palliation of bone metastasis. The FDA approval of the most recent radiopharmaceutical, 177Lu-PSMA-617, shows a clear overall survival benefit compared to the best SOC. Current studies are ongoing to evaluate the effectiveness of 177Lu-PSMA-617 in earlier lines of therapy, such as after only 1 line of therapy with an ARPI as in the PSMAfore study, or in mCSPC in combination with ADT and an ARPI as in the PSMAddition study. Studies are also ongoing with 177Lu-PSMA-617 in combination with other treatments which may produce a synergistic effect. As described, there are many clinical trials ongoing that are modifying the 177Lu-PSMA-617 to possibly achieve improved results. Studies are also ongoing looking at swapping the 177Lu for another radioactive agent, such as 225Ac (an alpha emitter) which may have benefits over the beta-emitting 177Lu. Other studies are looking at J591, a monoclonal antibody to PSMA which has unique differences compared to small-molecule PSMA binders. Overall, PSMA-based radioligand therapy has been shown to be an effective and life-prolonging therapy and should be considered a treatment option for selected men with mCRPC. As described, there are many ongoing studies further evaluating PSMA radioligand therapy in Australia, South Africa, Europe, and the United States, representing a truly global effort to improve prostate cancer care.
Click to Show/Hide
|
||||
| Description |
Toxicities of grade 3 or higher were experienced by 52.7% of patients. The most common all-grade toxicities with 177Lu-PSMA-617 were fatigue (43.1%), dry mouth (38.8%-0% grade 3 or higher), and nausea (35.3%). The most common grade 3 or higher toxicities included anemia (12.9%), thrombocytopenia (7.9%), and leucopenia (7.8%).
|
||||
| Experiment 157 Reporting the Activity Data of This PDC | [14] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Grade ≥3 xerostomia rate |
0% - 38.8%
|
|||
| Patients Enrolled |
831 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | Every 6 weeks for 4-6 cycles | ||||
| MOA of PDC |
Radiopharmaceuticals have been used in prostate cancer for decades with known efficacy in palliation of bone metastasis. The FDA approval of the most recent radiopharmaceutical, 177Lu-PSMA-617, shows a clear overall survival benefit compared to the best SOC. Current studies are ongoing to evaluate the effectiveness of 177Lu-PSMA-617 in earlier lines of therapy, such as after only 1 line of therapy with an ARPI as in the PSMAfore study, or in mCSPC in combination with ADT and an ARPI as in the PSMAddition study. Studies are also ongoing with 177Lu-PSMA-617 in combination with other treatments which may produce a synergistic effect. As described, there are many clinical trials ongoing that are modifying the 177Lu-PSMA-617 to possibly achieve improved results. Studies are also ongoing looking at swapping the 177Lu for another radioactive agent, such as 225Ac (an alpha emitter) which may have benefits over the beta-emitting 177Lu. Other studies are looking at J591, a monoclonal antibody to PSMA which has unique differences compared to small-molecule PSMA binders. Overall, PSMA-based radioligand therapy has been shown to be an effective and life-prolonging therapy and should be considered a treatment option for selected men with mCRPC. As described, there are many ongoing studies further evaluating PSMA radioligand therapy in Australia, South Africa, Europe, and the United States, representing a truly global effort to improve prostate cancer care.
Click to Show/Hide
|
||||
| Description |
Toxicities of grade 3 or higher were experienced by 52.7% of patients. The most common all-grade toxicities with 177Lu-PSMA-617 were fatigue (43.1%), dry mouth (38.8%-0% grade 3 or higher), and nausea (35.3%). The most common grade 3 or higher toxicities included anemia (12.9%), thrombocytopenia (7.9%), and leucopenia (7.8%).
|
||||
| Experiment 158 Reporting the Activity Data of This PDC | [51] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Grade 1 xerostomia |
14.30%
|
|||
| Patients Enrolled |
91 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 2 cycles | ||||
| Administration Dosage | Median 14.3 GBq, range 9.5-20.2 | ||||
| MOA of PDC |
Salivary gland dysfunction after 177Lu-PSMA-I&T/-617 PRLT has minor clinical relevance, both subjectively and objectively. Even after high cumulative activities, only mild-to-moderate dryness of mouth occurs in a minority of the patients. The prevalence of xerostomia appears to be significantly lower than the historical controls after external radiotherapy, radioiodine therapy, and especially after PRLT with 225Ac-PSMA-617. A validated questionnaire on xerostomia, salivary gland scintigraphy, and PSMA-PET/CT parameters can help to objectify, standardize, and quantify the SG toxicity of PRLT. A decrease of the excretion fraction on SGS and of the metabolic volume on PSMA PET/CT can be early indicators of SG impairment. The co-administration of lower doses of 225Ac in combination with 177Lu-PSMA-617 (Tandem concept) can decrease severe xerostomia after PRLT with alpha-emitters.
Click to Show/Hide
|
||||
| Description |
Grade 1 xerostomia was reported in 13 (14.3%) patients at the baseline and in 22 (24.2%) patients after two cycles of Lu-177 PSMA-I&T/-617 (p < 0.01), with a correlated significant increase of the median sXI-score from 7 (IQR 5.3-9) before to 8 (IQR 6.3-11) after PRLT (p < 0.05). In addition, a moderate correlation of xerostomia symptoms and the sXI-score was found during follow-up (r = 0.43, p < 0.01).
Click to Show/Hide
|
||||
| Experiment 159 Reporting the Activity Data of This PDC | [51] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Grade 1 xerostomia |
37.50%
|
|||
| Patients Enrolled |
40 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | A median of 5.5 (range: 2-9) cycles, median follow up 22.7 months (iqr: 16.4-30.2) | ||||
| Administration Dosage | Median cumulative activity of 35.3 GBq | ||||
| MOA of PDC |
Salivary gland dysfunction after 177Lu-PSMA-I&T/-617 PRLT has minor clinical relevance, both subjectively and objectively. Even after high cumulative activities, only mild-to-moderate dryness of mouth occurs in a minority of the patients. The prevalence of xerostomia appears to be significantly lower than the historical controls after external radiotherapy, radioiodine therapy, and especially after PRLT with 225Ac-PSMA-617. A validated questionnaire on xerostomia, salivary gland scintigraphy, and PSMA-PET/CT parameters can help to objectify, standardize, and quantify the SG toxicity of PRLT. A decrease of the excretion fraction on SGS and of the metabolic volume on PSMA PET/CT can be early indicators of SG impairment. The co-administration of lower doses of 225Ac in combination with 177Lu-PSMA-617 (Tandem concept) can decrease severe xerostomia after PRLT with alpha-emitters.
Click to Show/Hide
|
||||
| Description |
From the baseline to follow-up, xerostomia became more frequent (grade 1 in 2 (5%) patients at baseline, grade 1 in 15 (37.5%) patients, and grade 2 in 1 (2.5%) patient at follow-up; p < 0.001). No grade 3 xerostomia occurred. The data of the sXI questionnaires were available only at the follow-up, showing a moderate but significant correlation to the subjective dryness of mouth (r = 0.41, p < 0.05).
Click to Show/Hide
|
||||
| Experiment 160 Reporting the Activity Data of This PDC | [51] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Grade 1 xerostomia |
55.56%
|
|||
| Patients Enrolled |
18 patients with metastatic castration-resistant prostate cancer treated with tandem-cohort PRLT.
|
||||
| Administration Time | 1 week | ||||
| Administration Dosage | A median activity of 4.25 GBq (range 3.6-7.2 GBq) | ||||
| MOA of PDC |
Salivary gland dysfunction after 177Lu-PSMA-I&T/-617 PRLT has minor clinical relevance, both subjectively and objectively. Even after high cumulative activities, only mild-to-moderate dryness of mouth occurs in a minority of the patients. The prevalence of xerostomia appears to be significantly lower than the historical controls after external radiotherapy, radioiodine therapy, and especially after PRLT with 225Ac-PSMA-617. A validated questionnaire on xerostomia, salivary gland scintigraphy, and PSMA-PET/CT parameters can help to objectify, standardize, and quantify the SG toxicity of PRLT. A decrease of the excretion fraction on SGS and of the metabolic volume on PSMA PET/CT can be early indicators of SG impairment. The co-administration of lower doses of 225Ac in combination with 177Lu-PSMA-617 (Tandem concept) can decrease severe xerostomia after PRLT with alpha-emitters.
Click to Show/Hide
|
||||
| Description |
One-third (6/18) of the patients reported grade 1 xerostomia at the baseline, while, after one cycle of Tandem-PRLT, xerostomia grade 1 in 10/18 patients and grade 2 in 2/18 patients was observed (p = 0.001), and 6/18 patients did not report any xerostomia at the follow-up. There was no patient-requested treatment discontinuation. The sXI-score increased significantly from 9.5 (95%CI: 7.0-14.2) before to 14.0 (95%CI: 11.5-19.6) after Tandem-PRLT (p = 0.005).
Click to Show/Hide
|
||||
| Experiment 161 Reporting the Activity Data of This PDC | [14] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Grade 1 xerostomia rate |
87%
|
|||
| Patients Enrolled |
30 patients with metastatic castration-resistant prostate cancer who underwent 4 cycles of mean 7.5 GBq Lu-PSMA 617 at 6weeks interval.
|
||||
| Administration Time | 4 cycles at 6-week intervals | ||||
| MOA of PDC |
Radiopharmaceuticals have been used in prostate cancer for decades with known efficacy in palliation of bone metastasis. The FDA approval of the most recent radiopharmaceutical, 177Lu-PSMA-617, shows a clear overall survival benefit compared to the best SOC. Current studies are ongoing to evaluate the effectiveness of 177Lu-PSMA-617 in earlier lines of therapy, such as after only 1 line of therapy with an ARPI as in the PSMAfore study, or in mCSPC in combination with ADT and an ARPI as in the PSMAddition study. Studies are also ongoing with 177Lu-PSMA-617 in combination with other treatments which may produce a synergistic effect. As described, there are many clinical trials ongoing that are modifying the 177Lu-PSMA-617 to possibly achieve improved results. Studies are also ongoing looking at swapping the 177Lu for another radioactive agent, such as 225Ac (an alpha emitter) which may have benefits over the beta-emitting 177Lu. Other studies are looking at J591, a monoclonal antibody to PSMA which has unique differences compared to small-molecule PSMA binders. Overall, PSMA-based radioligand therapy has been shown to be an effective and life-prolonging therapy and should be considered a treatment option for selected men with mCRPC. As described, there are many ongoing studies further evaluating PSMA radioligand therapy in Australia, South Africa, Europe, and the United States, representing a truly global effort to improve prostate cancer care.
Click to Show/Hide
|
||||
| Description |
Thirty patients received treatment in this study out of 43 screened patients, thus only 70% of patients were treated. A PSA response was seen in 17 patients (57%). There were no treatment-related deaths in the study and the most common AEs were grade 1 dry mouth in 26 patients (87%), grade 1-2 nausea in 15 patients (50%), and grade 1-2 fatigue in 15 patients (50%).
Click to Show/Hide
|
||||
| Experiment 162 Reporting the Activity Data of This PDC | [52] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Grade 1/2 anemia |
68%
|
|||
| Patients Enrolled |
19 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 45 ± 21 months after all cycles | ||||
| Administration Dosage | A cumulative activity of 32 ± 11 GBq | ||||
| Evaluation Method | 68Ga-PSMA-11 PET/CT assay | ||||
| MOA of PDC |
Intermittent 177Lu-PSMA-617 radioligand therapy in early responders with oligometastatic castration-resistant prostate cancer seems to not compromise survival outcome, despite long treatment-free intervals. The safety profile remained favorable, warranting further investigation of the concept of intermittent treatment in selected patients with a longer life-expectancy.
Click to Show/Hide
|
||||
| Description |
No grade ≥ 3 nephrotoxicity was observed but mean eGFR-levels declined from 80.6 ± 18.0 mL/min/1.73 m2 at baseline to 73.4 ± 15.6 mL/min/1.73 m2 (p = 0.055) at the last follow-up. The mean absorbed renal dose was 0.53 ± 0.21 Gy/GBq, with significant absorbed doses from the first cycle onward, resulting in a cumulative absorbed renal dose of 16.7 ± 8.3 Gy. A significant correlation, however, between the cumulative renal absorbed dose and administered activity (rs = 0.576, p = 0.010) could be observed. Concordantly, in 3/19 (16%) patients with an absorbed renal dose >28 Gy, the administered activity was significantly higher than in patients with <28 Gy of absorbed renal dose (44 ± 7 vs. 30 ± 10 GBq, p = 0.036). No grade ≥ 3 hematological toxicity was observed during intermittent 177Lu-PSMA-RLT or follow-up. Nevertheless, Hb, WBC, and PLT showed an absolute decline throughout the course of intermittent 177Lu-PSMA-RLT. Mean Hb declined from 12.7 ± 1.4 to 12.0 ± 1.6 g/dL (p = 0.021), WBC declined from 7.4 ± 2.8 109/L to 5.9 ± 1.6 109/L (p = 0.005), and PLT declined from 233 ± 76 109/L to 218 ± 71 109/L (p = 0.047). Significant xerostomia was not detected during 177Lu-PSMA-RLT and the follow-up period; one patient developed mild to moderate xerostomia after three treatment cycles, which was not reversible during follow-up.
Click to Show/Hide
|
||||
| Experiment 163 Reporting the Activity Data of This PDC | [52] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Grade 1/2 anemia |
84%
|
|||
| Patients Enrolled |
19 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 5 (iqr: 3-6) cycles | ||||
| Administration Dosage | A cumulative activity of 32 ± 11 GBq | ||||
| Evaluation Method | 68Ga-PSMA-11 PET/CT assay | ||||
| MOA of PDC |
Intermittent 177Lu-PSMA-617 radioligand therapy in early responders with oligometastatic castration-resistant prostate cancer seems to not compromise survival outcome, despite long treatment-free intervals. The safety profile remained favorable, warranting further investigation of the concept of intermittent treatment in selected patients with a longer life-expectancy.
Click to Show/Hide
|
||||
| Description |
No grade ≥ 3 nephrotoxicity was observed but mean eGFR-levels declined from 80.6 ± 18.0 mL/min/1.73 m2 at baseline to 73.4 ± 15.6 mL/min/1.73 m2 (p = 0.055) at the last follow-up. The mean absorbed renal dose was 0.53 ± 0.21 Gy/GBq, with significant absorbed doses from the first cycle onward, resulting in a cumulative absorbed renal dose of 16.7 ± 8.3 Gy. A significant correlation, however, between the cumulative renal absorbed dose and administered activity (rs = 0.576, p = 0.010) could be observed. Concordantly, in 3/19 (16%) patients with an absorbed renal dose >28 Gy, the administered activity was significantly higher than in patients with <28 Gy of absorbed renal dose (44 ± 7 vs. 30 ± 10 GBq, p = 0.036). No grade ≥ 3 hematological toxicity was observed during intermittent 177Lu-PSMA-RLT or follow-up. Nevertheless, Hb, WBC, and PLT showed an absolute decline throughout the course of intermittent 177Lu-PSMA-RLT. Mean Hb declined from 12.7 ± 1.4 to 12.0 ± 1.6 g/dL (p = 0.021), WBC declined from 7.4 ± 2.8 109/L to 5.9 ± 1.6 109/L (p = 0.005), and PLT declined from 233 ± 76 109/L to 218 ± 71 109/L (p = 0.047). Significant xerostomia was not detected during 177Lu-PSMA-RLT and the follow-up period; one patient developed mild to moderate xerostomia after three treatment cycles, which was not reversible during follow-up.
Click to Show/Hide
|
||||
| Experiment 164 Reporting the Activity Data of This PDC | [53] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Grade 1/2 diarrhea |
25.80%
|
|||
| Administration Time | 1-7 cycles | ||||
| Administration Dosage | 7081 MBq (IQR 6995-7188) | ||||
| MOA of PDC |
177Lu-PSMA-RLT in a four-week interval with a fixed dose was safe and effective. A significant PSA response was observed in six out of ten patients, which was also associated with better OS and PFS. A shorter treatment interval may broaden the therapeutic window among mCRPC patients with high volume disease and rapidly rising PSA. Pre-treatment staging PSMA was not helpful in distinguishing responders from non-responders. However, parameters for tumor burden and its activity provide prognostic information related to OS and PFS.
Click to Show/Hide
|
||||
| Description |
In this patient cohort, grade 1-2 hemoglobin values were observed in 57 (91.9%) patients after treatment, but there were no grade 3 hemoglobin values. Grade 1-2 leucopenia was observed in thirteen patients and two patients had grade 3 leucopenia. Grade 1-2 thrombocytopenia was observed in seventeen patients and only one patient had grade 3 trombocytopenia. Tiredness appeared to be the most serious patient-reported adverse event during treatment. Grade 3 tiredness was reported by ten (16.1%) and grade 1-2 tiredness by twenty-seven (43.5%) of the patients. Grade 3 pain was reported by four subjects (6.5%) and grade 3 infection was reported by two subjects. None of the grade 3 pain or infections were related to 177Lu-PSMA-617 treatment. Grade 1-2 dryness of the mouth was reported by thirty-three (53.2%) of the patients. Grade 1-2 nausea was reported by twenty-two (35.5%) and diarrhea by sixteen (25.8%) of the patients. Grade 4-5 side effects were not reported at all.
Click to Show/Hide
|
||||
| In Vivo Model | 62 men with pathologically confirmed castration resistant metastatic prostate cancer. | ||||
| Experiment 165 Reporting the Activity Data of This PDC | [52] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Grade 1/2 eGFR * |
5%
|
|||
| Patients Enrolled |
19 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 45 ± 21 months after all cycles | ||||
| Administration Dosage | A cumulative activity of 32 ± 11 GBq | ||||
| Evaluation Method | 68Ga-PSMA-11 PET/CT assay | ||||
| MOA of PDC |
Intermittent 177Lu-PSMA-617 radioligand therapy in early responders with oligometastatic castration-resistant prostate cancer seems to not compromise survival outcome, despite long treatment-free intervals. The safety profile remained favorable, warranting further investigation of the concept of intermittent treatment in selected patients with a longer life-expectancy.
Click to Show/Hide
|
||||
| Description |
No grade ≥ 3 nephrotoxicity was observed but mean eGFR-levels declined from 80.6 ± 18.0 mL/min/1.73 m2 at baseline to 73.4 ± 15.6 mL/min/1.73 m2 (p = 0.055) at the last follow-up. The mean absorbed renal dose was 0.53 ± 0.21 Gy/GBq, with significant absorbed doses from the first cycle onward, resulting in a cumulative absorbed renal dose of 16.7 ± 8.3 Gy. A significant correlation, however, between the cumulative renal absorbed dose and administered activity (rs = 0.576, p = 0.010) could be observed. Concordantly, in 3/19 (16%) patients with an absorbed renal dose >28 Gy, the administered activity was significantly higher than in patients with <28 Gy of absorbed renal dose (44 ± 7 vs. 30 ± 10 GBq, p = 0.036). No grade ≥ 3 hematological toxicity was observed during intermittent 177Lu-PSMA-RLT or follow-up. Nevertheless, Hb, WBC, and PLT showed an absolute decline throughout the course of intermittent 177Lu-PSMA-RLT. Mean Hb declined from 12.7 ± 1.4 to 12.0 ± 1.6 g/dL (p = 0.021), WBC declined from 7.4 ± 2.8 109/L to 5.9 ± 1.6 109/L (p = 0.005), and PLT declined from 233 ± 76 109/L to 218 ± 71 109/L (p = 0.047). Significant xerostomia was not detected during 177Lu-PSMA-RLT and the follow-up period; one patient developed mild to moderate xerostomia after three treatment cycles, which was not reversible during follow-up.
Click to Show/Hide
|
||||
| Experiment 166 Reporting the Activity Data of This PDC | [52] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Grade 1/2 eGFR * |
16%
|
|||
| Patients Enrolled |
19 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 5 (iqr: 3-6) cycles | ||||
| Administration Dosage | A cumulative activity of 32 ± 11 GBq | ||||
| Evaluation Method | 68Ga-PSMA-11 PET/CT assay | ||||
| MOA of PDC |
Intermittent 177Lu-PSMA-617 radioligand therapy in early responders with oligometastatic castration-resistant prostate cancer seems to not compromise survival outcome, despite long treatment-free intervals. The safety profile remained favorable, warranting further investigation of the concept of intermittent treatment in selected patients with a longer life-expectancy.
Click to Show/Hide
|
||||
| Description |
No grade ≥ 3 nephrotoxicity was observed but mean eGFR-levels declined from 80.6 ± 18.0 mL/min/1.73 m2 at baseline to 73.4 ± 15.6 mL/min/1.73 m2 (p = 0.055) at the last follow-up. The mean absorbed renal dose was 0.53 ± 0.21 Gy/GBq, with significant absorbed doses from the first cycle onward, resulting in a cumulative absorbed renal dose of 16.7 ± 8.3 Gy. A significant correlation, however, between the cumulative renal absorbed dose and administered activity (rs = 0.576, p = 0.010) could be observed. Concordantly, in 3/19 (16%) patients with an absorbed renal dose >28 Gy, the administered activity was significantly higher than in patients with <28 Gy of absorbed renal dose (44 ± 7 vs. 30 ± 10 GBq, p = 0.036). No grade ≥ 3 hematological toxicity was observed during intermittent 177Lu-PSMA-RLT or follow-up. Nevertheless, Hb, WBC, and PLT showed an absolute decline throughout the course of intermittent 177Lu-PSMA-RLT. Mean Hb declined from 12.7 ± 1.4 to 12.0 ± 1.6 g/dL (p = 0.021), WBC declined from 7.4 ± 2.8 109/L to 5.9 ± 1.6 109/L (p = 0.005), and PLT declined from 233 ± 76 109/L to 218 ± 71 109/L (p = 0.047). Significant xerostomia was not detected during 177Lu-PSMA-RLT and the follow-up period; one patient developed mild to moderate xerostomia after three treatment cycles, which was not reversible during follow-up.
Click to Show/Hide
|
||||
| Experiment 167 Reporting the Activity Data of This PDC | [14] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Grade 1/2 fatigue |
50%
|
|||
| Patients Enrolled |
30 patients with metastatic castration-resistant prostate cancer who underwent 4 cycles of mean 7.5 GBq Lu-PSMA 617 at 6weeks interval.
|
||||
| Administration Time | 4 cycles at 6-week intervals | ||||
| MOA of PDC |
Radiopharmaceuticals have been used in prostate cancer for decades with known efficacy in palliation of bone metastasis. The FDA approval of the most recent radiopharmaceutical, 177Lu-PSMA-617, shows a clear overall survival benefit compared to the best SOC. Current studies are ongoing to evaluate the effectiveness of 177Lu-PSMA-617 in earlier lines of therapy, such as after only 1 line of therapy with an ARPI as in the PSMAfore study, or in mCSPC in combination with ADT and an ARPI as in the PSMAddition study. Studies are also ongoing with 177Lu-PSMA-617 in combination with other treatments which may produce a synergistic effect. As described, there are many clinical trials ongoing that are modifying the 177Lu-PSMA-617 to possibly achieve improved results. Studies are also ongoing looking at swapping the 177Lu for another radioactive agent, such as 225Ac (an alpha emitter) which may have benefits over the beta-emitting 177Lu. Other studies are looking at J591, a monoclonal antibody to PSMA which has unique differences compared to small-molecule PSMA binders. Overall, PSMA-based radioligand therapy has been shown to be an effective and life-prolonging therapy and should be considered a treatment option for selected men with mCRPC. As described, there are many ongoing studies further evaluating PSMA radioligand therapy in Australia, South Africa, Europe, and the United States, representing a truly global effort to improve prostate cancer care.
Click to Show/Hide
|
||||
| Description |
Thirty patients received treatment in this study out of 43 screened patients, thus only 70% of patients were treated. A PSA response was seen in 17 patients (57%). There were no treatment-related deaths in the study and the most common AEs were grade 1 dry mouth in 26 patients (87%), grade 1-2 nausea in 15 patients (50%), and grade 1-2 fatigue in 15 patients (50%).
Click to Show/Hide
|
||||
| Experiment 168 Reporting the Activity Data of This PDC | [53] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Grade 1/2 hemoglobin |
91.90%
|
|||
| Patients Enrolled |
This is a single-center retrospective analysis in 62 men with pathologically confirmed castration resistant metastatic prostate cancer who were treated with <sup>177</sup>Lu-PSMA-617 during January 2017-February 2019. Grade 1-2 hemoglobin values were observed in 57 (91.9%) patients after treatment.
|
||||
| Administration Time | 1-7 cycles | ||||
| Administration Dosage | 7081 MBq (IQR 6995-7188) | ||||
| MOA of PDC |
177Lu-PSMA-RLT in a four-week interval with a fixed dose was safe and effective. A significant PSA response was observed in six out of ten patients, which was also associated with better OS and PFS. A shorter treatment interval may broaden the therapeutic window among mCRPC patients with high volume disease and rapidly rising PSA. Pre-treatment staging PSMA was not helpful in distinguishing responders from non-responders. However, parameters for tumor burden and its activity provide prognostic information related to OS and PFS.
Click to Show/Hide
|
||||
| Description |
In this patient cohort, grade 1-2 hemoglobin values were observed in 57 (91.9%) patients after treatment, but there were no grade 3 hemoglobin values. Grade 1-2 leucopenia was observed in thirteen patients and two patients had grade 3 leucopenia. Grade 1-2 thrombocytopenia was observed in seventeen patients and only one patient had grade 3 trombocytopenia. Tiredness appeared to be the most serious patient-reported adverse event during treatment. Grade 3 tiredness was reported by ten (16.1%) and grade 1-2 tiredness by twenty-seven (43.5%) of the patients. Grade 3 pain was reported by four subjects (6.5%) and grade 3 infection was reported by two subjects. None of the grade 3 pain or infections were related to 177Lu-PSMA-617 treatment. Grade 1-2 dryness of the mouth was reported by thirty-three (53.2%) of the patients. Grade 1-2 nausea was reported by twenty-two (35.5%) and diarrhea by sixteen (25.8%) of the patients. Grade 4-5 side effects were not reported at all.
Click to Show/Hide
|
||||
| Experiment 169 Reporting the Activity Data of This PDC | [53] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Grade 1/2 leucopenia |
21.00%
|
|||
| Patients Enrolled |
This is a single-center retrospective analysis in 62 men with pathologically confirmed castration resistant metastatic prostate cancer who were treated with <sup>177</sup>Lu-PSMA-617 during January 2017-February 2019. Grade 1-2 leucopenia was observed in thirteen patients.
|
||||
| Administration Time | 1-7 cycles | ||||
| Administration Dosage | 7081 MBq (IQR 6995-7188) | ||||
| MOA of PDC |
177Lu-PSMA-RLT in a four-week interval with a fixed dose was safe and effective. A significant PSA response was observed in six out of ten patients, which was also associated with better OS and PFS. A shorter treatment interval may broaden the therapeutic window among mCRPC patients with high volume disease and rapidly rising PSA. Pre-treatment staging PSMA was not helpful in distinguishing responders from non-responders. However, parameters for tumor burden and its activity provide prognostic information related to OS and PFS.
Click to Show/Hide
|
||||
| Description |
In this patient cohort, grade 1-2 hemoglobin values were observed in 57 (91.9%) patients after treatment, but there were no grade 3 hemoglobin values. Grade 1-2 leucopenia was observed in thirteen patients and two patients had grade 3 leucopenia. Grade 1-2 thrombocytopenia was observed in seventeen patients and only one patient had grade 3 trombocytopenia. Tiredness appeared to be the most serious patient-reported adverse event during treatment. Grade 3 tiredness was reported by ten (16.1%) and grade 1-2 tiredness by twenty-seven (43.5%) of the patients. Grade 3 pain was reported by four subjects (6.5%) and grade 3 infection was reported by two subjects. None of the grade 3 pain or infections were related to 177Lu-PSMA-617 treatment. Grade 1-2 dryness of the mouth was reported by thirty-three (53.2%) of the patients. Grade 1-2 nausea was reported by twenty-two (35.5%) and diarrhea by sixteen (25.8%) of the patients. Grade 4-5 side effects were not reported at all.
Click to Show/Hide
|
||||
| Experiment 170 Reporting the Activity Data of This PDC | [52] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Grade 1/2 leukopenia |
5%
|
|||
| Patients Enrolled |
19 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 45 ± 21 months after all cycles | ||||
| Administration Dosage | A cumulative activity of 32 ± 11 GBq | ||||
| Evaluation Method | 68Ga-PSMA-11 PET/CT assay | ||||
| MOA of PDC |
Intermittent 177Lu-PSMA-617 radioligand therapy in early responders with oligometastatic castration-resistant prostate cancer seems to not compromise survival outcome, despite long treatment-free intervals. The safety profile remained favorable, warranting further investigation of the concept of intermittent treatment in selected patients with a longer life-expectancy.
Click to Show/Hide
|
||||
| Description |
No grade ≥ 3 nephrotoxicity was observed but mean eGFR-levels declined from 80.6 ± 18.0 mL/min/1.73 m2 at baseline to 73.4 ± 15.6 mL/min/1.73 m2 (p = 0.055) at the last follow-up. The mean absorbed renal dose was 0.53 ± 0.21 Gy/GBq, with significant absorbed doses from the first cycle onward, resulting in a cumulative absorbed renal dose of 16.7 ± 8.3 Gy. A significant correlation, however, between the cumulative renal absorbed dose and administered activity (rs = 0.576, p = 0.010) could be observed. Concordantly, in 3/19 (16%) patients with an absorbed renal dose >28 Gy, the administered activity was significantly higher than in patients with <28 Gy of absorbed renal dose (44 ± 7 vs. 30 ± 10 GBq, p = 0.036). No grade ≥ 3 hematological toxicity was observed during intermittent 177Lu-PSMA-RLT or follow-up. Nevertheless, Hb, WBC, and PLT showed an absolute decline throughout the course of intermittent 177Lu-PSMA-RLT. Mean Hb declined from 12.7 ± 1.4 to 12.0 ± 1.6 g/dL (p = 0.021), WBC declined from 7.4 ± 2.8 109/L to 5.9 ± 1.6 109/L (p = 0.005), and PLT declined from 233 ± 76 109/L to 218 ± 71 109/L (p = 0.047). Significant xerostomia was not detected during 177Lu-PSMA-RLT and the follow-up period; one patient developed mild to moderate xerostomia after three treatment cycles, which was not reversible during follow-up.
Click to Show/Hide
|
||||
| Experiment 171 Reporting the Activity Data of This PDC | [52] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Grade 1/2 leukopenia |
16%
|
|||
| Patients Enrolled |
19 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 5 (iqr: 3-6) cycles | ||||
| Administration Dosage | A cumulative activity of 32 ± 11 GBq | ||||
| Evaluation Method | 68Ga-PSMA-11 PET/CT assay | ||||
| MOA of PDC |
Intermittent 177Lu-PSMA-617 radioligand therapy in early responders with oligometastatic castration-resistant prostate cancer seems to not compromise survival outcome, despite long treatment-free intervals. The safety profile remained favorable, warranting further investigation of the concept of intermittent treatment in selected patients with a longer life-expectancy.
Click to Show/Hide
|
||||
| Description |
No grade ≥ 3 nephrotoxicity was observed but mean eGFR-levels declined from 80.6 ± 18.0 mL/min/1.73 m2 at baseline to 73.4 ± 15.6 mL/min/1.73 m2 (p = 0.055) at the last follow-up. The mean absorbed renal dose was 0.53 ± 0.21 Gy/GBq, with significant absorbed doses from the first cycle onward, resulting in a cumulative absorbed renal dose of 16.7 ± 8.3 Gy. A significant correlation, however, between the cumulative renal absorbed dose and administered activity (rs = 0.576, p = 0.010) could be observed. Concordantly, in 3/19 (16%) patients with an absorbed renal dose >28 Gy, the administered activity was significantly higher than in patients with <28 Gy of absorbed renal dose (44 ± 7 vs. 30 ± 10 GBq, p = 0.036). No grade ≥ 3 hematological toxicity was observed during intermittent 177Lu-PSMA-RLT or follow-up. Nevertheless, Hb, WBC, and PLT showed an absolute decline throughout the course of intermittent 177Lu-PSMA-RLT. Mean Hb declined from 12.7 ± 1.4 to 12.0 ± 1.6 g/dL (p = 0.021), WBC declined from 7.4 ± 2.8 109/L to 5.9 ± 1.6 109/L (p = 0.005), and PLT declined from 233 ± 76 109/L to 218 ± 71 109/L (p = 0.047). Significant xerostomia was not detected during 177Lu-PSMA-RLT and the follow-up period; one patient developed mild to moderate xerostomia after three treatment cycles, which was not reversible during follow-up.
Click to Show/Hide
|
||||
| Experiment 172 Reporting the Activity Data of This PDC | [53] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Grade 1/2 nausea |
35.50%
|
|||
| Administration Time | 1-7 cycles | ||||
| Administration Dosage | 7081 MBq (IQR 6995-7188) | ||||
| MOA of PDC |
177Lu-PSMA-RLT in a four-week interval with a fixed dose was safe and effective. A significant PSA response was observed in six out of ten patients, which was also associated with better OS and PFS. A shorter treatment interval may broaden the therapeutic window among mCRPC patients with high volume disease and rapidly rising PSA. Pre-treatment staging PSMA was not helpful in distinguishing responders from non-responders. However, parameters for tumor burden and its activity provide prognostic information related to OS and PFS.
Click to Show/Hide
|
||||
| Description |
In this patient cohort, grade 1-2 hemoglobin values were observed in 57 (91.9%) patients after treatment, but there were no grade 3 hemoglobin values. Grade 1-2 leucopenia was observed in thirteen patients and two patients had grade 3 leucopenia. Grade 1-2 thrombocytopenia was observed in seventeen patients and only one patient had grade 3 trombocytopenia. Tiredness appeared to be the most serious patient-reported adverse event during treatment. Grade 3 tiredness was reported by ten (16.1%) and grade 1-2 tiredness by twenty-seven (43.5%) of the patients. Grade 3 pain was reported by four subjects (6.5%) and grade 3 infection was reported by two subjects. None of the grade 3 pain or infections were related to 177Lu-PSMA-617 treatment. Grade 1-2 dryness of the mouth was reported by thirty-three (53.2%) of the patients. Grade 1-2 nausea was reported by twenty-two (35.5%) and diarrhea by sixteen (25.8%) of the patients. Grade 4-5 side effects were not reported at all.
Click to Show/Hide
|
||||
| In Vivo Model | This is a single-center retrospective analysis in 62 men with pathologically confirmed castration resistant metastatic prostate cancer who were treated with 177Lu-PSMA-617 during January 2017-February 2019. Grade 1-2 nausea was reported by twenty-two (35.5%). | ||||
| Experiment 173 Reporting the Activity Data of This PDC | [14] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Grade 1/2 nausea |
50%
|
|||
| Patients Enrolled |
30 patients with metastatic castration-resistant prostate cancer who underwent 4 cycles of mean 7.5 GBq Lu-PSMA 617 at 6weeks interval.
|
||||
| Administration Time | 4 cycles at 6-week intervals | ||||
| MOA of PDC |
Radiopharmaceuticals have been used in prostate cancer for decades with known efficacy in palliation of bone metastasis. The FDA approval of the most recent radiopharmaceutical, 177Lu-PSMA-617, shows a clear overall survival benefit compared to the best SOC. Current studies are ongoing to evaluate the effectiveness of 177Lu-PSMA-617 in earlier lines of therapy, such as after only 1 line of therapy with an ARPI as in the PSMAfore study, or in mCSPC in combination with ADT and an ARPI as in the PSMAddition study. Studies are also ongoing with 177Lu-PSMA-617 in combination with other treatments which may produce a synergistic effect. As described, there are many clinical trials ongoing that are modifying the 177Lu-PSMA-617 to possibly achieve improved results. Studies are also ongoing looking at swapping the 177Lu for another radioactive agent, such as 225Ac (an alpha emitter) which may have benefits over the beta-emitting 177Lu. Other studies are looking at J591, a monoclonal antibody to PSMA which has unique differences compared to small-molecule PSMA binders. Overall, PSMA-based radioligand therapy has been shown to be an effective and life-prolonging therapy and should be considered a treatment option for selected men with mCRPC. As described, there are many ongoing studies further evaluating PSMA radioligand therapy in Australia, South Africa, Europe, and the United States, representing a truly global effort to improve prostate cancer care.
Click to Show/Hide
|
||||
| Description |
Thirty patients received treatment in this study out of 43 screened patients, thus only 70% of patients were treated. A PSA response was seen in 17 patients (57%). There were no treatment-related deaths in the study and the most common AEs were grade 1 dry mouth in 26 patients (87%), grade 1-2 nausea in 15 patients (50%), and grade 1-2 fatigue in 15 patients (50%).
Click to Show/Hide
|
||||
| Experiment 174 Reporting the Activity Data of This PDC | [52] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Grade 1/2 thrombocytopenia |
15%
|
|||
| Patients Enrolled |
19 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 45 ± 21 months after all cycles | ||||
| Administration Dosage | A cumulative activity of 32 ± 11 GBq | ||||
| Evaluation Method | 68Ga-PSMA-11 PET/CT assay | ||||
| MOA of PDC |
Intermittent 177Lu-PSMA-617 radioligand therapy in early responders with oligometastatic castration-resistant prostate cancer seems to not compromise survival outcome, despite long treatment-free intervals. The safety profile remained favorable, warranting further investigation of the concept of intermittent treatment in selected patients with a longer life-expectancy.
Click to Show/Hide
|
||||
| Description |
No grade ≥ 3 nephrotoxicity was observed but mean eGFR-levels declined from 80.6 ± 18.0 mL/min/1.73 m2 at baseline to 73.4 ± 15.6 mL/min/1.73 m2 (p = 0.055) at the last follow-up. The mean absorbed renal dose was 0.53 ± 0.21 Gy/GBq, with significant absorbed doses from the first cycle onward, resulting in a cumulative absorbed renal dose of 16.7 ± 8.3 Gy. A significant correlation, however, between the cumulative renal absorbed dose and administered activity (rs = 0.576, p = 0.010) could be observed. Concordantly, in 3/19 (16%) patients with an absorbed renal dose >28 Gy, the administered activity was significantly higher than in patients with <28 Gy of absorbed renal dose (44 ± 7 vs. 30 ± 10 GBq, p = 0.036). No grade ≥ 3 hematological toxicity was observed during intermittent 177Lu-PSMA-RLT or follow-up. Nevertheless, Hb, WBC, and PLT showed an absolute decline throughout the course of intermittent 177Lu-PSMA-RLT. Mean Hb declined from 12.7 ± 1.4 to 12.0 ± 1.6 g/dL (p = 0.021), WBC declined from 7.4 ± 2.8 109/L to 5.9 ± 1.6 109/L (p = 0.005), and PLT declined from 233 ± 76 109/L to 218 ± 71 109/L (p = 0.047). Significant xerostomia was not detected during 177Lu-PSMA-RLT and the follow-up period; one patient developed mild to moderate xerostomia after three treatment cycles, which was not reversible during follow-up.
Click to Show/Hide
|
||||
| Experiment 175 Reporting the Activity Data of This PDC | [53] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Grade 1/2 thrombocytopenia |
27.40%
|
|||
| Patients Enrolled |
This is a single-center retrospective analysis in 62 men with pathologically confirmed castration resistant metastatic prostate cancer who were treated with <sup>177</sup>Lu-PSMA-617 during January 2017-February 2019. Only one patient had grade 3 trombocytopenia.
|
||||
| Administration Time | 1-7 cycles | ||||
| Administration Dosage | 7081 MBq (IQR 6995-7188) | ||||
| MOA of PDC |
177Lu-PSMA-RLT in a four-week interval with a fixed dose was safe and effective. A significant PSA response was observed in six out of ten patients, which was also associated with better OS and PFS. A shorter treatment interval may broaden the therapeutic window among mCRPC patients with high volume disease and rapidly rising PSA. Pre-treatment staging PSMA was not helpful in distinguishing responders from non-responders. However, parameters for tumor burden and its activity provide prognostic information related to OS and PFS.
Click to Show/Hide
|
||||
| Description |
In this patient cohort, grade 1-2 hemoglobin values were observed in 57 (91.9%) patients after treatment, but there were no grade 3 hemoglobin values. Grade 1-2 leucopenia was observed in thirteen patients and two patients had grade 3 leucopenia. Grade 1-2 thrombocytopenia was observed in seventeen patients and only one patient had grade 3 trombocytopenia. Tiredness appeared to be the most serious patient-reported adverse event during treatment. Grade 3 tiredness was reported by ten (16.1%) and grade 1-2 tiredness by twenty-seven (43.5%) of the patients. Grade 3 pain was reported by four subjects (6.5%) and grade 3 infection was reported by two subjects. None of the grade 3 pain or infections were related to 177Lu-PSMA-617 treatment. Grade 1-2 dryness of the mouth was reported by thirty-three (53.2%) of the patients. Grade 1-2 nausea was reported by twenty-two (35.5%) and diarrhea by sixteen (25.8%) of the patients. Grade 4-5 side effects were not reported at all.
Click to Show/Hide
|
||||
| Experiment 176 Reporting the Activity Data of This PDC | [52] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Grade 1/2 thrombocytopenia |
32%
|
|||
| Patients Enrolled |
19 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 5 (iqr: 3-6) cycles | ||||
| Administration Dosage | A cumulative activity of 32 ± 11 GBq | ||||
| Evaluation Method | 68Ga-PSMA-11 PET/CT assay | ||||
| MOA of PDC |
Intermittent 177Lu-PSMA-617 radioligand therapy in early responders with oligometastatic castration-resistant prostate cancer seems to not compromise survival outcome, despite long treatment-free intervals. The safety profile remained favorable, warranting further investigation of the concept of intermittent treatment in selected patients with a longer life-expectancy.
Click to Show/Hide
|
||||
| Description |
No grade ≥ 3 nephrotoxicity was observed but mean eGFR-levels declined from 80.6 ± 18.0 mL/min/1.73 m2 at baseline to 73.4 ± 15.6 mL/min/1.73 m2 (p = 0.055) at the last follow-up. The mean absorbed renal dose was 0.53 ± 0.21 Gy/GBq, with significant absorbed doses from the first cycle onward, resulting in a cumulative absorbed renal dose of 16.7 ± 8.3 Gy. A significant correlation, however, between the cumulative renal absorbed dose and administered activity (rs = 0.576, p = 0.010) could be observed. Concordantly, in 3/19 (16%) patients with an absorbed renal dose >28 Gy, the administered activity was significantly higher than in patients with <28 Gy of absorbed renal dose (44 ± 7 vs. 30 ± 10 GBq, p = 0.036). No grade ≥ 3 hematological toxicity was observed during intermittent 177Lu-PSMA-RLT or follow-up. Nevertheless, Hb, WBC, and PLT showed an absolute decline throughout the course of intermittent 177Lu-PSMA-RLT. Mean Hb declined from 12.7 ± 1.4 to 12.0 ± 1.6 g/dL (p = 0.021), WBC declined from 7.4 ± 2.8 109/L to 5.9 ± 1.6 109/L (p = 0.005), and PLT declined from 233 ± 76 109/L to 218 ± 71 109/L (p = 0.047). Significant xerostomia was not detected during 177Lu-PSMA-RLT and the follow-up period; one patient developed mild to moderate xerostomia after three treatment cycles, which was not reversible during follow-up.
Click to Show/Hide
|
||||
| Experiment 177 Reporting the Activity Data of This PDC | [53] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Grade 1/2 tiredness |
43.50%
|
|||
| Patients Enrolled |
This is a single-center retrospective analysis in 62 men with pathologically confirmed castration resistant metastatic prostate cancer who were treated with <sup>177</sup>Lu-PSMA-617 during January 2017-February 2019. Grade 1-2 tiredness by twenty-seven (43.5%) of the patients.
|
||||
| Administration Time | 1-7 cycles | ||||
| Administration Dosage | 7081 MBq (IQR 6995-7188) | ||||
| MOA of PDC |
177Lu-PSMA-RLT in a four-week interval with a fixed dose was safe and effective. A significant PSA response was observed in six out of ten patients, which was also associated with better OS and PFS. A shorter treatment interval may broaden the therapeutic window among mCRPC patients with high volume disease and rapidly rising PSA. Pre-treatment staging PSMA was not helpful in distinguishing responders from non-responders. However, parameters for tumor burden and its activity provide prognostic information related to OS and PFS.
Click to Show/Hide
|
||||
| Description |
In this patient cohort, grade 1-2 hemoglobin values were observed in 57 (91.9%) patients after treatment, but there were no grade 3 hemoglobin values. Grade 1-2 leucopenia was observed in thirteen patients and two patients had grade 3 leucopenia. Grade 1-2 thrombocytopenia was observed in seventeen patients and only one patient had grade 3 trombocytopenia. Tiredness appeared to be the most serious patient-reported adverse event during treatment. Grade 3 tiredness was reported by ten (16.1%) and grade 1-2 tiredness by twenty-seven (43.5%) of the patients. Grade 3 pain was reported by four subjects (6.5%) and grade 3 infection was reported by two subjects. None of the grade 3 pain or infections were related to 177Lu-PSMA-617 treatment. Grade 1-2 dryness of the mouth was reported by thirty-three (53.2%) of the patients. Grade 1-2 nausea was reported by twenty-two (35.5%) and diarrhea by sixteen (25.8%) of the patients. Grade 4-5 side effects were not reported at all.
Click to Show/Hide
|
||||
| Experiment 178 Reporting the Activity Data of This PDC | [52] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Grade 1/2 xerostomia |
5%
|
|||
| Patients Enrolled |
19 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 5 (iqr: 3-6) cycles | ||||
| Administration Dosage | A cumulative activity of 32 ± 11 GBq | ||||
| Evaluation Method | 68Ga-PSMA-11 PET/CT assay | ||||
| MOA of PDC |
Intermittent 177Lu-PSMA-617 radioligand therapy in early responders with oligometastatic castration-resistant prostate cancer seems to not compromise survival outcome, despite long treatment-free intervals. The safety profile remained favorable, warranting further investigation of the concept of intermittent treatment in selected patients with a longer life-expectancy.
Click to Show/Hide
|
||||
| Description |
No grade ≥ 3 nephrotoxicity was observed but mean eGFR-levels declined from 80.6 ± 18.0 mL/min/1.73 m2 at baseline to 73.4 ± 15.6 mL/min/1.73 m2 (p = 0.055) at the last follow-up. The mean absorbed renal dose was 0.53 ± 0.21 Gy/GBq, with significant absorbed doses from the first cycle onward, resulting in a cumulative absorbed renal dose of 16.7 ± 8.3 Gy. A significant correlation, however, between the cumulative renal absorbed dose and administered activity (rs = 0.576, p = 0.010) could be observed. Concordantly, in 3/19 (16%) patients with an absorbed renal dose >28 Gy, the administered activity was significantly higher than in patients with <28 Gy of absorbed renal dose (44 ± 7 vs. 30 ± 10 GBq, p = 0.036). No grade ≥ 3 hematological toxicity was observed during intermittent 177Lu-PSMA-RLT or follow-up. Nevertheless, Hb, WBC, and PLT showed an absolute decline throughout the course of intermittent 177Lu-PSMA-RLT. Mean Hb declined from 12.7 ± 1.4 to 12.0 ± 1.6 g/dL (p = 0.021), WBC declined from 7.4 ± 2.8 109/L to 5.9 ± 1.6 109/L (p = 0.005), and PLT declined from 233 ± 76 109/L to 218 ± 71 109/L (p = 0.047). Significant xerostomia was not detected during 177Lu-PSMA-RLT and the follow-up period; one patient developed mild to moderate xerostomia after three treatment cycles, which was not reversible during follow-up.
Click to Show/Hide
|
||||
| Experiment 179 Reporting the Activity Data of This PDC | [52] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Grade 1/2 xerostomia |
5%
|
|||
| Patients Enrolled |
19 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 45 ± 21 months after all cycles | ||||
| Administration Dosage | A cumulative activity of 32 ± 11 GBq | ||||
| Evaluation Method | 68Ga-PSMA-11 PET/CT assay | ||||
| MOA of PDC |
Intermittent 177Lu-PSMA-617 radioligand therapy in early responders with oligometastatic castration-resistant prostate cancer seems to not compromise survival outcome, despite long treatment-free intervals. The safety profile remained favorable, warranting further investigation of the concept of intermittent treatment in selected patients with a longer life-expectancy.
Click to Show/Hide
|
||||
| Description |
No grade ≥ 3 nephrotoxicity was observed but mean eGFR-levels declined from 80.6 ± 18.0 mL/min/1.73 m2 at baseline to 73.4 ± 15.6 mL/min/1.73 m2 (p = 0.055) at the last follow-up. The mean absorbed renal dose was 0.53 ± 0.21 Gy/GBq, with significant absorbed doses from the first cycle onward, resulting in a cumulative absorbed renal dose of 16.7 ± 8.3 Gy. A significant correlation, however, between the cumulative renal absorbed dose and administered activity (rs = 0.576, p = 0.010) could be observed. Concordantly, in 3/19 (16%) patients with an absorbed renal dose >28 Gy, the administered activity was significantly higher than in patients with <28 Gy of absorbed renal dose (44 ± 7 vs. 30 ± 10 GBq, p = 0.036). No grade ≥ 3 hematological toxicity was observed during intermittent 177Lu-PSMA-RLT or follow-up. Nevertheless, Hb, WBC, and PLT showed an absolute decline throughout the course of intermittent 177Lu-PSMA-RLT. Mean Hb declined from 12.7 ± 1.4 to 12.0 ± 1.6 g/dL (p = 0.021), WBC declined from 7.4 ± 2.8 109/L to 5.9 ± 1.6 109/L (p = 0.005), and PLT declined from 233 ± 76 109/L to 218 ± 71 109/L (p = 0.047). Significant xerostomia was not detected during 177Lu-PSMA-RLT and the follow-up period; one patient developed mild to moderate xerostomia after three treatment cycles, which was not reversible during follow-up.
Click to Show/Hide
|
||||
| Experiment 180 Reporting the Activity Data of This PDC | [53] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Grade 1/2 xerostomia |
53.20%
|
|||
| Patients Enrolled |
This is a single-center retrospective analysis in 62 men with pathologically confirmed castration resistant metastatic prostate cancer who were treated with <sup>177</sup>Lu-PSMA-617 during January 2017-February 2019. Grade 1-2 dryness of the mouth was reported by thirty-three (53.2%) of the patients.
|
||||
| Administration Time | 1-7 cycles | ||||
| Administration Dosage | 7081 MBq (IQR 6995-7188) | ||||
| MOA of PDC |
177Lu-PSMA-RLT in a four-week interval with a fixed dose was safe and effective. A significant PSA response was observed in six out of ten patients, which was also associated with better OS and PFS. A shorter treatment interval may broaden the therapeutic window among mCRPC patients with high volume disease and rapidly rising PSA. Pre-treatment staging PSMA was not helpful in distinguishing responders from non-responders. However, parameters for tumor burden and its activity provide prognostic information related to OS and PFS.
Click to Show/Hide
|
||||
| Description |
In this patient cohort, grade 1-2 hemoglobin values were observed in 57 (91.9%) patients after treatment, but there were no grade 3 hemoglobin values. Grade 1-2 leucopenia was observed in thirteen patients and two patients had grade 3 leucopenia. Grade 1-2 thrombocytopenia was observed in seventeen patients and only one patient had grade 3 trombocytopenia. Tiredness appeared to be the most serious patient-reported adverse event during treatment. Grade 3 tiredness was reported by ten (16.1%) and grade 1-2 tiredness by twenty-seven (43.5%) of the patients. Grade 3 pain was reported by four subjects (6.5%) and grade 3 infection was reported by two subjects. None of the grade 3 pain or infections were related to 177Lu-PSMA-617 treatment. Grade 1-2 dryness of the mouth was reported by thirty-three (53.2%) of the patients. Grade 1-2 nausea was reported by twenty-two (35.5%) and diarrhea by sixteen (25.8%) of the patients. Grade 4-5 side effects were not reported at all.
Click to Show/Hide
|
||||
| Experiment 181 Reporting the Activity Data of This PDC | [51] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Grade 2 xerostomia |
2.50%
|
|||
| Patients Enrolled |
40 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | A median of 5.5 (range: 2-9) cycles, median follow up 22.7 months (iqr: 16.4-30.2) | ||||
| Administration Dosage | Median cumulative activity of 35.3 GBq | ||||
| MOA of PDC |
Salivary gland dysfunction after 177Lu-PSMA-I&T/-617 PRLT has minor clinical relevance, both subjectively and objectively. Even after high cumulative activities, only mild-to-moderate dryness of mouth occurs in a minority of the patients. The prevalence of xerostomia appears to be significantly lower than the historical controls after external radiotherapy, radioiodine therapy, and especially after PRLT with 225Ac-PSMA-617. A validated questionnaire on xerostomia, salivary gland scintigraphy, and PSMA-PET/CT parameters can help to objectify, standardize, and quantify the SG toxicity of PRLT. A decrease of the excretion fraction on SGS and of the metabolic volume on PSMA PET/CT can be early indicators of SG impairment. The co-administration of lower doses of 225Ac in combination with 177Lu-PSMA-617 (Tandem concept) can decrease severe xerostomia after PRLT with alpha-emitters.
Click to Show/Hide
|
||||
| Description |
From the baseline to follow-up, xerostomia became more frequent (grade 1 in 2 (5%) patients at baseline, grade 1 in 15 (37.5%) patients, and grade 2 in 1 (2.5%) patient at follow-up; p < 0.001). No grade 3 xerostomia occurred. The data of the sXI questionnaires were available only at the follow-up, showing a moderate but significant correlation to the subjective dryness of mouth (r = 0.41, p < 0.05).
Click to Show/Hide
|
||||
| Experiment 182 Reporting the Activity Data of This PDC | [51] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Grade 2 xerostomia |
11.11%
|
|||
| Patients Enrolled |
18 patients with metastatic castration-resistant prostate cancer treated with tandem-cohort PRLT.
|
||||
| Administration Time | 1 week | ||||
| Administration Dosage | A median activity of 4.25 GBq (range 3.6-7.2 GBq) | ||||
| MOA of PDC |
Salivary gland dysfunction after 177Lu-PSMA-I&T/-617 PRLT has minor clinical relevance, both subjectively and objectively. Even after high cumulative activities, only mild-to-moderate dryness of mouth occurs in a minority of the patients. The prevalence of xerostomia appears to be significantly lower than the historical controls after external radiotherapy, radioiodine therapy, and especially after PRLT with 225Ac-PSMA-617. A validated questionnaire on xerostomia, salivary gland scintigraphy, and PSMA-PET/CT parameters can help to objectify, standardize, and quantify the SG toxicity of PRLT. A decrease of the excretion fraction on SGS and of the metabolic volume on PSMA PET/CT can be early indicators of SG impairment. The co-administration of lower doses of 225Ac in combination with 177Lu-PSMA-617 (Tandem concept) can decrease severe xerostomia after PRLT with alpha-emitters.
Click to Show/Hide
|
||||
| Description |
One-third (6/18) of the patients reported grade 1 xerostomia at the baseline, while, after one cycle of Tandem-PRLT, xerostomia grade 1 in 10/18 patients and grade 2 in 2/18 patients was observed (p = 0.001), and 6/18 patients did not report any xerostomia at the follow-up. There was no patient-requested treatment discontinuation. The sXI-score increased significantly from 9.5 (95%CI: 7.0-14.2) before to 14.0 (95%CI: 11.5-19.6) after Tandem-PRLT (p = 0.005).
Click to Show/Hide
|
||||
| Experiment 183 Reporting the Activity Data of This PDC | [44] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Grade 3 anaemia |
8%
|
|||
| Patients Enrolled |
64 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 2 cycles | ||||
| Administration Dosage | Cumulative mean activity of 11.5 (8.1-14.9) GBq | ||||
| MOA of PDC |
In general, the first two cycles of PSMA-RLT were well tolerated haematologically. Qualitative and quantitative bone marrow impairment appears closely associated with osseous tumour burden as only patients with advanced bone involvement and non-response to therapy exhibited high-grade haematological adverse events as well as a significant mean decline of haematological parameters. This implies that in patients with already advanced mCRPC, non-response to PSMA-RLT may be a major cause of bone marrow impairment during early treatment cycles.
Click to Show/Hide
|
||||
| Description |
In addition, lower grade thrombopenia and leukopenia were observed in 9 (14%) and 11 (17%) patients at baseline, respectively. During the observation period, severe (grade 3) anaemia, thrombopenia and leukopenia occurred in 5 (8%), 2 (3%) and 1 (2%) patients, all of whom suffered from disseminated or diffuse bone involvement according to promise criteria and none of whom experienced biochemical response over the course of therapy
Click to Show/Hide
|
||||
| Experiment 184 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Grade 3 anemia |
19%
|
|||
| Patients Enrolled |
59 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | A median of 3 cycles | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
Another study retrospectively studied fifty-nine mCRPC patients after receiving at least one antihormonal drug as well as chemotherapy. These patients were treated with a median of three cycles of 177Lu-PSMA-61. The primary end point was overall survival, and secondary end point was decrease in PSA level. Follow-up data was available for forty-five patients with 91% showing a PSA decline. A decline in PSA levels of greater than or equal to 50% occurred in 53% of the patients. The median overall survival was 32 weeks. An initial alkaline phosphatase (ALP) level less than 220 U/L and a PSA decline after the first cycle were associated with a longer overall survival (56 vs. 28 weeks, p < 0.01, and 56 vs. 29 weeks, p = 0.04, respectively). Toxicity overview showed grade 3 leukopenia and thrombocytopenia in 3% patients and grade 3 anemia in 19%. No grade 3 or 4 nephrotoxicity or grade 4 blood toxicity was observed. This study showed a statistically significant decline in ALP levels after the first cycle of 177Lu-PSMA-617.
Click to Show/Hide
|
||||
| Experiment 185 Reporting the Activity Data of This PDC | [54] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Grade 3 anemia |
30%
|
|||
| Patients Enrolled |
10 patients with metastatic castration-resistant prostate cancer and with visceral metastasis.
|
||||
| Administration Time | One cycle | ||||
| Administration Dosage | 4.88 GBq | ||||
| MOA of PDC |
Lutetium-177-PSMA was a reasonable palliative treatment option with limited toxicity for these end-stage mCRPC patients with visceral metastasis with adequate PSA stabilization. A synergistic drug amalgamation may be an ideal way to boost the outcome in the future.
|
||||
| Description |
Liver (80%), lung (30%), adrenal (10%), and peritoneum (10%) were the sites of visceral metastasis in our study. On PSA response assessment, 10%, 60%, and 30% of the patients had partial response, stable disease, and progressive disease, respectively. Forty percent of the patients had improvement in the VAS, while 50% had improvement in the AQS score. Median PFS was 24 weeks in our study. A cut-off of 4.88GBq of 177Lu-PSMA was the best-predicted progression with 66.67% sensitivity and 100% specificity on ROC analysis. Thirty percent of the patients showed grade 3 anemia. No other significant toxicity was seen.
Click to Show/Hide
|
||||
| Experiment 186 Reporting the Activity Data of This PDC | [53] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Grade 3 infection |
3.20%
|
|||
| Administration Time | 1-7 cycles | ||||
| Administration Dosage | 7081 MBq (IQR 6995-7188) | ||||
| MOA of PDC |
177Lu-PSMA-RLT in a four-week interval with a fixed dose was safe and effective. A significant PSA response was observed in six out of ten patients, which was also associated with better OS and PFS. A shorter treatment interval may broaden the therapeutic window among mCRPC patients with high volume disease and rapidly rising PSA. Pre-treatment staging PSMA was not helpful in distinguishing responders from non-responders. However, parameters for tumor burden and its activity provide prognostic information related to OS and PFS.
Click to Show/Hide
|
||||
| Description |
In this patient cohort, grade 1-2 hemoglobin values were observed in 57 (91.9%) patients after treatment, but there were no grade 3 hemoglobin values. Grade 1-2 leucopenia was observed in thirteen patients and two patients had grade 3 leucopenia. Grade 1-2 thrombocytopenia was observed in seventeen patients and only one patient had grade 3 trombocytopenia. Tiredness appeared to be the most serious patient-reported adverse event during treatment. Grade 3 tiredness was reported by ten (16.1%) and grade 1-2 tiredness by twenty-seven (43.5%) of the patients. Grade 3 pain was reported by four subjects (6.5%) and grade 3 infection was reported by two subjects. None of the grade 3 pain or infections were related to 177Lu-PSMA-617 treatment. Grade 1-2 dryness of the mouth was reported by thirty-three (53.2%) of the patients. Grade 1-2 nausea was reported by twenty-two (35.5%) and diarrhea by sixteen (25.8%) of the patients. Grade 4-5 side effects were not reported at all.
Click to Show/Hide
|
||||
| In Vivo Model | This is a single-center retrospective analysis in 62 men with pathologically confirmed castration resistant metastatic prostate cancer who were treated with 177Lu-PSMA-617 during January 2017-February 2019. Grade 3 infection was reported by two subjects. | ||||
| Experiment 187 Reporting the Activity Data of This PDC | [53] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Grade 3 leucopenia |
3.20%
|
|||
| Patients Enrolled |
This is a single-center retrospective analysis in 62 men with pathologically confirmed castration resistant metastatic prostate cancer who were treated with <sup>177</sup>Lu-PSMA-617 during January 2017-February 2019. Two patients had grade 3 leucopenia.
|
||||
| Administration Time | 1-7 cycles | ||||
| Administration Dosage | 7081 MBq (IQR 6995-7188) | ||||
| MOA of PDC |
177Lu-PSMA-RLT in a four-week interval with a fixed dose was safe and effective. A significant PSA response was observed in six out of ten patients, which was also associated with better OS and PFS. A shorter treatment interval may broaden the therapeutic window among mCRPC patients with high volume disease and rapidly rising PSA. Pre-treatment staging PSMA was not helpful in distinguishing responders from non-responders. However, parameters for tumor burden and its activity provide prognostic information related to OS and PFS.
Click to Show/Hide
|
||||
| Description |
In this patient cohort, grade 1-2 hemoglobin values were observed in 57 (91.9%) patients after treatment, but there were no grade 3 hemoglobin values. Grade 1-2 leucopenia was observed in thirteen patients and two patients had grade 3 leucopenia. Grade 1-2 thrombocytopenia was observed in seventeen patients and only one patient had grade 3 trombocytopenia. Tiredness appeared to be the most serious patient-reported adverse event during treatment. Grade 3 tiredness was reported by ten (16.1%) and grade 1-2 tiredness by twenty-seven (43.5%) of the patients. Grade 3 pain was reported by four subjects (6.5%) and grade 3 infection was reported by two subjects. None of the grade 3 pain or infections were related to 177Lu-PSMA-617 treatment. Grade 1-2 dryness of the mouth was reported by thirty-three (53.2%) of the patients. Grade 1-2 nausea was reported by twenty-two (35.5%) and diarrhea by sixteen (25.8%) of the patients. Grade 4-5 side effects were not reported at all.
Click to Show/Hide
|
||||
| Experiment 188 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Grade 3 leukopenia/thrombocytopenia |
3%
|
|||
| Patients Enrolled |
59 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | A median of 3 cycles | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
Another study retrospectively studied fifty-nine mCRPC patients after receiving at least one antihormonal drug as well as chemotherapy. These patients were treated with a median of three cycles of 177Lu-PSMA-61. The primary end point was overall survival, and secondary end point was decrease in PSA level. Follow-up data was available for forty-five patients with 91% showing a PSA decline. A decline in PSA levels of greater than or equal to 50% occurred in 53% of the patients. The median overall survival was 32 weeks. An initial alkaline phosphatase (ALP) level less than 220 U/L and a PSA decline after the first cycle were associated with a longer overall survival (56 vs. 28 weeks, p < 0.01, and 56 vs. 29 weeks, p = 0.04, respectively). Toxicity overview showed grade 3 leukopenia and thrombocytopenia in 3% patients and grade 3 anemia in 19%. No grade 3 or 4 nephrotoxicity or grade 4 blood toxicity was observed. This study showed a statistically significant decline in ALP levels after the first cycle of 177Lu-PSMA-617.
Click to Show/Hide
|
||||
| Experiment 189 Reporting the Activity Data of This PDC | [53] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Grade 3 pain |
6.50%
|
|||
| Administration Time | 1-7 cycles | ||||
| Administration Dosage | 7081 MBq (IQR 6995-7188) | ||||
| MOA of PDC |
177Lu-PSMA-RLT in a four-week interval with a fixed dose was safe and effective. A significant PSA response was observed in six out of ten patients, which was also associated with better OS and PFS. A shorter treatment interval may broaden the therapeutic window among mCRPC patients with high volume disease and rapidly rising PSA. Pre-treatment staging PSMA was not helpful in distinguishing responders from non-responders. However, parameters for tumor burden and its activity provide prognostic information related to OS and PFS.
Click to Show/Hide
|
||||
| Description |
In this patient cohort, grade 1-2 hemoglobin values were observed in 57 (91.9%) patients after treatment, but there were no grade 3 hemoglobin values. Grade 1-2 leucopenia was observed in thirteen patients and two patients had grade 3 leucopenia. Grade 1-2 thrombocytopenia was observed in seventeen patients and only one patient had grade 3 trombocytopenia. Tiredness appeared to be the most serious patient-reported adverse event during treatment. Grade 3 tiredness was reported by ten (16.1%) and grade 1-2 tiredness by twenty-seven (43.5%) of the patients. Grade 3 pain was reported by four subjects (6.5%) and grade 3 infection was reported by two subjects. None of the grade 3 pain or infections were related to 177Lu-PSMA-617 treatment. Grade 1-2 dryness of the mouth was reported by thirty-three (53.2%) of the patients. Grade 1-2 nausea was reported by twenty-two (35.5%) and diarrhea by sixteen (25.8%) of the patients. Grade 4-5 side effects were not reported at all.
Click to Show/Hide
|
||||
| In Vivo Model | This is a single-center retrospective analysis in 62 men with pathologically confirmed castration resistant metastatic prostate cancer who were treated with 177Lu-PSMA-617 during January 2017-February 2019. Grade 3 pain was reported by four subjects (6.5%). | ||||
| Experiment 190 Reporting the Activity Data of This PDC | [53] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Grade 3 thrombocytopenia |
1.60%
|
|||
| Patients Enrolled |
This is a single-center retrospective analysis in 62 men with pathologically confirmed castration resistant metastatic prostate cancer who were treated with <sup>177</sup>Lu-PSMA-617 during January 2017-February 2019. Grade 1-2 thrombocytopenia was observed in seventeen patients.
|
||||
| Administration Time | 1-7 cycles | ||||
| Administration Dosage | 7081 MBq (IQR 6995-7188) | ||||
| MOA of PDC |
177Lu-PSMA-RLT in a four-week interval with a fixed dose was safe and effective. A significant PSA response was observed in six out of ten patients, which was also associated with better OS and PFS. A shorter treatment interval may broaden the therapeutic window among mCRPC patients with high volume disease and rapidly rising PSA. Pre-treatment staging PSMA was not helpful in distinguishing responders from non-responders. However, parameters for tumor burden and its activity provide prognostic information related to OS and PFS.
Click to Show/Hide
|
||||
| Description |
In this patient cohort, grade 1-2 hemoglobin values were observed in 57 (91.9%) patients after treatment, but there were no grade 3 hemoglobin values. Grade 1-2 leucopenia was observed in thirteen patients and two patients had grade 3 leucopenia. Grade 1-2 thrombocytopenia was observed in seventeen patients and only one patient had grade 3 trombocytopenia. Tiredness appeared to be the most serious patient-reported adverse event during treatment. Grade 3 tiredness was reported by ten (16.1%) and grade 1-2 tiredness by twenty-seven (43.5%) of the patients. Grade 3 pain was reported by four subjects (6.5%) and grade 3 infection was reported by two subjects. None of the grade 3 pain or infections were related to 177Lu-PSMA-617 treatment. Grade 1-2 dryness of the mouth was reported by thirty-three (53.2%) of the patients. Grade 1-2 nausea was reported by twenty-two (35.5%) and diarrhea by sixteen (25.8%) of the patients. Grade 4-5 side effects were not reported at all.
Click to Show/Hide
|
||||
| Experiment 191 Reporting the Activity Data of This PDC | [53] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Grade 3 tiredness |
16.10%
|
|||
| Administration Time | 1-7 cycles | ||||
| Administration Dosage | 7081 MBq (IQR 6995-7188) | ||||
| MOA of PDC |
177Lu-PSMA-RLT in a four-week interval with a fixed dose was safe and effective. A significant PSA response was observed in six out of ten patients, which was also associated with better OS and PFS. A shorter treatment interval may broaden the therapeutic window among mCRPC patients with high volume disease and rapidly rising PSA. Pre-treatment staging PSMA was not helpful in distinguishing responders from non-responders. However, parameters for tumor burden and its activity provide prognostic information related to OS and PFS.
Click to Show/Hide
|
||||
| Description |
In this patient cohort, grade 1-2 hemoglobin values were observed in 57 (91.9%) patients after treatment, but there were no grade 3 hemoglobin values. Grade 1-2 leucopenia was observed in thirteen patients and two patients had grade 3 leucopenia. Grade 1-2 thrombocytopenia was observed in seventeen patients and only one patient had grade 3 trombocytopenia. Tiredness appeared to be the most serious patient-reported adverse event during treatment. Grade 3 tiredness was reported by ten (16.1%) and grade 1-2 tiredness by twenty-seven (43.5%) of the patients. Grade 3 pain was reported by four subjects (6.5%) and grade 3 infection was reported by two subjects. None of the grade 3 pain or infections were related to 177Lu-PSMA-617 treatment. Grade 1-2 dryness of the mouth was reported by thirty-three (53.2%) of the patients. Grade 1-2 nausea was reported by twenty-two (35.5%) and diarrhea by sixteen (25.8%) of the patients. Grade 4-5 side effects were not reported at all.
Click to Show/Hide
|
||||
| In Vivo Model | This is a single-center retrospective analysis in 62 men with pathologically confirmed castration resistant metastatic prostate cancer who were treated with 177Lu-PSMA-617 during January 2017-February 2019. Grade 3 tiredness was reported by ten (16.1%). | ||||
| Experiment 192 Reporting the Activity Data of This PDC | [20] | ||||
| Indication | Advanced prostate cancer | ||||
| Efficacy Data | Grade 3 toxicity |
37.50%
|
|||
| Patients Enrolled |
Patients with advanced prostate cancer.
|
||||
| Administration Time | 2 cycles | ||||
| Description |
No grade 4 toxicity was noticed, and grade 3 toxicity occurred in 3 patients (37.5%).
|
||||
| Experiment 193 Reporting the Activity Data of This PDC | [14] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Grade 3/4 adverse events |
33%
|
|||
| Patients Enrolled |
200 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | Every 6 weeks (up to 6 cycles) | ||||
| MOA of PDC |
Radiopharmaceuticals have been used in prostate cancer for decades with known efficacy in palliation of bone metastasis. The FDA approval of the most recent radiopharmaceutical, 177Lu-PSMA-617, shows a clear overall survival benefit compared to the best SOC. Current studies are ongoing to evaluate the effectiveness of 177Lu-PSMA-617 in earlier lines of therapy, such as after only 1 line of therapy with an ARPI as in the PSMAfore study, or in mCSPC in combination with ADT and an ARPI as in the PSMAddition study. Studies are also ongoing with 177Lu-PSMA-617 in combination with other treatments which may produce a synergistic effect. As described, there are many clinical trials ongoing that are modifying the 177Lu-PSMA-617 to possibly achieve improved results. Studies are also ongoing looking at swapping the 177Lu for another radioactive agent, such as 225Ac (an alpha emitter) which may have benefits over the beta-emitting 177Lu. Other studies are looking at J591, a monoclonal antibody to PSMA which has unique differences compared to small-molecule PSMA binders. Overall, PSMA-based radioligand therapy has been shown to be an effective and life-prolonging therapy and should be considered a treatment option for selected men with mCRPC. As described, there are many ongoing studies further evaluating PSMA radioligand therapy in Australia, South Africa, Europe, and the United States, representing a truly global effort to improve prostate cancer care.
Click to Show/Hide
|
||||
| Description |
Grade 3-4 AEs occurred in 32 (33%) of men who received 177Lu-PSMA-617 versus 45 (53%) of men in the cabazitaxel group. All-grade toxicities that were more common in the 177Lu-PSMA-617 were dry mouth (60% vs. 21%), dry eyes (30% vs. 4%), and thrombocytopenia (18% vs. 5%). All-grade toxicities that were more common with cabazitaxel were diarrhea (52% vs. 18%), neuropathy (26% vs. 10%), and dysgeusia (27% vs. 12%).
Click to Show/Hide
|
||||
| Experiment 194 Reporting the Activity Data of This PDC | [14] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Grade 3/4 hematotoxicity |
12%
|
|||
| Patients Enrolled |
145 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 1-4 cycles | ||||
| MOA of PDC |
Radiopharmaceuticals have been used in prostate cancer for decades with known efficacy in palliation of bone metastasis. The FDA approval of the most recent radiopharmaceutical, 177Lu-PSMA-617, shows a clear overall survival benefit compared to the best SOC. Current studies are ongoing to evaluate the effectiveness of 177Lu-PSMA-617 in earlier lines of therapy, such as after only 1 line of therapy with an ARPI as in the PSMAfore study, or in mCSPC in combination with ADT and an ARPI as in the PSMAddition study. Studies are also ongoing with 177Lu-PSMA-617 in combination with other treatments which may produce a synergistic effect. As described, there are many clinical trials ongoing that are modifying the 177Lu-PSMA-617 to possibly achieve improved results. Studies are also ongoing looking at swapping the 177Lu for another radioactive agent, such as 225Ac (an alpha emitter) which may have benefits over the beta-emitting 177Lu. Other studies are looking at J591, a monoclonal antibody to PSMA which has unique differences compared to small-molecule PSMA binders. Overall, PSMA-based radioligand therapy has been shown to be an effective and life-prolonging therapy and should be considered a treatment option for selected men with mCRPC. As described, there are many ongoing studies further evaluating PSMA radioligand therapy in Australia, South Africa, Europe, and the United States, representing a truly global effort to improve prostate cancer care.
Click to Show/Hide
|
||||
| Description |
A larger retrospective multicenter analysis of 145 patients treated with 248 therapy cycles of 177Lu-PSMA-617 at 12 nuclear medicine centers throughout Germany between 2014 and 2015 was conducted. Patients had received 1-4 therapy cycles of treatment. In their analysis, the biochemical response rate (defined as a 50% or greater drop in PSA) was 45% after all therapy cycles. Grade 3 or 4 hematotoxicity occurred in 18 patients (12%) and xerostomia occurred in 11 patients (8%).
Click to Show/Hide
|
||||
| Experiment 195 Reporting the Activity Data of This PDC | [7], [55] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Grade 3/4 kidney injury |
3%
|
|||
| Patients Enrolled |
Of the 1003 patients who underwent scanning, 831 (82.9%) were judged to have met all the trial eligibility criteria, including the PSMA imaging criteria, and were randomly assigned, between June 4, 2018, and October 23, 2019, to receive either <sup>177</sup>Lu-PSMA-617 plus protocol-permitted standard care (551 patients) or standard care alone (280).
Click to Show/Hide
|
||||
| Administration Time | Every 6 weeks for up to six doses | ||||
| Administration Dosage | 7.4 GBq | ||||
| MOA of PDC |
After binding to the PSMA receptor, [177Lu]Lu-PSMA-617 is internalized into the PSMA positive cells, resulting in a long retention within these cells; the high energy electrons emitted during the decay can selectively induce tissue and DNA damage, leading to cell death.
|
||||
| Description |
Observed hematological toxicity is most pronounced in patients with extensive bone metastases, as the uptake in these metastases may lead to radiation-induced damage in the neighboring bone marrow. Renal toxicity resulting in grade 3 or 4 kidney injury occurred in 3% of patients during the VISION trial.
|
||||
| Half life period | 41.1 ± 9.3 h | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT03511664 | Clinical Status | Phase 3 | ||
| Experiment 196 Reporting the Activity Data of This PDC | [30] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Grade 3/4 thrombocytopenia |
13%
|
|||
| Patients Enrolled |
30 patients with metastatic castration-resistant prostate cancer who underwent 4 cycles of mean 7.5 GBq Lu-PSMA 617 at 6weeks interval.
|
||||
| Administration Time | 4 cycles at 6-week intervals | ||||
| Administration Dosage | 7.5 GBq | ||||
| Description |
The first prospective study published by the Australian group (LuPSMA trial) was a single-center, single-arm phase 2 study in 30 mCRPC patients who underwent 4 cycles of mean 7.5 GBq Lu-PSMA 617 at 6 weeks interval. Seventeen (56.7%) of the patients reported ≥50% decline in PSA. Four patients (13%) reported relevant grade 3-4 thrombocytopenia.
|
||||
| Experiment 197 Reporting the Activity Data of This PDC | [30] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Grade 3/4 thrombocytopenia/anemia |
10%
|
|||
| Patients Enrolled |
50 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 4 cycles at 6-week intervals | ||||
| Administration Dosage | 7.5 GBq | ||||
| Description |
A further extension of this study with 50 patients recently reported ≥50% decrease in PSA in 64% of patients and grade 3-4 thrombocytopenia or anemia in 10% of the patients. Median progression-free survival (PFS) and overall survival (OS) was 6.9 months and 13.3 months, respectively.
|
||||
| Experiment 198 Reporting the Activity Data of This PDC | [55], [56] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Grades 3/5 myelosuppression |
23.40%
|
|||
| Patients Enrolled |
Of the 1003 patients who underwent scanning, 831 (82.9%) were judged to have met all the trial eligibility criteria, including the PSMA imaging criteria, and were randomly assigned, between June 4, 2018, and October 23, 2019, to receive either <sup>177</sup>Lu-PSMA-617 plus protocol-permitted standard care (551 patients) or standard care alone (280).
Click to Show/Hide
|
||||
| Evaluation Method | PET/CT assay | ||||
| MOA of PDC |
Prostate-specific membrane antigen (PSMA)-targeted radiopharmaceutical like 177Lu-PSMA-617, a beta particle emitter has demonstrated improvement in overall survival in mCRPC patients pretreated with ARAT or taxanes. Although immune checkpoint inhibitors are being tested in mCRPC, there is no robust evidence to support this premise.
|
||||
| Description |
Myelosuppression was noted in 47.4% (grades 3-5 in 23.4%) patients in the Lu-PSMA-617 arm. Additional concerning toxicities included fatigue, xerostomia because of expression of PSMA in salivary glands, and nausea-vomiting.
|
||||
| Related Clinical Trial | |||||
| NCT Number | NCT03511664 | Clinical Status | Phase 3 | ||
| Experiment 199 Reporting the Activity Data of This PDC | [51] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Grading stage 0 visual salivary gland scintigraphy |
5.56%
|
|||
| Patients Enrolled |
18 patients with metastatic castration-resistant prostate cancer treated with tandem-cohort PRLT.
|
||||
| Administration Time | 1 week | ||||
| Administration Dosage | A median activity of 4.25 GBq (range 3.6-7.2 GBq) | ||||
| Evaluation Method | Salivary gland scintigraphy assay | ||||
| MOA of PDC |
Salivary gland dysfunction after 177Lu-PSMA-I&T/-617 PRLT has minor clinical relevance, both subjectively and objectively. Even after high cumulative activities, only mild-to-moderate dryness of mouth occurs in a minority of the patients. The prevalence of xerostomia appears to be significantly lower than the historical controls after external radiotherapy, radioiodine therapy, and especially after PRLT with 225Ac-PSMA-617. A validated questionnaire on xerostomia, salivary gland scintigraphy, and PSMA-PET/CT parameters can help to objectify, standardize, and quantify the SG toxicity of PRLT. A decrease of the excretion fraction on SGS and of the metabolic volume on PSMA PET/CT can be early indicators of SG impairment. The co-administration of lower doses of 225Ac in combination with 177Lu-PSMA-617 (Tandem concept) can decrease severe xerostomia after PRLT with alpha-emitters.
Click to Show/Hide
|
||||
| Description |
The stage of xerostomia at the baseline according to SGS was 0 in 10/18 patients, 1 in 6/18 patients, and 2 in 2/18 patients, while, at the follow-up, stage 0 was noted in 1/18 patients, stage 1 in 8/18 patients, and stage 2 in 9/18 patients (p < 0.001).
|
||||
| Experiment 200 Reporting the Activity Data of This PDC | [51] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Grading stage 0 visual salivary gland scintigraphy |
40%
|
|||
| Patients Enrolled |
40 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | A median of 5.5 (range: 2-9) cycles, median follow up 22.7 months (iqr: 16.4-30.2) | ||||
| Administration Dosage | Median cumulative activity of 35.3 GBq | ||||
| Evaluation Method | Salivary gland scintigraphy assay | ||||
| MOA of PDC |
Salivary gland dysfunction after 177Lu-PSMA-I&T/-617 PRLT has minor clinical relevance, both subjectively and objectively. Even after high cumulative activities, only mild-to-moderate dryness of mouth occurs in a minority of the patients. The prevalence of xerostomia appears to be significantly lower than the historical controls after external radiotherapy, radioiodine therapy, and especially after PRLT with 225Ac-PSMA-617. A validated questionnaire on xerostomia, salivary gland scintigraphy, and PSMA-PET/CT parameters can help to objectify, standardize, and quantify the SG toxicity of PRLT. A decrease of the excretion fraction on SGS and of the metabolic volume on PSMA PET/CT can be early indicators of SG impairment. The co-administration of lower doses of 225Ac in combination with 177Lu-PSMA-617 (Tandem concept) can decrease severe xerostomia after PRLT with alpha-emitters.
Click to Show/Hide
|
||||
| Description |
In the visual grading, no significant changes were found on SGS after PRLT (stage 0 in 16 (40%) patients, stage 1 in 16 (40%) patients, and stage 2 in 8 (20%) patients at the baseline; stage 0 in 16 (40%) patients, stage 1 in 20 (50%) patients, and stage 2 in 4 (10%) patients at the follow-up; p = 0.63). A comparison of the Umax and EF of all SG confirmed no significant changes before and after PRLT.
Click to Show/Hide
|
||||
| Experiment 201 Reporting the Activity Data of This PDC | [51] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Grading stage 1 visual salivary gland scintigraphy |
44.44%
|
|||
| Patients Enrolled |
18 patients with metastatic castration-resistant prostate cancer treated with tandem-cohort PRLT.
|
||||
| Administration Time | 1 week | ||||
| Administration Dosage | A median activity of 4.25 GBq (range 3.6-7.2 GBq) | ||||
| Evaluation Method | Salivary gland scintigraphy assay | ||||
| MOA of PDC |
Salivary gland dysfunction after 177Lu-PSMA-I&T/-617 PRLT has minor clinical relevance, both subjectively and objectively. Even after high cumulative activities, only mild-to-moderate dryness of mouth occurs in a minority of the patients. The prevalence of xerostomia appears to be significantly lower than the historical controls after external radiotherapy, radioiodine therapy, and especially after PRLT with 225Ac-PSMA-617. A validated questionnaire on xerostomia, salivary gland scintigraphy, and PSMA-PET/CT parameters can help to objectify, standardize, and quantify the SG toxicity of PRLT. A decrease of the excretion fraction on SGS and of the metabolic volume on PSMA PET/CT can be early indicators of SG impairment. The co-administration of lower doses of 225Ac in combination with 177Lu-PSMA-617 (Tandem concept) can decrease severe xerostomia after PRLT with alpha-emitters.
Click to Show/Hide
|
||||
| Description |
The stage of xerostomia at the baseline according to SGS was 0 in 10/18 patients, 1 in 6/18 patients, and 2 in 2/18 patients, while, at the follow-up, stage 0 was noted in 1/18 patients, stage 1 in 8/18 patients, and stage 2 in 9/18 patients (p < 0.001).
|
||||
| Experiment 202 Reporting the Activity Data of This PDC | [51] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Grading stage 1 visual salivary gland scintigraphy |
50%
|
|||
| Patients Enrolled |
40 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | A median of 5.5 (range: 2-9) cycles, median follow up 22.7 months (iqr: 16.4-30.2) | ||||
| Administration Dosage | Median cumulative activity of 35.3 GBq | ||||
| Evaluation Method | Salivary gland scintigraphy assay | ||||
| MOA of PDC |
Salivary gland dysfunction after 177Lu-PSMA-I&T/-617 PRLT has minor clinical relevance, both subjectively and objectively. Even after high cumulative activities, only mild-to-moderate dryness of mouth occurs in a minority of the patients. The prevalence of xerostomia appears to be significantly lower than the historical controls after external radiotherapy, radioiodine therapy, and especially after PRLT with 225Ac-PSMA-617. A validated questionnaire on xerostomia, salivary gland scintigraphy, and PSMA-PET/CT parameters can help to objectify, standardize, and quantify the SG toxicity of PRLT. A decrease of the excretion fraction on SGS and of the metabolic volume on PSMA PET/CT can be early indicators of SG impairment. The co-administration of lower doses of 225Ac in combination with 177Lu-PSMA-617 (Tandem concept) can decrease severe xerostomia after PRLT with alpha-emitters.
Click to Show/Hide
|
||||
| Description |
In the visual grading, no significant changes were found on SGS after PRLT (stage 0 in 16 (40%) patients, stage 1 in 16 (40%) patients, and stage 2 in 8 (20%) patients at the baseline; stage 0 in 16 (40%) patients, stage 1 in 20 (50%) patients, and stage 2 in 4 (10%) patients at the follow-up; p = 0.63). A comparison of the Umax and EF of all SG confirmed no significant changes before and after PRLT.
Click to Show/Hide
|
||||
| Experiment 203 Reporting the Activity Data of This PDC | [51] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Grading stage 2 visual salivary gland scintigraphy |
10%
|
|||
| Patients Enrolled |
40 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | A median of 5.5 (range: 2-9) cycles, median follow up 22.7 months (iqr: 16.4-30.2) | ||||
| Administration Dosage | Median cumulative activity of 35.3 GBq | ||||
| Evaluation Method | Salivary gland scintigraphy assay | ||||
| MOA of PDC |
Salivary gland dysfunction after 177Lu-PSMA-I&T/-617 PRLT has minor clinical relevance, both subjectively and objectively. Even after high cumulative activities, only mild-to-moderate dryness of mouth occurs in a minority of the patients. The prevalence of xerostomia appears to be significantly lower than the historical controls after external radiotherapy, radioiodine therapy, and especially after PRLT with 225Ac-PSMA-617. A validated questionnaire on xerostomia, salivary gland scintigraphy, and PSMA-PET/CT parameters can help to objectify, standardize, and quantify the SG toxicity of PRLT. A decrease of the excretion fraction on SGS and of the metabolic volume on PSMA PET/CT can be early indicators of SG impairment. The co-administration of lower doses of 225Ac in combination with 177Lu-PSMA-617 (Tandem concept) can decrease severe xerostomia after PRLT with alpha-emitters.
Click to Show/Hide
|
||||
| Description |
In the visual grading, no significant changes were found on SGS after PRLT (stage 0 in 16 (40%) patients, stage 1 in 16 (40%) patients, and stage 2 in 8 (20%) patients at the baseline; stage 0 in 16 (40%) patients, stage 1 in 20 (50%) patients, and stage 2 in 4 (10%) patients at the follow-up; p = 0.63). A comparison of the Umax and EF of all SG confirmed no significant changes before and after PRLT.
Click to Show/Hide
|
||||
| Experiment 204 Reporting the Activity Data of This PDC | [51] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Grading stage 2 visual salivary gland scintigraphy |
50%
|
|||
| Patients Enrolled |
18 patients with metastatic castration-resistant prostate cancer treated with tandem-cohort PRLT.
|
||||
| Administration Time | 1 week | ||||
| Administration Dosage | A median activity of 4.25 GBq (range 3.6-7.2 GBq) | ||||
| Evaluation Method | Salivary gland scintigraphy assay | ||||
| MOA of PDC |
Salivary gland dysfunction after 177Lu-PSMA-I&T/-617 PRLT has minor clinical relevance, both subjectively and objectively. Even after high cumulative activities, only mild-to-moderate dryness of mouth occurs in a minority of the patients. The prevalence of xerostomia appears to be significantly lower than the historical controls after external radiotherapy, radioiodine therapy, and especially after PRLT with 225Ac-PSMA-617. A validated questionnaire on xerostomia, salivary gland scintigraphy, and PSMA-PET/CT parameters can help to objectify, standardize, and quantify the SG toxicity of PRLT. A decrease of the excretion fraction on SGS and of the metabolic volume on PSMA PET/CT can be early indicators of SG impairment. The co-administration of lower doses of 225Ac in combination with 177Lu-PSMA-617 (Tandem concept) can decrease severe xerostomia after PRLT with alpha-emitters.
Click to Show/Hide
|
||||
| Description |
The stage of xerostomia at the baseline according to SGS was 0 in 10/18 patients, 1 in 6/18 patients, and 2 in 2/18 patients, while, at the follow-up, stage 0 was noted in 1/18 patients, stage 1 in 8/18 patients, and stage 2 in 9/18 patients (p < 0.001).
|
||||
| Experiment 205 Reporting the Activity Data of This PDC | [41] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Hemoglobin decrease rate | ≥ 30% | |||
| Patients Enrolled |
734 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 5 doses (range: 1 to 6) | ||||
| Administration Dosage | Median cumulative dose 37.5 GBq (range, 7.0 to 48.3) | ||||
| MOA of PDC |
On March 23, 2022, the FDA approved 177Lu-PSMA-617 for the treatment of adult patients with PSMA-positive mCRPC who have been treated with androgen receptor pathway inhibition and taxane-based chemotherapy. The approval was based on a meaningful advantage in overall survival supported by a delay in tumor progression and higher objective response rate. The decision took into account several important factors unique to this applications context. Metastatic castration-resistant prostate cancer (mCRPC) is a life-threatening condition that lacks curative treatment, creating an unmet need. This product provides a novel mechanism of action as the first radioligand therapeutic agent for mCRPC providing anti-tumor effects in both bone and non-bone sites and may provide an opportunity to be combined with other available therapies with different toxicity profiles across mechanistic classes. Finally, 177Lu-PSMA-617 offers a different safety profile than other available systemic therapies which was determined to be acceptable for the indicated patient population, expanding treatment options that can be individualized to a patients preferences and comorbidities.
Click to Show/Hide
|
||||
| Description |
Serious adverse reactions occurred in 36% of patients who received 177Lu-PSMA-617 plus BSoC. Fatal adverse reactions occurred in 2.8% of patients who received 177Lu-PSMA-617 plus BSoC, including sepsis (0.9%), pancytopenia (0.6%), hepatic failure (0.4%), intracranial hemorrhage (0.2%), subdural hematoma (0.2%), ischemic stroke (0.2%), COVID-19 (0.2%), and aspiration pneumonia (0.2%). The 2 fatal adverse reactions of intracranial hemorrhage and subdural hematoma occurred in patients who had concurrent treatment-related thrombocytopenia. The most common adverse reactions (≥ 20%) occurring at a higher incidence in patients who received 177Lu-PSMA-617 plus BSoC were fatigue, dry mouth, nausea, anemia, decreased appetite, and constipation. The most common laboratory abnormalities that worsened from baseline in ≥ 30% of patients who received 177Lu-PSMA-617 plus BSoC were decreased lymphocytes, decreased hemoglobin, decreased leukocytes, decreased platelets, decreased calcium, and decreased sodium.
Click to Show/Hide
|
||||
| Experiment 206 Reporting the Activity Data of This PDC | [41] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Hepatic failure |
0.40%
|
|||
| Patients Enrolled |
734 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 5 doses (range: 1 to 6) | ||||
| Administration Dosage | Median cumulative dose 37.5 GBq (range, 7.0 to 48.3) | ||||
| MOA of PDC |
On March 23, 2022, the FDA approved 177Lu-PSMA-617 for the treatment of adult patients with PSMA-positive mCRPC who have been treated with androgen receptor pathway inhibition and taxane-based chemotherapy. The approval was based on a meaningful advantage in overall survival supported by a delay in tumor progression and higher objective response rate. The decision took into account several important factors unique to this applications context. Metastatic castration-resistant prostate cancer (mCRPC) is a life-threatening condition that lacks curative treatment, creating an unmet need. This product provides a novel mechanism of action as the first radioligand therapeutic agent for mCRPC providing anti-tumor effects in both bone and non-bone sites and may provide an opportunity to be combined with other available therapies with different toxicity profiles across mechanistic classes. Finally, 177Lu-PSMA-617 offers a different safety profile than other available systemic therapies which was determined to be acceptable for the indicated patient population, expanding treatment options that can be individualized to a patients preferences and comorbidities.
Click to Show/Hide
|
||||
| Description |
Serious adverse reactions occurred in 36% of patients who received 177Lu-PSMA-617 plus BSoC. Fatal adverse reactions occurred in 2.8% of patients who received 177Lu-PSMA-617 plus BSoC, including sepsis (0.9%), pancytopenia (0.6%), hepatic failure (0.4%), intracranial hemorrhage (0.2%), subdural hematoma (0.2%), ischemic stroke (0.2%), COVID-19 (0.2%), and aspiration pneumonia (0.2%). The 2 fatal adverse reactions of intracranial hemorrhage and subdural hematoma occurred in patients who had concurrent treatment-related thrombocytopenia. The most common adverse reactions (≥ 20%) occurring at a higher incidence in patients who received 177Lu-PSMA-617 plus BSoC were fatigue, dry mouth, nausea, anemia, decreased appetite, and constipation. The most common laboratory abnormalities that worsened from baseline in ≥ 30% of patients who received 177Lu-PSMA-617 plus BSoC were decreased lymphocytes, decreased hemoglobin, decreased leukocytes, decreased platelets, decreased calcium, and decreased sodium.
Click to Show/Hide
|
||||
| Experiment 207 Reporting the Activity Data of This PDC | [19] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Imaging response rate |
44%
|
|||
| Patients Enrolled |
25 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | A median of four (iqr: 2-6) cycles every 6-8 weeks | ||||
| Administration Dosage | Mean of 7.7 ± 1.4 GBq/cycle | ||||
| Evaluation Method | 68Ga-PSMA-11 PET/CT assay | ||||
| MOA of PDC |
The response to radioligand therapy with 177Lu-PSMA-617 seems to be independent of the presence of early-onset prostate cancer (EOPC); however, the less favorable survival outcome observed in our study may indicate a more aggressive disease course. Expectedly, the safety of LuPSMA-RLT does not seem to be compromised in metastasized castration-resistant EOPC patients. Comparative studies on age at diagnosis of prostate cancer and the patients outcome after LuPSMA-RLT are needed.
Click to Show/Hide
|
||||
| Description |
Imaging-based response using 68Ga-PSMA-11-PET/CT after two to three cycles was seen in 11/25 (44%). Additionally, responders had a significantly longer median PFS (8.7 months, 95% CI 1.3-16.1 vs. 1.9 months, 95% CI 1.7-2.2, p < 0.001) and OS (16.0 months, 95% CI 7.6-24.4 vs. 4.0 months, 95% CI 0.9-7.1; p = 0.002).
|
||||
| Experiment 208 Reporting the Activity Data of This PDC | [57] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Incresae of serum troponin I levels |
0.04 ng/ml
|
|||
| Patients Enrolled |
Patients with prostate cancer and neuroendocrine tumours referred for PRRT and RLT.
|
||||
| Description |
In all patients, the value of troponin I was in normal range. In all patients, the median values of serum troponin I before and after treatment were 0.2 ± 0.02 (range: 0.00-0.42) and 0.28 ± 0.02 (range: 0.00-0.46) ng/ml, respectively (p > 0.05). In the prostate cancer patients, the median values of serum troponin I before and after treatment were 0.26 ± 0.04 (0.04-0.42) and 0.30 ± 0.04 (0.00-0.41) ng/ml, respectively (p > 0.05). In the NET patients, the median values of serum troponin I before and after treatment were 0.18 ± 0.03 (0.00-0.42) and 0.17 ± 0.03 (0.00-0.46) ng/ml, respectively (p > 0.05).
Click to Show/Hide
|
||||
| Experiment 209 Reporting the Activity Data of This PDC | [41] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Leukocytes decrease | ≥ 30% | |||
| Patients Enrolled |
734 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 5 doses (range: 1 to 6) | ||||
| Administration Dosage | Median cumulative dose 37.5 GBq (range, 7.0 to 48.3) | ||||
| MOA of PDC |
On March 23, 2022, the FDA approved 177Lu-PSMA-617 for the treatment of adult patients with PSMA-positive mCRPC who have been treated with androgen receptor pathway inhibition and taxane-based chemotherapy. The approval was based on a meaningful advantage in overall survival supported by a delay in tumor progression and higher objective response rate. The decision took into account several important factors unique to this applications context. Metastatic castration-resistant prostate cancer (mCRPC) is a life-threatening condition that lacks curative treatment, creating an unmet need. This product provides a novel mechanism of action as the first radioligand therapeutic agent for mCRPC providing anti-tumor effects in both bone and non-bone sites and may provide an opportunity to be combined with other available therapies with different toxicity profiles across mechanistic classes. Finally, 177Lu-PSMA-617 offers a different safety profile than other available systemic therapies which was determined to be acceptable for the indicated patient population, expanding treatment options that can be individualized to a patients preferences and comorbidities.
Click to Show/Hide
|
||||
| Description |
Serious adverse reactions occurred in 36% of patients who received 177Lu-PSMA-617 plus BSoC. Fatal adverse reactions occurred in 2.8% of patients who received 177Lu-PSMA-617 plus BSoC, including sepsis (0.9%), pancytopenia (0.6%), hepatic failure (0.4%), intracranial hemorrhage (0.2%), subdural hematoma (0.2%), ischemic stroke (0.2%), COVID-19 (0.2%), and aspiration pneumonia (0.2%). The 2 fatal adverse reactions of intracranial hemorrhage and subdural hematoma occurred in patients who had concurrent treatment-related thrombocytopenia. The most common adverse reactions (≥ 20%) occurring at a higher incidence in patients who received 177Lu-PSMA-617 plus BSoC were fatigue, dry mouth, nausea, anemia, decreased appetite, and constipation. The most common laboratory abnormalities that worsened from baseline in ≥ 30% of patients who received 177Lu-PSMA-617 plus BSoC were decreased lymphocytes, decreased hemoglobin, decreased leukocytes, decreased platelets, decreased calcium, and decreased sodium.
Click to Show/Hide
|
||||
| Experiment 210 Reporting the Activity Data of This PDC | [44] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Leukopenia |
2%
|
|||
| Patients Enrolled |
64 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 2 cycles | ||||
| Administration Dosage | Cumulative mean activity of 11.5 (8.1-14.9) GBq | ||||
| MOA of PDC |
In general, the first two cycles of PSMA-RLT were well tolerated haematologically. Qualitative and quantitative bone marrow impairment appears closely associated with osseous tumour burden as only patients with advanced bone involvement and non-response to therapy exhibited high-grade haematological adverse events as well as a significant mean decline of haematological parameters. This implies that in patients with already advanced mCRPC, non-response to PSMA-RLT may be a major cause of bone marrow impairment during early treatment cycles.
Click to Show/Hide
|
||||
| Description |
In addition, lower grade thrombopenia and leukopenia were observed in 9 (14%) and 11 (17%) patients at baseline, respectively. During the observation period, severe (grade 3) anaemia, thrombopenia and leukopenia occurred in 5 (8%), 2 (3%) and 1 (2%) patients, all of whom suffered from disseminated or diffuse bone involvement according to promise criteria and none of whom experienced biochemical response over the course of therapy
Click to Show/Hide
|
||||
| Experiment 211 Reporting the Activity Data of This PDC | [40] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Leukopenia |
3.60%
|
|||
| Patients Enrolled |
14 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 140 patients receiving a total of 497 cycles | ||||
| Administration Dosage | 6.9 GBq/cycle | ||||
| MOA of PDC |
Hematologic adverse events after RLT have an acceptable overall incidence and are frequently reversible. High bone tumor burden, previous taxane-based chemotherapy and pretreatment grade 2 cytopenia may be considered as risk factors for developing clinically relevant myelosuppression, whereas cumulative RLT activity and previous 223Ra-dichloride treatment show no significant contribution to incidence rates.
Click to Show/Hide
|
||||
| Description |
Significant (grade ≥ 3) hematologic adverse events occurred in 13 (9.3%) patients, with anemia in 10 (7.1%), leukopenia in 5 (3.6%) and thrombocytopenia in 6 (4.3%). Hematotoxicity was reversible to grade ≤ 2 through a median follow-up of 8 (IQR 9) months in all but two patients who died from disease progression within less than 3 months after RLT.
Click to Show/Hide
|
||||
| Experiment 212 Reporting the Activity Data of This PDC | [19] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Leukopenia |
4%
|
|||
| Patients Enrolled |
25 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | A median of four (iqr: 2-6) cycles every 6-8 weeks | ||||
| Administration Dosage | Mean of 7.7 ± 1.4 GBq/cycle | ||||
| MOA of PDC |
The response to radioligand therapy with 177Lu-PSMA-617 seems to be independent of the presence of early-onset prostate cancer (EOPC); however, the less favorable survival outcome observed in our study may indicate a more aggressive disease course. Expectedly, the safety of LuPSMA-RLT does not seem to be compromised in metastasized castration-resistant EOPC patients. Comparative studies on age at diagnosis of prostate cancer and the patients outcome after LuPSMA-RLT are needed.
Click to Show/Hide
|
||||
| Description |
Intra- or post-therapeutic toxicity was graded according to the CTCAE v5.0 criteria. Newly developing grade ≥ 3 anemia, leukopenia, and thrombocytopenia occurred in three (12%), one (4%), and three (12%) patients, respectively. One patient showed renal toxicity (grade ≥ 3) during follow-up. Pain palliation (>2 level VAS decline) was achieved in 9/14 (64%) and performance status improvement (ECOG level decline ≥ 1) in 8/17 (47%) of patients.
Click to Show/Hide
|
||||
| Experiment 213 Reporting the Activity Data of This PDC | [42] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Leukopenia |
13%
|
|||
| Patients Enrolled |
45 patients with progressive metastatic castration-resistant prostate cancer and diffuse bone marrow involvement.
|
||||
| Administration Time | 4 cycles | ||||
| Administration Dosage | 7.4 ± 1.4 GBq | ||||
| Evaluation Method | 68Ga-PSMA-11 PET/CT assay | ||||
| MOA of PDC |
Our findings suggest that repeated cycles of RLT with 177Lu-PSMA-617 can be carried out at an acceptable safety profile in mCRPC patients with diffuse bone marrow involvement. RLT may provide a suitable strategy for prolonged disease control with substantial clinical benefit. After a minimum of two cycles, treatment response translated into significantly longer median OS. Further studies should be carried out to investigate the role of individualized RLT concepts in this advanced stage setting.
Click to Show/Hide
|
||||
| Description |
Patients with PR on interim imaging after two cycles had a longer median OS compared to patients with stable or progressive disease (15.5 vs. 7.1 mo, p < 0.001). Previous taxane-based chemotherapy (HR 3.21, 95%CI 1.18-8.70, p = 0.02) and baseline LDH levels (HR 1.001, 95%CI 1.000-1.001, p = 0.04) were inversely associated with OS on a Cox-regression analysis. Grade ≥ 3 hematological decline was observed after 22/201 (11%) cycles with anemia, leukopenia and thrombocytopenia in 15/45 (33%), 6/45 (13%) and 8/45 (18%) patients, respectively.
Click to Show/Hide
|
||||
| Experiment 214 Reporting the Activity Data of This PDC | [35] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Leukopenia |
14.30%
|
|||
| Administration Time | Median of 4 (iqr: 2-7) cycles | ||||
| Administration Dosage | Mean cumulative activity of 30.7 ± 23.4 GBq | ||||
| MOA of PDC |
RLT with 177Lu-PSMA-617 can be effectively and safely initiated as early as 8 weeks after failure of 223Ra in patients with progressive bone-metastatic mCRPC refractory to 223Ra. Objective response can be achieved even in patients with more advanced disease and disseminated/diffuse bone metastases, albeit with increasing incidence of significant hematotoxicity.
Click to Show/Hide
|
||||
| Description |
Grade ≥ 3 hematological toxicity was observed in six patients after their last treatment cycle with anemia, leukopenia and thrombocytopenia in 5/28 (17.9%), 4/28 (14.3%) and 6/28 (21.4%) patients, respectively.
|
||||
| In Vivo Model | 28 men with progressive metastatic castration-resistant prostate cancer who median age 73 years, range 63-89 years). | ||||
| Experiment 215 Reporting the Activity Data of This PDC | [15] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Lymph node metastases |
77%
|
|||
| Patients Enrolled |
Patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 351 cycles | ||||
| Description |
A total of 51 patients (49%) died during the observation period. The majority of patients (97%) presented with bone metastases, 77% with lymph node metastases and 32% with visceral metastases.
|
||||
| Experiment 216 Reporting the Activity Data of This PDC | [41] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Lymphocytes decrease rate | ≥ 30% | |||
| Patients Enrolled |
734 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 5 doses (range: 1 to 6) | ||||
| Administration Dosage | Median cumulative dose 37.5 GBq (range, 7.0 to 48.3) | ||||
| MOA of PDC |
On March 23, 2022, the FDA approved 177Lu-PSMA-617 for the treatment of adult patients with PSMA-positive mCRPC who have been treated with androgen receptor pathway inhibition and taxane-based chemotherapy. The approval was based on a meaningful advantage in overall survival supported by a delay in tumor progression and higher objective response rate. The decision took into account several important factors unique to this applications context. Metastatic castration-resistant prostate cancer (mCRPC) is a life-threatening condition that lacks curative treatment, creating an unmet need. This product provides a novel mechanism of action as the first radioligand therapeutic agent for mCRPC providing anti-tumor effects in both bone and non-bone sites and may provide an opportunity to be combined with other available therapies with different toxicity profiles across mechanistic classes. Finally, 177Lu-PSMA-617 offers a different safety profile than other available systemic therapies which was determined to be acceptable for the indicated patient population, expanding treatment options that can be individualized to a patients preferences and comorbidities.
Click to Show/Hide
|
||||
| Description |
Serious adverse reactions occurred in 36% of patients who received 177Lu-PSMA-617 plus BSoC. Fatal adverse reactions occurred in 2.8% of patients who received 177Lu-PSMA-617 plus BSoC, including sepsis (0.9%), pancytopenia (0.6%), hepatic failure (0.4%), intracranial hemorrhage (0.2%), subdural hematoma (0.2%), ischemic stroke (0.2%), COVID-19 (0.2%), and aspiration pneumonia (0.2%). The 2 fatal adverse reactions of intracranial hemorrhage and subdural hematoma occurred in patients who had concurrent treatment-related thrombocytopenia. The most common adverse reactions (≥ 20%) occurring at a higher incidence in patients who received 177Lu-PSMA-617 plus BSoC were fatigue, dry mouth, nausea, anemia, decreased appetite, and constipation. The most common laboratory abnormalities that worsened from baseline in ≥ 30% of patients who received 177Lu-PSMA-617 plus BSoC were decreased lymphocytes, decreased hemoglobin, decreased leukocytes, decreased platelets, decreased calcium, and decreased sodium.
Click to Show/Hide
|
||||
| Experiment 217 Reporting the Activity Data of This PDC | [50] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Malondialdehyde increase rate |
0.55 µM
|
|||
| Patients Enrolled |
Prostate cancer and neuroendocrine tumor patients referred to therapy with <sup>177</sup>Lu-PSMA and <sup>177</sup>Lu-DOTATATE, respectively.
|
||||
| Administration Time | 48 h | ||||
| Administration Dosage | 5.5 GBq | ||||
| MOA of PDC |
Although RNT with 177Lu-DOTATATE/PSMA is known as a novel and effective therapy option for cancer that significantly improves the quality of life and survival of patients, it may have acute or chronic side effects. Therefore, any method that can ameliorate these side effects is useful in the RNT process. For this purpose, a few clinical studies have reported that antioxidants as free radical scavengers such as amifostine and vitamins C and E can reduce radioiodine-related side effects, particularly in salivary glands in thyroid cancer patients.
Click to Show/Hide
|
||||
| Description |
In total, 61 RNT cycles were evaluated in 34 patients with age of 65 ± 2.83 (median ± SE) years (range of 27-99); this total included 20 (59%) prostate cancer patients [35 cycles (57.4%)] and 14 patients (41%) with NET [26 cycles (42.6%)]. Of the 61 evaluated cycles, 27 cycles were given in the control group and 34 cycles were given in the intervention group. The serum level of MDA was significantly increased after treatment compared to before treatment (P = 0.02) in the control group, while no significant change in the serum level of MDA was observed in the intervention group (P = 0.52). The serum level of GSH was insignificantly decreased after treatment compared to before treatment in the control group and slightly increased after treatment in the intervention group (P > 0.05). The serum level of glutathione reductase was insignificantly increased in all groups of patients after treatment (P > 0.05).
Click to Show/Hide
|
||||
| Experiment 218 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Maximum standardized uptake value (SUVmax) |
18.2
|
|||
| Patients Enrolled |
31 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 2 cycles (range: 1-4) | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
A prospective single center phase II study included 31 patients with mCRPC who had progressed despite second-line hormonal therapy and/or docetaxel chemotherapy. The patients underwent an average of two cycles (range 1-4) of 177Lu-DKFZ-PSMA-617 therapy. The primary endpoints of the study were to determine radiographic progression-free survival (RPFS) using PET/CT scans and overall survival (OS). The treatment response was evaluated based on biochemical response using serum PSA, molecular response using PET/CT scans, and clinical response using VAS (visual analogue scale), AS (analgesic score) and ECOG (Eastern Cooperative Oncology Group) performance status. Biochemical response showed that the mean serum PSA level after three months of initial therapy was 141.75 ± 187.43 ng/mL (range 2.5-807). The mean serum PSA level three months after the second cycle was 153.07 ± 204 ng/mL (range 1.34-762). The molecular response estimated by the mean SUVmax (maximum standardized uptake value) of tumor lesions before and after therapy was 56.7 and 18.2 respectively. In two patients it was reduced from 32.67 to 0.38 after 177Lu-DKFZ-PSMA-617 therapy, thus indicating a complete remission. The clinical response was estimated using the mean VASmax and AS. The pre-therapy VASmax was 7.5 ± 1, and post-therapy was 3 ± 0.9 (p < 0.0001), while the mean AS pre-therapy and post therapy was 2.5 ± 1.09 and 1.8 ± 0.98 (p = 0.009) respectively, and mean ECOG performance status improved from 2.54 ± 0.85 to 1.78 ± 0.92 after completion of therapy (p = 0.001). The median overall survival was 16 months, and progression-free survival was 12 months. 16.1% patients died due to disease during follow-up. This trial particularly highlighted an improvement in the ECOG performance status in patients receiving 177Lu-DKFZ-PSMA-617 for the treatment of mCRPC.
Click to Show/Hide
|
||||
| Experiment 219 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Maximum standardized uptake value (SUVmax) |
56.7
|
|||
| Patients Enrolled |
31 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 2 cycles (range: 1-4) | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
A prospective single center phase II study included 31 patients with mCRPC who had progressed despite second-line hormonal therapy and/or docetaxel chemotherapy. The patients underwent an average of two cycles (range 1-4) of 177Lu-DKFZ-PSMA-617 therapy. The primary endpoints of the study were to determine radiographic progression-free survival (RPFS) using PET/CT scans and overall survival (OS). The treatment response was evaluated based on biochemical response using serum PSA, molecular response using PET/CT scans, and clinical response using VAS (visual analogue scale), AS (analgesic score) and ECOG (Eastern Cooperative Oncology Group) performance status. Biochemical response showed that the mean serum PSA level after three months of initial therapy was 141.75 ± 187.43 ng/mL (range 2.5-807). The mean serum PSA level three months after the second cycle was 153.07 ± 204 ng/mL (range 1.34-762). The molecular response estimated by the mean SUVmax (maximum standardized uptake value) of tumor lesions before and after therapy was 56.7 and 18.2 respectively. In two patients it was reduced from 32.67 to 0.38 after 177Lu-DKFZ-PSMA-617 therapy, thus indicating a complete remission. The clinical response was estimated using the mean VASmax and AS. The pre-therapy VASmax was 7.5 ± 1, and post-therapy was 3 ± 0.9 (p < 0.0001), while the mean AS pre-therapy and post therapy was 2.5 ± 1.09 and 1.8 ± 0.98 (p = 0.009) respectively, and mean ECOG performance status improved from 2.54 ± 0.85 to 1.78 ± 0.92 after completion of therapy (p = 0.001). The median overall survival was 16 months, and progression-free survival was 12 months. 16.1% patients died due to disease during follow-up. This trial particularly highlighted an improvement in the ECOG performance status in patients receiving 177Lu-DKFZ-PSMA-617 for the treatment of mCRPC.
Click to Show/Hide
|
||||
| Experiment 220 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Maximum standardized uptake value (SUVmax) |
15.7
|
|||
| Patients Enrolled |
56 patients with metastatic castration-resistant prostate cancer.
|
||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
Another prospective trial studied 56 patients with progressive mCRPC and rising PSA levels who then received 177Lu-PSMA. Clinical efficacy was assessed using the visual analogue scale for pain, PSA levels, median overall survival, and Gallium-68-labeled prostate-specific membrane antigen (68Ga-PSMA PET/CT) for objective response. There was a decline in PSA of greater than 80% in 23.2% of patients, a decline of greater than 50% in 58.9%, and a decline of greater than 30% in 66.1% of patients. Progressive disease was noted in 10.7% of patients with a rise in PSA level greater than 25%. 68Ga-PSMA PET/CT prior to PSMA radioligand therapy showed the median SUVmax of the target lesion to be 37.5, which decreased to 15.7 after PSMA RLT. Ga-PSMA PET/CT was used to measure response rates which included a partial remission in 56%, stable disease in 8%, and progressive disease in 36% of patients. The median progression-free survival was 13.7 months, and median overall survival was not reached. PET/CT results showing a decrease in SUV max of the target lesion are indicative of a favorable objective response to Lu-PSMA therapy.
Click to Show/Hide
|
||||
| Experiment 221 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Maximum standardized uptake value (SUVmax) |
37.5
|
|||
| Patients Enrolled |
56 patients with metastatic castration-resistant prostate cancer.
|
||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
Another prospective trial studied 56 patients with progressive mCRPC and rising PSA levels who then received 177Lu-PSMA. Clinical efficacy was assessed using the visual analogue scale for pain, PSA levels, median overall survival, and Gallium-68-labeled prostate-specific membrane antigen (68Ga-PSMA PET/CT) for objective response. There was a decline in PSA of greater than 80% in 23.2% of patients, a decline of greater than 50% in 58.9%, and a decline of greater than 30% in 66.1% of patients. Progressive disease was noted in 10.7% of patients with a rise in PSA level greater than 25%. 68Ga-PSMA PET/CT prior to PSMA radioligand therapy showed the median SUVmax of the target lesion to be 37.5, which decreased to 15.7 after PSMA RLT. Ga-PSMA PET/CT was used to measure response rates which included a partial remission in 56%, stable disease in 8%, and progressive disease in 36% of patients. The median progression-free survival was 13.7 months, and median overall survival was not reached. PET/CT results showing a decrease in SUV max of the target lesion are indicative of a favorable objective response to Lu-PSMA therapy.
Click to Show/Hide
|
||||
| Experiment 222 Reporting the Activity Data of This PDC | [58] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Mean absorbed dose |
0.06 Gy/MBq
|
|||
| Patients Enrolled |
Patients with prostate cancer.
|
||||
| Description |
Mean absorbed dose to kidneys, submandibular and parotid glands, liver, spleen, and bone marrow was 0.39, 0.44, 0.58, 0.1, 0.06, and 0.11 Gy/MBq, respectively. Median whole-body tumor-absorbed dose was 11.55 Gy and correlated with prostate-specific antigen (PSA) response at 12 wk. A median dose of 14.1 Gy was observed in patients achieving a PSA decline of at least 50%, versus 9.6 Gy for those achieving a PSA decline of less than 50% (P < 0.01). Of 11 patients receiving a tumor dose of less than 10 Gy, only one achieved a PSA response of at least 50%.
Click to Show/Hide
|
||||
| Experiment 223 Reporting the Activity Data of This PDC | [58] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Mean absorbed dose |
0.1 Gy/MBq
|
|||
| Patients Enrolled |
Patients with prostate cancer.
|
||||
| Description |
Mean absorbed dose to kidneys, submandibular and parotid glands, liver, spleen, and bone marrow was 0.39, 0.44, 0.58, 0.1, 0.06, and 0.11 Gy/MBq, respectively. Median whole-body tumor-absorbed dose was 11.55 Gy and correlated with prostate-specific antigen (PSA) response at 12 wk. A median dose of 14.1 Gy was observed in patients achieving a PSA decline of at least 50%, versus 9.6 Gy for those achieving a PSA decline of less than 50% (P < 0.01). Of 11 patients receiving a tumor dose of less than 10 Gy, only one achieved a PSA response of at least 50%.
Click to Show/Hide
|
||||
| Experiment 224 Reporting the Activity Data of This PDC | [58] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Mean absorbed dose |
0.11 Gy/MBq
|
|||
| Patients Enrolled |
Patients with prostate cancer.
|
||||
| Description |
Mean absorbed dose to kidneys, submandibular and parotid glands, liver, spleen, and bone marrow was 0.39, 0.44, 0.58, 0.1, 0.06, and 0.11 Gy/MBq, respectively. Median whole-body tumor-absorbed dose was 11.55 Gy and correlated with prostate-specific antigen (PSA) response at 12 wk. A median dose of 14.1 Gy was observed in patients achieving a PSA decline of at least 50%, versus 9.6 Gy for those achieving a PSA decline of less than 50% (P < 0.01). Of 11 patients receiving a tumor dose of less than 10 Gy, only one achieved a PSA response of at least 50%.
Click to Show/Hide
|
||||
| Experiment 225 Reporting the Activity Data of This PDC | [58] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Mean absorbed dose |
0.39 Gy/MBq
|
|||
| Patients Enrolled |
Patients with prostate cancer.
|
||||
| Description |
Mean absorbed dose to kidneys, submandibular and parotid glands, liver, spleen, and bone marrow was 0.39, 0.44, 0.58, 0.1, 0.06, and 0.11 Gy/MBq, respectively. Median whole-body tumor-absorbed dose was 11.55 Gy and correlated with prostate-specific antigen (PSA) response at 12 wk. A median dose of 14.1 Gy was observed in patients achieving a PSA decline of at least 50%, versus 9.6 Gy for those achieving a PSA decline of less than 50% (P < 0.01). Of 11 patients receiving a tumor dose of less than 10 Gy, only one achieved a PSA response of at least 50%.
Click to Show/Hide
|
||||
| Experiment 226 Reporting the Activity Data of This PDC | [58] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Mean absorbed dose |
0.44 Gy/MBq
|
|||
| Patients Enrolled |
Patients with prostate cancer.
|
||||
| Description |
Mean absorbed dose to kidneys, submandibular and parotid glands, liver, spleen, and bone marrow was 0.39, 0.44, 0.58, 0.1, 0.06, and 0.11 Gy/MBq, respectively. Median whole-body tumor-absorbed dose was 11.55 Gy and correlated with prostate-specific antigen (PSA) response at 12 wk. A median dose of 14.1 Gy was observed in patients achieving a PSA decline of at least 50%, versus 9.6 Gy for those achieving a PSA decline of less than 50% (P < 0.01). Of 11 patients receiving a tumor dose of less than 10 Gy, only one achieved a PSA response of at least 50%.
Click to Show/Hide
|
||||
| Experiment 227 Reporting the Activity Data of This PDC | [58] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Mean absorbed dose |
0.58 Gy/MBq
|
|||
| Patients Enrolled |
Patients with prostate cancer.
|
||||
| Description |
Mean absorbed dose to kidneys, submandibular and parotid glands, liver, spleen, and bone marrow was 0.39, 0.44, 0.58, 0.1, 0.06, and 0.11 Gy/MBq, respectively. Median whole-body tumor-absorbed dose was 11.55 Gy and correlated with prostate-specific antigen (PSA) response at 12 wk. A median dose of 14.1 Gy was observed in patients achieving a PSA decline of at least 50%, versus 9.6 Gy for those achieving a PSA decline of less than 50% (P < 0.01). Of 11 patients receiving a tumor dose of less than 10 Gy, only one achieved a PSA response of at least 50%.
Click to Show/Hide
|
||||
| Experiment 228 Reporting the Activity Data of This PDC | [39] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Mean intensity of PSMA tumour uptake hazard ratio |
0.89
|
|||
| Administration Time | After receiving 177lu-psma-617 treatment | ||||
| Description |
This analysis identified FDG-positive tumour volume (FDGvol; HR 2.6; 95% CI, 1.4-4.8), mean intensity of PSMA-avid tumour uptake (PSMAmean; HR 0.89; 95% CI, 0.8-0.98), bone scan index (BSI; HR 2.3; 95% CI, 1.2-4.4), ALP (HR 1.1; 95% CI, 1-1.2) and LDH (HR 1.2; 95% CI, 1-1.6) as biomarkers prognostic of overall survival.
|
||||
| In Vivo Model | Men with metastatic castrate-resistant prostate cancer. | ||||
| Experiment 229 Reporting the Activity Data of This PDC | [58] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median dose |
9.6 Gy/MBq
|
|||
| Patients Enrolled |
Patients achieving a psa decline of at least 50%.
|
||||
| Description |
Mean absorbed dose to kidneys, submandibular and parotid glands, liver, spleen, and bone marrow was 0.39, 0.44, 0.58, 0.1, 0.06, and 0.11 Gy/MBq, respectively. Median whole-body tumor-absorbed dose was 11.55 Gy and correlated with prostate-specific antigen (PSA) response at 12 wk. A median dose of 14.1 Gy was observed in patients achieving a PSA decline of at least 50%, versus 9.6 Gy for those achieving a PSA decline of less than 50% (P < 0.01). Of 11 patients receiving a tumor dose of less than 10 Gy, only one achieved a PSA response of at least 50%.
Click to Show/Hide
|
||||
| Experiment 230 Reporting the Activity Data of This PDC | [58] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median dose |
14.1 Gy/MBq
|
|||
| Patients Enrolled |
Patients achieving a psa decline of less than 50%.
|
||||
| Description |
Mean absorbed dose to kidneys, submandibular and parotid glands, liver, spleen, and bone marrow was 0.39, 0.44, 0.58, 0.1, 0.06, and 0.11 Gy/MBq, respectively. Median whole-body tumor-absorbed dose was 11.55 Gy and correlated with prostate-specific antigen (PSA) response at 12 wk. A median dose of 14.1 Gy was observed in patients achieving a PSA decline of at least 50%, versus 9.6 Gy for those achieving a PSA decline of less than 50% (P < 0.01). Of 11 patients receiving a tumor dose of less than 10 Gy, only one achieved a PSA response of at least 50%.
Click to Show/Hide
|
||||
| Experiment 231 Reporting the Activity Data of This PDC | [59] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median health-related quality of life (HRQoL) |
7.5 months
|
|||
| Patients Enrolled |
234 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 6 cycles | ||||
| MOA of PDC |
177Lu-PSMA-617 represents not just a new therapy but a new therapeutic class for the treatment of prostate cancer. As such, clinical pathways need to be developed and clinicians involved in the treatment of mCRPC must become familiar with these new processes in order to realize the benefits of RLT for their patients. While not all the suggestions included in this discussion are strictly evidence-based, it is the hope of the authors that this review of the evidence and associated expert opinions help practitioners translate these data into the current Canadian practice setting. Finally, as the therapeutic landscape for mCRPC continues to evolve, new treatments and emerging data will need to be considered when making treatment decisions.
Click to Show/Hide
|
||||
| Description |
In PSMAfore, which enrolled patients who were chemotherapy-nave, at the time of the second interim analysis median imaging-based PFS was 6.4 months longer in the 177Lu-PSMA-617 arm vs. the ARPI change arm (HR = 0.43; 95% CI 0.33-0.54; p < 0.0001), while there was no significant difference in median OS, which was 19.25 vs. 19.71 months in the 177Lu-PSMA-617 and ARPI change arms, respectively (HR = 1.18; 95% CI 0.83-1.64). It is important to note that a high crossover rate occurred, with 84.2% of patients who progressed in the ARPI change arm subsequently receiving 177Lu-PSMA-617, thus likely diminishing the between-arm differences.
Click to Show/Hide
|
||||
| Experiment 232 Reporting the Activity Data of This PDC | [59] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median health-related quality of life (HRQoL) |
14.3 months
|
|||
| Patients Enrolled |
551 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 6 cycles | ||||
| MOA of PDC |
177Lu-PSMA-617 represents not just a new therapy but a new therapeutic class for the treatment of prostate cancer. As such, clinical pathways need to be developed and clinicians involved in the treatment of mCRPC must become familiar with these new processes in order to realize the benefits of RLT for their patients. While not all the suggestions included in this discussion are strictly evidence-based, it is the hope of the authors that this review of the evidence and associated expert opinions help practitioners translate these data into the current Canadian practice setting. Finally, as the therapeutic landscape for mCRPC continues to evolve, new treatments and emerging data will need to be considered when making treatment decisions.
Click to Show/Hide
|
||||
| Description |
In the VISION trial, which enrolled patients with mCRPC who had received at least one line of ARPI treatment and one line of chemotherapy, 177Lu-PSMA-617 improved imaging-based progression-free survival (PFS) by 60% (hazard ratio [HR] = 0.40; 95% confidence interval [CI] 0.29-0.57; p < 0.001) and OS by 38% (HR = 0.62; 95% CI 0.52-0.74; p < 0.001) vs. trial-permitted best standard of care (SOC). The median imaging-based PFS was 8.7 months and median OS was 15.3 months for the 177Lu-PSMA-617 arm, vs. 3.4 months and 11.3 months, respectively, for the SOC arm.
Click to Show/Hide
|
||||
| Experiment 233 Reporting the Activity Data of This PDC | [60] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median hepatic progression-free survival |
5.7 months
|
|||
| Patients Enrolled |
28 patients with consecutive metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 4-6 cycles at 6 ± 2-week intervals | ||||
| Administration Dosage | 6.5 ± 0.5 GBq | ||||
| Evaluation Method | PET/CT assay | ||||
| MOA of PDC |
Recently, several studies demonstrated promising results of 177Lu-labeled prostate-specific membrane antigen radioligand therapy (177Lu-PSMA RLT) in late-stage/end-stage mCRPC. However, little is known about this modalitys efficacy specifically against liver metastases in this setting.
|
||||
| Description |
Median (minimum-maximum) follow-up was 37.5 (2.3-50.6) months. In liver metastases, complete or partial response was observed in 6 patients (21%) each, and stable disease in 1 (4%), for hepatic disease control in 46%. Overall, median (95% confidence interval) PFShep was 5.7 (2.2-9.2) months, and OS, 11.7 (3.0-20.4) months. Patients with hepatic disease control did not reach the median OS, while those with hepatic progressive disease had median OS (95% confidence interval) of 6.4 (1.6-11.1) months. In multivariate analysis, hepatic disease control by 177Lu-PSMA-617 RLT was significantly independently associated with OS, as was a prostate-specific antigen decline of ≥ 50% after 2 RLT cycles, and good baseline performance status (Eastern Cooperative Oncology Group 0-1). Hepatic tumor burden (≤ 25% vs. > 25% of liver volume) had no apparent relationship with hepatic tumor response, PFShep, or OS.
Click to Show/Hide
|
||||
| Experiment 234 Reporting the Activity Data of This PDC | [41] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median objective response rate (mORR) |
30%
|
|||
| Patients Enrolled |
319 patients with metastatic castration-resistant prostate cancer who underwent 4 cycles of mean 7.5 GBq Lu-PSMA 617 at 6weeks interval.
|
||||
| Administration Time | Every 6 weeks for up to a total of 6 doses | ||||
| Administration Dosage | 7.4 GBq (200 mCi) | ||||
| MOA of PDC |
On March 23, 2022, the FDA approved 177Lu-PSMA-617 for the treatment of adult patients with PSMA-positive mCRPC who have been treated with androgen receptor pathway inhibition and taxane-based chemotherapy. The approval was based on a meaningful advantage in overall survival supported by a delay in tumor progression and higher objective response rate. The decision took into account several important factors unique to this applications context. Metastatic castration-resistant prostate cancer (mCRPC) is a life-threatening condition that lacks curative treatment, creating an unmet need. This product provides a novel mechanism of action as the first radioligand therapeutic agent for mCRPC providing anti-tumor effects in both bone and non-bone sites and may provide an opportunity to be combined with other available therapies with different toxicity profiles across mechanistic classes. Finally, 177Lu-PSMA-617 offers a different safety profile than other available systemic therapies which was determined to be acceptable for the indicated patient population, expanding treatment options that can be individualized to a patients preferences and comorbidities.
Click to Show/Hide
|
||||
| Description |
The co-primary endpoint of OS was statistically significant, with patients randomized to receive 177Lu-PSMA-617 plus BSoC having prolonged OS (median estimate 15.3 months) compared to BSoC alone (median estimate 11.3 months), hazard ratio (HR) 0.62 (95% CI: 0.52, 0.74, p<0.001). The planned interim OS analysis was not necessary as the targeted number of OS events were observed before the targeted number of rPFS events. Therefore, the final OS analysis was evaluated at the time of rPFS analysis.
Click to Show/Hide
|
||||
| Experiment 235 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median overall survival (mOS) |
15.3 months
|
|||
| Patients Enrolled |
551 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 6 doses every 6 weeks plus bsoc | ||||
| Administration Dosage | 7.4 GBq | ||||
| MOA of PDC |
Lutetium Lu 177 vipivotide tetraxetan is a PSMA-binding ligand bound to a DOTA chelator (i.e., tetraxetan) radiolabeled with lutetium-177. Once lutetium Lu 177 vipivotide tetraxetan is bound to PSMA-expressing cells, the beta-minus emission from lutetium-177 delivers radiation to PSMA-expressing and surrounding cells, inducing DNA damage that leads to cell death. The exposure-efficacy relationships of lutetium Lu 177 vipivotide tetraxetan and the time course of the pharmacodynamic response are not fully characterized [9]. Lutetium-177 decays to a stable hafnium-177 with a physical half-life of 6.647 days by emitting beta-minus radiation with a maximum energy of 0.498 MeV (79%) and photonic radiation (γ) of 0.208 MeV (11%) and 0.113 MeV (6.4%).
Click to Show/Hide
|
||||
| Description |
Median OS was significantly longer with lutetium Lu 177 vipivotide tetraxetan plus BSoC (n = 551) than with BSoC alone (n = 280) [15.3 vs 11.3 months [HR 0.62 (95% CI 0.52-0.74); p < 0.001]. Median rPFS was 8.7 months in the lutetium Lu 177 vipivotide tetraxetan plus BSoC arm (n = 385) compared with 3.4 months in the BSoC alone arm (n = 196) [HR for progression or death 0.40 (99.2% CI 0.29-0.57); p < 0.001). The overall response rate was also significantly higher in lutetium Lu 177 vipivotide tetraxetan arm (n = 319 patients with evaluable disease at baseline) than in the BSoC alone arm (n = 120) [30% vs 2%; p < 0.001].
Click to Show/Hide
|
||||
| Half life period | 41.6 h | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT03511664 | Clinical Status | Phase 3 | ||
| Clinical Description | The primary objective of this study was to compare the two alternate primary endpoints of radiographic progression-free survival (rPFS) and overall survival (OS) in patients with progressive prostate-specific membrane antigen (PSMA)-positive metastatic castration-resistant prostate cancer (mCRPC) who received 177Lu-PSMA-617 in addition to best supportive/best standard of care (BSC/BSoC) versus patients treated with best supportive/best standard of care alone. | ||||
| Experiment 236 Reporting the Activity Data of This PDC | [55], [56] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median overall survival (mOS) |
15.3 months
|
|||
| Patients Enrolled |
Of the 1003 patients who underwent scanning, 831 (82.9%) were judged to have met all the trial eligibility criteria, including the PSMA imaging criteria, and were randomly assigned, between June 4, 2018, and October 23, 2019, to receive either <sup>177</sup>Lu-PSMA-617 plus protocol-permitted standard care (551 patients) or standard care alone (280).
Click to Show/Hide
|
||||
| Evaluation Method | PET/CT assay | ||||
| MOA of PDC |
Prostate-specific membrane antigen (PSMA)-targeted radiopharmaceutical like 177Lu-PSMA-617, a beta particle emitter has demonstrated improvement in overall survival in mCRPC patients pretreated with ARAT or taxanes. Although immune checkpoint inhibitors are being tested in mCRPC, there is no robust evidence to support this premise.
|
||||
| Description |
In an international phase III randomized controlled trial (VISION), men with PSMA positive mCRPC, previously treated with at least one ARAT and one or two taxane regimens, were randomly assigned in a 2 : 1 ratio to either 177Lu-PSMA-617 for four to six cycles and protocol-permitted standard of care vs. standard of care therapy alone. The addition of Lu-PSMA-617 to a standard of care therapy improved the imaging-based PFS (8.7 vs. 3.4 months, hazard ratio: 0.40, 99% CI, 0.29-0.57) and OS (15.3 vs. 11.3 months, hazard ratio: 0.62, 95% CI: 0.52-0.74).
Click to Show/Hide
|
||||
| Related Clinical Trial | |||||
| NCT Number | NCT03511664 | Clinical Status | Phase 3 | ||
| Experiment 237 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median overall survival (mOS) |
13.3 months
|
|||
| Patients Enrolled |
50 patients with progressive, PSMA-positive, symptomatic metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 4 cycles every 6 weeks | ||||
| Administration Dosage | 7.5 GBq (range 4-8.9 GBq) | ||||
| MOA of PDC |
Lutetium Lu 177 vipivotide tetraxetan is a PSMA-binding ligand bound to a DOTA chelator (i.e., tetraxetan) radiolabeled with lutetium-177. Once lutetium Lu 177 vipivotide tetraxetan is bound to PSMA-expressing cells, the beta-minus emission from lutetium-177 delivers radiation to PSMA-expressing and surrounding cells, inducing DNA damage that leads to cell death. The exposure-efficacy relationships of lutetium Lu 177 vipivotide tetraxetan and the time course of the pharmacodynamic response are not fully characterized [9]. Lutetium-177 decays to a stable hafnium-177 with a physical half-life of 6.647 days by emitting beta-minus radiation with a maximum energy of 0.498 MeV (79%) and photonic radiation (γ) of 0.208 MeV (11%) and 0.113 MeV (6.4%).
Click to Show/Hide
|
||||
| Description |
A PSA response (PSA reduction of ≥ 50% from baseline) was seen in 32 of 50 patients (64%) with progressive, PSMA-positive, symptomatic mCRPC who received up to 4 cycles of lutetium Lu 177 vipivotide tetraxetan every 6 weeks in the LuPSMA study (ACTRN12615000912583). 22 of 50 patients (44%) had a ≥ 80% decrease in PSA. At a median follow-up of 31.4 months, median OS was 13.3 months in the overall population and 18.4 months in those achieving a PSA response.
Click to Show/Hide
|
||||
| Half life period | 41.6 h | ||||
| Related Clinical Trial | |||||
| NCT Number | ACTRN12615000912583 | Clinical Status | Phase 2 | ||
| Clinical Description | Background: Lutetium-177 (177Lu)-PSMA-617 (LuPSMA) is a radiolabelled small molecule that binds with high affinity to prostate specific membrane antigen (PSMA) enabling targeted delivery of beta-radiation. We have previously reported favourable activity with low toxicity in a 30 patient study in men with metastatic castrate-resistant prostate cancer (mCRPC) and now report updated results including a twenty patient extension cohort. Methods: In this phase II trial, 50 patients with PSMA-avid mCRPC who had progressed after standard therapies received up to 4 cycles of LuPSMA every 6 weeks. The primary endpoints were PSA response (PCWG2) and toxicity (CTCAE v4). Other endpoints included imaging response, PSA PFS and OS. Cut-off for analysis 5 Oct 2018. Results: 76 men were screened to identify 50 patients eligible for treatment. Median PSA doubling time was 2.6 months. The majority of patients had received prior docetaxel (84%), cabazitaxel (48%), and abiraterone and/or enzalutamide (90%). The mean administered radioactivity was 7.5 GBq/cycle. PSA decline 50% was achieved in 32 of 50 patients (64%, 95% CI 50-77%), including 22 patients (44%, 95% CI 30-59%) with a PSA decline 80%. 27 patients had measurable soft tissue at baseline and 56% of these patients had a partial or complete response by RECIST 1.1. The most common toxicities attributed to LuPSMA were transient G1-2 dry mouth in 68%, G1-2 nausea in 48%, and G1-2 fatigue in 36%. G3-4 toxicities attributed to LuPSMA were infrequent with thrombocytopenia in 10% and anaemia in 10%. Median PSA PFS was 6.9 months (95% CI 6.0-8.7) and median OS was 13.3 months (95% CI 10.5-18.0). Upon subsequent progression, further LuPSMA was administered to 14 patients (median 2 cycles commencing 359 days from enrolment); PSA 50% response occurred in 9 patients (64%). Conclusions: This expanded 50 patient cohort confirms high response rates and low toxicity with LuPSMA in men who had progressed after standard therapies. In patients who subsequently progressed and were administered further LuPSMA, high response rates were also observed. These results have provided the basis for randomised controlled trials currently underway. | ||||
| Experiment 238 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median overall survival (mOS) |
14 months
|
|||
| Patients Enrolled |
43 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 4 cycles | ||||
| Administration Dosage | 6.0/7.4 GBq | ||||
| MOA of PDC |
Lutetium Lu 177 vipivotide tetraxetan is a PSMA-binding ligand bound to a DOTA chelator (i.e., tetraxetan) radiolabeled with lutetium-177. Once lutetium Lu 177 vipivotide tetraxetan is bound to PSMA-expressing cells, the beta-minus emission from lutetium-177 delivers radiation to PSMA-expressing and surrounding cells, inducing DNA damage that leads to cell death. The exposure-efficacy relationships of lutetium Lu 177 vipivotide tetraxetan and the time course of the pharmacodynamic response are not fully characterized [9]. Lutetium-177 decays to a stable hafnium-177 with a physical half-life of 6.647 days by emitting beta-minus radiation with a maximum energy of 0.498 MeV (79%) and photonic radiation (γ) of 0.208 MeV (11%) and 0.113 MeV (6.4%).
Click to Show/Hide
|
||||
| Description |
Treatment with lutetium Lu 177 vipivotide tetraxetan was associated with a median OS of 14 months in the RESIST-PC trial (NCT03042312). Eligible patients had progressive mCRPC after treatment with AR pathway inhibition, were either chemotherapy nave or were post chemotherapy and had sufficient PSMA expression by PSMA PET and were randomized to receive up to 4 cycles of lutetium Lu 177 vipivotide tetraxetan 6.0 or 7.4 GBq. The trial was terminated early because of sponsorship transfer; data are from 43 patients the US arm of the trial.
Click to Show/Hide
|
||||
| Half life period | 41.6 h | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT03042312 | Clinical Status | Phase 2 | ||
| Clinical Description | This was an open-label, multicenter, prospective trial to assess safety and efficacy of 177Lu-PSMA-617 in patients with metastatic castration resistant prostate cancer. | ||||
| Experiment 239 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median overall survival (mOS) |
14.5 months
|
|||
| Patients Enrolled |
254 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 3 median number cycles, delivered at a median interval of 5.7 weeks | ||||
| Administration Dosage | 6.5 GBq/cycle (median cumulative dose 21.2 GBq) | ||||
| MOA of PDC |
Lutetium Lu 177 vipivotide tetraxetan is a PSMA-binding ligand bound to a DOTA chelator (i.e., tetraxetan) radiolabeled with lutetium-177. Once lutetium Lu 177 vipivotide tetraxetan is bound to PSMA-expressing cells, the beta-minus emission from lutetium-177 delivers radiation to PSMA-expressing and surrounding cells, inducing DNA damage that leads to cell death. The exposure-efficacy relationships of lutetium Lu 177 vipivotide tetraxetan and the time course of the pharmacodynamic response are not fully characterized [9]. Lutetium-177 decays to a stable hafnium-177 with a physical half-life of 6.647 days by emitting beta-minus radiation with a maximum energy of 0.498 MeV (79%) and photonic radiation (γ) of 0.208 MeV (11%) and 0.113 MeV (6.4%).
Click to Show/Hide
|
||||
| Description |
A ≥ 50% reduction in PSA was seen in 52.0% of patients (132/254); at a median follow-up of 14.5 months, median PSA PFS was 5.5 months and median OS was 14.5 months. The median dose of lutetium Lu 177 vipivotide tetraxetan was 6.5 GBq/cycle (median cumulative dose 21.2 GBq), the median number cycles was 3, delivered at a median interval of 5.7 weeks.
Click to Show/Hide
|
||||
| Half life period | 41.6 h | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT04833517 | Clinical Status | Phase 2 | ||
| Clinical Description | This prospective registry aims to assess outcome and toxicity of targeted radionuclide therapies in patients with advanced prostate cancer in clinical routine. While the major investigated treatment modality is prostate-specific membrane antigen (PSMA)-targeted radioligand therapy, also other radionuclide therapies such as Ra223 and liver-directed radioembolization are included. The investigators believe that prospectively assessed long-term outcome data on implementation of radionuclide therapy, especially in the palliative setting of advanced mCRPC, help to better define the real benefits and risks of the respective treatment modalities for patients regarding survival and quality-of-life. | ||||
| Experiment 240 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median overall survival (mOS) |
15.2 months
|
|||
| Patients Enrolled |
27 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 7.4-22 gbq on days 1 and 15 in the p hase 1 dose-escalation co hort (n = 29); 22gbq on days 1 and 15 in the p hase 2 co hort (n = 21) | ||||
| Administration Dosage | 22 GBq | ||||
| MOA of PDC |
Lutetium Lu 177 vipivotide tetraxetan is a PSMA-binding ligand bound to a DOTA chelator (i.e., tetraxetan) radiolabeled with lutetium-177. Once lutetium Lu 177 vipivotide tetraxetan is bound to PSMA-expressing cells, the beta-minus emission from lutetium-177 delivers radiation to PSMA-expressing and surrounding cells, inducing DNA damage that leads to cell death. The exposure-efficacy relationships of lutetium Lu 177 vipivotide tetraxetan and the time course of the pharmacodynamic response are not fully characterized [9]. Lutetium-177 decays to a stable hafnium-177 with a physical half-life of 6.647 days by emitting beta-minus radiation with a maximum energy of 0.498 MeV (79%) and photonic radiation (γ) of 0.208 MeV (11%) and 0.113 MeV (6.4%).
Click to Show/Hide
|
||||
| Description |
A phase 1/2 study (NCT03042468) found that a single cycle of fractionated-dose of lutetium Lu 177 vipivotide tetraxetan [7.4-22 GBq on days 1 and 15 in the phase 1 dose-escalation cohort (n = 29); 22GBq on days 1 and 15 in the phase 2 cohort (n = 21); 27 patients treated at 22 GBq] was effective in patients with progressive mCRPC. A >50% PSA reduction was seen in 27 of 50 patients (54%); median PSA PFS was 5.6 months and median OS was 15.2 months.
Click to Show/Hide
|
||||
| Half life period | 41.6 h | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT03042468 | Clinical Status | Phase 1/2 | ||
| Clinical Description | The purpose of this study is to find the highest dose level of the study drug, 177Lu-PSMA-617 that can be given without severe side effects for advanced prostate cancer. | ||||
| Experiment 241 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median overall survival (mOS) |
19.7 months
|
|||
| Patients Enrolled |
56 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | On day 1 of each 6-week cycle | ||||
| Administration Dosage | 7.5 GBq | ||||
| MOA of PDC |
Lutetium Lu 177 vipivotide tetraxetan is a PSMA-binding ligand bound to a DOTA chelator (i.e., tetraxetan) radiolabeled with lutetium-177. Once lutetium Lu 177 vipivotide tetraxetan is bound to PSMA-expressing cells, the beta-minus emission from lutetium-177 delivers radiation to PSMA-expressing and surrounding cells, inducing DNA damage that leads to cell death. The exposure-efficacy relationships of lutetium Lu 177 vipivotide tetraxetan and the time course of the pharmacodynamic response are not fully characterized [9]. Lutetium-177 decays to a stable hafnium-177 with a physical half-life of 6.647 days by emitting beta-minus radiation with a maximum energy of 0.498 MeV (79%) and photonic radiation (γ) of 0.208 MeV (11%) and 0.113 MeV (6.4%).
Click to Show/Hide
|
||||
| Description |
A > 50% reduction in PSA after administration of up to 6 cycles of lutetium Lu 177 vipivotide tetraxetan plus idronoxil (a synthetic flavonoid derivative with radiosensitising properties) was seen in 34 of 56 (61%) patients with progressive mCRPC previously treated with AR pathway inhibition and taxanes in the phase 1/2 LuPin trial (ACTRN12618001073291). The median PSA PFS was 7.5 months and median OS was 19.7 months. Patients received lutetium Lu 177 vipivotide tetraxetan 7.5 GBq on day 1 of each 6-week cycle, with escalating doses of NOX66 on days 1-10 of a 6-week cycle.
Click to Show/Hide
|
||||
| Half life period | 41.6 h | ||||
| Related Clinical Trial | |||||
| NCT Number | ACTRN12618001073291 | Clinical Status | Phase 1/2 | ||
| Clinical Description | Background: Trials of lutetium prostate specific membrane antigen (PSMA) in men with metastatic castration-resistant prostate cancer (mCRPC) have demonstrated good safety and efficacy, but combination strategies may improve outcomes. Idronoxil is a synthetic flavonoid derivative with radiosensitising properties. 2. Objective: To evaluate the safety and activity of 177Lu PSMA 617 (LuPSMA-617) in combination with idronoxil suppositories (NOX66) in patients with end-stage mCRPC. 3. Design, setting, and participants: Thirty-two men with progressive mCRPC previously treated with taxane-based chemotherapy (91% treated with both docetaxel and cabazitaxel) and abiraterone and/or enzalutamide were enrolled in this phase I dose escalation study with phase II dose expansion. 4. Intervention: Screening with 68Ga PSMA and 18F-fludeoxyglucose positron emission tomography (PET)/computed tomography (CT) was performed. Men received up to six cycles of LuPSMA-617 (7.5 GBq) on day 1, with escalating doses of NOX66 on days 110 of a 6-wk cycle. Cohort 1 (n = 8) received 400 mg and cohort 2 (n = 24) 800 mg of NOX66. 5. Outcome measurements and statistical analysis: Adverse events (AEs), pain inventory scores, prostate-specific antigen (PSA) response, progression-free survival, and overall survival were evaluated. | ||||
| Experiment 242 Reporting the Activity Data of This PDC | [59] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median overall survival (mOS) |
15.3 months
|
|||
| Patients Enrolled |
551 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 6 cycles | ||||
| MOA of PDC |
177Lu-PSMA-617 represents not just a new therapy but a new therapeutic class for the treatment of prostate cancer. As such, clinical pathways need to be developed and clinicians involved in the treatment of mCRPC must become familiar with these new processes in order to realize the benefits of RLT for their patients. While not all the suggestions included in this discussion are strictly evidence-based, it is the hope of the authors that this review of the evidence and associated expert opinions help practitioners translate these data into the current Canadian practice setting. Finally, as the therapeutic landscape for mCRPC continues to evolve, new treatments and emerging data will need to be considered when making treatment decisions.
Click to Show/Hide
|
||||
| Description |
In the VISION trial, which enrolled patients with mCRPC who had received at least one line of ARPI treatment and one line of chemotherapy, 177Lu-PSMA-617 improved imaging-based progression-free survival (PFS) by 60% (hazard ratio [HR] = 0.40; 95% confidence interval [CI] 0.29-0.57; p < 0.001) and OS by 38% (HR = 0.62; 95% CI 0.52-0.74; p < 0.001) vs. trial-permitted best standard of care (SOC). The median imaging-based PFS was 8.7 months and median OS was 15.3 months for the 177Lu-PSMA-617 arm, vs. 3.4 months and 11.3 months, respectively, for the SOC arm.
Click to Show/Hide
|
||||
| Experiment 243 Reporting the Activity Data of This PDC | [59] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median overall survival (mOS) |
19.2 months
|
|||
| Patients Enrolled |
234 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 6 cycles | ||||
| MOA of PDC |
177Lu-PSMA-617 represents not just a new therapy but a new therapeutic class for the treatment of prostate cancer. As such, clinical pathways need to be developed and clinicians involved in the treatment of mCRPC must become familiar with these new processes in order to realize the benefits of RLT for their patients. While not all the suggestions included in this discussion are strictly evidence-based, it is the hope of the authors that this review of the evidence and associated expert opinions help practitioners translate these data into the current Canadian practice setting. Finally, as the therapeutic landscape for mCRPC continues to evolve, new treatments and emerging data will need to be considered when making treatment decisions.
Click to Show/Hide
|
||||
| Description |
In PSMAfore, which enrolled patients who were chemotherapy-nave, at the time of the second interim analysis median imaging-based PFS was 6.4 months longer in the 177Lu-PSMA-617 arm vs. the ARPI change arm (HR = 0.43; 95% CI 0.33-0.54; p < 0.0001), while there was no significant difference in median OS, which was 19.25 vs. 19.71 months in the 177Lu-PSMA-617 and ARPI change arms, respectively (HR = 1.18; 95% CI 0.83-1.64). It is important to note that a high crossover rate occurred, with 84.2% of patients who progressed in the ARPI change arm subsequently receiving 177Lu-PSMA-617, thus likely diminishing the between-arm differences.
Click to Show/Hide
|
||||
| Experiment 244 Reporting the Activity Data of This PDC | [53] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median overall survival (mOS) |
1.6 years
|
|||
| Administration Time | 1-7 cycles | ||||
| Administration Dosage | 7081 MBq (IQR 6995-7188) | ||||
| Evaluation Method | 18F/68Ga-PSMA PET/CT assay | ||||
| MOA of PDC |
177Lu-PSMA-RLT in a four-week interval with a fixed dose was safe and effective. A significant PSA response was observed in six out of ten patients, which was also associated with better OS and PFS. A shorter treatment interval may broaden the therapeutic window among mCRPC patients with high volume disease and rapidly rising PSA. Pre-treatment staging PSMA was not helpful in distinguishing responders from non-responders. However, parameters for tumor burden and its activity provide prognostic information related to OS and PFS.
Click to Show/Hide
|
||||
| Description |
The median follow-up time was 1.7 years (y; IQR 0.7-2.2). The median PSA progression-free survival was 0.4 y (IQR 0.2-0.8) and the OS was 1.6 y (IQR 0.7-2.2). During follow-up, 36 (58%) patients died. The survival probability was significantly better among patients with significant (>50%) PSA response compared to non-responders, p < 0.04.
|
||||
| In Vivo Model | This is a single-center retrospective analysis in 62 men with pathologically confirmed castration resistant metastatic prostate cancer who were treated with 177Lu-PSMA-617 during January 2017-February 2019. | ||||
| Experiment 245 Reporting the Activity Data of This PDC | [61] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median overall survival (mOS) |
5.7 months
|
|||
| Patients Enrolled |
Patients with metastatic castration-resistant prostate cancer and liver metastases.
|
||||
| Administration Time | 7-8 wk | ||||
| Administration Dosage | 6-7.5 MBq/cycle | ||||
| Description |
Median estimated survival was 5.7 mo for 177Lu-PSMA alone and 8.4 mo for combined sequential 177Lu-PSMA and SIRT.
|
||||
| Experiment 246 Reporting the Activity Data of This PDC | [62] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median overall survival (mOS) |
8 months
|
|||
| Patients Enrolled |
58 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 1 to 5 cycles | ||||
| Administration Dosage | Average administered total cumulative dose of 13.32 GBq | ||||
| MOA of PDC |
Thus, the combination of 177Lu-PSMA-617 PRLT and AA therapy significantly improved patient's symptoms, PFS and OS as compared to only 177Lu-PSMA PRLT monotherapy in this study analysis. Based upon this promising observation, future prospective randomized controlled, multicenter clinical trials in a larger number of patients would be warranted to confirm this documented benefit of the combined 177Lu-PSMA-617 PRLT and AA therapy approach versus 177Lu-PSMA-617 PRLT monotherapy in patients of mCRPC.
Click to Show/Hide
|
||||
| Description |
On comparison of the treatment outcome between two groups, significant p value was found for symptomatic responders (58% in Group 1 vs. 85% in Group 2), median PFS (7 months in Group 1 vs. not reached in Group 2), and median OS (8 months in Group 1 vs. 16 months in Group 2), with better outcome in Group 2 patients for these variables.
|
||||
| Experiment 247 Reporting the Activity Data of This PDC | [61] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median overall survival (mOS) |
8.4 months
|
|||
| Patients Enrolled |
Patients with metastatic castration-resistant prostate cancer and liver metastases.
|
||||
| Administration Time | 7-8 wk | ||||
| Administration Dosage | 6-7.5 MBq/cycle (Combined sequential 177Lu-PSMA and SIRT) | ||||
| Description |
Median estimated survival was 5.7 mo for 177Lu-PSMA alone and 8.4 mo for combined sequential 177Lu-PSMA and SIRT.
|
||||
| Experiment 248 Reporting the Activity Data of This PDC | [19] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median overall survival (mOS) |
8.5 months
|
|||
| Patients Enrolled |
25 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | A median of four (iqr: 2-6) cycles every 6-8 weeks | ||||
| Administration Dosage | Mean of 7.7 ± 1.4 GBq/cycle | ||||
| MOA of PDC |
The response to radioligand therapy with 177Lu-PSMA-617 seems to be independent of the presence of early-onset prostate cancer (EOPC); however, the less favorable survival outcome observed in our study may indicate a more aggressive disease course. Expectedly, the safety of LuPSMA-RLT does not seem to be compromised in metastasized castration-resistant EOPC patients. Comparative studies on age at diagnosis of prostate cancer and the patients outcome after LuPSMA-RLT are needed.
Click to Show/Hide
|
||||
| Description |
The median progression-free survival (PFS) was 3.8 months (95% CI 2.3-5.3), and overall survival (OS) was 8.5 months (95% CI 6.2-10.8).
|
||||
| Experiment 249 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median overall survival (mOS) |
8.5 months
|
|||
| Patients Enrolled |
25 patients with prostate cancer.
|
||||
| Administration Time | A median of four cycles | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
Another retrospective study studied 25 patients less than 55 years of age at prostate cancer diagnosis who were treated with a median of four cycles (range 2-6) of 177Lu-PSMA-617. The median PFS was 3.8 months (95% CI 2.5-5.3) and OS was 8.5 months (95% 6.2-10.8). An initial PSA reduction of greater than 50% was seen in 36% of patients but not associated with OS benefit (p = 0.601). A PSA response greater than 50% at three months was seen in 48% of patients and associated with improvement in OS (16 months, 95% CI 7.4-24.6 versus 4.0 months, 95% CI: 1.1-6.9, p = 0.002). They also used 68Ga-PSMA-PET/CT and correlated imaging response after up to three cycles in 44% of patients. Responders had a longer median PFS (8.7 months, 95% CI 1.3-16.1 vs. 1.9 months, 95% CI 1.7-2.2, p < 0.001) and OS (16.0 months, 95% CI 7.6-24.4 vs. 4.0 months, 95% CI 0.9-7.1; p = 0.002).
Click to Show/Hide
|
||||
| Experiment 250 Reporting the Activity Data of This PDC | [63] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median overall survival (mOS) |
9.9 months
|
|||
| Patients Enrolled |
Patients with metastatic castration-resistant prostate cancer.
|
||||
| Experiment 251 Reporting the Activity Data of This PDC | [42] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median overall survival (mOS) |
10.2 months
|
|||
| Patients Enrolled |
45 patients with progressive metastatic castration-resistant prostate cancer and diffuse bone marrow involvement.
|
||||
| Administration Time | 4 cycles | ||||
| Administration Dosage | 7.4 ± 1.4 GBq | ||||
| Evaluation Method | 68Ga-PSMA-11 PET/CT assay | ||||
| MOA of PDC |
Our findings suggest that repeated cycles of RLT with 177Lu-PSMA-617 can be carried out at an acceptable safety profile in mCRPC patients with diffuse bone marrow involvement. RLT may provide a suitable strategy for prolonged disease control with substantial clinical benefit. After a minimum of two cycles, treatment response translated into significantly longer median OS. Further studies should be carried out to investigate the role of individualized RLT concepts in this advanced stage setting.
Click to Show/Hide
|
||||
| Description |
Median imaging-based progression-free survival (PFS) was 6.4 mo (95% CI, 3.0-9.8) and the median overall survival (OS) was 10.2 months (95% CI, 7.2-12.8). The biochemical response translated into a significantly prolonged PFS (12.9 vs. 2.8 mo, p < 0.001) and OS (13.5 vs. 6.7 mo, p < 0.001).
|
||||
| Experiment 252 Reporting the Activity Data of This PDC | [21] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median overall survival (mOS) |
10.7 months
|
|||
| Patients Enrolled |
Patients with metastatic castration-resistant prostate cancer; taxane chemotherapy pretreated.
|
||||
| Experiment 253 Reporting the Activity Data of This PDC | [22] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median overall survival (mOS) |
11.1 months
|
|||
| Patients Enrolled |
416 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 3 cycles | ||||
| MOA of PDC |
The PSMA molecule acts as a target for theranostics in detecting and treating prostatic lesions. This ultimately promotes the concept of precision and personalized medicine. Several published articles showed favorable outcomes of Lu-PSMA-PRLT in mCRPC patients, which quickly translated into routine clinical practices with real effectiveness, a low toxicity profile, and documentation of the risk-benefit of PRLT. Nevertheless, many questions related to PRLT remain unresolved such as the sequencing of PRLT with ARTA or taxane-based chemotherapy, re-challenge therapy, combined therapy, alpha therapy in mCRPC patients, and early treatment of PRLT in mHNPC patients. To solve these questions, several clinical trials are currently under way, and the results of these trials will be helpful in deciding treatment strategies for prostate cancer patients.
Click to Show/Hide
|
||||
| Description |
Since initial retrospective studies had a limited number of patients and a heterogeneous population, the WARMTH (World Association of Radiopharmaceutical and Molecular Therapy) planned a multi-center retrospective study to evaluate response rate, OS, and the impact of prior therapies on OS in more than 300 mCRPC patients treated with 177Lu-PSMA-617. The study included 416 mCRPC patients who received a total of 1493 cycles of 177Lu-PSMA-617, with a median of 3 cycles per patient. Post-177Lu-PSMA-617, serum PSA decline was seen in 282 (71.8%) patients, of whom 163 (41.5%) showed a serum PSA decline of ≥50%, whereas 111 patients (28.2%) showed an increase in serum PSA levels. A median OS of 11.1 months (95% CI 9.7-12.5 months) was observed. Prior chemotherapy, the presence of bone and liver metastases, and poor ECOG status were significant adverse prognosticators for survival in both univariate and multivariate analyses. No imaging response evaluation and no determination of PFS after 177Lu-PSMA-617 were major limitations for this study.
Click to Show/Hide
|
||||
| Experiment 254 Reporting the Activity Data of This PDC | [16] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median overall survival (mOS) |
11.3 months
|
|||
| Patients Enrolled |
Patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | Every 6weeks | ||||
| Administration Dosage | 7.5 GBq | ||||
| Description |
There was no significant difference comparing the rate of > 50% PSA decline or best PSA response between the 6.0 GBq and 7.5 GBq group (35% vs. 54%, p = 0.065; and - 40.2% vs. - 57.8%, p = 0.329). The median estimated survival and PSA-PFS did not significantly differ between the 6.0 GBq and 7.5 GBq groups as well (11.3 vs. 12.7 months, p = 0.384; and 9.5 vs. 12.3 months, p = 0.258).
Click to Show/Hide
|
||||
| Experiment 255 Reporting the Activity Data of This PDC | [31] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median overall survival (mOS) |
11.3 months
|
|||
| Patients Enrolled |
Patients with advanced metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 1 cycle | ||||
| Administration Dosage | 6 GBq | ||||
| Description |
During a median follow-up length of 13.7 months (range, 9.8-32.3 months), median overall survival from start of the first therapy cycle was 11.3 months (range, 1.4-32.3 months).
|
||||
| Experiment 256 Reporting the Activity Data of This PDC | [45] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median overall survival (mOS) |
12.0 months
|
|||
| Patients Enrolled |
23 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 39.1 months | ||||
| Administration Dosage | 6 GBq (162.16 mCi) | ||||
| MOA of PDC |
This study shows that PSA changes in patients with mCRPC as early as four weeks after the first administration of PSMA-RLT are predictive of both long-term biochemical and PET imaging responses, as well as overall survival. At this early stage, a PSA decrease of at least 30% was found to be more suitable to detect future responders, as well as a longer overall survival compared to the threshold of 50% proposed by the PCWG for long-term biochemical evaluation. An early increase in PSA (+25%) is a strong predictor for biochemical progression and shorter overall survival. Larger prospective studies are warranted to validate these findings and provide criteria for the early assessment of PSMA-RLT, including even more lenient thresholds, as suggested by our explorative retrospective ROC analysis.
Click to Show/Hide
|
||||
| Description |
Patient follow-up was of over 51 months, with the median follow-up (reverse Kaplan-Meier estimator) being 39.1 months (95% CI 32.1-46.1). Median survival was 12.0 (95% CI 10.8-13.2) months, with five patients (19%) still alive at the last follow-up. There were no therapy-related deaths documented. At w16, 14 patients (52%) stated an improvement in pain status from the baseline of at least one tier/level, 11 of which were biochemical responders.
Click to Show/Hide
|
||||
| Experiment 257 Reporting the Activity Data of This PDC | [22] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median overall survival (mOS) |
12 months
|
|||
| Patients Enrolled |
40 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 2-5 cycles | ||||
| Administration Dosage | 4.44-5.55 GBq/cycle | ||||
| MOA of PDC |
The PSMA molecule acts as a target for theranostics in detecting and treating prostatic lesions. This ultimately promotes the concept of precision and personalized medicine. Several published articles showed favorable outcomes of Lu-PSMA-PRLT in mCRPC patients, which quickly translated into routine clinical practices with real effectiveness, a low toxicity profile, and documentation of the risk-benefit of PRLT. Nevertheless, many questions related to PRLT remain unresolved such as the sequencing of PRLT with ARTA or taxane-based chemotherapy, re-challenge therapy, combined therapy, alpha therapy in mCRPC patients, and early treatment of PRLT in mHNPC patients. To solve these questions, several clinical trials are currently under way, and the results of these trials will be helpful in deciding treatment strategies for prostate cancer patients.
Click to Show/Hide
|
||||
| Description |
Suman et al. evaluated the efficacy of 177Lu-PSMA-617 in heavily pre-treated mCRPC patients. A total of 40 mCRPC patients who received at least 2 cycles of 177Lu-PSMA-617 were included in this study. Twenty-one (52.5%) patients were responders (CR, PR, and SD) and 19 (47.5%) patients were non-responders (PD) on both symptomatic and biochemical scales. As per PET response criteria in solid tumor (PERCIST) criteria, 16 patients (43%) and 21 patients (57%) were responders and non-responders, respectively, on 68Ga-PSMA-11 PET/CT imaging. Metastatic nodal lesions responded better compared to liver and bony lesions. The median OS of 12 months and the median PFS of 7 months were registered without any grade 3/4 toxicity. The authors concluded that 177Lu-PSMA-617 controlled disease with good symptomatic and biochemical response rates without any high-grade clinical toxicity.
Click to Show/Hide
|
||||
| Experiment 258 Reporting the Activity Data of This PDC | [22] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median overall survival (mOS) |
12 months
|
|||
| Patients Enrolled |
30 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 3 cycles | ||||
| Administration Dosage | 3.8-6.7 GBq/cycle | ||||
| MOA of PDC |
The PSMA molecule acts as a target for theranostics in detecting and treating prostatic lesions. This ultimately promotes the concept of precision and personalized medicine. Several published articles showed favorable outcomes of Lu-PSMA-PRLT in mCRPC patients, which quickly translated into routine clinical practices with real effectiveness, a low toxicity profile, and documentation of the risk-benefit of PRLT. Nevertheless, many questions related to PRLT remain unresolved such as the sequencing of PRLT with ARTA or taxane-based chemotherapy, re-challenge therapy, combined therapy, alpha therapy in mCRPC patients, and early treatment of PRLT in mHNPC patients. To solve these questions, several clinical trials are currently under way, and the results of these trials will be helpful in deciding treatment strategies for prostate cancer patients.
Click to Show/Hide
|
||||
| Description |
Yordanova et al., evaluated the response rate and clinical toxicity of re-challenge 177Lu-PSMA-617 in progressive prostatic cancer patients who previously benefited from this therapy. In this retrospective study, a total of 30 patients were re-treated with a median of 3 (range 1-6) cycles of 177Lu-PSMA-617. They found that 75-90% of patients demonstrated favorable serum PSA responses following re-challenge cycles, with a median OS of 12 months after the first re-challenge cycle and without any life-threatening grade-4 adverse event. The authors concluded that the majority of patients benefited from re-challenging 177Lu-PSMA-617 with a longer OS in biochemically responsive patients. At present, data on re-challenge 177Lu-PSMA-617 is limited and requires a prospective randomized trial before a definitive conclusion.
Click to Show/Hide
|
||||
| Experiment 259 Reporting the Activity Data of This PDC | [16] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median overall survival (mOS) |
12.7 months
|
|||
| Patients Enrolled |
Patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | Every 8weeks | ||||
| Administration Dosage | 6.0 GBq | ||||
| Description |
There was no significant difference comparing the rate of > 50% PSA decline or best PSA response between the 6.0 GBq and 7.5 GBq group (35% vs. 54%, p = 0.065; and - 40.2% vs. - 57.8%, p = 0.329). The median estimated survival and PSA-PFS did not significantly differ between the 6.0 GBq and 7.5 GBq groups as well (11.3 vs. 12.7 months, p = 0.384; and 9.5 vs. 12.3 months, p = 0.258).
Click to Show/Hide
|
||||
| Experiment 260 Reporting the Activity Data of This PDC | [9] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median overall survival (mOS) |
13.3 months
|
|||
| Patients Enrolled |
Patients with PSMA-avid metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 4 cycles; every 6 wk | ||||
| Administration Dosage | 7.5 GBq/cycle | ||||
| Description |
median overall survival was 13.3 mo (95% CI, 10.5-18.7 mo)
|
||||
| Experiment 261 Reporting the Activity Data of This PDC | [36] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median overall survival (mOS) |
13.5 months
|
|||
| Patients Enrolled |
56 patients with metastatic castration-resistant prostate cancer.
|
||||
| Description |
In a study of 56 patients, Chen et al. found that 23.2% had at least one PSMA (-)/FDG (+) lesion, and that PSA and Gleason score were both higher in these patients with discordant hypermetabolic disease. A sub-analysis of a single center phase II trial of 177Lu PSMA-617 RLT similarly found that 16/50 patients had at least one PSMA (-)/FDG (+) lesion and were deemed ineligible for 177Lu PSMA-617 therapy. The OS of these patients with discordant hypermetabolic disease was 2.6 months (compared to 13.5 months for patients that received 177Lu PSMA-617).
Click to Show/Hide
|
||||
| Experiment 262 Reporting the Activity Data of This PDC | [22] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median overall survival (mOS) |
13.5 months
|
|||
| Patients Enrolled |
30 patients with metastatic castration-resistant prostate cancer who underwent 4 cycles of mean 7.5 GBq Lu-PSMA 617 at 6weeks interval.
|
||||
| Administration Time | 1-4 cycles | ||||
| Administration Dosage | 4.4-8.7 GBq/cycle | ||||
| MOA of PDC |
The PSMA molecule acts as a target for theranostics in detecting and treating prostatic lesions. This ultimately promotes the concept of precision and personalized medicine. Several published articles showed favorable outcomes of Lu-PSMA-PRLT in mCRPC patients, which quickly translated into routine clinical practices with real effectiveness, a low toxicity profile, and documentation of the risk-benefit of PRLT. Nevertheless, many questions related to PRLT remain unresolved such as the sequencing of PRLT with ARTA or taxane-based chemotherapy, re-challenge therapy, combined therapy, alpha therapy in mCRPC patients, and early treatment of PRLT in mHNPC patients. To solve these questions, several clinical trials are currently under way, and the results of these trials will be helpful in deciding treatment strategies for prostate cancer patients.
Click to Show/Hide
|
||||
| Description |
In 2018, a phase II trial on 177Lu-PSMA-617 (LuPSMA trial) was published by Hofman et al. In this study, they included a total of 30 mCRPC patients who showed PD on standard therapies and received 1-4 cycles with 7.5 GBq of 177Lu-PSMA-617 (range: 4.4-8.7 GBq). They found >50% PSA decline in 17 patients (57%) and an objective response rate of 40%, 37%, and 37% of patients on 68Ga PSMA-11, FDG-PET/CT, and bone imaging, respectively. The median PFS was 7.6 months, and the median OS was 13.5 months after 177Lu-PSMA-617. Improvement in pain level was noted in 27 patients (90%), which significantly contributed to a better quality of life. 177Lu-PSMA-617 was well tolerated with minimal side effects. Commonly seen side effects were grade 1 dryness of mouth (87%), grade 1-2 transient nausea (50%) and fatigue (50%). Uncommonly seen side effects included grade 3-4 thrombocytopenia (13%), grade 3 anemia (13%), and neutropenia (7%). This was the first prospective single-arm, single-center, phase II study on the use of 177Lu-PSMA-617 in mCRPC patients.
Click to Show/Hide
|
||||
| Experiment 263 Reporting the Activity Data of This PDC | [22], [26] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median overall survival (mOS) |
13.7 months
|
|||
| Patients Enrolled |
175 metastatic castration-resistant prostate cancer (mCRPC) patient were included in this meta-analysis. Median OS was 13.7 months.
|
||||
| Administration Dosage | 3.7-8.7 GBq/cycle | ||||
| MOA of PDC |
The PSMA molecule acts as a target for theranostics in detecting and treating prostatic lesions. This ultimately promotes the concept of precision and personalized medicine. Several published articles showed favorable outcomes of Lu-PSMA-PRLT in mCRPC patients, which quickly translated into routine clinical practices with real effectiveness, a low toxicity profile, and documentation of the risk-benefit of PRLT. Nevertheless, many questions related to PRLT remain unresolved such as the sequencing of PRLT with ARTA or taxane-based chemotherapy, re-challenge therapy, combined therapy, alpha therapy in mCRPC patients, and early treatment of PRLT in mHNPC patients. To solve these questions, several clinical trials are currently under way, and the results of these trials will be helpful in deciding treatment strategies for prostate cancer patients.
Click to Show/Hide
|
||||
| Description |
Yadav et al. provided a meta-analysis of 177Lu-PSMA-PRLT for treating mCRPC patients. They analyzed 16 articles (13 articles used 177Lu-PSMA-617, 2 articles used 177Lu-PSMA-I&T, and 1 article used both radioligands). The authors showed >50% PSA decline after 177Lu-PSMA-PRLT in 46% of patients. Anatomical imaging response as per the RECIST criteria was reported by eight studies, with a proportion of 37.2% of patients had PR, SD in 38.3% of patients and PD in 24.5% of patients, whereas molecular imaging response as per the PERCIST criteria demonstrated PR in 74 patients (44.3%), SD in 39 patients (23.4%), and PD in 54 patients (32.3%). Common clinical toxicities were grades 1-2, which included anemia (23%), leukopenia (14.2%), thrombocytopenia (15%), nephrotoxicity (9.5%), and xerostomia (14.5%). The authors observed significant heterogeneity in several studies while analyzing this meta-analysis. They concluded that 177Lu-PSMA-PRLT is a promising treatment modality in mCRPC patients who showed PD after standard care treatments.
Click to Show/Hide
|
||||
| Experiment 264 Reporting the Activity Data of This PDC | [64] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median overall survival (mOS) |
14 months
|
|||
| Patients Enrolled |
Patients with progressive disease (PD) on second-line hormonal therapy and/or docetaxel chemotherapy.
|
||||
| Administration Time | 8- to 12-weekly intervals | ||||
| Administration Dosage | 3.7 to 8 GBq | ||||
| Description |
The disease control rates according to the radiographic and molecular response were 77% and 71%, respectively. The median overall survival and median progression-free survivals were 14 and 11.8 months, respectively.
|
||||
| Experiment 265 Reporting the Activity Data of This PDC | [22], [23] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median overall survival (mOS) |
14 months
|
|||
| Patients Enrolled |
Twelve studies including 669 metastatic castration-resistant prostate cancer patients reported <sup>177</sup>Lu-PSMA radioligand therapy(RLT). In evaluable articles, the patients had a median overall survival of 14 months.
|
||||
| MOA of PDC |
The PSMA molecule acts as a target for theranostics in detecting and treating prostatic lesions. This ultimately promotes the concept of precision and personalized medicine. Several published articles showed favorable outcomes of Lu-PSMA-PRLT in mCRPC patients, which quickly translated into routine clinical practices with real effectiveness, a low toxicity profile, and documentation of the risk-benefit of PRLT. Nevertheless, many questions related to PRLT remain unresolved such as the sequencing of PRLT with ARTA or taxane-based chemotherapy, re-challenge therapy, combined therapy, alpha therapy in mCRPC patients, and early treatment of PRLT in mHNPC patients. To solve these questions, several clinical trials are currently under way, and the results of these trials will be helpful in deciding treatment strategies for prostate cancer patients.
Click to Show/Hide
|
||||
| Description |
A systematic review on the comparison of 177Lu-PSMA-PRLT with third-line treatments such as abiraterone, enzalutamide, and cabazitaxel was published by Von Eyben et al. A significant difference of PSA response was seen between the two groups (a PSA decline of ≥50% in 44% of patients in Lu-PSMA-PRLT group versus only 22% of patients in third-line treatment group). The authors mentioned that, despite variations in doses and number of cycles, 177Lu-PSMA-PRLT group showed a favorable response rate as compared to the third-line treatment group, and they also mentioned more side effects and discontinuation of third-line treatment as compared to 177Lu-PSMA- PRLT group.
Click to Show/Hide
|
||||
| Experiment 266 Reporting the Activity Data of This PDC | [22] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median overall survival (mOS) |
14 months
|
|||
| Patients Enrolled |
90 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 1-7 cycles | ||||
| Administration Dosage | 3.7-8 GBq/cycle | ||||
| MOA of PDC |
The PSMA molecule acts as a target for theranostics in detecting and treating prostatic lesions. This ultimately promotes the concept of precision and personalized medicine. Several published articles showed favorable outcomes of Lu-PSMA-PRLT in mCRPC patients, which quickly translated into routine clinical practices with real effectiveness, a low toxicity profile, and documentation of the risk-benefit of PRLT. Nevertheless, many questions related to PRLT remain unresolved such as the sequencing of PRLT with ARTA or taxane-based chemotherapy, re-challenge therapy, combined therapy, alpha therapy in mCRPC patients, and early treatment of PRLT in mHNPC patients. To solve these questions, several clinical trials are currently under way, and the results of these trials will be helpful in deciding treatment strategies for prostate cancer patients.
Click to Show/Hide
|
||||
| Description |
A favorable response rate (PSA and objective response) and safe profile of 177Lu-PSMA-617 were demonstrated in this study, leading to greater use of Lu-PSMA-PRLT in clinical practices. Similarly, Yadav et al. reported favorable outcomes of 177Lu-PSMA-617 in a prospective, single-arm, single-center study in 90 mCRPC patients.
|
||||
| Experiment 267 Reporting the Activity Data of This PDC | [48] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median overall survival (mOS) |
15 months
|
|||
| Patients Enrolled |
Patients with metastatic castration-resistant prostate cancer who underwent 68Ga-PSMA and FDG PET-CT scans.
|
||||
| Evaluation Method | 6AN2237:AN22568Ga-PSMA/18F-FDG PET-CT assay | ||||
| Description |
In the period between 2016 and 2018, 58 patients were referred for [177Lu]-PSMA PRLT to the center, of which 51 patients underwent both [68Ga]-PSMA and FDG PET-CT scans and provisionally qualified for the analysis; out of these complete information of four patients was not available and hence were excluded. Thus, 47 patients were retrospectively recruited and categorized according to the proposed Pro-PET scoring scheme and were analyzed as discussed above. The cohort comprised of heavily pretreated patients with 2 (4.3%) underwent radical prostatectomy; surgical castration was performed in 45 (95.7%) patients; first-line hormonal therapy (with estrogen analogues, leutinizing hormone releasing hormone agonists and antagonists and antiandrogens) in 44 (93.6%) patients, second-line hormonal therapy (with CYP17 blockers and newer anti-androgens) in 34 (72.4%) patients; first-line chemotherapy (with docetaxel) in 33 (70.2%) patients, second-line chemotherapy (with cabazitaxel, oral metronomic chemotherapy, etc.) in 22 (46.8%) and radiotherapy in 26 (55.3%) patients.
Click to Show/Hide
|
||||
| Experiment 268 Reporting the Activity Data of This PDC | [65] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median overall survival (mOS) |
15.3 months
|
|||
| Description |
Pluvicto's efficacy was evaluated in a randomized (2:1), multicenter, open-label trial that compared Pluvicto plus best standard of care with best standard of care alone in men with progressive, PSMA-positive mCRPC. There was statistically significant improvement in overall survival and radiographic progression-free survival for those who received Pluvicto with best standard of care compared with those who received best standard of care alone. Median overall survival was 15.3 months in the intervention arm and 11.3 months in the control arm, although data interpretation may be limited owing to the number of dropouts from the control arm.
Click to Show/Hide
|
||||
| In Vivo Model | Men with progressive , PSMA-positive metastatic castration-resistant prostate cancer. | ||||
| Experiment 269 Reporting the Activity Data of This PDC | [36] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median overall survival (mOS) |
15.3 months
|
|||
| Patients Enrolled |
831 patients with metastatic castration-resistant prostate cancer.
|
||||
| Description |
Primary outcomes measured radiographic progression-free survival (rPFS) and OS between 177Lu PSMA-617 RLT plus SOC versus standard of care (SOC) alone. When compared to SOC alone, 177Lu PSMA-617 plus SOC significantly prolonged rPFS (median, 8.7 vs. 3.4 months; HR for progression or death 0.40; 99.2% CI, 0.29 to 0.57) and median OS (15.3 vs. 11.3 months; HR for death, 0.62; 95% CI, 0.52 to 0.74; p < 0.001).
Click to Show/Hide
|
||||
| Experiment 270 Reporting the Activity Data of This PDC | [41] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median overall survival (mOS) |
15.3 months
|
|||
| Patients Enrolled |
551 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | Every 6 weeks for up to a total of 6 doses | ||||
| Administration Dosage | 7.4 GBq (200 mCi) | ||||
| MOA of PDC |
On March 23, 2022, the FDA approved 177Lu-PSMA-617 for the treatment of adult patients with PSMA-positive mCRPC who have been treated with androgen receptor pathway inhibition and taxane-based chemotherapy. The approval was based on a meaningful advantage in overall survival supported by a delay in tumor progression and higher objective response rate. The decision took into account several important factors unique to this applications context. Metastatic castration-resistant prostate cancer (mCRPC) is a life-threatening condition that lacks curative treatment, creating an unmet need. This product provides a novel mechanism of action as the first radioligand therapeutic agent for mCRPC providing anti-tumor effects in both bone and non-bone sites and may provide an opportunity to be combined with other available therapies with different toxicity profiles across mechanistic classes. Finally, 177Lu-PSMA-617 offers a different safety profile than other available systemic therapies which was determined to be acceptable for the indicated patient population, expanding treatment options that can be individualized to a patients preferences and comorbidities.
Click to Show/Hide
|
||||
| Description |
The co-primary endpoint of OS was statistically significant, with patients randomized to receive 177Lu-PSMA-617 plus BSoC having prolonged OS (median estimate 15.3 months) compared to BSoC alone (median estimate 11.3 months), hazard ratio (HR) 0.62 (95% CI: 0.52, 0.74, p<0.001). The planned interim OS analysis was not necessary as the targeted number of OS events were observed before the targeted number of rPFS events. Therefore, the final OS analysis was evaluated at the time of rPFS analysis.
Click to Show/Hide
|
||||
| Experiment 271 Reporting the Activity Data of This PDC | [14] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median overall survival (mOS) |
15.3 months
|
|||
| Patients Enrolled |
831 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | Every 6 weeks for 4-6 cycles | ||||
| Evaluation Method | PSMA PET assay | ||||
| MOA of PDC |
Radiopharmaceuticals have been used in prostate cancer for decades with known efficacy in palliation of bone metastasis. The FDA approval of the most recent radiopharmaceutical, 177Lu-PSMA-617, shows a clear overall survival benefit compared to the best SOC. Current studies are ongoing to evaluate the effectiveness of 177Lu-PSMA-617 in earlier lines of therapy, such as after only 1 line of therapy with an ARPI as in the PSMAfore study, or in mCSPC in combination with ADT and an ARPI as in the PSMAddition study. Studies are also ongoing with 177Lu-PSMA-617 in combination with other treatments which may produce a synergistic effect. As described, there are many clinical trials ongoing that are modifying the 177Lu-PSMA-617 to possibly achieve improved results. Studies are also ongoing looking at swapping the 177Lu for another radioactive agent, such as 225Ac (an alpha emitter) which may have benefits over the beta-emitting 177Lu. Other studies are looking at J591, a monoclonal antibody to PSMA which has unique differences compared to small-molecule PSMA binders. Overall, PSMA-based radioligand therapy has been shown to be an effective and life-prolonging therapy and should be considered a treatment option for selected men with mCRPC. As described, there are many ongoing studies further evaluating PSMA radioligand therapy in Australia, South Africa, Europe, and the United States, representing a truly global effort to improve prostate cancer care.
Click to Show/Hide
|
||||
| Description |
Investigators found that patients who received 177Lu-PSMA-617 had a statistically significant improvement in overall survival with a median survival of 15.3 months vs. 11.3 months (HR for death 0.62, 95% CI 0.52-0.74, P<.001). Radiographic progression-free survival (rPFS) also improved and favored 177Lu-PSMA-617. Key secondary endpoints including time to the first symptomatic skeletal event or death, complete responses based on RECIST 1.1, confirmed decreases in PSA, time to deterioration in the FACT-P total score, and BPI-SF pain intensity score, all favored 177Lu-PSMA-617.
Click to Show/Hide
|
||||
| Experiment 272 Reporting the Activity Data of This PDC | [33] | ||||
| Indication | ATM-mutated metastatic castration resistant prostate cancer | ||||
| Efficacy Data | Median overall survival (mOS) |
16 months
|
|||
| Patients Enrolled |
121 metastatic castration-resistant prostate cancer patients.
|
||||
| Administration Dosage | Median administered cumulative activity: 20 GBq | ||||
| MOA of PDC |
177Lu-PSMA-617 RLT is an effective form of therapy in mCRPC patients and confirms the findings of the short-term studies. 177Lu-PSMA-617 prolongs the overall survival in mCRPC patients heavily pre-treated with chemotherapy, first and second-line anti-androgens, and androgen inhibitor therapies. The delayed toxicity is low and acceptable by most of these patients. Patients who were treated with various other mCRPC-approved compounds before 177Lu-PSMA-RLT were associated with a significantly shorter OS than that of the patients who received 177Lu-PSMA RLT at the earlier stages of mCRPC. An aggressive treatment approach, either sequential or in combination with second-generation anti-androgens, chemotherapies, or with investigational 225Ac-PSMA-617 alpha therapies, might prolong the survival of mCRPC patients in the future.
Click to Show/Hide
|
||||
| Description |
The median administered cumulative activity was 20 GBq (3.7-37 GBq). The median follow-up duration was 36 months (6-72 months). The estimated median PFS and OS were 12 months (mo) (95% CI: 10.3-13 mo) and 16 mo (95% CI: 13-17 mo), respectively. Any PSA decline and PSA decline >50% was achieved in 73% and 61% of the patients, respectively. Multivariate analysis revealed only failure to achieve >50% PSA decline as a significant factor associated with a poor PFS. Prognostic factors associated with reduced OS included, failure to experience >50% PSA decline, heavily pre-treated patient cohort who received >2 lines of prior treatment options, and patient sub-group treated with ≥2 lines of chemotherapy. Patients re-treated with additional treatment options after attaining 177Lu-PSMA refractory disease showed a remarkably prolonged OS. A significant clinical benefit was achieved post 177Lu-PSMA-617 RLT. The most common toxicities observed were fatigue (34.7%), followed by nausea (33%), and dry mouth (24.7%).
Click to Show/Hide
|
||||
| Experiment 273 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median overall survival (mOS) |
16 months
|
|||
| Patients Enrolled |
56 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 1-4 cycles | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
Another retrospective study evaluated 56 mCPRC patients with a median age of 69.5 (range 55-84) who received one to four cycles of 177Lu-PSMA-617. Biochemical response was defined using Prostate Cancer Working Group Criteria 3 (PCWG3). A total of 139 cycles of treatment were performed with a decline of greater than 50% in 54% of patients and any PSA decline in 65% of patients. Estimated median overall survival was 16 months versus 14 months in the chemotherapy alone group. Longer OS was observed in patients with a PSA decline of >50%, a baseline ALP level <220 U/l, more than two cycles of treatment, and cumulative activity of greater than 15 GBq.
Click to Show/Hide
|
||||
| Experiment 274 Reporting the Activity Data of This PDC | [22] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median overall survival (mOS) |
16 months
|
|||
| Patients Enrolled |
2346 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Dosage | 6 GBq/cycle | ||||
| MOA of PDC |
The PSMA molecule acts as a target for theranostics in detecting and treating prostatic lesions. This ultimately promotes the concept of precision and personalized medicine. Several published articles showed favorable outcomes of Lu-PSMA-PRLT in mCRPC patients, which quickly translated into routine clinical practices with real effectiveness, a low toxicity profile, and documentation of the risk-benefit of PRLT. Nevertheless, many questions related to PRLT remain unresolved such as the sequencing of PRLT with ARTA or taxane-based chemotherapy, re-challenge therapy, combined therapy, alpha therapy in mCRPC patients, and early treatment of PRLT in mHNPC patients. To solve these questions, several clinical trials are currently under way, and the results of these trials will be helpful in deciding treatment strategies for prostate cancer patients.
Click to Show/Hide
|
||||
| Description |
Von Eyben et al. published a review and meta-analysis on 177Lu-PSMA-PRLT with the inclusion of 2346 patients. They found a median OS of 16 months after PRLT and longer survival in asymptomatic patients and those with only lymph node metastatic disease as compared to symptomatic patients and those with extensive disease. They also demonstrated ≥50% PSA decline in 50% of patients with longer survival as compared to those with <50% PSA decline. Hematologic toxicity was observed in approximately 10% of the patients with anemia of grade 3 as the most severe adverse effect of 177Lu-PSMA-PRLT. The authors mentioned that the intensified schedule of 177Lu-PSMA-PRLT (increased dose activity up to 9 GBq per cycle with a shortened time interval between cycles) increases the survival and efficacy of PRLT without increasing hematological toxicity.
Click to Show/Hide
|
||||
| Experiment 275 Reporting the Activity Data of This PDC | [66] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median overall survival (mOS) |
16.3 months
|
|||
| Patients Enrolled |
55 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | At least 2 cycles | ||||
| Administration Dosage | 7,400 MBq/cycles | ||||
| MOA of PDC |
The 177Lu-PSMA-617 kinetics in LNM and BM appear to be prognostic of treatment response, as well as of survival. In particular, OS appears to be linked with the kinetics parameters of BM, in keeping with the concept that BM is the most threatening pathogenic mechanism of mCRPC. This information, which should be confirmed by prospective trials, is readily obtainable from posttherapy scans and could be used to prognosticate treatment outcomes and design studies aimed to investigate the potential of PET-based prediction, as well as the possibility of patient-adapted therapeutic protocols of RLT.
Click to Show/Hide
|
||||
| Description |
Forty-three patients died of disease. OS from the RLT start was 16.3 mo (95% CI, 11.1-21.6). %IDred in BM predicted OS, but neither LNM nor BM %ID was associated with OS.
|
||||
| Experiment 276 Reporting the Activity Data of This PDC | [5] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median overall survival (mOS) |
17.1 months
|
|||
| Patients Enrolled |
45 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 164 cycles of rnt, every 6-8 weeks | ||||
| Description |
Forty-five patients were treated with total of 164 cycles of RNT. Fifteen patients (33%) had PSA decline of ≥50%, 23 patients (51%) showed any PSA decline and 20 patients (44%) showed PSA increase of ≥25%. Median OS and PFS were 17,1 months and 7,4 months. Patients had any or ≥50% PSA response after the first cycle, lower initial ALP (<120U/L) had longer OS and PFS. Patients had normal Hb showed longer OS and patients had lower initial PSA (<51ng/mL) had longer PFS. Patients had PSA progression of ≥25% had shorter OS and PFS.
Click to Show/Hide
|
||||
| Experiment 277 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median overall survival (mOS) |
17.2 months
|
|||
| Patients Enrolled |
62 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | A median of 3 cycles (2-5) | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
A single center retrospective analysis studied 62 men with mCRPC who were treated with 177Lu-PSMA-617. A median of 3 treatment cycles (2-5) were administered over 4 weeks. Progression-free survival and overall survival were 4.9 months (2.4-9.6) and 17.2 months (6-26.4) respectively. Greater than 50% PSA response was found in 58.7% of patients (p < 0.004).
Click to Show/Hide
|
||||
| Experiment 278 Reporting the Activity Data of This PDC | [67] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median overall survival (mOS) |
17.7 months
|
|||
| Patients Enrolled |
52 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | Every 6-10 weeks for 6 cycles | ||||
| Administration Dosage | 7.3 GBq (5.9-7.4 GBq) | ||||
| Evaluation Method | 18F-Fluorodeoxyglucose (FDG) and 68Ga-PSMA (PSMA) Positron Emission Tomography/Computer Tomography (PET/CT) scans assay | ||||
| MOA of PDC |
PSA response patterns, PSA decline rate after the first RLT and pretherapy PSA doubling time are the most important predictors of OS in patients receiving Lu-177 PSMA RLT. FDG PET/CT can be utilized as additional decision-making for PSMA-RLT eligibility since high tumor heterogeneity and the presence of FDG > PSMA disease is associated with poor OS.
Click to Show/Hide
|
||||
| Description |
Median OS and PSA-PFS were 17.7 (95% confidence interval [CI]: 15.2-20.2) and 6.6 months (95% CI: 4.5-8.8), respectively. Primary resistance to PSMA-RLT (hazard ratio [HR]: 12.57, 95% CI: 2.4-65.2, p: 0.003), <30% PSA response rate after first cycle of PSMA-RLT (HR: 1.016, 95% CI: 1.006-1.03, p: 0.003), FDG > PSMA disease (HR: 4.9, 95% CI: 1.19-20.62, p: 0.03), PSA doubling time (PSA DT) of ≤2.4 months (HR: 15.7, 95% CI: 3.7-66.4, p: <0.0001), and low hemoglobin levels (HR: 0.59, 95% CI: 0.41-0.83, p: 0.003) were correlated with poor OS in the multivariate analysis. Bone scintigraphy > PSMA disease (HR: 5.6; 95% CI: 1.8-17, p: 0.002) and high C-reactive protein (HR: 1.4, 95% CI: 1.1-1.7, p: 0.001) were significant predictive biomarkers for PFS in the multivariate analysis.
Click to Show/Hide
|
||||
| Experiment 279 Reporting the Activity Data of This PDC | [35] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median overall survival (mOS) |
18 months
|
|||
| Administration Time | Median of 4 (iqr: 2-7) cycles | ||||
| Administration Dosage | Mean cumulative activity of 30.7 ± 23.4 GBq | ||||
| MOA of PDC |
RLT with 177Lu-PSMA-617 can be effectively and safely initiated as early as 8 weeks after failure of 223Ra in patients with progressive bone-metastatic mCRPC refractory to 223Ra. Objective response can be achieved even in patients with more advanced disease and disseminated/diffuse bone metastases, albeit with increasing incidence of significant hematotoxicity.
Click to Show/Hide
|
||||
| Description |
Median imaging-based progression-free survival (PFS) was 10 (95% CI, 6-14) months and median overall survival (OS) was 18 (95% CI, 14-22) months.
|
||||
| In Vivo Model | 28 men with progressive metastatic castration-resistant prostate cancer who median age 73 years, range 63-89 years). | ||||
| Experiment 280 Reporting the Activity Data of This PDC | [14] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median overall survival (mOS) |
19.1 months
|
|||
| Patients Enrolled |
200 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | Every 6 weeks (up to 6 cycles) | ||||
| Evaluation Method | 68Ga-PSMA PET assay | ||||
| MOA of PDC |
Radiopharmaceuticals have been used in prostate cancer for decades with known efficacy in palliation of bone metastasis. The FDA approval of the most recent radiopharmaceutical, 177Lu-PSMA-617, shows a clear overall survival benefit compared to the best SOC. Current studies are ongoing to evaluate the effectiveness of 177Lu-PSMA-617 in earlier lines of therapy, such as after only 1 line of therapy with an ARPI as in the PSMAfore study, or in mCSPC in combination with ADT and an ARPI as in the PSMAddition study. Studies are also ongoing with 177Lu-PSMA-617 in combination with other treatments which may produce a synergistic effect. As described, there are many clinical trials ongoing that are modifying the 177Lu-PSMA-617 to possibly achieve improved results. Studies are also ongoing looking at swapping the 177Lu for another radioactive agent, such as 225Ac (an alpha emitter) which may have benefits over the beta-emitting 177Lu. Other studies are looking at J591, a monoclonal antibody to PSMA which has unique differences compared to small-molecule PSMA binders. Overall, PSMA-based radioligand therapy has been shown to be an effective and life-prolonging therapy and should be considered a treatment option for selected men with mCRPC. As described, there are many ongoing studies further evaluating PSMA radioligand therapy in Australia, South Africa, Europe, and the United States, representing a truly global effort to improve prostate cancer care.
Click to Show/Hide
|
||||
| Description |
Of the patients with PET screening in TheraP, approximately 27% were excluded from treatment. Investigators found that patients who received 177Lu-PSMA-617 were more likely to receive a PSA response (66% vs. 37% in the intent-to-treat group, P<.0001). Updated survival analysis was presented at a 2022 meeting, and overall survival was similar between 177Lu-PSMA-617 and cabazitaxel at 19.1 months versus 19.6 months was not significantly different between the 2 arms. The finding of survival equivalence in a PSMA-selected patient population was surprising to some but it is well known that cabazitaxel is an important life-prolonging therapy in mCRPC.
Click to Show/Hide
|
||||
| Experiment 281 Reporting the Activity Data of This PDC | [21] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median overall survival (mOS) |
27.1 months
|
|||
| Patients Enrolled |
Patients with metastatic castration-resistant prostate cancer; naive (T-naive).
|
||||
| Experiment 282 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median overall survival (mOS) |
29.4 weeks
|
|||
| Patients Enrolled |
28 patients with metastatic castration-resistant prostate cancer.
|
||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
A retrospective analysis studied 28 patients with mCRPC who were treated with 177Lu-PSMA-617 [Citation47]. The estimated median survival was 29.4 weeks, significantly longer than survival in the supportive care group (HR, 0.44; 95% confidence interval, 0.20-0.95]; P = 0.031). Results of the study noted any PSA decline in 59% of patients after one cycle and 75% of patients after two cycles of treatment, while there was a noted PSA decline of 50% or greater in 32% of patients after one cycle of treatment and in 50% of patients after two cycles of treatment. Although this study found a 50% or greater PSA decline in majority of treated patients, 83% of patients reported a stable or improved quality of life after treatment.
Click to Show/Hide
|
||||
| Experiment 283 Reporting the Activity Data of This PDC | [28] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median overall survival (mOS) |
32 weeks
|
|||
| Patients Enrolled |
Patients with metastatic castration-resistant prostate cance, who had been treated with at least one next-generation antihormonal drug as well as chemotherapy.
|
||||
| Administration Time | 159 cycle | ||||
| Administration Dosage | Median dose 6.11 GBq | ||||
| Description |
A decline in prostate-specific antigen (PSA) of ≥50% occurred in 53%, and a decline in PSA of any amount in 91% of patients. The estimated median OS was 32 weeks.
|
||||
| Experiment 284 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median overall survival (mOS) |
32 weeks
|
|||
| Patients Enrolled |
59 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | A median of 3 cycles | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
Another study retrospectively studied fifty-nine mCRPC patients after receiving at least one antihormonal drug as well as chemotherapy. These patients were treated with a median of three cycles of 177Lu-PSMA-61. The primary end point was overall survival, and secondary end point was decrease in PSA level. Follow-up data was available for forty-five patients with 91% showing a PSA decline. A decline in PSA levels of greater than or equal to 50% occurred in 53% of the patients. The median overall survival was 32 weeks. An initial alkaline phosphatase (ALP) level less than 220 U/L and a PSA decline after the first cycle were associated with a longer overall survival (56 vs. 28 weeks, p < 0.01, and 56 vs. 29 weeks, p = 0.04, respectively). Toxicity overview showed grade 3 leukopenia and thrombocytopenia in 3% patients and grade 3 anemia in 19%. No grade 3 or 4 nephrotoxicity or grade 4 blood toxicity was observed. This study showed a statistically significant decline in ALP levels after the first cycle of 177Lu-PSMA-617.
Click to Show/Hide
|
||||
| Experiment 285 Reporting the Activity Data of This PDC | [52] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median overall survival (mOS) |
45 months
|
|||
| Patients Enrolled |
19 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 5 (iqr: 3-6) cycles | ||||
| Administration Dosage | A cumulative activity of 32 ± 11 GBq | ||||
| Evaluation Method | 68Ga-PSMA-11 PET/CT assay | ||||
| MOA of PDC |
Intermittent 177Lu-PSMA-617 radioligand therapy in early responders with oligometastatic castration-resistant prostate cancer seems to not compromise survival outcome, despite long treatment-free intervals. The safety profile remained favorable, warranting further investigation of the concept of intermittent treatment in selected patients with a longer life-expectancy.
Click to Show/Hide
|
||||
| Description |
Four (21%) patients showed no response (PD) to the 177Lu-PSMA-RLT cycles after the first treatment break, and in two patients (11%), progression after the initial disease stabilization (SD) under subsequent cycles led to treatment discontinuation. Two patients (11%) completed the intended six cycles with a stable disease. In the remaining 11/19 (84%) patients, resuming 177Lu-PSMA-RLT resulted in a repeated PR. Altogether, 14/19 (74%) patients died by the time of this analysis. The median PFS was 27 (95% CI: 23-31) months and the OS was 45 (95% CI: 28-62) months.
Click to Show/Hide
|
||||
| Experiment 286 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median overall survival (mOS) |
52 weeks
|
|||
| Patients Enrolled |
43 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | Every six to twelve weeks | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
A single center retrospective study reviewed 43 mCRPC patients with a median age of 71 (range 51-88) and 177Lu-PSMA-617 treatments every six to twelve weeks. A total of 112 cycles of RLT were conducted with a median of three cycles (range 1-6). Endpoints included PSA response, toxicity, median OS, and median PSA PFS. A PSA decline of greater than 90% was seen in 23% of patients, while a decline of greater than 50% was seen in 65% of patients. A median OS was 52 weeks, while a PSA PFS was found to be 20 weeks.
Click to Show/Hide
|
||||
| Experiment 287 Reporting the Activity Data of This PDC | [15] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median overall survival (mOS) |
56.0 weeks
|
|||
| Patients Enrolled |
Patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 351 cycles | ||||
| Description |
The median OS was 56.0 weeks (95%CI: 50.5-61.5).
|
||||
| Experiment 288 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median overall survival (mOS) |
56.0 weeks
|
|||
| Patients Enrolled |
104 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | A median of 3 cycles (1-8 cycles) | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
A total of 104 patients with mCRPC who were previously treated with one line of chemotherapy (docetaxel and/or cabazitaxel) and at least one of antihormonal therapies (enzalutamide and/or abiraterone) were retrospectively studied after being treated with 177Lu-PSMA-617 RLT. A median of three cycles were administered (1-8 cycles). Results of the study noted a median overall survival of 56.0 weeks (95% CI: 50.5-61.5) and PSA decline >50% in 33% patients after receiving first cycle of treatment.
Click to Show/Hide
|
||||
| Experiment 289 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median overall survival (mOS) |
60 weeks
|
|||
| Patients Enrolled |
52 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 1-3 cycles every eight weeks | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
An additional retrospective study of 52 mCRPC patients (mean age of 70, range 48-87 years) evaluated the PSA response of those treated with 177Lu-PSMA-617 after one to three cycles of radioligand therapy (RLT) every eight weeks. A total of 190 cycles of RLT (3-6 cycles per patient) were given and 80% of patients showed a decline after the first cycle with 44% of patients showing a PSA response of more than 50%. After the third cycle, 73% of patients showed any PSA decline. The median OS was 60 weeks for all patients and median OS was statistically longer for those who responded with decline in PSA after first cycle compared to those without (68 vs 33 weeks).
Click to Show/Hide
|
||||
| Experiment 290 Reporting the Activity Data of This PDC | [53] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median percentage decrease in PSA |
-94.20%
|
|||
| Administration Time | 6 cycles | ||||
| Administration Dosage | 7081 MBq (IQR 6995-7188) | ||||
| Evaluation Method | 18F/68Ga-PSMA PET/CT assay | ||||
| MOA of PDC |
177Lu-PSMA-RLT in a four-week interval with a fixed dose was safe and effective. A significant PSA response was observed in six out of ten patients, which was also associated with better OS and PFS. A shorter treatment interval may broaden the therapeutic window among mCRPC patients with high volume disease and rapidly rising PSA. Pre-treatment staging PSMA was not helpful in distinguishing responders from non-responders. However, parameters for tumor burden and its activity provide prognostic information related to OS and PFS.
Click to Show/Hide
|
||||
| Description |
The median percentage decrease in PSA (all patients) was -19.8% (IQR -37.1-4.3) after the first treatment, -42.9% (IQR -69.8-16.5) after the second treatment and -70.4% (IQR -88.6--35.1) after the third treatment. A trend towards a greater PSA decrease with a greater number of treatment cycles was also observed in patients who received more than three treatment cycles. For example, the median decrease in PSA was -94.2% (IQRT -91.0--35.6) for patients who received six treatment cycles (n = 10). Altogether, there were six patients (10%) with an exceptional (more than 98%) PSA treatment response. The best response was a 99.9% PSA decrease, which represented a change from 121 to 0.1 ng/L. All of the patients with an excellent treatment response had detectable PSA levels after PSMA-RLT. In general, the PSA response was not associated with Gleason score, pre-treatment PSA kinetics, MTV, TLA, SUVmax values or lesion diameters.
Click to Show/Hide
|
||||
| In Vivo Model | This is a single-center retrospective analysis in 62 men with pathologically confirmed castration resistant metastatic prostate cancer who were treated with 177Lu-PSMA-617 during January 2017-February 2019. | ||||
| Experiment 291 Reporting the Activity Data of This PDC | [53] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median percentage decrease in PSA |
-70.40%
|
|||
| Administration Time | 3 cycles | ||||
| Administration Dosage | 7081 MBq (IQR 6995-7188) | ||||
| Evaluation Method | 18F/68Ga-PSMA PET/CT assay | ||||
| MOA of PDC |
177Lu-PSMA-RLT in a four-week interval with a fixed dose was safe and effective. A significant PSA response was observed in six out of ten patients, which was also associated with better OS and PFS. A shorter treatment interval may broaden the therapeutic window among mCRPC patients with high volume disease and rapidly rising PSA. Pre-treatment staging PSMA was not helpful in distinguishing responders from non-responders. However, parameters for tumor burden and its activity provide prognostic information related to OS and PFS.
Click to Show/Hide
|
||||
| Description |
The median percentage decrease in PSA (all patients) was -19.8% (IQR -37.1-4.3) after the first treatment, -42.9% (IQR -69.8-16.5) after the second treatment and -70.4% (IQR -88.6--35.1) after the third treatment. A trend towards a greater PSA decrease with a greater number of treatment cycles was also observed in patients who received more than three treatment cycles. For example, the median decrease in PSA was -94.2% (IQRT -91.0--35.6) for patients who received six treatment cycles (n = 10). Altogether, there were six patients (10%) with an exceptional (more than 98%) PSA treatment response. The best response was a 99.9% PSA decrease, which represented a change from 121 to 0.1 ng/L. All of the patients with an excellent treatment response had detectable PSA levels after PSMA-RLT. In general, the PSA response was not associated with Gleason score, pre-treatment PSA kinetics, MTV, TLA, SUVmax values or lesion diameters.
Click to Show/Hide
|
||||
| In Vivo Model | This is a single-center retrospective analysis in 62 men with pathologically confirmed castration resistant metastatic prostate cancer who were treated with 177Lu-PSMA-617 during January 2017-February 2019. | ||||
| Experiment 292 Reporting the Activity Data of This PDC | [53] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median percentage decrease in PSA |
-42.90%
|
|||
| Administration Time | 2 cycles | ||||
| Administration Dosage | 7081 MBq (IQR 6995-7188) | ||||
| Evaluation Method | 18F/68Ga-PSMA PET/CT assay | ||||
| MOA of PDC |
177Lu-PSMA-RLT in a four-week interval with a fixed dose was safe and effective. A significant PSA response was observed in six out of ten patients, which was also associated with better OS and PFS. A shorter treatment interval may broaden the therapeutic window among mCRPC patients with high volume disease and rapidly rising PSA. Pre-treatment staging PSMA was not helpful in distinguishing responders from non-responders. However, parameters for tumor burden and its activity provide prognostic information related to OS and PFS.
Click to Show/Hide
|
||||
| Description |
The median percentage decrease in PSA (all patients) was -19.8% (IQR -37.1-4.3) after the first treatment, -42.9% (IQR -69.8-16.5) after the second treatment and -70.4% (IQR -88.6--35.1) after the third treatment. A trend towards a greater PSA decrease with a greater number of treatment cycles was also observed in patients who received more than three treatment cycles. For example, the median decrease in PSA was -94.2% (IQRT -91.0--35.6) for patients who received six treatment cycles (n = 10). Altogether, there were six patients (10%) with an exceptional (more than 98%) PSA treatment response. The best response was a 99.9% PSA decrease, which represented a change from 121 to 0.1 ng/L. All of the patients with an excellent treatment response had detectable PSA levels after PSMA-RLT. In general, the PSA response was not associated with Gleason score, pre-treatment PSA kinetics, MTV, TLA, SUVmax values or lesion diameters.
Click to Show/Hide
|
||||
| In Vivo Model | This is a single-center retrospective analysis in 62 men with pathologically confirmed castration resistant metastatic prostate cancer who were treated with 177Lu-PSMA-617 during January 2017-February 2019. | ||||
| Experiment 293 Reporting the Activity Data of This PDC | [53] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median percentage decrease in PSA |
-19.80%
|
|||
| Administration Time | 1 cycles | ||||
| Administration Dosage | 7081 MBq (IQR 6995-7188) | ||||
| Evaluation Method | 18F/68Ga-PSMA PET/CT assay | ||||
| MOA of PDC |
177Lu-PSMA-RLT in a four-week interval with a fixed dose was safe and effective. A significant PSA response was observed in six out of ten patients, which was also associated with better OS and PFS. A shorter treatment interval may broaden the therapeutic window among mCRPC patients with high volume disease and rapidly rising PSA. Pre-treatment staging PSMA was not helpful in distinguishing responders from non-responders. However, parameters for tumor burden and its activity provide prognostic information related to OS and PFS.
Click to Show/Hide
|
||||
| Description |
The median percentage decrease in PSA (all patients) was -19.8% (IQR -37.1-4.3) after the first treatment, -42.9% (IQR -69.8-16.5) after the second treatment and -70.4% (IQR -88.6--35.1) after the third treatment. A trend towards a greater PSA decrease with a greater number of treatment cycles was also observed in patients who received more than three treatment cycles. For example, the median decrease in PSA was -94.2% (IQRT -91.0--35.6) for patients who received six treatment cycles (n = 10). Altogether, there were six patients (10%) with an exceptional (more than 98%) PSA treatment response. The best response was a 99.9% PSA decrease, which represented a change from 121 to 0.1 ng/L. All of the patients with an excellent treatment response had detectable PSA levels after PSMA-RLT. In general, the PSA response was not associated with Gleason score, pre-treatment PSA kinetics, MTV, TLA, SUVmax values or lesion diameters.
Click to Show/Hide
|
||||
| In Vivo Model | This is a single-center retrospective analysis in 62 men with pathologically confirmed castration resistant metastatic prostate cancer who were treated with 177Lu-PSMA-617 during January 2017-February 2019. | ||||
| Experiment 294 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median progression-free survival (mPFS) |
5.5 months
|
|||
| Patients Enrolled |
254 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 3 median number cycles, delivered at a median interval of 5.7 weeks | ||||
| Administration Dosage | 6.5 GBq/cycle (median cumulative dose 21.2 GBq) | ||||
| MOA of PDC |
Lutetium Lu 177 vipivotide tetraxetan is a PSMA-binding ligand bound to a DOTA chelator (i.e., tetraxetan) radiolabeled with lutetium-177. Once lutetium Lu 177 vipivotide tetraxetan is bound to PSMA-expressing cells, the beta-minus emission from lutetium-177 delivers radiation to PSMA-expressing and surrounding cells, inducing DNA damage that leads to cell death. The exposure-efficacy relationships of lutetium Lu 177 vipivotide tetraxetan and the time course of the pharmacodynamic response are not fully characterized [9]. Lutetium-177 decays to a stable hafnium-177 with a physical half-life of 6.647 days by emitting beta-minus radiation with a maximum energy of 0.498 MeV (79%) and photonic radiation (γ) of 0.208 MeV (11%) and 0.113 MeV (6.4%).
Click to Show/Hide
|
||||
| Description |
A ≥ 50% reduction in PSA was seen in 52.0% of patients (132/254); at a median follow-up of 14.5 months, median PSA PFS was 5.5 months and median OS was 14.5 months. The median dose of lutetium Lu 177 vipivotide tetraxetan was 6.5 GBq/cycle (median cumulative dose 21.2 GBq), the median number cycles was 3, delivered at a median interval of 5.7 weeks.
Click to Show/Hide
|
||||
| Half life period | 41.6 h | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT04833517 | Clinical Status | Phase 2 | ||
| Clinical Description | This prospective registry aims to assess outcome and toxicity of targeted radionuclide therapies in patients with advanced prostate cancer in clinical routine. While the major investigated treatment modality is prostate-specific membrane antigen (PSMA)-targeted radioligand therapy, also other radionuclide therapies such as Ra223 and liver-directed radioembolization are included. The investigators believe that prospectively assessed long-term outcome data on implementation of radionuclide therapy, especially in the palliative setting of advanced mCRPC, help to better define the real benefits and risks of the respective treatment modalities for patients regarding survival and quality-of-life. | ||||
| Experiment 295 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median progression-free survival (mPFS) |
5.6 months
|
|||
| Patients Enrolled |
27 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 7.4-22 gbq on days 1 and 15 in the p hase 1 dose-escalation co hort (n = 29); 22gbq on days 1 and 15 in the p hase 2 co hort (n = 21) | ||||
| Administration Dosage | 22 GBq | ||||
| MOA of PDC |
Lutetium Lu 177 vipivotide tetraxetan is a PSMA-binding ligand bound to a DOTA chelator (i.e., tetraxetan) radiolabeled with lutetium-177. Once lutetium Lu 177 vipivotide tetraxetan is bound to PSMA-expressing cells, the beta-minus emission from lutetium-177 delivers radiation to PSMA-expressing and surrounding cells, inducing DNA damage that leads to cell death. The exposure-efficacy relationships of lutetium Lu 177 vipivotide tetraxetan and the time course of the pharmacodynamic response are not fully characterized [9]. Lutetium-177 decays to a stable hafnium-177 with a physical half-life of 6.647 days by emitting beta-minus radiation with a maximum energy of 0.498 MeV (79%) and photonic radiation (γ) of 0.208 MeV (11%) and 0.113 MeV (6.4%).
Click to Show/Hide
|
||||
| Description |
A phase 1/2 study (NCT03042468) found that a single cycle of fractionated-dose of lutetium Lu 177 vipivotide tetraxetan [7.4-22 GBq on days 1 and 15 in the phase 1 dose-escalation cohort (n = 29); 22GBq on days 1 and 15 in the phase 2 cohort (n = 21); 27 patients treated at 22 GBq] was effective in patients with progressive mCRPC. A >50% PSA reduction was seen in 27 of 50 patients (54%); median PSA PFS was 5.6 months and median OS was 15.2 months.
Click to Show/Hide
|
||||
| Half life period | 41.6 h | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT03042468 | Clinical Status | Phase 1/2 | ||
| Clinical Description | The purpose of this study is to find the highest dose level of the study drug, 177Lu-PSMA-617 that can be given without severe side effects for advanced prostate cancer. | ||||
| Experiment 296 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median progression-free survival (mPFS) |
7.5 months
|
|||
| Patients Enrolled |
56 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | On day 1 of each 6-week cycle | ||||
| Administration Dosage | 7.5 GBq | ||||
| MOA of PDC |
Lutetium Lu 177 vipivotide tetraxetan is a PSMA-binding ligand bound to a DOTA chelator (i.e., tetraxetan) radiolabeled with lutetium-177. Once lutetium Lu 177 vipivotide tetraxetan is bound to PSMA-expressing cells, the beta-minus emission from lutetium-177 delivers radiation to PSMA-expressing and surrounding cells, inducing DNA damage that leads to cell death. The exposure-efficacy relationships of lutetium Lu 177 vipivotide tetraxetan and the time course of the pharmacodynamic response are not fully characterized [9]. Lutetium-177 decays to a stable hafnium-177 with a physical half-life of 6.647 days by emitting beta-minus radiation with a maximum energy of 0.498 MeV (79%) and photonic radiation (γ) of 0.208 MeV (11%) and 0.113 MeV (6.4%).
Click to Show/Hide
|
||||
| Description |
A > 50% reduction in PSA after administration of up to 6 cycles of lutetium Lu 177 vipivotide tetraxetan plus idronoxil (a synthetic flavonoid derivative with radiosensitising properties) was seen in 34 of 56 (61%) patients with progressive mCRPC previously treated with AR pathway inhibition and taxanes in the phase 1/2 LuPin trial (ACTRN12618001073291). The median PSA PFS was 7.5 months and median OS was 19.7 months. Patients received lutetium Lu 177 vipivotide tetraxetan 7.5 GBq on day 1 of each 6-week cycle, with escalating doses of NOX66 on days 1-10 of a 6-week cycle.
Click to Show/Hide
|
||||
| Half life period | 41.6 h | ||||
| Related Clinical Trial | |||||
| NCT Number | ACTRN12618001073291 | Clinical Status | Phase 1/2 | ||
| Clinical Description | Background: Trials of lutetium prostate specific membrane antigen (PSMA) in men with metastatic castration-resistant prostate cancer (mCRPC) have demonstrated good safety and efficacy, but combination strategies may improve outcomes. Idronoxil is a synthetic flavonoid derivative with radiosensitising properties. 2. Objective: To evaluate the safety and activity of 177Lu PSMA 617 (LuPSMA-617) in combination with idronoxil suppositories (NOX66) in patients with end-stage mCRPC. 3. Design, setting, and participants: Thirty-two men with progressive mCRPC previously treated with taxane-based chemotherapy (91% treated with both docetaxel and cabazitaxel) and abiraterone and/or enzalutamide were enrolled in this phase I dose escalation study with phase II dose expansion. 4. Intervention: Screening with 68Ga PSMA and 18F-fludeoxyglucose positron emission tomography (PET)/computed tomography (CT) was performed. Men received up to six cycles of LuPSMA-617 (7.5 GBq) on day 1, with escalating doses of NOX66 on days 110 of a 6-wk cycle. Cohort 1 (n = 8) received 400 mg and cohort 2 (n = 24) 800 mg of NOX66. 5. Outcome measurements and statistical analysis: Adverse events (AEs), pain inventory scores, prostate-specific antigen (PSA) response, progression-free survival, and overall survival were evaluated. | ||||
| Experiment 297 Reporting the Activity Data of This PDC | [59] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median progression-free survival (mPFS) |
8.7 months
|
|||
| Patients Enrolled |
551 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 6 cycles | ||||
| Evaluation Method | PSMA PET assay | ||||
| MOA of PDC |
177Lu-PSMA-617 represents not just a new therapy but a new therapeutic class for the treatment of prostate cancer. As such, clinical pathways need to be developed and clinicians involved in the treatment of mCRPC must become familiar with these new processes in order to realize the benefits of RLT for their patients. While not all the suggestions included in this discussion are strictly evidence-based, it is the hope of the authors that this review of the evidence and associated expert opinions help practitioners translate these data into the current Canadian practice setting. Finally, as the therapeutic landscape for mCRPC continues to evolve, new treatments and emerging data will need to be considered when making treatment decisions.
Click to Show/Hide
|
||||
| Description |
In the VISION trial, which enrolled patients with mCRPC who had received at least one line of ARPI treatment and one line of chemotherapy, 177Lu-PSMA-617 improved imaging-based progression-free survival (PFS) by 60% (hazard ratio [HR] = 0.40; 95% confidence interval [CI] 0.29-0.57; p < 0.001) and OS by 38% (HR = 0.62; 95% CI 0.52-0.74; p < 0.001) vs. trial-permitted best standard of care (SOC). The median imaging-based PFS was 8.7 months and median OS was 15.3 months for the 177Lu-PSMA-617 arm, vs. 3.4 months and 11.3 months, respectively, for the SOC arm.
Click to Show/Hide
|
||||
| Experiment 298 Reporting the Activity Data of This PDC | [59] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median progression-free survival (mPFS) |
12 months
|
|||
| Patients Enrolled |
234 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 6 cycles | ||||
| Evaluation Method | PSMA PET assay | ||||
| MOA of PDC |
177Lu-PSMA-617 represents not just a new therapy but a new therapeutic class for the treatment of prostate cancer. As such, clinical pathways need to be developed and clinicians involved in the treatment of mCRPC must become familiar with these new processes in order to realize the benefits of RLT for their patients. While not all the suggestions included in this discussion are strictly evidence-based, it is the hope of the authors that this review of the evidence and associated expert opinions help practitioners translate these data into the current Canadian practice setting. Finally, as the therapeutic landscape for mCRPC continues to evolve, new treatments and emerging data will need to be considered when making treatment decisions.
Click to Show/Hide
|
||||
| Description |
In PSMAfore, which enrolled patients who were chemotherapy-nave, at the time of the second interim analysis median imaging-based PFS was 6.4 months longer in the 177Lu-PSMA-617 arm vs. the ARPI change arm (HR = 0.43; 95% CI 0.33-0.54; p < 0.0001), while there was no significant difference in median OS, which was 19.25 vs. 19.71 months in the 177Lu-PSMA-617 and ARPI change arms, respectively (HR = 1.18; 95% CI 0.83-1.64). It is important to note that a high crossover rate occurred, with 84.2% of patients who progressed in the ARPI change arm subsequently receiving 177Lu-PSMA-617, thus likely diminishing the between-arm differences.
Click to Show/Hide
|
||||
| Experiment 299 Reporting the Activity Data of This PDC | [53] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median progression-free survival (mPFS) |
0.4 year
|
|||
| Administration Time | 1-7 cycles | ||||
| Administration Dosage | 7081 MBq (IQR 6995-7188) | ||||
| Evaluation Method | 18F/68Ga-PSMA PET/CT assay | ||||
| MOA of PDC |
177Lu-PSMA-RLT in a four-week interval with a fixed dose was safe and effective. A significant PSA response was observed in six out of ten patients, which was also associated with better OS and PFS. A shorter treatment interval may broaden the therapeutic window among mCRPC patients with high volume disease and rapidly rising PSA. Pre-treatment staging PSMA was not helpful in distinguishing responders from non-responders. However, parameters for tumor burden and its activity provide prognostic information related to OS and PFS.
Click to Show/Hide
|
||||
| Description |
The median follow-up time was 1.7 years (y; IQR 0.7-2.2). The median PSA progression-free survival was 0.4 y (IQR 0.2-0.8) and the OS was 1.6 y (IQR 0.7-2.2). During follow-up, 36 (58%) patients died. The survival probability was significantly better among patients with significant (>50%) PSA response compared to non-responders, p < 0.04.
|
||||
| In Vivo Model | This is a single-center retrospective analysis in 62 men with pathologically confirmed castration resistant metastatic prostate cancer who were treated with 177Lu-PSMA-617 during January 2017-February 2019. | ||||
| Experiment 300 Reporting the Activity Data of This PDC | [22] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median progression-free survival (mPFS) |
2.8 months
|
|||
| Patients Enrolled |
30 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 3 cycles | ||||
| Administration Dosage | 3.8-6.7 GBq/cycle | ||||
| MOA of PDC |
The PSMA molecule acts as a target for theranostics in detecting and treating prostatic lesions. This ultimately promotes the concept of precision and personalized medicine. Several published articles showed favorable outcomes of Lu-PSMA-PRLT in mCRPC patients, which quickly translated into routine clinical practices with real effectiveness, a low toxicity profile, and documentation of the risk-benefit of PRLT. Nevertheless, many questions related to PRLT remain unresolved such as the sequencing of PRLT with ARTA or taxane-based chemotherapy, re-challenge therapy, combined therapy, alpha therapy in mCRPC patients, and early treatment of PRLT in mHNPC patients. To solve these questions, several clinical trials are currently under way, and the results of these trials will be helpful in deciding treatment strategies for prostate cancer patients.
Click to Show/Hide
|
||||
| Description |
Yordanova et al., evaluated the response rate and clinical toxicity of re-challenge 177Lu-PSMA-617 in progressive prostatic cancer patients who previously benefited from this therapy. In this retrospective study, a total of 30 patients were re-treated with a median of 3 (range 1-6) cycles of 177Lu-PSMA-617. They found that 75-90% of patients demonstrated favorable serum PSA responses following re-challenge cycles, with a median OS of 12 months after the first re-challenge cycle and without any life-threatening grade-4 adverse event. The authors concluded that the majority of patients benefited from re-challenging 177Lu-PSMA-617 with a longer OS in biochemically responsive patients. At present, data on re-challenge 177Lu-PSMA-617 is limited and requires a prospective randomized trial before a definitive conclusion.
Click to Show/Hide
|
||||
| Experiment 301 Reporting the Activity Data of This PDC | [20] | ||||
| Indication | Advanced prostate cancer | ||||
| Efficacy Data | Median progression-free survival (mPFS) |
3.2 months
|
|||
| Patients Enrolled |
Patients with advanced prostate cancer.
|
||||
| Administration Time | 2 cycles | ||||
| Description |
The median PSA-PFS and overall survival were 3.2 mo (95% confidence interval, 2.6-3.7 mo) and 14.0 mo (95% confidence interval, 6.2-21.8 mo), respectively.
|
||||
| Experiment 302 Reporting the Activity Data of This PDC | [19] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median progression-free survival (mPFS) |
3.8 months
|
|||
| Patients Enrolled |
25 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | A median of four (iqr: 2-6) cycles every 6-8 weeks | ||||
| Administration Dosage | Mean of 7.7 ± 1.4 GBq/cycle | ||||
| MOA of PDC |
The response to radioligand therapy with 177Lu-PSMA-617 seems to be independent of the presence of early-onset prostate cancer (EOPC); however, the less favorable survival outcome observed in our study may indicate a more aggressive disease course. Expectedly, the safety of LuPSMA-RLT does not seem to be compromised in metastasized castration-resistant EOPC patients. Comparative studies on age at diagnosis of prostate cancer and the patients outcome after LuPSMA-RLT are needed.
Click to Show/Hide
|
||||
| Description |
The median progression-free survival (PFS) was 3.8 months (95% CI 2.3-5.3), and overall survival (OS) was 8.5 months (95% CI 6.2-10.8).
|
||||
| Experiment 303 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median progression-free survival (mPFS) |
3.8 months
|
|||
| Patients Enrolled |
25 patients with prostate cancer.
|
||||
| Administration Time | A median of four cycles | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
Another retrospective study studied 25 patients less than 55 years of age at prostate cancer diagnosis who were treated with a median of four cycles (range 2-6) of 177Lu-PSMA-617. The median PFS was 3.8 months (95% CI 2.5-5.3) and OS was 8.5 months (95% 6.2-10.8). An initial PSA reduction of greater than 50% was seen in 36% of patients but not associated with OS benefit (p = 0.601). A PSA response greater than 50% at three months was seen in 48% of patients and associated with improvement in OS (16 months, 95% CI 7.4-24.6 versus 4.0 months, 95% CI: 1.1-6.9, p = 0.002). They also used 68Ga-PSMA-PET/CT and correlated imaging response after up to three cycles in 44% of patients. Responders had a longer median PFS (8.7 months, 95% CI 1.3-16.1 vs. 1.9 months, 95% CI 1.7-2.2, p < 0.001) and OS (16.0 months, 95% CI 7.6-24.4 vs. 4.0 months, 95% CI 0.9-7.1; p = 0.002).
Click to Show/Hide
|
||||
| Experiment 304 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median progression-free survival (mPFS) |
4.9 months
|
|||
| Patients Enrolled |
62 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | A median of 3 cycles (2-5) | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
A single center retrospective analysis studied 62 men with mCRPC who were treated with 177Lu-PSMA-617. A median of 3 treatment cycles (2-5) were administered over 4 weeks. Progression-free survival and overall survival were 4.9 months (2.4-9.6) and 17.2 months (6-26.4) respectively. Greater than 50% PSA response was found in 58.7% of patients (p < 0.004).
Click to Show/Hide
|
||||
| Experiment 305 Reporting the Activity Data of This PDC | [42] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median progression-free survival (mPFS) |
6.4 months
|
|||
| Patients Enrolled |
45 patients with progressive metastatic castration-resistant prostate cancer and diffuse bone marrow involvement.
|
||||
| Administration Time | 4 cycles | ||||
| Administration Dosage | 7.4 ± 1.4 GBq | ||||
| Evaluation Method | 68Ga-PSMA-11 PET/CT assay | ||||
| MOA of PDC |
Our findings suggest that repeated cycles of RLT with 177Lu-PSMA-617 can be carried out at an acceptable safety profile in mCRPC patients with diffuse bone marrow involvement. RLT may provide a suitable strategy for prolonged disease control with substantial clinical benefit. After a minimum of two cycles, treatment response translated into significantly longer median OS. Further studies should be carried out to investigate the role of individualized RLT concepts in this advanced stage setting.
Click to Show/Hide
|
||||
| Description |
Median imaging-based progression-free survival (PFS) was 6.4 mo (95% CI, 3.0-9.8) and the median overall survival (OS) was 10.2 months (95% CI, 7.2-12.8). The biochemical response translated into a significantly prolonged PFS (12.9 vs. 2.8 mo, p < 0.001) and OS (13.5 vs. 6.7 mo, p < 0.001).
|
||||
| Experiment 306 Reporting the Activity Data of This PDC | [67] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median progression-free survival (mPFS) |
6.6 months
|
|||
| Patients Enrolled |
52 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | Every 6-10 weeks for 6 cycles | ||||
| Administration Dosage | 7.3 GBq (5.9-7.4 GBq) | ||||
| Evaluation Method | 18F-Fluorodeoxyglucose (FDG) and 68Ga-PSMA (PSMA) Positron Emission Tomography/Computer Tomography (PET/CT) scans assay | ||||
| MOA of PDC |
PSA response patterns, PSA decline rate after the first RLT and pretherapy PSA doubling time are the most important predictors of OS in patients receiving Lu-177 PSMA RLT. FDG PET/CT can be utilized as additional decision-making for PSMA-RLT eligibility since high tumor heterogeneity and the presence of FDG > PSMA disease is associated with poor OS.
Click to Show/Hide
|
||||
| Description |
Median OS and PSA-PFS were 17.7 (95% confidence interval [CI]: 15.2-20.2) and 6.6 months (95% CI: 4.5-8.8), respectively. Primary resistance to PSMA-RLT (hazard ratio [HR]: 12.57, 95% CI: 2.4-65.2, p: 0.003), <30% PSA response rate after first cycle of PSMA-RLT (HR: 1.016, 95% CI: 1.006-1.03, p: 0.003), FDG > PSMA disease (HR: 4.9, 95% CI: 1.19-20.62, p: 0.03), PSA doubling time (PSA DT) of ≤2.4 months (HR: 15.7, 95% CI: 3.7-66.4, p: <0.0001), and low hemoglobin levels (HR: 0.59, 95% CI: 0.41-0.83, p: 0.003) were correlated with poor OS in the multivariate analysis. Bone scintigraphy > PSMA disease (HR: 5.6; 95% CI: 1.8-17, p: 0.002) and high C-reactive protein (HR: 1.4, 95% CI: 1.1-1.7, p: 0.001) were significant predictive biomarkers for PFS in the multivariate analysis.
Click to Show/Hide
|
||||
| Experiment 307 Reporting the Activity Data of This PDC | [30] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median progression-free survival (mPFS) |
6.9 months
|
|||
| Patients Enrolled |
50 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 4 cycles at 6-week intervals | ||||
| Administration Dosage | 7.5 GBq | ||||
| Description |
A further extension of this study with 50 patients recently reported ≥50% decrease in PSA in 64% of patients and grade 3-4 thrombocytopenia or anemia in 10% of the patients. Median progression-free survival (PFS) and overall survival (OS) was 6.9 months and 13.3 months, respectively.
|
||||
| Experiment 308 Reporting the Activity Data of This PDC | [62] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median progression-free survival (mPFS) |
7 months
|
|||
| Patients Enrolled |
58 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 1 to 5 cycles | ||||
| Administration Dosage | Average administered total cumulative dose of 13.32 GBq | ||||
| MOA of PDC |
Thus, the combination of 177Lu-PSMA-617 PRLT and AA therapy significantly improved patient's symptoms, PFS and OS as compared to only 177Lu-PSMA PRLT monotherapy in this study analysis. Based upon this promising observation, future prospective randomized controlled, multicenter clinical trials in a larger number of patients would be warranted to confirm this documented benefit of the combined 177Lu-PSMA-617 PRLT and AA therapy approach versus 177Lu-PSMA-617 PRLT monotherapy in patients of mCRPC.
Click to Show/Hide
|
||||
| Description |
On comparison of the treatment outcome between two groups, significant p value was found for symptomatic responders (58% in Group 1 vs. 85% in Group 2), median PFS (7 months in Group 1 vs. not reached in Group 2), and median OS (8 months in Group 1 vs. 16 months in Group 2), with better outcome in Group 2 patients for these variables.
|
||||
| Experiment 309 Reporting the Activity Data of This PDC | [22] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median progression-free survival (mPFS) |
7 months
|
|||
| Patients Enrolled |
40 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 2-5 cycles | ||||
| Administration Dosage | 4.44-5.55 GBq/cycle | ||||
| MOA of PDC |
The PSMA molecule acts as a target for theranostics in detecting and treating prostatic lesions. This ultimately promotes the concept of precision and personalized medicine. Several published articles showed favorable outcomes of Lu-PSMA-PRLT in mCRPC patients, which quickly translated into routine clinical practices with real effectiveness, a low toxicity profile, and documentation of the risk-benefit of PRLT. Nevertheless, many questions related to PRLT remain unresolved such as the sequencing of PRLT with ARTA or taxane-based chemotherapy, re-challenge therapy, combined therapy, alpha therapy in mCRPC patients, and early treatment of PRLT in mHNPC patients. To solve these questions, several clinical trials are currently under way, and the results of these trials will be helpful in deciding treatment strategies for prostate cancer patients.
Click to Show/Hide
|
||||
| Description |
Suman et al. evaluated the efficacy of 177Lu-PSMA-617 in heavily pre-treated mCRPC patients. A total of 40 mCRPC patients who received at least 2 cycles of 177Lu-PSMA-617 were included in this study. Twenty-one (52.5%) patients were responders (CR, PR, and SD) and 19 (47.5%) patients were non-responders (PD) on both symptomatic and biochemical scales. As per PET response criteria in solid tumor (PERCIST) criteria, 16 patients (43%) and 21 patients (57%) were responders and non-responders, respectively, on 68Ga-PSMA-11 PET/CT imaging. Metastatic nodal lesions responded better compared to liver and bony lesions. The median OS of 12 months and the median PFS of 7 months were registered without any grade 3/4 toxicity. The authors concluded that 177Lu-PSMA-617 controlled disease with good symptomatic and biochemical response rates without any high-grade clinical toxicity.
Click to Show/Hide
|
||||
| Experiment 310 Reporting the Activity Data of This PDC | [5] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median progression-free survival (mPFS) |
7.4 months
|
|||
| Patients Enrolled |
45 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 164 cycles of rnt, every 6-8 weeks | ||||
| Description |
Forty-five patients were treated with total of 164 cycles of RNT. Fifteen patients (33%) had PSA decline of ≥50%, 23 patients (51%) showed any PSA decline and 20 patients (44%) showed PSA increase of ≥25%. Median OS and PFS were 17,1 months and 7,4 months. Patients had any or ≥50% PSA response after the first cycle, lower initial ALP (<120U/L) had longer OS and PFS. Patients had normal Hb showed longer OS and patients had lower initial PSA (<51ng/mL) had longer PFS. Patients had PSA progression of ≥25% had shorter OS and PFS.
Click to Show/Hide
|
||||
| Experiment 311 Reporting the Activity Data of This PDC | [66] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median progression-free survival (mPFS) |
7.5 months
|
|||
| Patients Enrolled |
55 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | At least 2 cycles | ||||
| Administration Dosage | 7,400 MBq/cycles | ||||
| MOA of PDC |
The 177Lu-PSMA-617 kinetics in LNM and BM appear to be prognostic of treatment response, as well as of survival. In particular, OS appears to be linked with the kinetics parameters of BM, in keeping with the concept that BM is the most threatening pathogenic mechanism of mCRPC. This information, which should be confirmed by prospective trials, is readily obtainable from posttherapy scans and could be used to prognosticate treatment outcomes and design studies aimed to investigate the potential of PET-based prediction, as well as the possibility of patient-adapted therapeutic protocols of RLT.
Click to Show/Hide
|
||||
| Description |
Progression occurred in all patients, with a median time to the event of 7.5 mo (95% CI, 4.7-10.3 mo). An %IDred value above the median in both LNM and BM was associated with shorter survival. Moreover, higher %ID within the LNM correlated with longer survival. The kinetics of 177Lu-PSMA-617 within the organ metastasis had no prognostic implications.
Click to Show/Hide
|
||||
| Experiment 312 Reporting the Activity Data of This PDC | [22] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median progression-free survival (mPFS) |
7.6 months
|
|||
| Patients Enrolled |
30 patients with metastatic castration-resistant prostate cancer who underwent 4 cycles of mean 7.5 GBq Lu-PSMA 617 at 6weeks interval.
|
||||
| Administration Time | 1-4 cycles | ||||
| Administration Dosage | 4.4-8.7 GBq/cycle | ||||
| MOA of PDC |
The PSMA molecule acts as a target for theranostics in detecting and treating prostatic lesions. This ultimately promotes the concept of precision and personalized medicine. Several published articles showed favorable outcomes of Lu-PSMA-PRLT in mCRPC patients, which quickly translated into routine clinical practices with real effectiveness, a low toxicity profile, and documentation of the risk-benefit of PRLT. Nevertheless, many questions related to PRLT remain unresolved such as the sequencing of PRLT with ARTA or taxane-based chemotherapy, re-challenge therapy, combined therapy, alpha therapy in mCRPC patients, and early treatment of PRLT in mHNPC patients. To solve these questions, several clinical trials are currently under way, and the results of these trials will be helpful in deciding treatment strategies for prostate cancer patients.
Click to Show/Hide
|
||||
| Description |
In 2018, a phase II trial on 177Lu-PSMA-617 (LuPSMA trial) was published by Hofman et al. In this study, they included a total of 30 mCRPC patients who showed PD on standard therapies and received 1-4 cycles with 7.5 GBq of 177Lu-PSMA-617 (range: 4.4-8.7 GBq). They found >50% PSA decline in 17 patients (57%) and an objective response rate of 40%, 37%, and 37% of patients on 68Ga PSMA-11, FDG-PET/CT, and bone imaging, respectively. The median PFS was 7.6 months, and the median OS was 13.5 months after 177Lu-PSMA-617. Improvement in pain level was noted in 27 patients (90%), which significantly contributed to a better quality of life. 177Lu-PSMA-617 was well tolerated with minimal side effects. Commonly seen side effects were grade 1 dryness of mouth (87%), grade 1-2 transient nausea (50%) and fatigue (50%). Uncommonly seen side effects included grade 3-4 thrombocytopenia (13%), grade 3 anemia (13%), and neutropenia (7%). This was the first prospective single-arm, single-center, phase II study on the use of 177Lu-PSMA-617 in mCRPC patients.
Click to Show/Hide
|
||||
| Experiment 313 Reporting the Activity Data of This PDC | [68] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median progression-free survival (mPFS) |
8.0 months
|
|||
| Patients Enrolled |
51 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 2 cycles | ||||
| Administration Dosage | 12.9 GBq (range: 9.1-16.9) | ||||
| MOA of PDC |
68Ga-PSMA-11 PET-derived response assessment based on normalization of tumoral PSMA expression to normal liver tissue (TLR) may be an appropriate biomarker for monitoring 177Lu-PSMA-617 RLT in mCRPC patients and predicting survival outcome (PFS) of this treatment modality. Our study indicates the superiority of using liver-normalized tumor SUV values for molecular response assessment in this setting compared to the use of standard tumor SUV measurements, which are widely practiced at present. However, prospective studies with larger patient cohorts are needed to confirm these initial findings.
Click to Show/Hide
|
||||
| Description |
After a median follow-up of 49 months, the median PFS (95% CI) was 8.0 (5.9-10.1) months. In univariate analysis, responders showing partial remission (PRPSA and PRTLR) had significantly (p < 0.001, each) longer PFS (median: 10.5 and 9.3 months) than non-responders showing either stable or progressive disease (median: 4.0 and 3.5 months).
|
||||
| Experiment 314 Reporting the Activity Data of This PDC | [48] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median progression-free survival (mPFS) |
10 months
|
|||
| Patients Enrolled |
Patients with metastatic castration-resistant prostate cancer who underwent 68Ga-PSMA and FDG PET-CT scans.
|
||||
| Evaluation Method | 68Ga-PSMA/18F-FDG PET-CT assay | ||||
| Description |
In the period between 2016 and 2018, 58 patients were referred for [177Lu]-PSMA PRLT to the center, of which 51 patients underwent both [68Ga]-PSMA and FDG PET-CT scans and provisionally qualified for the analysis; out of these complete information of four patients was not available and hence were excluded. Thus, 47 patients were retrospectively recruited and categorized according to the proposed Pro-PET scoring scheme and were analyzed as discussed above. The cohort comprised of heavily pretreated patients with 2 (4.3%) underwent radical prostatectomy; surgical castration was performed in 45 (95.7%) patients; first-line hormonal therapy (with estrogen analogues, leutinizing hormone releasing hormone agonists and antagonists and antiandrogens) in 44 (93.6%) patients, second-line hormonal therapy (with CYP17 blockers and newer anti-androgens) in 34 (72.4%) patients; first-line chemotherapy (with docetaxel) in 33 (70.2%) patients, second-line chemotherapy (with cabazitaxel, oral metronomic chemotherapy, etc.) in 22 (46.8%) and radiotherapy in 26 (55.3%) patients.
Click to Show/Hide
|
||||
| Experiment 315 Reporting the Activity Data of This PDC | [35] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median progression-free survival (mPFS) |
10 months
|
|||
| Administration Time | Median of 4 (iqr: 2-7) cycles | ||||
| Administration Dosage | Mean cumulative activity of 30.7 ± 23.4 GBq | ||||
| MOA of PDC |
RLT with 177Lu-PSMA-617 can be effectively and safely initiated as early as 8 weeks after failure of 223Ra in patients with progressive bone-metastatic mCRPC refractory to 223Ra. Objective response can be achieved even in patients with more advanced disease and disseminated/diffuse bone metastases, albeit with increasing incidence of significant hematotoxicity.
Click to Show/Hide
|
||||
| Description |
Median imaging-based progression-free survival (PFS) was 10 (95% CI, 6-14) months and median overall survival (OS) was 18 (95% CI, 14-22) months.
|
||||
| In Vivo Model | 28 men with progressive metastatic castration-resistant prostate cancer who median age 73 years, range 63-89 years). | ||||
| Experiment 316 Reporting the Activity Data of This PDC | [22], [26] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median progression-free survival (mPFS) |
11 months
|
|||
| Patients Enrolled |
175 metastatic castration-resistant prostate cancer (mCRPC) patient were included in this meta-analysis. Median PFS was delineated in five studies and was 11 months (IQR, 7.6-13.7 months).
|
||||
| Administration Dosage | 3.7-8.7 GBq/cycle | ||||
| MOA of PDC |
The PSMA molecule acts as a target for theranostics in detecting and treating prostatic lesions. This ultimately promotes the concept of precision and personalized medicine. Several published articles showed favorable outcomes of Lu-PSMA-PRLT in mCRPC patients, which quickly translated into routine clinical practices with real effectiveness, a low toxicity profile, and documentation of the risk-benefit of PRLT. Nevertheless, many questions related to PRLT remain unresolved such as the sequencing of PRLT with ARTA or taxane-based chemotherapy, re-challenge therapy, combined therapy, alpha therapy in mCRPC patients, and early treatment of PRLT in mHNPC patients. To solve these questions, several clinical trials are currently under way, and the results of these trials will be helpful in deciding treatment strategies for prostate cancer patients.
Click to Show/Hide
|
||||
| Description |
Yadav et al. provided a meta-analysis of 177Lu-PSMA-PRLT for treating mCRPC patients. They analyzed 16 articles (13 articles used 177Lu-PSMA-617, 2 articles used 177Lu-PSMA-I&T, and 1 article used both radioligands). The authors showed >50% PSA decline after 177Lu-PSMA-PRLT in 46% of patients. Anatomical imaging response as per the RECIST criteria was reported by eight studies, with a proportion of 37.2% of patients had PR, SD in 38.3% of patients and PD in 24.5% of patients, whereas molecular imaging response as per the PERCIST criteria demonstrated PR in 74 patients (44.3%), SD in 39 patients (23.4%), and PD in 54 patients (32.3%). Common clinical toxicities were grades 1-2, which included anemia (23%), leukopenia (14.2%), thrombocytopenia (15%), nephrotoxicity (9.5%), and xerostomia (14.5%). The authors observed significant heterogeneity in several studies while analyzing this meta-analysis. They concluded that 177Lu-PSMA-PRLT is a promising treatment modality in mCRPC patients who showed PD after standard care treatments.
Click to Show/Hide
|
||||
| Experiment 317 Reporting the Activity Data of This PDC | [69] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median progression-free survival (mPFS) |
11.8 months
|
|||
| Patients Enrolled |
Patients with progressive disease (PD) on second-line hormonal therapy and/or docetaxel chemotherapy.
|
||||
| Administration Time | 8- to 12-weekly intervals | ||||
| Administration Dosage | 3.7 to 8 GBq | ||||
| Description |
The disease control rates according to the radiographic and molecular response were 77% and 71%, respectively. The median overall survival and median progression-free survivals were 14 and 11.8 months, respectively.
|
||||
| Experiment 318 Reporting the Activity Data of This PDC | [22] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median progression-free survival (mPFS) |
11.8 months
|
|||
| Patients Enrolled |
90 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 1-7 cycles | ||||
| Administration Dosage | 3.7-8 GBq/cycle | ||||
| MOA of PDC |
The PSMA molecule acts as a target for theranostics in detecting and treating prostatic lesions. This ultimately promotes the concept of precision and personalized medicine. Several published articles showed favorable outcomes of Lu-PSMA-PRLT in mCRPC patients, which quickly translated into routine clinical practices with real effectiveness, a low toxicity profile, and documentation of the risk-benefit of PRLT. Nevertheless, many questions related to PRLT remain unresolved such as the sequencing of PRLT with ARTA or taxane-based chemotherapy, re-challenge therapy, combined therapy, alpha therapy in mCRPC patients, and early treatment of PRLT in mHNPC patients. To solve these questions, several clinical trials are currently under way, and the results of these trials will be helpful in deciding treatment strategies for prostate cancer patients.
Click to Show/Hide
|
||||
| Description |
A favorable response rate (PSA and objective response) and safe profile of 177Lu-PSMA-617 were demonstrated in this study, leading to greater use of Lu-PSMA-PRLT in clinical practices. Similarly, Yadav et al. reported favorable outcomes of 177Lu-PSMA-617 in a prospective, single-arm, single-center study in 90 mCRPC patients.
|
||||
| Experiment 319 Reporting the Activity Data of This PDC | [33] | ||||
| Indication | ATM-mutated metastatic castration resistant prostate cancer | ||||
| Efficacy Data | Median progression-free survival (mPFS) |
12 months
|
|||
| Patients Enrolled |
121 metastatic castration-resistant prostate cancer patients.
|
||||
| Administration Dosage | Median administered cumulative activity: 20 GBq | ||||
| MOA of PDC |
177Lu-PSMA-617 RLT is an effective form of therapy in mCRPC patients and confirms the findings of the short-term studies. 177Lu-PSMA-617 prolongs the overall survival in mCRPC patients heavily pre-treated with chemotherapy, first and second-line anti-androgens, and androgen inhibitor therapies. The delayed toxicity is low and acceptable by most of these patients. Patients who were treated with various other mCRPC-approved compounds before 177Lu-PSMA-RLT were associated with a significantly shorter OS than that of the patients who received 177Lu-PSMA RLT at the earlier stages of mCRPC. An aggressive treatment approach, either sequential or in combination with second-generation anti-androgens, chemotherapies, or with investigational 225Ac-PSMA-617 alpha therapies, might prolong the survival of mCRPC patients in the future.
Click to Show/Hide
|
||||
| Description |
The median administered cumulative activity was 20 GBq (3.7-37 GBq). The median follow-up duration was 36 months (6-72 months). The estimated median PFS and OS were 12 months (mo) (95% CI: 10.3-13 mo) and 16 mo (95% CI: 13-17 mo), respectively. Any PSA decline and PSA decline >50% was achieved in 73% and 61% of the patients, respectively. Multivariate analysis revealed only failure to achieve >50% PSA decline as a significant factor associated with a poor PFS. Prognostic factors associated with reduced OS included, failure to experience >50% PSA decline, heavily pre-treated patient cohort who received >2 lines of prior treatment options, and patient sub-group treated with ≥2 lines of chemotherapy. Patients re-treated with additional treatment options after attaining 177Lu-PSMA refractory disease showed a remarkably prolonged OS. A significant clinical benefit was achieved post 177Lu-PSMA-617 RLT. The most common toxicities observed were fatigue (34.7%), followed by nausea (33%), and dry mouth (24.7%).
Click to Show/Hide
|
||||
| Experiment 320 Reporting the Activity Data of This PDC | [28] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median progression-free survival (mPFS) |
18 weeks
|
|||
| Patients Enrolled |
Patients with metastatic castration-resistant prostate cance, who had been treated with at least one next-generation antihormonal drug as well as chemotherapy.
|
||||
| Administration Time | 159 cycle | ||||
| Administration Dosage | Median dose 6.11 GBq | ||||
| Description |
The median estimated PSA progression-free survival (PPFS) was 18 weeks.
|
||||
| Experiment 321 Reporting the Activity Data of This PDC | [54] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median progression-free survival (mPFS) |
24 weeks
|
|||
| Patients Enrolled |
10 patients with metastatic castration-resistant prostate cancer and with visceral metastasis.
|
||||
| Administration Time | One cycle | ||||
| Administration Dosage | 4.88 GBq | ||||
| MOA of PDC |
Lutetium-177-PSMA was a reasonable palliative treatment option with limited toxicity for these end-stage mCRPC patients with visceral metastasis with adequate PSA stabilization. A synergistic drug amalgamation may be an ideal way to boost the outcome in the future.
|
||||
| Description |
Liver (80%), lung (30%), adrenal (10%), and peritoneum (10%) were the sites of visceral metastasis in our study. On PSA response assessment, 10%, 60%, and 30% of the patients had partial response, stable disease, and progressive disease, respectively. Forty percent of the patients had improvement in the VAS, while 50% had improvement in the AQS score. Median PFS was 24 weeks in our study. A cut-off of 4.88GBq of 177Lu-PSMA was the best-predicted progression with 66.67% sensitivity and 100% specificity on ROC analysis. Thirty percent of the patients showed grade 3 anemia. No other significant toxicity was seen.
Click to Show/Hide
|
||||
| Experiment 322 Reporting the Activity Data of This PDC | [52] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median progression-free survival (mPFS) |
27 months
|
|||
| Patients Enrolled |
19 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 5 (iqr: 3-6) cycles | ||||
| Administration Dosage | A cumulative activity of 32 ± 11 GBq | ||||
| Evaluation Method | 68Ga-PSMA-11 PET/CT assay | ||||
| MOA of PDC |
Intermittent 177Lu-PSMA-617 radioligand therapy in early responders with oligometastatic castration-resistant prostate cancer seems to not compromise survival outcome, despite long treatment-free intervals. The safety profile remained favorable, warranting further investigation of the concept of intermittent treatment in selected patients with a longer life-expectancy.
Click to Show/Hide
|
||||
| Description |
Four (21%) patients showed no response (PD) to the 177Lu-PSMA-RLT cycles after the first treatment break, and in two patients (11%), progression after the initial disease stabilization (SD) under subsequent cycles led to treatment discontinuation. Two patients (11%) completed the intended six cycles with a stable disease. In the remaining 11/19 (84%) patients, resuming 177Lu-PSMA-RLT resulted in a repeated PR. Altogether, 14/19 (74%) patients died by the time of this analysis. The median PFS was 27 (95% CI: 23-31) months and the OS was 45 (95% CI: 28-62) months.
Click to Show/Hide
|
||||
| Experiment 323 Reporting the Activity Data of This PDC | [18] | ||||
| Indication | ATM-mutated metastatic castration resistant prostate cancer | ||||
| Efficacy Data | Median PSA |
75 ng/mL
|
|||
| Patients Enrolled |
64 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 4 cycles | ||||
| Administration Dosage | 6.0/7.4 GBq | ||||
| MOA of PDC |
PSMA TRT involves conjugating radionuclides to antibodies and small molecule-ligands directed against PSMA. The most common radionuclide utilized to date is Lutetium-177, a beta-emitter with a mean path-length of 0.7 mm and maximum of 1.8 mm. Gamma-ray emission allows for concurrent single photon emission computed tomography (SPECT). Actinium-225 has been the most common alpha-emitter utilized. Alpha-emitters are thousands of times more potent and can induce double-stranded DNA breaks more difficult to repair, but mean path-length is much shorter than beta-emitters (under 0.01 mm).
Click to Show/Hide
|
||||
| Experiment 324 Reporting the Activity Data of This PDC | [18] | ||||
| Indication | ATM-mutated metastatic castration resistant prostate cancer | ||||
| Efficacy Data | Median PSA |
88 ng/mL
|
|||
| Patients Enrolled |
14 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 4 cycles | ||||
| Administration Dosage | Mean 7.0 GBq | ||||
| MOA of PDC |
PSMA TRT involves conjugating radionuclides to antibodies and small molecule-ligands directed against PSMA. The most common radionuclide utilized to date is Lutetium-177, a beta-emitter with a mean path-length of 0.7 mm and maximum of 1.8 mm. Gamma-ray emission allows for concurrent single photon emission computed tomography (SPECT). Actinium-225 has been the most common alpha-emitter utilized. Alpha-emitters are thousands of times more potent and can induce double-stranded DNA breaks more difficult to repair, but mean path-length is much shorter than beta-emitters (under 0.01 mm).
Click to Show/Hide
|
||||
| Experiment 325 Reporting the Activity Data of This PDC | [18] | ||||
| Indication | ATM-mutated metastatic castration resistant prostate cancer | ||||
| Efficacy Data | Median PSA |
182.97 ng/mL
|
|||
| Patients Enrolled |
44 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 1 cycle | ||||
| Administration Dosage | 7.4-22.2 GBq x 2 | ||||
| MOA of PDC |
PSMA TRT involves conjugating radionuclides to antibodies and small molecule-ligands directed against PSMA. The most common radionuclide utilized to date is Lutetium-177, a beta-emitter with a mean path-length of 0.7 mm and maximum of 1.8 mm. Gamma-ray emission allows for concurrent single photon emission computed tomography (SPECT). Actinium-225 has been the most common alpha-emitter utilized. Alpha-emitters are thousands of times more potent and can induce double-stranded DNA breaks more difficult to repair, but mean path-length is much shorter than beta-emitters (under 0.01 mm).
Click to Show/Hide
|
||||
| Experiment 326 Reporting the Activity Data of This PDC | [18] | ||||
| Indication | ATM-mutated metastatic castration resistant prostate cancer | ||||
| Efficacy Data | Median PSA |
189.8 ng/mL
|
|||
| Patients Enrolled |
50 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 4 cycles | ||||
| Administration Dosage | Median 7.4 GBq | ||||
| MOA of PDC |
PSMA TRT involves conjugating radionuclides to antibodies and small molecule-ligands directed against PSMA. The most common radionuclide utilized to date is Lutetium-177, a beta-emitter with a mean path-length of 0.7 mm and maximum of 1.8 mm. Gamma-ray emission allows for concurrent single photon emission computed tomography (SPECT). Actinium-225 has been the most common alpha-emitter utilized. Alpha-emitters are thousands of times more potent and can induce double-stranded DNA breaks more difficult to repair, but mean path-length is much shorter than beta-emitters (under 0.01 mm).
Click to Show/Hide
|
||||
| Experiment 327 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median radiographic progression-free survival (rPFS) |
8.7 months
|
|||
| Patients Enrolled |
551 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 6 doses every 6 weeks plus bsoc | ||||
| Administration Dosage | 7.4 GBq | ||||
| MOA of PDC |
Lutetium Lu 177 vipivotide tetraxetan is a PSMA-binding ligand bound to a DOTA chelator (i.e., tetraxetan) radiolabeled with lutetium-177. Once lutetium Lu 177 vipivotide tetraxetan is bound to PSMA-expressing cells, the beta-minus emission from lutetium-177 delivers radiation to PSMA-expressing and surrounding cells, inducing DNA damage that leads to cell death. The exposure-efficacy relationships of lutetium Lu 177 vipivotide tetraxetan and the time course of the pharmacodynamic response are not fully characterized [9]. Lutetium-177 decays to a stable hafnium-177 with a physical half-life of 6.647 days by emitting beta-minus radiation with a maximum energy of 0.498 MeV (79%) and photonic radiation (γ) of 0.208 MeV (11%) and 0.113 MeV (6.4%).
Click to Show/Hide
|
||||
| Description |
Median OS was significantly longer with lutetium Lu 177 vipivotide tetraxetan plus BSoC (n = 551) than with BSoC alone (n = 280) [15.3 vs 11.3 months [HR 0.62 (95% CI 0.52-0.74); p < 0.001]. Median rPFS was 8.7 months in the lutetium Lu 177 vipivotide tetraxetan plus BSoC arm (n = 385) compared with 3.4 months in the BSoC alone arm (n = 196) [HR for progression or death 0.40 (99.2% CI 0.29-0.57); p < 0.001). The overall response rate was also significantly higher in lutetium Lu 177 vipivotide tetraxetan arm (n = 319 patients with evaluable disease at baseline) than in the BSoC alone arm (n = 120) [30% vs 2%; p < 0.001].
Click to Show/Hide
|
||||
| Half life period | 41.6 h | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT03511664 | Clinical Status | Phase 3 | ||
| Clinical Description | The primary objective of this study was to compare the two alternate primary endpoints of radiographic progression-free survival (rPFS) and overall survival (OS) in patients with progressive prostate-specific membrane antigen (PSMA)-positive metastatic castration-resistant prostate cancer (mCRPC) who received 177Lu-PSMA-617 in addition to best supportive/best standard of care (BSC/BSoC) versus patients treated with best supportive/best standard of care alone. | ||||
| Experiment 328 Reporting the Activity Data of This PDC | [21] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median radiographic progression-free survival (rPFS) |
6.0 months
|
|||
| Patients Enrolled |
Patients with metastatic castration-resistant prostate cancer; taxane chemotherapy pretreated.
|
||||
| Experiment 329 Reporting the Activity Data of This PDC | [36] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median radiographic progression-free survival (rPFS) |
8.7 months
|
|||
| Patients Enrolled |
831 patients with metastatic castration-resistant prostate cancer.
|
||||
| Description |
Primary outcomes measured radiographic progression-free survival (rPFS) and OS between 177Lu PSMA-617 RLT plus SOC versus standard of care (SOC) alone. When compared to SOC alone, 177Lu PSMA-617 plus SOC significantly prolonged rPFS (median, 8.7 vs. 3.4 months; HR for progression or death 0.40; 99.2% CI, 0.29 to 0.57) and median OS (15.3 vs. 11.3 months; HR for death, 0.62; 95% CI, 0.52 to 0.74; p < 0.001).
Click to Show/Hide
|
||||
| Experiment 330 Reporting the Activity Data of This PDC | [41] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median radiographic progression-free survival (rPFS) |
8.7 months
|
|||
| Patients Enrolled |
385 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | Every 6 weeks for up to a total of 6 doses | ||||
| Administration Dosage | 7.4 GBq (200 mCi) | ||||
| MOA of PDC |
On March 23, 2022, the FDA approved 177Lu-PSMA-617 for the treatment of adult patients with PSMA-positive mCRPC who have been treated with androgen receptor pathway inhibition and taxane-based chemotherapy. The approval was based on a meaningful advantage in overall survival supported by a delay in tumor progression and higher objective response rate. The decision took into account several important factors unique to this applications context. Metastatic castration-resistant prostate cancer (mCRPC) is a life-threatening condition that lacks curative treatment, creating an unmet need. This product provides a novel mechanism of action as the first radioligand therapeutic agent for mCRPC providing anti-tumor effects in both bone and non-bone sites and may provide an opportunity to be combined with other available therapies with different toxicity profiles across mechanistic classes. Finally, 177Lu-PSMA-617 offers a different safety profile than other available systemic therapies which was determined to be acceptable for the indicated patient population, expanding treatment options that can be individualized to a patients preferences and comorbidities.
Click to Show/Hide
|
||||
| Description |
The co-primary endpoint of OS was statistically significant, with patients randomized to receive 177Lu-PSMA-617 plus BSoC having prolonged OS (median estimate 15.3 months) compared to BSoC alone (median estimate 11.3 months), hazard ratio (HR) 0.62 (95% CI: 0.52, 0.74, p<0.001). The planned interim OS analysis was not necessary as the targeted number of OS events were observed before the targeted number of rPFS events. Therefore, the final OS analysis was evaluated at the time of rPFS analysis.
Click to Show/Hide
|
||||
| Experiment 331 Reporting the Activity Data of This PDC | [21] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median radiographic progression-free survival (rPFS) |
8.8 months
|
|||
| Patients Enrolled |
Patients with metastatic castration-resistant prostate cancer; naive (T-naive).
|
||||
| Experiment 332 Reporting the Activity Data of This PDC | [70] | ||||
| Indication | ATM-mutated metastatic castration resistant prostate cancer | ||||
| Efficacy Data | Median survival time |
15.3 months
|
|||
| Patients Enrolled |
831 patients with that late-stage form of prostate cancer.
|
||||
| Description |
In the 831-person VISION trial, men with that late-stage form of prostate cancer who received 177Lu-PSMA-617 (Novartis) in addition to best supportive care had a median survival time of 15.3 months, compared with 11.3 months for individuals who received standard treatments alone.
|
||||
| Experiment 333 Reporting the Activity Data of This PDC | [14] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median survival time |
29.4 weeks
|
|||
| Patients Enrolled |
28 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 1-6 doses | ||||
| MOA of PDC |
Radiopharmaceuticals have been used in prostate cancer for decades with known efficacy in palliation of bone metastasis. The FDA approval of the most recent radiopharmaceutical, 177Lu-PSMA-617, shows a clear overall survival benefit compared to the best SOC. Current studies are ongoing to evaluate the effectiveness of 177Lu-PSMA-617 in earlier lines of therapy, such as after only 1 line of therapy with an ARPI as in the PSMAfore study, or in mCSPC in combination with ADT and an ARPI as in the PSMAddition study. Studies are also ongoing with 177Lu-PSMA-617 in combination with other treatments which may produce a synergistic effect. As described, there are many clinical trials ongoing that are modifying the 177Lu-PSMA-617 to possibly achieve improved results. Studies are also ongoing looking at swapping the 177Lu for another radioactive agent, such as 225Ac (an alpha emitter) which may have benefits over the beta-emitting 177Lu. Other studies are looking at J591, a monoclonal antibody to PSMA which has unique differences compared to small-molecule PSMA binders. Overall, PSMA-based radioligand therapy has been shown to be an effective and life-prolonging therapy and should be considered a treatment option for selected men with mCRPC. As described, there are many ongoing studies further evaluating PSMA radioligand therapy in Australia, South Africa, Europe, and the United States, representing a truly global effort to improve prostate cancer care.
Click to Show/Hide
|
||||
| Description |
A subsequent retrospective study, the first evaluating multiple administrations of 177Lu-PSMA-617, was reported by the same group. The authors reviewed 28 consecutive patients who received 50 infusions of 177Lu-PSMA-617 between 2014 and 2015. In their report, a PSA decline was noted in 59% and 75% of patients after 1 and 2 therapies, respectively, and a PSA decline of 50% or greater occurred in 32% and 50%, respectively. The estimated median survival was 29.4 weeks compared to 19.7 weeks in the historical best supportive care group which was statistically significant (HR 44; 95% CI 0.20-0.95; P=.031). Authors of the study also noted no significant changes in hematologic or renal parameters
Click to Show/Hide
|
||||
| Experiment 334 Reporting the Activity Data of This PDC | [38] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median time to pain progression |
8.3 months
|
|||
| Patients Enrolled |
Patients with metastatic castration-resistant prostate cancer treated with LuPSMA between December 2014 and July 2019.
|
||||
| Description |
Median baseline PSA was 1000 (interquartile range 431-2151) ng/ml. PSA decline of at least 50% at 12 wk was achieved in 22 (58%) patients, while median time to pain progression was 8.3 (95% confidence interval [CI] 4.1-12.6) mouth. Median overall survival was 11.6 (95% CI 8.8-14.3) mouth.
|
||||
| Related Clinical Trial | |||||
| NCT Number | NCT03511664 | Clinical Status | Phase 3 | ||
| Clinical Description | The primary objective of this study was to compare the two alternate primary endpoints of radiographic progression-free survival (rPFS) and overall survival (OS) in patients with progressive prostate-specific membrane antigen (PSMA)-positive metastatic castration-resistant prostate cancer (mCRPC) who received 177Lu-PSMA-617 in addition to best supportive/best standard of care (BSC/BSoC) versus patients treated with best supportive/best standard of care alone. | ||||
| Experiment 335 Reporting the Activity Data of This PDC | [59] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median time to pain progression |
1 months
|
|||
| Patients Enrolled |
551 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 6 cycles | ||||
| MOA of PDC |
177Lu-PSMA-617 represents not just a new therapy but a new therapeutic class for the treatment of prostate cancer. As such, clinical pathways need to be developed and clinicians involved in the treatment of mCRPC must become familiar with these new processes in order to realize the benefits of RLT for their patients. While not all the suggestions included in this discussion are strictly evidence-based, it is the hope of the authors that this review of the evidence and associated expert opinions help practitioners translate these data into the current Canadian practice setting. Finally, as the therapeutic landscape for mCRPC continues to evolve, new treatments and emerging data will need to be considered when making treatment decisions.
Click to Show/Hide
|
||||
| Description |
In the VISION trial, which enrolled patients with mCRPC who had received at least one line of ARPI treatment and one line of chemotherapy, 177Lu-PSMA-617 improved imaging-based progression-free survival (PFS) by 60% (hazard ratio [HR] = 0.40; 95% confidence interval [CI] 0.29-0.57; p < 0.001) and OS by 38% (HR = 0.62; 95% CI 0.52-0.74; p < 0.001) vs. trial-permitted best standard of care (SOC). The median imaging-based PFS was 8.7 months and median OS was 15.3 months for the 177Lu-PSMA-617 arm, vs. 3.4 months and 11.3 months, respectively, for the SOC arm.
Click to Show/Hide
|
||||
| Experiment 336 Reporting the Activity Data of This PDC | [59] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median time to pain progression |
5 months
|
|||
| Patients Enrolled |
234 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 6 cycles | ||||
| MOA of PDC |
177Lu-PSMA-617 represents not just a new therapy but a new therapeutic class for the treatment of prostate cancer. As such, clinical pathways need to be developed and clinicians involved in the treatment of mCRPC must become familiar with these new processes in order to realize the benefits of RLT for their patients. While not all the suggestions included in this discussion are strictly evidence-based, it is the hope of the authors that this review of the evidence and associated expert opinions help practitioners translate these data into the current Canadian practice setting. Finally, as the therapeutic landscape for mCRPC continues to evolve, new treatments and emerging data will need to be considered when making treatment decisions.
Click to Show/Hide
|
||||
| Description |
In PSMAfore, which enrolled patients who were chemotherapy-nave, at the time of the second interim analysis median imaging-based PFS was 6.4 months longer in the 177Lu-PSMA-617 arm vs. the ARPI change arm (HR = 0.43; 95% CI 0.33-0.54; p < 0.0001), while there was no significant difference in median OS, which was 19.25 vs. 19.71 months in the 177Lu-PSMA-617 and ARPI change arms, respectively (HR = 1.18; 95% CI 0.83-1.64). It is important to note that a high crossover rate occurred, with 84.2% of patients who progressed in the ARPI change arm subsequently receiving 177Lu-PSMA-617, thus likely diminishing the between-arm differences.
Click to Show/Hide
|
||||
| Experiment 337 Reporting the Activity Data of This PDC | [58] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Median whole-body tumor-absorbed dose |
11.55 Gy/MBq
|
|||
| Patients Enrolled |
Patients with prostate cancer.
|
||||
| Description |
Mean absorbed dose to kidneys, submandibular and parotid glands, liver, spleen, and bone marrow was 0.39, 0.44, 0.58, 0.1, 0.06, and 0.11 Gy/MBq, respectively. Median whole-body tumor-absorbed dose was 11.55 Gy and correlated with prostate-specific antigen (PSA) response at 12 wk. A median dose of 14.1 Gy was observed in patients achieving a PSA decline of at least 50%, versus 9.6 Gy for those achieving a PSA decline of less than 50% (P < 0.01). Of 11 patients receiving a tumor dose of less than 10 Gy, only one achieved a PSA response of at least 50%.
Click to Show/Hide
|
||||
| Experiment 338 Reporting the Activity Data of This PDC | [7], [71] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Mild nephrotoxic risk |
4.50%
|
|||
| Administration Time | Every 6 weeks for up to six doses | ||||
| Administration Dosage | 7.4 GBq | ||||
| MOA of PDC |
After binding to the PSMA receptor, [177Lu]Lu-PSMA-617 is internalized into the PSMA positive cells, resulting in a long retention within these cells; the high energy electrons emitted during the decay can selectively induce tissue and DNA damage, leading to cell death.
|
||||
| Description |
In a retrospective Australian study, the renal outcome during a longer follow-up time after treatment (median time 8 months) with either [177Lu]Lu-PSMA-617 or [177Lu]Lu-PSMA-I&T was evaluated at a mild nephrotoxic risk of 4.5%.
|
||||
| In Vivo Model | In this retrospective cohort study, we assessed 195 men with progressive mCRPC who had received therapy with 177Lu-PSMA as second- or third-line after standard therapeutic interventions. | ||||
| Half life period | 41.1 ± 9.3 h | ||||
| Experiment 339 Reporting the Activity Data of This PDC | [72] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Mild xerostomia |
3%
|
|||
| Patients Enrolled |
87 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 1 cycles | ||||
| Administration Dosage | 6.5 ± 1.1 GBq (range, 3.5-9.0 GBq) | ||||
| MOA of PDC |
Both 177Lu-PSMA I&T and 177Lu-PSMA-617 PRLT demonstrated favorable safety in mCRPC patients. The highest absorbed doses among healthy organs were in the lacrimal and parotid glands-not, however, resulting in any significant clinical sequel. 177Lu-PSMA-617 demonstrated a higher absorbed dose to the whole-body and lacrimal glands but a lower renal dose than did 177Lu-PSMA I&T. The mean absorbed tumor doses were comparable for both 177Lu-PSMA I&T and 177Lu-PSMA-617. There was a large interpatient variability in the dosimetry parameters. Therefore, individual patient-based dosimetry seems favorable for personalized PRLT.
Click to Show/Hide
|
||||
| Description |
Five patients (3.6%) reported mild, reversible xerostomia. 2 patients (3.9%) in the 177Lu-PSMA I&T group and 3 (3.4%) in 177Lu-PSMA-617 groupafter 2-6 cycles of treatment and in follow-up. Xerophthalmia was not reported by any patients. No other adverse symptoms were noticed during the entire follow-up period.
|
||||
| Experiment 340 Reporting the Activity Data of This PDC | [15] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Mortality rate |
49%
|
|||
| Patients Enrolled |
Patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 351 cycles | ||||
| Description |
A total of 51 patients (49%) died during the observation period. The majority of patients (97%) presented with bone metastases, 77% with lymph node metastases and 32% with visceral metastases.
|
||||
| Experiment 341 Reporting the Activity Data of This PDC | [63] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Mortality rate |
49.50%
|
|||
| Patients Enrolled |
Patients with metastatic castration-resistant prostate cancer.
|
||||
| Experiment 342 Reporting the Activity Data of This PDC | [55], [56] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Myelosuppression |
47.40%
|
|||
| Patients Enrolled |
Of the 1003 patients who underwent scanning, 831 (82.9%) were judged to have met all the trial eligibility criteria, including the PSMA imaging criteria, and were randomly assigned, between June 4, 2018, and October 23, 2019, to receive either <sup>177</sup>Lu-PSMA-617 plus protocol-permitted standard care (551 patients) or standard care alone (280).
Click to Show/Hide
|
||||
| Evaluation Method | PET/CT assay | ||||
| MOA of PDC |
Prostate-specific membrane antigen (PSMA)-targeted radiopharmaceutical like 177Lu-PSMA-617, a beta particle emitter has demonstrated improvement in overall survival in mCRPC patients pretreated with ARAT or taxanes. Although immune checkpoint inhibitors are being tested in mCRPC, there is no robust evidence to support this premise.
|
||||
| Description |
Myelosuppression was noted in 47.4% (grades 3-5 in 23.4%) patients in the Lu-PSMA-617 arm. Additional concerning toxicities included fatigue, xerostomia because of expression of PSMA in salivary glands, and nausea-vomiting.
|
||||
| Related Clinical Trial | |||||
| NCT Number | NCT03511664 | Clinical Status | Phase 3 | ||
| Experiment 343 Reporting the Activity Data of This PDC | [41] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Nausea | ≥ 20% | |||
| Patients Enrolled |
734 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 5 doses (range: 1 to 6) | ||||
| Administration Dosage | Median cumulative dose 37.5 GBq (range, 7.0 to 48.3) | ||||
| MOA of PDC |
On March 23, 2022, the FDA approved 177Lu-PSMA-617 for the treatment of adult patients with PSMA-positive mCRPC who have been treated with androgen receptor pathway inhibition and taxane-based chemotherapy. The approval was based on a meaningful advantage in overall survival supported by a delay in tumor progression and higher objective response rate. The decision took into account several important factors unique to this applications context. Metastatic castration-resistant prostate cancer (mCRPC) is a life-threatening condition that lacks curative treatment, creating an unmet need. This product provides a novel mechanism of action as the first radioligand therapeutic agent for mCRPC providing anti-tumor effects in both bone and non-bone sites and may provide an opportunity to be combined with other available therapies with different toxicity profiles across mechanistic classes. Finally, 177Lu-PSMA-617 offers a different safety profile than other available systemic therapies which was determined to be acceptable for the indicated patient population, expanding treatment options that can be individualized to a patients preferences and comorbidities.
Click to Show/Hide
|
||||
| Description |
Serious adverse reactions occurred in 36% of patients who received 177Lu-PSMA-617 plus BSoC. Fatal adverse reactions occurred in 2.8% of patients who received 177Lu-PSMA-617 plus BSoC, including sepsis (0.9%), pancytopenia (0.6%), hepatic failure (0.4%), intracranial hemorrhage (0.2%), subdural hematoma (0.2%), ischemic stroke (0.2%), COVID-19 (0.2%), and aspiration pneumonia (0.2%). The 2 fatal adverse reactions of intracranial hemorrhage and subdural hematoma occurred in patients who had concurrent treatment-related thrombocytopenia. The most common adverse reactions (≥ 20%) occurring at a higher incidence in patients who received 177Lu-PSMA-617 plus BSoC were fatigue, dry mouth, nausea, anemia, decreased appetite, and constipation. The most common laboratory abnormalities that worsened from baseline in ≥ 30% of patients who received 177Lu-PSMA-617 plus BSoC were decreased lymphocytes, decreased hemoglobin, decreased leukocytes, decreased platelets, decreased calcium, and decreased sodium.
Click to Show/Hide
|
||||
| Experiment 344 Reporting the Activity Data of This PDC | [33] | ||||
| Indication | ATM-mutated metastatic castration resistant prostate cancer | ||||
| Efficacy Data | Nausea |
33%
|
|||
| Patients Enrolled |
121 metastatic castration-resistant prostate cancer patients.
|
||||
| Administration Dosage | Median administered cumulative activity: 20 GBq | ||||
| MOA of PDC |
177Lu-PSMA-617 RLT is an effective form of therapy in mCRPC patients and confirms the findings of the short-term studies. 177Lu-PSMA-617 prolongs the overall survival in mCRPC patients heavily pre-treated with chemotherapy, first and second-line anti-androgens, and androgen inhibitor therapies. The delayed toxicity is low and acceptable by most of these patients. Patients who were treated with various other mCRPC-approved compounds before 177Lu-PSMA-RLT were associated with a significantly shorter OS than that of the patients who received 177Lu-PSMA RLT at the earlier stages of mCRPC. An aggressive treatment approach, either sequential or in combination with second-generation anti-androgens, chemotherapies, or with investigational 225Ac-PSMA-617 alpha therapies, might prolong the survival of mCRPC patients in the future.
Click to Show/Hide
|
||||
| Description |
The median administered cumulative activity was 20 GBq (3.7-37 GBq). The median follow-up duration was 36 months (6-72 months). The estimated median PFS and OS were 12 months (mo) (95% CI: 10.3-13 mo) and 16 mo (95% CI: 13-17 mo), respectively. Any PSA decline and PSA decline >50% was achieved in 73% and 61% of the patients, respectively. Multivariate analysis revealed only failure to achieve >50% PSA decline as a significant factor associated with a poor PFS. Prognostic factors associated with reduced OS included, failure to experience >50% PSA decline, heavily pre-treated patient cohort who received >2 lines of prior treatment options, and patient sub-group treated with ≥2 lines of chemotherapy. Patients re-treated with additional treatment options after attaining 177Lu-PSMA refractory disease showed a remarkably prolonged OS. A significant clinical benefit was achieved post 177Lu-PSMA-617 RLT. The most common toxicities observed were fatigue (34.7%), followed by nausea (33%), and dry mouth (24.7%).
Click to Show/Hide
|
||||
| Experiment 345 Reporting the Activity Data of This PDC | [14] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Nausea |
35%
|
|||
| Patients Enrolled |
831 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | Every 6 weeks for 4-6 cycles | ||||
| MOA of PDC |
Radiopharmaceuticals have been used in prostate cancer for decades with known efficacy in palliation of bone metastasis. The FDA approval of the most recent radiopharmaceutical, 177Lu-PSMA-617, shows a clear overall survival benefit compared to the best SOC. Current studies are ongoing to evaluate the effectiveness of 177Lu-PSMA-617 in earlier lines of therapy, such as after only 1 line of therapy with an ARPI as in the PSMAfore study, or in mCSPC in combination with ADT and an ARPI as in the PSMAddition study. Studies are also ongoing with 177Lu-PSMA-617 in combination with other treatments which may produce a synergistic effect. As described, there are many clinical trials ongoing that are modifying the 177Lu-PSMA-617 to possibly achieve improved results. Studies are also ongoing looking at swapping the 177Lu for another radioactive agent, such as 225Ac (an alpha emitter) which may have benefits over the beta-emitting 177Lu. Other studies are looking at J591, a monoclonal antibody to PSMA which has unique differences compared to small-molecule PSMA binders. Overall, PSMA-based radioligand therapy has been shown to be an effective and life-prolonging therapy and should be considered a treatment option for selected men with mCRPC. As described, there are many ongoing studies further evaluating PSMA radioligand therapy in Australia, South Africa, Europe, and the United States, representing a truly global effort to improve prostate cancer care.
Click to Show/Hide
|
||||
| Description |
Toxicities of grade 3 or higher were experienced by 52.7% of patients. The most common all-grade toxicities with 177Lu-PSMA-617 were fatigue (43.1%), dry mouth (38.8%-0% grade 3 or higher), and nausea (35.3%). The most common grade 3 or higher toxicities included anemia (12.9%), thrombocytopenia (7.9%), and leucopenia (7.8%).
|
||||
| Experiment 346 Reporting the Activity Data of This PDC | [14] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Neuropathy |
26%
|
|||
| Patients Enrolled |
200 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | Every 6 weeks (up to 6 cycles) | ||||
| MOA of PDC |
Radiopharmaceuticals have been used in prostate cancer for decades with known efficacy in palliation of bone metastasis. The FDA approval of the most recent radiopharmaceutical, 177Lu-PSMA-617, shows a clear overall survival benefit compared to the best SOC. Current studies are ongoing to evaluate the effectiveness of 177Lu-PSMA-617 in earlier lines of therapy, such as after only 1 line of therapy with an ARPI as in the PSMAfore study, or in mCSPC in combination with ADT and an ARPI as in the PSMAddition study. Studies are also ongoing with 177Lu-PSMA-617 in combination with other treatments which may produce a synergistic effect. As described, there are many clinical trials ongoing that are modifying the 177Lu-PSMA-617 to possibly achieve improved results. Studies are also ongoing looking at swapping the 177Lu for another radioactive agent, such as 225Ac (an alpha emitter) which may have benefits over the beta-emitting 177Lu. Other studies are looking at J591, a monoclonal antibody to PSMA which has unique differences compared to small-molecule PSMA binders. Overall, PSMA-based radioligand therapy has been shown to be an effective and life-prolonging therapy and should be considered a treatment option for selected men with mCRPC. As described, there are many ongoing studies further evaluating PSMA radioligand therapy in Australia, South Africa, Europe, and the United States, representing a truly global effort to improve prostate cancer care.
Click to Show/Hide
|
||||
| Description |
Grade 3-4 AEs occurred in 32 (33%) of men who received 177Lu-PSMA-617 versus 45 (53%) of men in the cabazitaxel group. All-grade toxicities that were more common in the 177Lu-PSMA-617 were dry mouth (60% vs. 21%), dry eyes (30% vs. 4%), and thrombocytopenia (18% vs. 5%). All-grade toxicities that were more common with cabazitaxel were diarrhea (52% vs. 18%), neuropathy (26% vs. 10%), and dysgeusia (27% vs. 12%).
Click to Show/Hide
|
||||
| Experiment 347 Reporting the Activity Data of This PDC | [6] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Objective response rate (ORR) |
30%
|
|||
| Patients Enrolled |
319 patients with metastatic castration-resistant prostate cancer and evaluable disease at baseline.
|
||||
| Administration Time | 6 doses every 6 weeks plus bsoc | ||||
| Administration Dosage | 7.4 GBq | ||||
| MOA of PDC |
Lutetium Lu 177 vipivotide tetraxetan is a PSMA-binding ligand bound to a DOTA chelator (i.e., tetraxetan) radiolabeled with lutetium-177. Once lutetium Lu 177 vipivotide tetraxetan is bound to PSMA-expressing cells, the beta-minus emission from lutetium-177 delivers radiation to PSMA-expressing and surrounding cells, inducing DNA damage that leads to cell death. The exposure-efficacy relationships of lutetium Lu 177 vipivotide tetraxetan and the time course of the pharmacodynamic response are not fully characterized [9]. Lutetium-177 decays to a stable hafnium-177 with a physical half-life of 6.647 days by emitting beta-minus radiation with a maximum energy of 0.498 MeV (79%) and photonic radiation (γ) of 0.208 MeV (11%) and 0.113 MeV (6.4%).
Click to Show/Hide
|
||||
| Description |
Median OS was significantly longer with lutetium Lu 177 vipivotide tetraxetan plus BSoC (n = 551) than with BSoC alone (n = 280) [15.3 vs 11.3 months [HR 0.62 (95% CI 0.52-0.74); p < 0.001]. Median rPFS was 8.7 months in the lutetium Lu 177 vipivotide tetraxetan plus BSoC arm (n = 385) compared with 3.4 months in the BSoC alone arm (n = 196) [HR for progression or death 0.40 (99.2% CI 0.29-0.57); p < 0.001). The overall response rate was also significantly higher in lutetium Lu 177 vipivotide tetraxetan arm (n = 319 patients with evaluable disease at baseline) than in the BSoC alone arm (n = 120) [30% vs 2%; p < 0.001].
Click to Show/Hide
|
||||
| Half life period | 41.6 h | ||||
| Related Clinical Trial | |||||
| NCT Number | NCT03511664 | Clinical Status | Phase 3 | ||
| Clinical Description | The primary objective of this study was to compare the two alternate primary endpoints of radiographic progression-free survival (rPFS) and overall survival (OS) in patients with progressive prostate-specific membrane antigen (PSMA)-positive metastatic castration-resistant prostate cancer (mCRPC) who received 177Lu-PSMA-617 in addition to best supportive/best standard of care (BSC/BSoC) versus patients treated with best supportive/best standard of care alone. | ||||
| Experiment 348 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Objective response rate (ORR) |
39%
|
|||
| Patients Enrolled |
35 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | Up to 4 cycles every 8 weeks | ||||
| Administration Dosage | 6.0-7.4 GBq/cycle | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
A randomized, parallel group, open label, and non-inferiority phase II trial conducted between 2019 and 2021 studied a group of thirty five chemo-naive patients with mCPRC and high expressing PSMA lesions on 68Ga-PSMA-11 on PET/CT. Patients were randomized in 1:1 ratio to either 177Lu PSMA-617 (6.0-7.4 GBq/cycle, every 8 weeks, up to 4 cycles) or docetaxel (75 mg/m2/cycle, every 3 weeks, for up to 10 cycles), with fifteen and twenty patients in each group, respectively. The primary endpoint was best PSA response rate (PSA-RR), which is defined as a ≥ 50% decline in PSA from baseline. The 177Lu PSMA-617 arm PSA-RR was 60% versus 40% in docetaxel group with a difference in PSA-RR of 20% (95% CI:1-47, p = 0.025) and met the pre-specified criterion for non-inferiority which was defined as margin of 15% decline in PSA-RR. The PFS rate for 177Lu PSMA-617 was 30% versus 20% for docetaxel (95% CI:18-38, p = 0.5). The number of treatment-related adverse events grade 3 or higher occurred less in the 177Lu PSMA-617 arm than the docetaxel arm (30% versus 50% respectively, p = 0.2).
Click to Show/Hide
|
||||
| Experiment 349 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Objective response rate (ORR) |
46%
|
|||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
The Thera-P trial was a phase II prospective multicenter trial looking at those with mCPRC who progressed after docetaxel chemotherapy and were randomly assigned to 177Lu PSMA-617 or cabazitaxel. Initial reported results found that those who were treated with 177Lu PSMA-617 treatment led to improvement in PSA response rate (66% vs 37%), RECIST response rate (49% vs 24%), PFS (HR 0.63), less G3-G4 toxicities (33% vs 53%), and overall better patient reported outcomes.
Click to Show/Hide
|
||||
| Experiment 350 Reporting the Activity Data of This PDC | [22], [23] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Objective response rate (ORR) |
29%
|
|||
| Patients Enrolled |
Twelve studies including 669 metastatic castration-resistant prostate cancer patients reported <sup>177</sup>Lu-PSMA radioligand therapy(RLT). Of evaluable articles, a median of 29% (IQR 8-36%) of the patients had objective remission.
|
||||
| Evaluation Method | PET/CT assay | ||||
| MOA of PDC |
The PSMA molecule acts as a target for theranostics in detecting and treating prostatic lesions. This ultimately promotes the concept of precision and personalized medicine. Several published articles showed favorable outcomes of Lu-PSMA-PRLT in mCRPC patients, which quickly translated into routine clinical practices with real effectiveness, a low toxicity profile, and documentation of the risk-benefit of PRLT. Nevertheless, many questions related to PRLT remain unresolved such as the sequencing of PRLT with ARTA or taxane-based chemotherapy, re-challenge therapy, combined therapy, alpha therapy in mCRPC patients, and early treatment of PRLT in mHNPC patients. To solve these questions, several clinical trials are currently under way, and the results of these trials will be helpful in deciding treatment strategies for prostate cancer patients.
Click to Show/Hide
|
||||
| Description |
A systematic review on the comparison of 177Lu-PSMA-PRLT with third-line treatments such as abiraterone, enzalutamide, and cabazitaxel was published by Von Eyben et al. A significant difference of PSA response was seen between the two groups (a PSA decline of ≥50% in 44% of patients in Lu-PSMA-PRLT group versus only 22% of patients in third-line treatment group). The authors mentioned that, despite variations in doses and number of cycles, 177Lu-PSMA-PRLT group showed a favorable response rate as compared to the third-line treatment group, and they also mentioned more side effects and discontinuation of third-line treatment as compared to 177Lu-PSMA- PRLT group.
Click to Show/Hide
|
||||
| Experiment 351 Reporting the Activity Data of This PDC | [22] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Objective response rate (ORR) |
40%
|
|||
| Patients Enrolled |
30 patients with metastatic castration-resistant prostate cancer who underwent 4 cycles of mean 7.5 GBq Lu-PSMA 617 at 6weeks interval.
|
||||
| Administration Time | 1-4 cycles | ||||
| Administration Dosage | 4.4-8.7 GBq/cycle | ||||
| Evaluation Method | PET/CT assay | ||||
| MOA of PDC |
The PSMA molecule acts as a target for theranostics in detecting and treating prostatic lesions. This ultimately promotes the concept of precision and personalized medicine. Several published articles showed favorable outcomes of Lu-PSMA-PRLT in mCRPC patients, which quickly translated into routine clinical practices with real effectiveness, a low toxicity profile, and documentation of the risk-benefit of PRLT. Nevertheless, many questions related to PRLT remain unresolved such as the sequencing of PRLT with ARTA or taxane-based chemotherapy, re-challenge therapy, combined therapy, alpha therapy in mCRPC patients, and early treatment of PRLT in mHNPC patients. To solve these questions, several clinical trials are currently under way, and the results of these trials will be helpful in deciding treatment strategies for prostate cancer patients.
Click to Show/Hide
|
||||
| Description |
In 2018, a phase II trial on 177Lu-PSMA-617 (LuPSMA trial) was published by Hofman et al. In this study, they included a total of 30 mCRPC patients who showed PD on standard therapies and received 1-4 cycles with 7.5 GBq of 177Lu-PSMA-617 (range: 4.4-8.7 GBq). They found >50% PSA decline in 17 patients (57%) and an objective response rate of 40%, 37%, and 37% of patients on 68Ga PSMA-11, FDG-PET/CT, and bone imaging, respectively. The median PFS was 7.6 months, and the median OS was 13.5 months after 177Lu-PSMA-617. Improvement in pain level was noted in 27 patients (90%), which significantly contributed to a better quality of life. 177Lu-PSMA-617 was well tolerated with minimal side effects. Commonly seen side effects were grade 1 dryness of mouth (87%), grade 1-2 transient nausea (50%) and fatigue (50%). Uncommonly seen side effects included grade 3-4 thrombocytopenia (13%), grade 3 anemia (13%), and neutropenia (7%). This was the first prospective single-arm, single-center, phase II study on the use of 177Lu-PSMA-617 in mCRPC patients.
Click to Show/Hide
|
||||
| Experiment 352 Reporting the Activity Data of This PDC | [73] | ||||
| Indication | Prostate cancer | ||||
| Efficacy Data | Overall detection rates |
38.50%
|
|||
| Patients Enrolled |
Patients with biochemical relapse and negative conventional (MRI, MRS, CT scan and bone scintigraphy) imaging.
|
||||
| Administration Time | 3 h, 24 h and 72 h | ||||
| Administration Dosage | 185 MBq | ||||
| Evaluation Method | 177Lu-PSMA SPECT scan assay | ||||
| Description |
A total of 26 patients, with a mean age of 70 years (range: 46 to 89 years) were included in this study. The overall detection rates were 38.5% (10 out of 26 patients).
|
||||
| Experiment 353 Reporting the Activity Data of This PDC | [47] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Overall survival (OS) |
24.9 months
|
|||
| Patients Enrolled |
40 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | Once every 6-8 weeks, for a maximum of four to six cycles | ||||
| Administration Dosage | 6.0-8.5 GBq | ||||
| Evaluation Method | 68Ga-PSMA-11 PET/CT assay | ||||
| MOA of PDC |
Also, previously identified risk factors in mCRPC, such as lactate dehydrogenase or albumin, were not available or were not collected systematically and consequently not tested in the models. Similarly, 2-[18F]FDG-PET was available only in a minority of patients in this study and thus could not be tested in the models. Dual-tracer PET imaging with [68Ga]Ga-PSMA-11 and 2-[18F]FDG-PET can improve patient selection for 177Lu-PSMA therapy; however, several steps are required to establish 2-[18F]FDG-PET as a screening tool for 177Lu-PSMA in practice (ie, confirmation of its prognostic value in a multicentre setting, standardisation of image interpretation, inclusion in drug label and guidelines, and insurance coverage).
Click to Show/Hide
|
||||
| Description |
The C-index of the overall survival model was 071 (95% CI 069-073). Similar C-indices were achieved at internal validation (071 [069-073]) and external validation (072 [068-076]). The C-index of the PSA-progression-free survival model was 070 (95% CI 068-072). Similar C-indices were achieved at internal validation (070 [068-072]) and external validation (071 [068-074]). Both models were adequately calibrated and their predictions correlated with the observed outcome. Compared with high-risk patients, low-risk patients had significantly longer overall survival in the validation cohort (249 months [95% CI 168-273] vs 74 months [40-108]; p<00001) and PSA-progression-free survival (66 months [60-71] vs 25 months [12-38]; p=0022).
Click to Show/Hide
|
||||
| Related Clinical Trial | |||||
| NCT Number | NCT03042312 | Clinical Status | Phase 2 | ||
| Clinical Description | This was an open-label, multicenter, prospective trial to assess safety and efficacy of 177Lu-PSMA-617 in patients with metastatic castration resistant prostate cancer. | ||||
| Experiment 354 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Overall survival (OS) |
15.3 months
|
|||
| Patients Enrolled |
581 patients with metastatic castration-resistant prostate cancer.
|
||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
The VISION trial was an international open-label phase 3 trial that assigned 581 mCRPC patients who previously received a novel hormonal agent and chemotherapy to either the treatment group (receiving 177Lu-PSMA-617 and standard of care) or control group (standard of care alone). Primary end points were progression-free survival, median overall survival, and median follow-up. Median progression-free survival was 8.7 months in the 177Lu-PSMA-617 group, as compared with 3.4 months in the control group (HR for progression or death, 0.40; 99.2% confidence interval, 0.29 to 0.57; P < 0.001). Median overall survival was 15.3 months in the 177Lu-PSMA-617 group, as compared with 11.3 months in the control group (hazard ratio for death, 0.62; 95% CI, 0.52 to 0.74; P < 0.001). The median follow-up was 20.3 months (95% CI, 19.8 to 21.0) in the 177Lu-PSMA-617 group and 19.8 months (95% CI, 18.3 to 20.8) in the control group. Secondary end points included median time to the first symptomatic skeletal event or death and PSA level. The median time to the first symptomatic skeletal event or death was 11.5 months in the 177Lu-PSMA-617 group, as compared with 6.8 months in the control group (P < 0.001). The proportions of patients with confirmed decreases in the PSA level of at least 50% and 80% from baseline were higher in the 177Lu-PSMA-617 group than in the control group.
Click to Show/Hide
|
||||
| Experiment 355 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Overall survival (OS) |
12.4 months
|
|||
| Patients Enrolled |
40 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | Up to 4 cycles (median number of 3 cycles, range 2-5) every eight to twelve weeks | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
A phase II study followed forty patients with PET/CT-68Ga-PSMA positive mCRPC treated with 177Lu PSMA-617. 177Lu PSMA-617 was given for up to four cycles (median number of three cycles, range 2-5) every eight to twelve weeks. With a median follow-up of 15.5 months (range 6-22 ), 37.5% of patients had a greater than 50% PSA decline and 50% had a PSA decline greater than 30%. The median PFS was 7.5 months (95% CI: 4.8-10.5) and median OS was 12.4 months (95% CI 7.4-20.3 months).
Click to Show/Hide
|
||||
| Experiment 356 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Overall survival (OS) |
13.5 months
|
|||
| Patients Enrolled |
30 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 4 cycles | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
Another single-arm, single-center, phase 2 trial recruited thirty men with mCRPC and progressive disease after receiving standard treatments including taxane-based chemotherapy and second-generation anti-androgen treatment (abiraterone, enzalutamide, or both). They were administered four cycles of 177Lu-PSMA-617. The primary end points included PSA level, imaging response using bone scan, and PET/CT and quality of life. The PSA decline of greater than or equal to 50% was achieved in 57% of patients. Imaging response using PSMA PET showed a complete response in 10% of patients, a partial response in 30% of patients, and progressive disease in 27% of patients. Cognitive functioning, insomnia, and pain, which were measured using the EORTC-QLQ30 (European Organization for the Research and Treatment of Cancer Quality of Life Questionnaire) and BPI (brief pain inventory) scoring tools showed improvement during treatment compared to baseline, thus indicating improved quality of life.
Click to Show/Hide
|
||||
| Experiment 357 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Overall survival (OS) |
15.3 months
|
|||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
The Thera-P trial was a phase II prospective multicenter trial looking at those with mCPRC who progressed after docetaxel chemotherapy and were randomly assigned to 177Lu PSMA-617 or cabazitaxel. Initial reported results found that those who were treated with 177Lu PSMA-617 treatment led to improvement in PSA response rate (66% vs 37%), RECIST response rate (49% vs 24%), PFS (HR 0.63), less G3-G4 toxicities (33% vs 53%), and overall better patient reported outcomes.
Click to Show/Hide
|
||||
| Experiment 358 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Overall survival (OS) |
50 weeks
|
|||
| Patients Enrolled |
14 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | Up to 3 cycles every six weeks | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
A prospective phase II pilot study enrolled fourteen patients with progressive and symptomatic mCRPC despite taxane and novel anti-androgen therapy to receive up to four cycles of 177Lu PSMA-617 every six weeks. Ten out of the 14 patients had a mean PSA reduction of 59%, with five patients having over a 50% reduction, and nine patients having over a 30% reduction in PSA levels. At baseline testing, the PSMA PET SUV predicted a reduction in PSA of more than 30%, with an SUV max value of 17 ± 9 compared to 44 ± 15 (p < 0.007), and a PSMA SUV mean of 6 ± 4 compared to 10 ± 4 (p < 0.04).
Click to Show/Hide
|
||||
| Experiment 359 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Overall survival (OS) |
16 months
|
|||
| Patients Enrolled |
31 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 2 cycles (range: 1-4) | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
A prospective single center phase II study included 31 patients with mCRPC who had progressed despite second-line hormonal therapy and/or docetaxel chemotherapy. The patients underwent an average of two cycles (range 1-4) of 177Lu-DKFZ-PSMA-617 therapy. The primary endpoints of the study were to determine radiographic progression-free survival (RPFS) using PET/CT scans and overall survival (OS). The treatment response was evaluated based on biochemical response using serum PSA, molecular response using PET/CT scans, and clinical response using VAS (visual analogue scale), AS (analgesic score) and ECOG (Eastern Cooperative Oncology Group) performance status. Biochemical response showed that the mean serum PSA level after three months of initial therapy was 141.75 ± 187.43 ng/mL (range 2.5-807). The mean serum PSA level three months after the second cycle was 153.07 ± 204 ng/mL (range 1.34-762). The molecular response estimated by the mean SUVmax (maximum standardized uptake value) of tumor lesions before and after therapy was 56.7 and 18.2 respectively. In two patients it was reduced from 32.67 to 0.38 after 177Lu-DKFZ-PSMA-617 therapy, thus indicating a complete remission. The clinical response was estimated using the mean VASmax and AS. The pre-therapy VASmax was 7.5 ± 1, and post-therapy was 3 ± 0.9 (p < 0.0001), while the mean AS pre-therapy and post therapy was 2.5 ± 1.09 and 1.8 ± 0.98 (p = 0.009) respectively, and mean ECOG performance status improved from 2.54 ± 0.85 to 1.78 ± 0.92 after completion of therapy (p = 0.001). The median overall survival was 16 months, and progression-free survival was 12 months. 16.1% patients died due to disease during follow-up. This trial particularly highlighted an improvement in the ECOG performance status in patients receiving 177Lu-DKFZ-PSMA-617 for the treatment of mCRPC.
Click to Show/Hide
|
||||
| Experiment 360 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Overall survival (OS) |
12 months
|
|||
| Patients Enrolled |
191 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 1-5 cycles | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
A real-world study evaluated 191 patients with mCPRC treated with 177Lu-PSMA-617. Patients had confirmation of PSMA expressing lesions by 68Ga-PSMA-ligand PET/CT. The majority of individuals (90%) had first- and second-line systemic treatment prior to being treated with 177Lu-PSMA-617. Patients received one to five cycles of treatment and specific endpoints included biochemical response, radiologic response, PSA PFS, and OS. A PSA RR (defined as a decline of ≥50% in PSA) was found in 56% of patients, and any PSA decline occurred in 75% of patients. The median radiographic progression-free survival was found to be six months (range 3-10), PSA PFS (n = 132) was 4 months (range 3-8), and the overall survival (n = 191) was 12 months (range 5-18).
Click to Show/Hide
|
||||
| Experiment 361 Reporting the Activity Data of This PDC | [30] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Overall survival (OS) |
13.3 months
|
|||
| Patients Enrolled |
50 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 4 cycles at 6-week intervals | ||||
| Administration Dosage | 7.5 GBq | ||||
| Description |
A further extension of this study with 50 patients recently reported ≥50% decrease in PSA in 64% of patients and grade 3-4 thrombocytopenia or anemia in 10% of the patients. Median progression-free survival (PFS) and overall survival (OS) was 6.9 months and 13.3 months, respectively.
|
||||
| Experiment 362 Reporting the Activity Data of This PDC | [18] | ||||
| Indication | ATM-mutated metastatic castration resistant prostate cancer | ||||
| Efficacy Data | Overall survival (OS) |
13.3 months
|
|||
| Patients Enrolled |
50 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 4 cycles | ||||
| Administration Dosage | Median 7.4 GBq | ||||
| MOA of PDC |
PSMA TRT involves conjugating radionuclides to antibodies and small molecule-ligands directed against PSMA. The most common radionuclide utilized to date is Lutetium-177, a beta-emitter with a mean path-length of 0.7 mm and maximum of 1.8 mm. Gamma-ray emission allows for concurrent single photon emission computed tomography (SPECT). Actinium-225 has been the most common alpha-emitter utilized. Alpha-emitters are thousands of times more potent and can induce double-stranded DNA breaks more difficult to repair, but mean path-length is much shorter than beta-emitters (under 0.01 mm).
Click to Show/Hide
|
||||
| Experiment 363 Reporting the Activity Data of This PDC | [20] | ||||
| Indication | Advanced prostate cancer | ||||
| Efficacy Data | Overall survival (OS) |
14 months
|
|||
| Patients Enrolled |
Patients with advanced prostate cancer.
|
||||
| Administration Time | 2 cycles | ||||
| Description |
The median PSA-PFS and overall survival were 3.2 mo (95% confidence interval, 2.6-3.7 mo) and 14.0 mo (95% confidence interval, 6.2-21.8 mo), respectively.
|
||||
| Experiment 364 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Overall survival (OS) |
14.5 months
|
|||
| Patients Enrolled |
254 patients with metastatic castration-resistant prostate cancer.
|
||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
The REALITY (REgistry to Assess Outcome and Toxicity of Targeted RadionucLIde TherapY) study was a prospective real world cohort of 254 patients with mCRPC who received 177Lu-PSMA-617 as experimental salvage therapy after conventional treatments had failed. The primary end points were efficacy, reflected by PSA-PFS, (prostate specific antigen-progression-free survival) OS, (overall survival) and safety which was reflected by the incidence of treatment-related (AEs). Over the entire course of 177Lu-PSMA-617 RLT (radioligand therapy), 52.0% patients had a greater than 50% decline in their PSA response. At a median (minimum - maximum) follow-up of 14.9 (5.0-64.4) months, the median PSA-PFS was 5.5 (4.4-6.6) months, while the median OS was 14.5 (11.5-17.5) months.
Click to Show/Hide
|
||||
| Experiment 365 Reporting the Activity Data of This PDC | [18] | ||||
| Indication | ATM-mutated metastatic castration resistant prostate cancer | ||||
| Efficacy Data | Overall survival (OS) |
16 months
|
|||
| Patients Enrolled |
44 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 1 cycle | ||||
| Administration Dosage | 7.4-22.2 GBq x 2 | ||||
| MOA of PDC |
PSMA TRT involves conjugating radionuclides to antibodies and small molecule-ligands directed against PSMA. The most common radionuclide utilized to date is Lutetium-177, a beta-emitter with a mean path-length of 0.7 mm and maximum of 1.8 mm. Gamma-ray emission allows for concurrent single photon emission computed tomography (SPECT). Actinium-225 has been the most common alpha-emitter utilized. Alpha-emitters are thousands of times more potent and can induce double-stranded DNA breaks more difficult to repair, but mean path-length is much shorter than beta-emitters (under 0.01 mm).
Click to Show/Hide
|
||||
| Experiment 366 Reporting the Activity Data of This PDC | [16] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Overall survival (OS) |
47 weeks
|
|||
| Patients Enrolled |
Patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | Every 6weeks | ||||
| Administration Dosage | 7.5 GBq | ||||
| Description |
There was no significant difference comparing the rate of > 50% PSA decline or best PSA response between the 6.0 GBq and 7.5 GBq group (35% vs. 54%, p = 0.065; and - 40.2% vs. - 57.8%, p = 0.329). The median estimated survival and PSA-PFS did not significantly differ between the 6.0 GBq and 7.5 GBq groups as well (11.3 vs. 12.7 months, p = 0.384; and 9.5 vs. 12.3 months, p = 0.258).
Click to Show/Hide
|
||||
| Experiment 367 Reporting the Activity Data of This PDC | [16] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Overall survival (OS) |
47 weeks
|
|||
| Patients Enrolled |
Patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | Every 8weeks | ||||
| Administration Dosage | 6.0 GBq | ||||
| Description |
There was no significant difference comparing the rate of > 50% PSA decline or best PSA response between the 6.0 GBq and 7.5 GBq group (35% vs. 54%, p = 0.065; and - 40.2% vs. - 57.8%, p = 0.329). The median estimated survival and PSA-PFS did not significantly differ between the 6.0 GBq and 7.5 GBq groups as well (11.3 vs. 12.7 months, p = 0.384; and 9.5 vs. 12.3 months, p = 0.258).
Click to Show/Hide
|
||||
| Experiment 368 Reporting the Activity Data of This PDC | [18] | ||||
| Indication | ATM-mutated metastatic castration resistant prostate cancer | ||||
| Efficacy Data | Overall survival (OS) |
50 weeks
|
|||
| Patients Enrolled |
14 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 4 cycles | ||||
| Administration Dosage | Mean 7.0 GBq | ||||
| MOA of PDC |
PSMA TRT involves conjugating radionuclides to antibodies and small molecule-ligands directed against PSMA. The most common radionuclide utilized to date is Lutetium-177, a beta-emitter with a mean path-length of 0.7 mm and maximum of 1.8 mm. Gamma-ray emission allows for concurrent single photon emission computed tomography (SPECT). Actinium-225 has been the most common alpha-emitter utilized. Alpha-emitters are thousands of times more potent and can induce double-stranded DNA breaks more difficult to repair, but mean path-length is much shorter than beta-emitters (under 0.01 mm).
Click to Show/Hide
|
||||
| Experiment 369 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Overall survival (OS) |
62.7 weeks
|
|||
| Patients Enrolled |
21 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | Every 8 weeks | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
Another real-world prospective cohort study included twenty-one treatments refractory mCRPC patients at Bushehr Department of Nuclear Medicine between December 2016 to December 2018 treated with 177Lu-PSMA-617 every 8 weeks. Patients had to have PSMA secreting lesions detected by PSMA imaging with 68Ga-PSMA PET or 177Lu/99Tc-PSMA before to undergoing treatment. The mean age of patients was 70.3 ± 9.6 (range 54-88) with a median of two cycles of treatment (range 1-4). The primary endpoint of the study was to assess biochemical response (BCR), which was defined as a drop in the PSA of more than 50. Additional secondary endpoints included response by ECOG and overall survival. A BCR was seen in 62% of patients. The estimated overall survival was seen to be 62.69 weeks (95% confidence interval: 42.06-83.33) with a median follow-up period of 9 months (range 1-25 months).
Click to Show/Hide
|
||||
| Experiment 370 Reporting the Activity Data of This PDC | [54] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Pain relief rate |
50%
|
|||
| Patients Enrolled |
10 patients with metastatic castration-resistant prostate cancer and with visceral metastasis.
|
||||
| Administration Time | One cycle | ||||
| Administration Dosage | 4.88 GBq | ||||
| MOA of PDC |
Lutetium-177-PSMA was a reasonable palliative treatment option with limited toxicity for these end-stage mCRPC patients with visceral metastasis with adequate PSA stabilization. A synergistic drug amalgamation may be an ideal way to boost the outcome in the future.
|
||||
| Description |
Liver (80%), lung (30%), adrenal (10%), and peritoneum (10%) were the sites of visceral metastasis in our study. On PSA response assessment, 10%, 60%, and 30% of the patients had partial response, stable disease, and progressive disease, respectively. Forty percent of the patients had improvement in the VAS, while 50% had improvement in the AQS score. Median PFS was 24 weeks in our study. A cut-off of 4.88GBq of 177Lu-PSMA was the best-predicted progression with 66.67% sensitivity and 100% specificity on ROC analysis. Thirty percent of the patients showed grade 3 anemia. No other significant toxicity was seen.
Click to Show/Hide
|
||||
| Experiment 371 Reporting the Activity Data of This PDC | [45] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Pain relief rate |
52%
|
|||
| Patients Enrolled |
23 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 16 week | ||||
| Administration Dosage | 6 GBq (162.16 mCi) | ||||
| MOA of PDC |
This study shows that PSA changes in patients with mCRPC as early as four weeks after the first administration of PSMA-RLT are predictive of both long-term biochemical and PET imaging responses, as well as overall survival. At this early stage, a PSA decrease of at least 30% was found to be more suitable to detect future responders, as well as a longer overall survival compared to the threshold of 50% proposed by the PCWG for long-term biochemical evaluation. An early increase in PSA (+25%) is a strong predictor for biochemical progression and shorter overall survival. Larger prospective studies are warranted to validate these findings and provide criteria for the early assessment of PSMA-RLT, including even more lenient thresholds, as suggested by our explorative retrospective ROC analysis.
Click to Show/Hide
|
||||
| Description |
Patient follow-up was of over 51 months, with the median follow-up (reverse Kaplan-Meier estimator) being 39.1 months (95% CI 32.1-46.1). Median survival was 12.0 (95% CI 10.8-13.2) months, with five patients (19%) still alive at the last follow-up. There were no therapy-related deaths documented. At w16, 14 patients (52%) stated an improvement in pain status from the baseline of at least one tier/level, 11 of which were biochemical responders.
Click to Show/Hide
|
||||
| Experiment 372 Reporting the Activity Data of This PDC | [19] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Pain relief rate |
64%
|
|||
| Patients Enrolled |
25 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | A median of four (iqr: 2-6) cycles every 6-8 weeks | ||||
| Administration Dosage | Mean of 7.7 ± 1.4 GBq/cycle | ||||
| MOA of PDC |
The response to radioligand therapy with 177Lu-PSMA-617 seems to be independent of the presence of early-onset prostate cancer (EOPC); however, the less favorable survival outcome observed in our study may indicate a more aggressive disease course. Expectedly, the safety of LuPSMA-RLT does not seem to be compromised in metastasized castration-resistant EOPC patients. Comparative studies on age at diagnosis of prostate cancer and the patients outcome after LuPSMA-RLT are needed.
Click to Show/Hide
|
||||
| Description |
Intra- or post-therapeutic toxicity was graded according to the CTCAE v5.0 criteria. Newly developing grade ≥ 3 anemia, leukopenia, and thrombocytopenia occurred in three (12%), one (4%), and three (12%) patients, respectively. One patient showed renal toxicity (grade ≥ 3) during follow-up. Pain palliation (>2 level VAS decline) was achieved in 9/14 (64%) and performance status improvement (ECOG level decline ≥ 1) in 8/17 (47%) of patients.
Click to Show/Hide
|
||||
| Experiment 373 Reporting the Activity Data of This PDC | [41] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Pancytopenia |
0.60%
|
|||
| Patients Enrolled |
734 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 5 doses (range: 1 to 6) | ||||
| Administration Dosage | Median cumulative dose 37.5 GBq (range, 7.0 to 48.3) | ||||
| MOA of PDC |
On March 23, 2022, the FDA approved 177Lu-PSMA-617 for the treatment of adult patients with PSMA-positive mCRPC who have been treated with androgen receptor pathway inhibition and taxane-based chemotherapy. The approval was based on a meaningful advantage in overall survival supported by a delay in tumor progression and higher objective response rate. The decision took into account several important factors unique to this applications context. Metastatic castration-resistant prostate cancer (mCRPC) is a life-threatening condition that lacks curative treatment, creating an unmet need. This product provides a novel mechanism of action as the first radioligand therapeutic agent for mCRPC providing anti-tumor effects in both bone and non-bone sites and may provide an opportunity to be combined with other available therapies with different toxicity profiles across mechanistic classes. Finally, 177Lu-PSMA-617 offers a different safety profile than other available systemic therapies which was determined to be acceptable for the indicated patient population, expanding treatment options that can be individualized to a patients preferences and comorbidities.
Click to Show/Hide
|
||||
| Description |
Serious adverse reactions occurred in 36% of patients who received 177Lu-PSMA-617 plus BSoC. Fatal adverse reactions occurred in 2.8% of patients who received 177Lu-PSMA-617 plus BSoC, including sepsis (0.9%), pancytopenia (0.6%), hepatic failure (0.4%), intracranial hemorrhage (0.2%), subdural hematoma (0.2%), ischemic stroke (0.2%), COVID-19 (0.2%), and aspiration pneumonia (0.2%). The 2 fatal adverse reactions of intracranial hemorrhage and subdural hematoma occurred in patients who had concurrent treatment-related thrombocytopenia. The most common adverse reactions (≥ 20%) occurring at a higher incidence in patients who received 177Lu-PSMA-617 plus BSoC were fatigue, dry mouth, nausea, anemia, decreased appetite, and constipation. The most common laboratory abnormalities that worsened from baseline in ≥ 30% of patients who received 177Lu-PSMA-617 plus BSoC were decreased lymphocytes, decreased hemoglobin, decreased leukocytes, decreased platelets, decreased calcium, and decreased sodium.
Click to Show/Hide
|
||||
| Experiment 374 Reporting the Activity Data of This PDC | [68] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Partial biochemical response |
61%
|
|||
| Patients Enrolled |
51 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 2 cycles | ||||
| Administration Dosage | 12.9 GBq (range: 9.1-16.9) | ||||
| MOA of PDC |
68Ga-PSMA-11 PET-derived response assessment based on normalization of tumoral PSMA expression to normal liver tissue (TLR) may be an appropriate biomarker for monitoring 177Lu-PSMA-617 RLT in mCRPC patients and predicting survival outcome (PFS) of this treatment modality. Our study indicates the superiority of using liver-normalized tumor SUV values for molecular response assessment in this setting compared to the use of standard tumor SUV measurements, which are widely practiced at present. However, prospective studies with larger patient cohorts are needed to confirm these initial findings.
Click to Show/Hide
|
||||
| Description |
Thirty-one patients (61%) showed partial biochemical response (PRPSA), 18 patients (35%) stable disease (SDPSA), and two patients (4%) progressive disease (PDPSA). Using molecular-imaging based response assessed by SUVpeak, 37 patients (73%) showed partial response (PRSUV), 12 patients (23%) stable disease (SDSUV), and two patients (4%) progressive disease (PDSUV). Response assessment using TLR gave similar results, with PRTLR in 35 patients (69%), SDTLR in 13 patients (25%), and PDTLR in three patients (6%).
Click to Show/Hide
|
||||
| Experiment 375 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Partial response (PR) |
41.80%
|
|||
| Patients Enrolled |
581 patients with metastatic castration-resistant prostate cancer.
|
||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
The VISION trial was an international open-label phase 3 trial that assigned 581 mCRPC patients who previously received a novel hormonal agent and chemotherapy to either the treatment group (receiving 177Lu-PSMA-617 and standard of care) or control group (standard of care alone). Primary end points were progression-free survival, median overall survival, and median follow-up. Median progression-free survival was 8.7 months in the 177Lu-PSMA-617 group, as compared with 3.4 months in the control group (HR for progression or death, 0.40;99.2% confidence interval, 0.29 to 0.57;P < 0.001). Median overall survival was 15.3 months in the 177Lu-PSMA-617 group, as compared with 11.3 months in the control group (hazard ratio for death, 0.62;95% CI, 0.52 to 0.74;P < 0.001). The median follow-up was 20.3 months (95% CI, 19.8 to 21.0) in the 177Lu-PSMA-617 group and 19.8 months (95% CI, 18.3 to 20.8) in the control group. Secondary end points included median time to the first symptomatic skeletal event or death and PSA level. The median time to the first symptomatic skeletal event or death was 11.5 months in the 177Lu-PSMA-617 group, as compared with 6.8 months in the control group (P < 0.001). The proportions of patients with confirmed decreases in the PSA level of at least 50% and 80% from baseline were higher in the 177Lu-PSMA-617 group than in the control group.
Click to Show/Hide
|
||||
| Experiment 376 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Partial response (PR) |
29%
|
|||
| Patients Enrolled |
14 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | Up to 3 cycles every six weeks | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
A prospective phase II pilot study enrolled fourteen patients with progressive and symptomatic mCRPC despite taxane and novel anti-androgen therapy to receive up to four cycles of 177Lu PSMA-617 every six weeks. Ten out of the 14 patients had a mean PSA reduction of 59%, with five patients having over a 50% reduction, and nine patients having over a 30% reduction in PSA levels. At baseline testing, the PSMA PET SUV predicted a reduction in PSA of more than 30%, with an SUV max value of 17 ± 9 compared to 44 ± 15 (p < 0.007), and a PSMA SUV mean of 6 ± 4 compared to 10 ± 4 (p < 0.04).
Click to Show/Hide
|
||||
| Experiment 377 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Partial response (PR) |
30%
|
|||
| Patients Enrolled |
30 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 4 cycles | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
Another single-arm, single-center, phase 2 trial recruited thirty men with mCRPC and progressive disease after receiving standard treatments including taxane-based chemotherapy and second-generation anti-androgen treatment (abiraterone, enzalutamide, or both). They were administered four cycles of 177Lu-PSMA-617. The primary end points included PSA level, imaging response using bone scan, and PET/CT and quality of life. The PSA decline of greater than or equal to 50% was achieved in 57% of patients. Imaging response using PSMA PET showed a complete response in 10% of patients, a partial response in 30% of patients, and progressive disease in 27% of patients. Cognitive functioning, insomnia, and pain, which were measured using the EORTC-QLQ30 (European Organization for the Research and Treatment of Cancer Quality of Life Questionnaire) and BPI (brief pain inventory) scoring tools showed improvement during treatment compared to baseline, thus indicating improved quality of life.
Click to Show/Hide
|
||||
| Experiment 378 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Partial response (PR) |
53%
|
|||
| Patients Enrolled |
30 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 4 cycles | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
Another single-arm, single-center, phase 2 trial recruited thirty men with mCRPC and progressive disease after receiving standard treatments including taxane-based chemotherapy and second-generation anti-androgen treatment (abiraterone, enzalutamide, or both). They were administered four cycles of 177Lu-PSMA-617. The primary end points included PSA level, imaging response using bone scan, and PET/CT and quality of life. The PSA decline of greater than or equal to 50% was achieved in 57% of patients. Imaging response using PSMA PET showed a complete response in 10% of patients, a partial response in 30% of patients, and progressive disease in 27% of patients. Cognitive functioning, insomnia, and pain, which were measured using the EORTC-QLQ30 (European Organization for the Research and Treatment of Cancer Quality of Life Questionnaire) and BPI (brief pain inventory) scoring tools showed improvement during treatment compared to baseline, thus indicating improved quality of life.
Click to Show/Hide
|
||||
| Experiment 379 Reporting the Activity Data of This PDC | [48] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Partial response (PR) |
4.30%
|
|||
| Patients Enrolled |
Patients with metastatic castration-resistant prostate cancer who underwent 68Ga-PSMA and FDG PET-CT scans.
|
||||
| Evaluation Method | 68Ga-PSMA/18F-FDG PET-CT assay | ||||
| Description |
In the period between 2016 and 2018, 58 patients were referred for [177Lu]-PSMA PRLT to the center, of which 51 patients underwent both [68Ga]-PSMA and FDG PET-CT scans and provisionally qualified for the analysis; out of these complete information of four patients was not available and hence were excluded. Thus, 47 patients were retrospectively recruited and categorized according to the proposed Pro-PET scoring scheme and were analyzed as discussed above. The cohort comprised of heavily pretreated patients with 2 (4.3%) underwent radical prostatectomy; surgical castration was performed in 45 (95.7%) patients; first-line hormonal therapy (with estrogen analogues, leutinizing hormone releasing hormone agonists and antagonists and antiandrogens) in 44 (93.6%) patients, second-line hormonal therapy (with CYP17 blockers and newer anti-androgens) in 34 (72.4%) patients; first-line chemotherapy (with docetaxel) in 33 (70.2%) patients, second-line chemotherapy (with cabazitaxel, oral metronomic chemotherapy, etc.) in 22 (46.8%) and radiotherapy in 26 (55.3%) patients.
Click to Show/Hide
|
||||
| Experiment 380 Reporting the Activity Data of This PDC | [54] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Partial response (PR) |
10%
|
|||
| Patients Enrolled |
10 patients with metastatic castration-resistant prostate cancer and with visceral metastasis.
|
||||
| Administration Time | One cycle | ||||
| Administration Dosage | 4.88 GBq | ||||
| Evaluation Method | Prostate-specific antigen (PSA) response assessment assay | ||||
| MOA of PDC |
Lutetium-177-PSMA was a reasonable palliative treatment option with limited toxicity for these end-stage mCRPC patients with visceral metastasis with adequate PSA stabilization. A synergistic drug amalgamation may be an ideal way to boost the outcome in the future.
|
||||
| Description |
Liver (80%), lung (30%), adrenal (10%), and peritoneum (10%) were the sites of visceral metastasis in our study. On PSA response assessment, 10%, 60%, and 30% of the patients had partial response, stable disease, and progressive disease, respectively. Forty percent of the patients had improvement in the VAS, while 50% had improvement in the AQS score. Median PFS was 24 weeks in our study. A cut-off of 4.88GBq of 177Lu-PSMA was the best-predicted progression with 66.67% sensitivity and 100% specificity on ROC analysis. Thirty percent of the patients showed grade 3 anemia. No other significant toxicity was seen.
Click to Show/Hide
|
||||
| Experiment 381 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Partial response (PR) |
20%
|
|||
| Patients Enrolled |
56 patients with metastatic castration-resistant prostate cancer.
|
||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
Another prospective trial studied 56 patients with progressive mCRPC and rising PSA levels who then received 177Lu-PSMA. Clinical efficacy was assessed using the visual analogue scale for pain, PSA levels, median overall survival, and Gallium-68-labeled prostate-specific membrane antigen (68Ga-PSMA PET/CT) for objective response. There was a decline in PSA of greater than 80% in 23.2% of patients, a decline of greater than 50% in 58.9%, and a decline of greater than 30% in 66.1% of patients. Progressive disease was noted in 10.7% of patients with a rise in PSA level greater than 25%. 68Ga-PSMA PET/CT prior to PSMA radioligand therapy showed the median SUVmax of the target lesion to be 37.5, which decreased to 15.7 after PSMA RLT. Ga-PSMA PET/CT was used to measure response rates which included a partial remission in 56%, stable disease in 8%, and progressive disease in 36% of patients. The median progression-free survival was 13.7 months, and median overall survival was not reached. PET/CT results showing a decrease in SUV max of the target lesion are indicative of a favorable objective response to Lu-PSMA therapy.
Click to Show/Hide
|
||||
| Experiment 382 Reporting the Activity Data of This PDC | [22] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Partial response (PR) |
23%
|
|||
| Patients Enrolled |
90 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 1-7 cycles | ||||
| Administration Dosage | 3.7-8 GBq/cycle | ||||
| Evaluation Method | PET/CT assay | ||||
| MOA of PDC |
The PSMA molecule acts as a target for theranostics in detecting and treating prostatic lesions. This ultimately promotes the concept of precision and personalized medicine. Several published articles showed favorable outcomes of Lu-PSMA-PRLT in mCRPC patients, which quickly translated into routine clinical practices with real effectiveness, a low toxicity profile, and documentation of the risk-benefit of PRLT. Nevertheless, many questions related to PRLT remain unresolved such as the sequencing of PRLT with ARTA or taxane-based chemotherapy, re-challenge therapy, combined therapy, alpha therapy in mCRPC patients, and early treatment of PRLT in mHNPC patients. To solve these questions, several clinical trials are currently under way, and the results of these trials will be helpful in deciding treatment strategies for prostate cancer patients.
Click to Show/Hide
|
||||
| Description |
A favorable response rate (PSA and objective response) and safe profile of 177Lu-PSMA-617 were demonstrated in this study, leading to greater use of Lu-PSMA-PRLT in clinical practices. Similarly, Yadav et al. reported favorable outcomes of 177Lu-PSMA-617 in a prospective, single-arm, single-center study in 90 mCRPC patients.
|
||||
| Experiment 383 Reporting the Activity Data of This PDC | [48] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Partial response (PR) |
23.40%
|
|||
| Patients Enrolled |
Patients with metastatic castration-resistant prostate cancer who underwent 68Ga-PSMA and FDG PET-CT scans.
|
||||
| Evaluation Method | 68Ga-PSMA/18F-FDG PET-CT assay | ||||
| Description |
In the period between 2016 and 2018, 58 patients were referred for [177Lu]-PSMA PRLT to the center, of which 51 patients underwent both [68Ga]-PSMA and FDG PET-CT scans and provisionally qualified for the analysis; out of these complete information of four patients was not available and hence were excluded. Thus, 47 patients were retrospectively recruited and categorized according to the proposed Pro-PET scoring scheme and were analyzed as discussed above. The cohort comprised of heavily pretreated patients with 2 (4.3%) underwent radical prostatectomy; surgical castration was performed in 45 (95.7%) patients; first-line hormonal therapy (with estrogen analogues, leutinizing hormone releasing hormone agonists and antagonists and antiandrogens) in 44 (93.6%) patients, second-line hormonal therapy (with CYP17 blockers and newer anti-androgens) in 34 (72.4%) patients; first-line chemotherapy (with docetaxel) in 33 (70.2%) patients, second-line chemotherapy (with cabazitaxel, oral metronomic chemotherapy, etc.) in 22 (46.8%) and radiotherapy in 26 (55.3%) patients.
Click to Show/Hide
|
||||
| Experiment 384 Reporting the Activity Data of This PDC | [41] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Partial response (PR) |
24%
|
|||
| Patients Enrolled |
319 patients with metastatic castration-resistant prostate cancer who underwent 4 cycles of mean 7.5 GBq Lu-PSMA 617 at 6weeks interval.
|
||||
| Administration Time | Every 6 weeks for up to a total of 6 doses | ||||
| Administration Dosage | 7.4 GBq (200 mCi) | ||||
| MOA of PDC |
On March 23, 2022, the FDA approved 177Lu-PSMA-617 for the treatment of adult patients with PSMA-positive mCRPC who have been treated with androgen receptor pathway inhibition and taxane-based chemotherapy. The approval was based on a meaningful advantage in overall survival supported by a delay in tumor progression and higher objective response rate. The decision took into account several important factors unique to this applications context. Metastatic castration-resistant prostate cancer (mCRPC) is a life-threatening condition that lacks curative treatment, creating an unmet need. This product provides a novel mechanism of action as the first radioligand therapeutic agent for mCRPC providing anti-tumor effects in both bone and non-bone sites and may provide an opportunity to be combined with other available therapies with different toxicity profiles across mechanistic classes. Finally, 177Lu-PSMA-617 offers a different safety profile than other available systemic therapies which was determined to be acceptable for the indicated patient population, expanding treatment options that can be individualized to a patients preferences and comorbidities.
Click to Show/Hide
|
||||
| Description |
The co-primary endpoint of OS was statistically significant, with patients randomized to receive 177Lu-PSMA-617 plus BSoC having prolonged OS (median estimate 15.3 months) compared to BSoC alone (median estimate 11.3 months), hazard ratio (HR) 0.62 (95% CI: 0.52, 0.74, p<0.001). The planned interim OS analysis was not necessary as the targeted number of OS events were observed before the targeted number of rPFS events. Therefore, the final OS analysis was evaluated at the time of rPFS analysis.
Click to Show/Hide
|
||||
| Experiment 385 Reporting the Activity Data of This PDC | [48] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Partial response (PR) |
34.00%
|
|||
| Patients Enrolled |
Patients with metastatic castration-resistant prostate cancer who underwent 68Ga-PSMA and FDG PET-CT scans.
|
||||
| Evaluation Method | 68Ga-PSMA/18F-FDG PET-CT assay | ||||
| Description |
In the period between 2016 and 2018, 58 patients were referred for [177Lu]-PSMA PRLT to the center, of which 51 patients underwent both [68Ga]-PSMA and FDG PET-CT scans and provisionally qualified for the analysis; out of these complete information of four patients was not available and hence were excluded. Thus, 47 patients were retrospectively recruited and categorized according to the proposed Pro-PET scoring scheme and were analyzed as discussed above. The cohort comprised of heavily pretreated patients with 2 (4.3%) underwent radical prostatectomy; surgical castration was performed in 45 (95.7%) patients; first-line hormonal therapy (with estrogen analogues, leutinizing hormone releasing hormone agonists and antagonists and antiandrogens) in 44 (93.6%) patients, second-line hormonal therapy (with CYP17 blockers and newer anti-androgens) in 34 (72.4%) patients; first-line chemotherapy (with docetaxel) in 33 (70.2%) patients, second-line chemotherapy (with cabazitaxel, oral metronomic chemotherapy, etc.) in 22 (46.8%) and radiotherapy in 26 (55.3%) patients.
Click to Show/Hide
|
||||
| Experiment 386 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Partial response (PR) |
35.70%
|
|||
| Patients Enrolled |
50 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | A median of 3 cycles | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
Fifty patients were studied prospectively with PSMA-avid prostate cancer metastases who underwent a median of three cycles (range 1-4) of 177Lu PSMA-617 therapy. Nine were deemed 177Lu PSMA-617 refractory prior to death with a total of twelve deaths in the study. A PSA decline was noted in 23 patients, with 11 patients having a PSA decline of ≥50% after the first cycle of treatment. 12 patients had a PSA decline of <50% ranging from 11.3 to 43.5%. The remaining 23 patients experienced a PSA increase after the first 177Lu PSMA-617 cycle (range 19.7-100%).
Click to Show/Hide
|
||||
| Experiment 387 Reporting the Activity Data of This PDC | [22], [26] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Partial response (PR) |
37.20%
|
|||
| Patients Enrolled |
175 metastatic castration-resistant prostate cancer (mCRPC) patient were included in this meta-analysis. 65 (37.2%) patients experienced partial remission, 67 had stable disease (38.3%), and 43 (24.5%) had progressive disease.
|
||||
| Administration Dosage | 3.7-8.7 GBq/cycle | ||||
| Evaluation Method | PET/CT assay | ||||
| MOA of PDC |
The PSMA molecule acts as a target for theranostics in detecting and treating prostatic lesions. This ultimately promotes the concept of precision and personalized medicine. Several published articles showed favorable outcomes of Lu-PSMA-PRLT in mCRPC patients, which quickly translated into routine clinical practices with real effectiveness, a low toxicity profile, and documentation of the risk-benefit of PRLT. Nevertheless, many questions related to PRLT remain unresolved such as the sequencing of PRLT with ARTA or taxane-based chemotherapy, re-challenge therapy, combined therapy, alpha therapy in mCRPC patients, and early treatment of PRLT in mHNPC patients. To solve these questions, several clinical trials are currently under way, and the results of these trials will be helpful in deciding treatment strategies for prostate cancer patients.
Click to Show/Hide
|
||||
| Description |
Yadav et al. provided a meta-analysis of 177Lu-PSMA-PRLT for treating mCRPC patients. They analyzed 16 articles (13 articles used 177Lu-PSMA-617, 2 articles used 177Lu-PSMA-I&T, and 1 article used both radioligands). The authors showed >50% PSA decline after 177Lu-PSMA-PRLT in 46% of patients. Anatomical imaging response as per the RECIST criteria was reported by eight studies, with a proportion of 37.2% of patients had PR, SD in 38.3% of patients and PD in 24.5% of patients, whereas molecular imaging response as per the PERCIST criteria demonstrated PR in 74 patients (44.3%), SD in 39 patients (23.4%), and PD in 54 patients (32.3%). Common clinical toxicities were grades 1-2, which included anemia (23%), leukopenia (14.2%), thrombocytopenia (15%), nephrotoxicity (9.5%), and xerostomia (14.5%). The authors observed significant heterogeneity in several studies while analyzing this meta-analysis. They concluded that 177Lu-PSMA-PRLT is a promising treatment modality in mCRPC patients who showed PD after standard care treatments.
Click to Show/Hide
|
||||
| Experiment 388 Reporting the Activity Data of This PDC | [48] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Partial response (PR) |
38.30%
|
|||
| Patients Enrolled |
Patients with metastatic castration-resistant prostate cancer who underwent 68Ga-PSMA and FDG PET-CT scans.
|
||||
| Evaluation Method | 68Ga-PSMA/18F-FDG PET-CT assay | ||||
| Description |
In the period between 2016 and 2018, 58 patients were referred for [177Lu]-PSMA PRLT to the center, of which 51 patients underwent both [68Ga]-PSMA and FDG PET-CT scans and provisionally qualified for the analysis; out of these complete information of four patients was not available and hence were excluded. Thus, 47 patients were retrospectively recruited and categorized according to the proposed Pro-PET scoring scheme and were analyzed as discussed above. The cohort comprised of heavily pretreated patients with 2 (4.3%) underwent radical prostatectomy; surgical castration was performed in 45 (95.7%) patients; first-line hormonal therapy (with estrogen analogues, leutinizing hormone releasing hormone agonists and antagonists and antiandrogens) in 44 (93.6%) patients, second-line hormonal therapy (with CYP17 blockers and newer anti-androgens) in 34 (72.4%) patients; first-line chemotherapy (with docetaxel) in 33 (70.2%) patients, second-line chemotherapy (with cabazitaxel, oral metronomic chemotherapy, etc.) in 22 (46.8%) and radiotherapy in 26 (55.3%) patients.
Click to Show/Hide
|
||||
| Experiment 389 Reporting the Activity Data of This PDC | [35] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Partial response (PR) |
39.30%
|
|||
| Administration Time | 12 weeks after the first cycle | ||||
| Administration Dosage | 6.5 ± 1.2 GBq | ||||
| MOA of PDC |
RLT with 177Lu-PSMA-617 can be effectively and safely initiated as early as 8 weeks after failure of 223Ra in patients with progressive bone-metastatic mCRPC refractory to 223Ra. Objective response can be achieved even in patients with more advanced disease and disseminated/diffuse bone metastases, albeit with increasing incidence of significant hematotoxicity.
Click to Show/Hide
|
||||
| Description |
A PSA response (≥50% PSA decline 12 weeks after the first177Lu-PSMA-617 cycle) was observed in 18/28 (64.3%) patients and imaging-based partial remission (PR) was observed in 11/28 (39.3%) patients.
|
||||
| In Vivo Model | 28 men with progressive metastatic castration-resistant prostate cancer who median age 73 years, range 63-89 years). | ||||
| Experiment 390 Reporting the Activity Data of This PDC | [22] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Partial response (PR) |
40%
|
|||
| Patients Enrolled |
30 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 3 cycles | ||||
| Administration Dosage | 3.8-6.7 GBq/cycle | ||||
| Evaluation Method | PET/CT assay | ||||
| MOA of PDC |
The PSMA molecule acts as a target for theranostics in detecting and treating prostatic lesions. This ultimately promotes the concept of precision and personalized medicine. Several published articles showed favorable outcomes of Lu-PSMA-PRLT in mCRPC patients, which quickly translated into routine clinical practices with real effectiveness, a low toxicity profile, and documentation of the risk-benefit of PRLT. Nevertheless, many questions related to PRLT remain unresolved such as the sequencing of PRLT with ARTA or taxane-based chemotherapy, re-challenge therapy, combined therapy, alpha therapy in mCRPC patients, and early treatment of PRLT in mHNPC patients. To solve these questions, several clinical trials are currently under way, and the results of these trials will be helpful in deciding treatment strategies for prostate cancer patients.
Click to Show/Hide
|
||||
| Description |
Yordanova et al., evaluated the response rate and clinical toxicity of re-challenge 177Lu-PSMA-617 in progressive prostatic cancer patients who previously benefited from this therapy. In this retrospective study, a total of 30 patients were re-treated with a median of 3 (range 1-6) cycles of 177Lu-PSMA-617. They found that 75-90% of patients demonstrated favorable serum PSA responses following re-challenge cycles, with a median OS of 12 months after the first re-challenge cycle and without any life-threatening grade-4 adverse event. The authors concluded that the majority of patients benefited from re-challenging 177Lu-PSMA-617 with a longer OS in biochemically responsive patients. At present, data on re-challenge 177Lu-PSMA-617 is limited and requires a prospective randomized trial before a definitive conclusion.
Click to Show/Hide
|
||||
| Experiment 391 Reporting the Activity Data of This PDC | [22] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Partial response (PR) |
45%
|
|||
| Patients Enrolled |
145 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 1-4 cycles | ||||
| Administration Dosage | 2-8 GBq/cycle | ||||
| Evaluation Method | PET/CT assay | ||||
| MOA of PDC |
The PSMA molecule acts as a target for theranostics in detecting and treating prostatic lesions. This ultimately promotes the concept of precision and personalized medicine. Several published articles showed favorable outcomes of Lu-PSMA-PRLT in mCRPC patients, which quickly translated into routine clinical practices with real effectiveness, a low toxicity profile, and documentation of the risk-benefit of PRLT. Nevertheless, many questions related to PRLT remain unresolved such as the sequencing of PRLT with ARTA or taxane-based chemotherapy, re-challenge therapy, combined therapy, alpha therapy in mCRPC patients, and early treatment of PRLT in mHNPC patients. To solve these questions, several clinical trials are currently under way, and the results of these trials will be helpful in deciding treatment strategies for prostate cancer patients.
Click to Show/Hide
|
||||
| Description |
The first major multi-center retrospective study on 177Lu-PSMA-617 was published by Rahbar et al., reporting 145 patients with mCRPC who progressed after second-line systemic therapies. The overall response rate in terms of serum PSA decline >50% was seen in 45% of patients after all 177Lu-PSMA-617 cycles. On imaging, 21 (45%) patients and 13 (28%) patients had PR and SD, respectively. There was grade 3-4 toxicity in 18 patients (13%), which included severe anemia, thrombocytopenia, and leukopenia. They found elevated alkaline phosphatase and visceral metastases as negative predictors of response to 177Lu-PSMA-617. A major drawback of this study was the variable cycles and doses of 177Lu-PSMA-617 given to patients
Click to Show/Hide
|
||||
| Experiment 392 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Partial response (PR) |
56%
|
|||
| Patients Enrolled |
56 patients with metastatic castration-resistant prostate cancer.
|
||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
Another prospective trial studied 56 patients with progressive mCRPC and rising PSA levels who then received 177Lu-PSMA. Clinical efficacy was assessed using the visual analogue scale for pain, PSA levels, median overall survival, and Gallium-68-labeled prostate-specific membrane antigen (68Ga-PSMA PET/CT) for objective response. There was a decline in PSA of greater than 80% in 23.2% of patients, a decline of greater than 50% in 58.9%, and a decline of greater than 30% in 66.1% of patients. Progressive disease was noted in 10.7% of patients with a rise in PSA level greater than 25%. 68Ga-PSMA PET/CT prior to PSMA radioligand therapy showed the median SUVmax of the target lesion to be 37.5, which decreased to 15.7 after PSMA RLT. Ga-PSMA PET/CT was used to measure response rates which included a partial remission in 56%, stable disease in 8%, and progressive disease in 36% of patients. The median progression-free survival was 13.7 months, and median overall survival was not reached. PET/CT results showing a decrease in SUV max of the target lesion are indicative of a favorable objective response to Lu-PSMA therapy.
Click to Show/Hide
|
||||
| Experiment 393 Reporting the Activity Data of This PDC | [68] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Partial response (PR) |
69%
|
|||
| Patients Enrolled |
51 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 2 cycles | ||||
| Administration Dosage | 12.9 GBq (range: 9.1-16.9) | ||||
| Evaluation Method | TLR gave similar results assay | ||||
| MOA of PDC |
68Ga-PSMA-11 PET-derived response assessment based on normalization of tumoral PSMA expression to normal liver tissue (TLR) may be an appropriate biomarker for monitoring 177Lu-PSMA-617 RLT in mCRPC patients and predicting survival outcome (PFS) of this treatment modality. Our study indicates the superiority of using liver-normalized tumor SUV values for molecular response assessment in this setting compared to the use of standard tumor SUV measurements, which are widely practiced at present. However, prospective studies with larger patient cohorts are needed to confirm these initial findings.
Click to Show/Hide
|
||||
| Description |
Thirty-one patients (61%) showed partial biochemical response (PRPSA), 18 patients (35%) stable disease (SDPSA), and two patients (4%) progressive disease (PDPSA). Using molecular-imaging based response assessed by SUVpeak, 37 patients (73%) showed partial response (PRSUV), 12 patients (23%) stable disease (SDSUV), and two patients (4%) progressive disease (PDSUV). Response assessment using TLR gave similar results, with PRTLR in 35 patients (69%), SDTLR in 13 patients (25%), and PDTLR in three patients (6%).
Click to Show/Hide
|
||||
| Experiment 394 Reporting the Activity Data of This PDC | [68] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Partial response (PR) |
73%
|
|||
| Patients Enrolled |
51 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 2 cycles | ||||
| Administration Dosage | 12.9 GBq (range: 9.1-16.9) | ||||
| Evaluation Method | Molecular-imaging based response assessed by SUVpeak | ||||
| MOA of PDC |
68Ga-PSMA-11 PET-derived response assessment based on normalization of tumoral PSMA expression to normal liver tissue (TLR) may be an appropriate biomarker for monitoring 177Lu-PSMA-617 RLT in mCRPC patients and predicting survival outcome (PFS) of this treatment modality. Our study indicates the superiority of using liver-normalized tumor SUV values for molecular response assessment in this setting compared to the use of standard tumor SUV measurements, which are widely practiced at present. However, prospective studies with larger patient cohorts are needed to confirm these initial findings.
Click to Show/Hide
|
||||
| Description |
Thirty-one patients (61%) showed partial biochemical response (PRPSA), 18 patients (35%) stable disease (SDPSA), and two patients (4%) progressive disease (PDPSA). Using molecular-imaging based response assessed by SUVpeak, 37 patients (73%) showed partial response (PRSUV), 12 patients (23%) stable disease (SDSUV), and two patients (4%) progressive disease (PDSUV). Response assessment using TLR gave similar results, with PRTLR in 35 patients (69%), SDTLR in 13 patients (25%), and PDTLR in three patients (6%).
Click to Show/Hide
|
||||
| Experiment 395 Reporting the Activity Data of This PDC | [52] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Partial response (PR) |
84%
|
|||
| Patients Enrolled |
19 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 5 (iqr: 3-6) cycles | ||||
| Administration Dosage | A cumulative activity of 32 ± 11 GBq | ||||
| Evaluation Method | 68Ga-PSMA-11 PET/CT assay | ||||
| MOA of PDC |
Intermittent 177Lu-PSMA-617 radioligand therapy in early responders with oligometastatic castration-resistant prostate cancer seems to not compromise survival outcome, despite long treatment-free intervals. The safety profile remained favorable, warranting further investigation of the concept of intermittent treatment in selected patients with a longer life-expectancy.
Click to Show/Hide
|
||||
| Description |
Four (21%) patients showed no response (PD) to the 177Lu-PSMA-RLT cycles after the first treatment break, and in two patients (11%), progression after the initial disease stabilization (SD) under subsequent cycles led to treatment discontinuation. Two patients (11%) completed the intended six cycles with a stable disease. In the remaining 11/19 (84%) patients, resuming 177Lu-PSMA-RLT resulted in a repeated PR. Altogether, 14/19 (74%) patients died by the time of this analysis. The median PFS was 27 (95% CI: 23-31) months and the OS was 45 (95% CI: 28-62) months.
Click to Show/Hide
|
||||
| Experiment 396 Reporting the Activity Data of This PDC | [41] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Platelets decrease rate | ≥ 30% | |||
| Patients Enrolled |
734 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 5 doses (range: 1 to 6) | ||||
| Administration Dosage | Median cumulative dose 37.5 GBq (range, 7.0 to 48.3) | ||||
| MOA of PDC |
On March 23, 2022, the FDA approved 177Lu-PSMA-617 for the treatment of adult patients with PSMA-positive mCRPC who have been treated with androgen receptor pathway inhibition and taxane-based chemotherapy. The approval was based on a meaningful advantage in overall survival supported by a delay in tumor progression and higher objective response rate. The decision took into account several important factors unique to this applications context. Metastatic castration-resistant prostate cancer (mCRPC) is a life-threatening condition that lacks curative treatment, creating an unmet need. This product provides a novel mechanism of action as the first radioligand therapeutic agent for mCRPC providing anti-tumor effects in both bone and non-bone sites and may provide an opportunity to be combined with other available therapies with different toxicity profiles across mechanistic classes. Finally, 177Lu-PSMA-617 offers a different safety profile than other available systemic therapies which was determined to be acceptable for the indicated patient population, expanding treatment options that can be individualized to a patients preferences and comorbidities.
Click to Show/Hide
|
||||
| Description |
Serious adverse reactions occurred in 36% of patients who received 177Lu-PSMA-617 plus BSoC. Fatal adverse reactions occurred in 2.8% of patients who received 177Lu-PSMA-617 plus BSoC, including sepsis (0.9%), pancytopenia (0.6%), hepatic failure (0.4%), intracranial hemorrhage (0.2%), subdural hematoma (0.2%), ischemic stroke (0.2%), COVID-19 (0.2%), and aspiration pneumonia (0.2%). The 2 fatal adverse reactions of intracranial hemorrhage and subdural hematoma occurred in patients who had concurrent treatment-related thrombocytopenia. The most common adverse reactions (≥ 20%) occurring at a higher incidence in patients who received 177Lu-PSMA-617 plus BSoC were fatigue, dry mouth, nausea, anemia, decreased appetite, and constipation. The most common laboratory abnormalities that worsened from baseline in ≥ 30% of patients who received 177Lu-PSMA-617 plus BSoC were decreased lymphocytes, decreased hemoglobin, decreased leukocytes, decreased platelets, decreased calcium, and decreased sodium.
Click to Show/Hide
|
||||
| Experiment 397 Reporting the Activity Data of This PDC | [48] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Progression rate |
59.60%
|
|||
| Patients Enrolled |
Patients with metastatic castration-resistant prostate cancer who underwent 68Ga-PSMA and FDG PET-CT scans.
|
||||
| Evaluation Method | 68Ga-PSMA/18F-FDG PET-CT assay | ||||
| Description |
In the period between 2016 and 2018, 58 patients were referred for [177Lu]-PSMA PRLT to the center, of which 51 patients underwent both [68Ga]-PSMA and FDG PET-CT scans and provisionally qualified for the analysis; out of these complete information of four patients was not available and hence were excluded. Thus, 47 patients were retrospectively recruited and categorized according to the proposed Pro-PET scoring scheme and were analyzed as discussed above. The cohort comprised of heavily pretreated patients with 2 (4.3%) underwent radical prostatectomy; surgical castration was performed in 45 (95.7%) patients; first-line hormonal therapy (with estrogen analogues, leutinizing hormone releasing hormone agonists and antagonists and antiandrogens) in 44 (93.6%) patients, second-line hormonal therapy (with CYP17 blockers and newer anti-androgens) in 34 (72.4%) patients; first-line chemotherapy (with docetaxel) in 33 (70.2%) patients, second-line chemotherapy (with cabazitaxel, oral metronomic chemotherapy, etc.) in 22 (46.8%) and radiotherapy in 26 (55.3%) patients.
Click to Show/Hide
|
||||
| Experiment 398 Reporting the Activity Data of This PDC | [55], [56] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Progression-free survival (PFS) |
8.7 months
|
|||
| Patients Enrolled |
Of the 1003 patients who underwent scanning, 831 (82.9%) were judged to have met all the trial eligibility criteria, including the PSMA imaging criteria, and were randomly assigned, between June 4, 2018, and October 23, 2019, to receive either <sup>177</sup>Lu-PSMA-617 plus protocol-permitted standard care (551 patients) or standard care alone (280).
Click to Show/Hide
|
||||
| Evaluation Method | PET/CT assay | ||||
| MOA of PDC |
Prostate-specific membrane antigen (PSMA)-targeted radiopharmaceutical like 177Lu-PSMA-617, a beta particle emitter has demonstrated improvement in overall survival in mCRPC patients pretreated with ARAT or taxanes. Although immune checkpoint inhibitors are being tested in mCRPC, there is no robust evidence to support this premise.
|
||||
| Description |
In an international phase III randomized controlled trial (VISION), men with PSMA positive mCRPC, previously treated with at least one ARAT and one or two taxane regimens, were randomly assigned in a 2 : 1 ratio to either 177Lu-PSMA-617 for four to six cycles and protocol-permitted standard of care vs. standard of care therapy alone. The addition of Lu-PSMA-617 to a standard of care therapy improved the imaging-based PFS (8.7 vs. 3.4 months, hazard ratio: 0.40, 99% CI, 0.29-0.57) and OS (15.3 vs. 11.3 months, hazard ratio: 0.62, 95% CI: 0.52-0.74).
Click to Show/Hide
|
||||
| Related Clinical Trial | |||||
| NCT Number | NCT03511664 | Clinical Status | Phase 3 | ||
| Experiment 399 Reporting the Activity Data of This PDC | [47] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Progression-free survival (PFS) |
6.6 months
|
|||
| Patients Enrolled |
40 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | Once every 6-8 weeks, for a maximum of four to six cycles | ||||
| Administration Dosage | 6.0-8.5 GBq | ||||
| Evaluation Method | 68Ga-PSMA-11 PET/CT assay | ||||
| MOA of PDC |
Also, previously identified risk factors in mCRPC, such as lactate dehydrogenase or albumin, were not available or were not collected systematically and consequently not tested in the models. Similarly, 2-[18F]FDG-PET was available only in a minority of patients in this study and thus could not be tested in the models. Dual-tracer PET imaging with [68Ga]Ga-PSMA-11 and 2-[18F]FDG-PET can improve patient selection for 177Lu-PSMA therapy; however, several steps are required to establish 2-[18F]FDG-PET as a screening tool for 177Lu-PSMA in practice (ie, confirmation of its prognostic value in a multicentre setting, standardisation of image interpretation, inclusion in drug label and guidelines, and insurance coverage).
Click to Show/Hide
|
||||
| Description |
The C-index of the overall survival model was 071 (95% CI 069-073). Similar C-indices were achieved at internal validation (071 [069-073]) and external validation (072 [068-076]). The C-index of the PSA-progression-free survival model was 070 (95% CI 068-072). Similar C-indices were achieved at internal validation (070 [068-072]) and external validation (071 [068-074]). Both models were adequately calibrated and their predictions correlated with the observed outcome. Compared with high-risk patients, low-risk patients had significantly longer overall survival in the validation cohort (249 months [95% CI 168-273] vs 74 months [40-108]; p<00001) and PSA-progression-free survival (66 months [60-71] vs 25 months [12-38]; p=0022).
Click to Show/Hide
|
||||
| Related Clinical Trial | |||||
| NCT Number | NCT03042312 | Clinical Status | Phase 2 | ||
| Clinical Description | This was an open-label, multicenter, prospective trial to assess safety and efficacy of 177Lu-PSMA-617 in patients with metastatic castration resistant prostate cancer. | ||||
| Experiment 400 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Progression-free survival (PFS) |
8.7 months
|
|||
| Patients Enrolled |
581 patients with metastatic castration-resistant prostate cancer.
|
||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
The VISION trial was an international open-label phase 3 trial that assigned 581 mCRPC patients who previously received a novel hormonal agent and chemotherapy to either the treatment group (receiving 177Lu-PSMA-617 and standard of care) or control group (standard of care alone). Primary end points were progression-free survival, median overall survival, and median follow-up. Median progression-free survival was 8.7 months in the 177Lu-PSMA-617 group, as compared with 3.4 months in the control group (HR for progression or death, 0.40; 99.2% confidence interval, 0.29 to 0.57; P < 0.001). Median overall survival was 15.3 months in the 177Lu-PSMA-617 group, as compared with 11.3 months in the control group (hazard ratio for death, 0.62; 95% CI, 0.52 to 0.74; P < 0.001). The median follow-up was 20.3 months (95% CI, 19.8 to 21.0) in the 177Lu-PSMA-617 group and 19.8 months (95% CI, 18.3 to 20.8) in the control group. Secondary end points included median time to the first symptomatic skeletal event or death and PSA level. The median time to the first symptomatic skeletal event or death was 11.5 months in the 177Lu-PSMA-617 group, as compared with 6.8 months in the control group (P < 0.001). The proportions of patients with confirmed decreases in the PSA level of at least 50% and 80% from baseline were higher in the 177Lu-PSMA-617 group than in the control group.
Click to Show/Hide
|
||||
| Experiment 401 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Progression-free survival (PFS) |
4 months
|
|||
| Patients Enrolled |
35 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | Up to 4 cycles every 8 weeks | ||||
| Administration Dosage | 6.0-7.4 GBq/cycle | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
A randomized, parallel group, open label, and non-inferiority phase II trial conducted between 2019 and 2021 studied a group of thirty five chemo-naive patients with mCPRC and high expressing PSMA lesions on 68Ga-PSMA-11 on PET/CT. Patients were randomized in 1:1 ratio to either 177Lu PSMA-617 (6.0-7.4 GBq/cycle, every 8 weeks, up to 4 cycles) or docetaxel (75 mg/m2/cycle, every 3 weeks, for up to 10 cycles), with fifteen and twenty patients in each group, respectively. The primary endpoint was best PSA response rate (PSA-RR), which is defined as a ≥ 50% decline in PSA from baseline. The 177Lu PSMA-617 arm PSA-RR was 60% versus 40% in docetaxel group with a difference in PSA-RR of 20% (95% CI: 1-47, p = 0.025) and met the pre-specified criterion for non-inferiority which was defined as margin of 15% decline in PSA-RR. The PFS rate for 177Lu PSMA-617 was 30% versus 20% for docetaxel (95% CI: 18-38, p = 0.5). The number of treatment-related adverse events grade 3 or higher occurred less in the 177Lu PSMA-617 arm than the docetaxel arm (30% versus 50% respectively, p = 0.2).
Click to Show/Hide
|
||||
| Experiment 402 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Progression-free survival (PFS) |
7.5 months
|
|||
| Patients Enrolled |
40 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | Up to 4 cycles (median number of 3 cycles, range 2-5) every eight to twelve weeks | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
A phase II study followed forty patients with PET/CT-68Ga-PSMA positive mCRPC treated with 177Lu PSMA-617. 177Lu PSMA-617 was given for up to four cycles (median number of three cycles, range 2-5) every eight to twelve weeks. With a median follow-up of 15.5 months (range 6-22 ), 37.5% of patients had a greater than 50% PSA decline and 50% had a PSA decline greater than 30%. The median PFS was 7.5 months (95% CI: 4.8-10.5) and median OS was 12.4 months (95% CI 7.4-20.3 months).
Click to Show/Hide
|
||||
| Experiment 403 Reporting the Activity Data of This PDC | [22], [23] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Progression-free survival (PFS) |
8.7 months
|
|||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
The Thera-P trial was a phase II prospective multicenter trial looking at those with mCPRC who progressed after docetaxel chemotherapy and were randomly assigned to 177Lu PSMA-617 or cabazitaxel. Initial reported results found that those who were treated with 177Lu PSMA-617 treatment led to improvement in PSA response rate (66% vs 37%), RECIST response rate (49% vs 24%), PFS (HR 0.63), less G3-G4 toxicities (33% vs 53%), and overall better patient reported outcomes.
Click to Show/Hide
|
||||
| In Vivo Model | Patients with progressive metastatic castration-resistant prostate cancer. | ||||
| Experiment 404 Reporting the Activity Data of This PDC | [11] | ||||
| Indication | ATM-mutated metastatic castration resistant prostate cancer | ||||
| Efficacy Data | Progression-free survival (PFS) |
3-13.7 months
|
|||
| Patients Enrolled |
Metastatic castration-resistant prostate cancer patients.
|
||||
| Administration Time | 4-6 cycles at 6-12 weekly intervals | ||||
| Administration Dosage | 2-8 GBq | ||||
| MOA of PDC |
177Lu-PSMA therapy is a promising treatment alternative in patients with mCRPC, with good clinical efficacy, even in heavily pretreated patients with multiple lines of systemic therapy. Additionally, the available data regarding 177Lu-PSMA therapy revealed that this type of therapy is safe, with a low toxicity profile. There is also some preliminary evidence that 177Lu-PSMA therapy is more effective, if used prior to other systemic therapies, earlier during the disease course. Consequently, this treatment alternative may shift its place from the last treatment step of mCRPC to one of the initial therapy steps for PCa, probably combined with other systemic treatment options in the future.
Click to Show/Hide
|
||||
| Description |
Although there are some different approaches regarding the use of 177Lu-PSMA therapy in different countries, this type of therapy is generally safe, with a low toxicity profile. From the oncological point of view, a PSA (prostate specific antigen) decline of ≥50% was seen in 10.6-69% of patients with mCRPC; whereas progression-free survival (PFS) was reported to be 3-13.7 months in different studies.
Click to Show/Hide
|
||||
| Experiment 405 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Progression-free survival (PFS) |
4 months
|
|||
| Patients Enrolled |
191 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 1-5 cycles | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
A real-world study evaluated 191 patients with mCPRC treated with 177Lu-PSMA-617. Patients had confirmation of PSMA expressing lesions by 68Ga-PSMA-ligand PET/CT. The majority of individuals (90%) had first- and second-line systemic treatment prior to being treated with 177Lu-PSMA-617. Patients received one to five cycles of treatment and specific endpoints included biochemical response, radiologic response, PSA PFS, and OS. A PSA RR (defined as a decline of ≥50% in PSA) was found in 56% of patients, and any PSA decline occurred in 75% of patients. The median radiographic progression-free survival was found to be six months (range 3-10), PSA PFS (n = 132) was 4 months (range 3-8), and the overall survival (n = 191) was 12 months (range 5-18).
Click to Show/Hide
|
||||
| Experiment 406 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Progression-free survival (PFS) |
5.5 months
|
|||
| Patients Enrolled |
254 patients with metastatic castration-resistant prostate cancer.
|
||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
The REALITY (REgistry to Assess Outcome and Toxicity of Targeted RadionucLIde TherapY) study was a prospective real world cohort of 254 patients with mCRPC who received 177Lu-PSMA-617 as experimental salvage therapy after conventional treatments had failed. The primary end points were efficacy, reflected by PSA-PFS, (prostate specific antigen-progression-free survival) OS, (overall survival) and safety which was reflected by the incidence of treatment-related (AEs). Over the entire course of 177Lu-PSMA-617 RLT (radioligand therapy), 52.0% patients had a greater than 50% decline in their PSA response. At a median (minimum - maximum) follow-up of 14.9 (5.0-64.4) months, the median PSA-PFS was 5.5 (4.4-6.6) months, while the median OS was 14.5 (11.5-17.5) months.
Click to Show/Hide
|
||||
| Experiment 407 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Progression-free survival (PFS) |
6 months
|
|||
| Patients Enrolled |
191 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 1-5 cycles | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
A real-world study evaluated 191 patients with mCPRC treated with 177Lu-PSMA-617. Patients had confirmation of PSMA expressing lesions by 68Ga-PSMA-ligand PET/CT. The majority of individuals (90%) had first- and second-line systemic treatment prior to being treated with 177Lu-PSMA-617. Patients received one to five cycles of treatment and specific endpoints included biochemical response, radiologic response, PSA PFS, and OS. A PSA RR (defined as a decline of ≥50% in PSA) was found in 56% of patients, and any PSA decline occurred in 75% of patients. The median radiographic progression-free survival was found to be six months (range 3-10), PSA PFS (n = 132) was 4 months (range 3-8), and the overall survival (n = 191) was 12 months (range 5-18).
Click to Show/Hide
|
||||
| Experiment 408 Reporting the Activity Data of This PDC | [18] | ||||
| Indication | ATM-mutated metastatic castration resistant prostate cancer | ||||
| Efficacy Data | Progression-free survival (PFS) |
6.9 months
|
|||
| Patients Enrolled |
50 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 4 cycles | ||||
| Administration Dosage | Median 7.4 GBq | ||||
| MOA of PDC |
PSMA TRT involves conjugating radionuclides to antibodies and small molecule-ligands directed against PSMA. The most common radionuclide utilized to date is Lutetium-177, a beta-emitter with a mean path-length of 0.7 mm and maximum of 1.8 mm. Gamma-ray emission allows for concurrent single photon emission computed tomography (SPECT). Actinium-225 has been the most common alpha-emitter utilized. Alpha-emitters are thousands of times more potent and can induce double-stranded DNA breaks more difficult to repair, but mean path-length is much shorter than beta-emitters (under 0.01 mm).
Click to Show/Hide
|
||||
| Experiment 409 Reporting the Activity Data of This PDC | [16] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Progression-free survival (PFS) |
9.5 months
|
|||
| Patients Enrolled |
Patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | Every 6weeks | ||||
| Administration Dosage | 7.5 GBq | ||||
| Description |
There was no significant difference comparing the rate of > 50% PSA decline or best PSA response between the 6.0 GBq and 7.5 GBq group (35% vs. 54%, p = 0.065; and - 40.2% vs. - 57.8%, p = 0.329). The median estimated survival and PSA-PFS did not significantly differ between the 6.0 GBq and 7.5 GBq groups as well (11.3 vs. 12.7 months, p = 0.384; and 9.5 vs. 12.3 months, p = 0.258).
Click to Show/Hide
|
||||
| Experiment 410 Reporting the Activity Data of This PDC | [16] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Progression-free survival (PFS) |
12.3 months
|
|||
| Patients Enrolled |
Patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | Every 8weeks | ||||
| Administration Dosage | 6.0 GBq | ||||
| Description |
There was no significant difference comparing the rate of > 50% PSA decline or best PSA response between the 6.0 GBq and 7.5 GBq group (35% vs. 54%, p = 0.065; and - 40.2% vs. - 57.8%, p = 0.329). The median estimated survival and PSA-PFS did not significantly differ between the 6.0 GBq and 7.5 GBq groups as well (11.3 vs. 12.7 months, p = 0.384; and 9.5 vs. 12.3 months, p = 0.258).
Click to Show/Hide
|
||||
| Experiment 411 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Progression-free survival (PFS) |
13.7 months
|
|||
| Patients Enrolled |
56 patients with metastatic castration-resistant prostate cancer.
|
||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
Another prospective trial studied 56 patients with progressive mCRPC and rising PSA levels who then received 177Lu-PSMA. Clinical efficacy was assessed using the visual analogue scale for pain, PSA levels, median overall survival, and Gallium-68-labeled prostate-specific membrane antigen (68Ga-PSMA PET/CT) for objective response. There was a decline in PSA of greater than 80% in 23.2% of patients, a decline of greater than 50% in 58.9%, and a decline of greater than 30% in 66.1% of patients. Progressive disease was noted in 10.7% of patients with a rise in PSA level greater than 25%. 68Ga-PSMA PET/CT prior to PSMA radioligand therapy showed the median SUVmax of the target lesion to be 37.5, which decreased to 15.7 after PSMA RLT. Ga-PSMA PET/CT was used to measure response rates which included a partial remission in 56%, stable disease in 8%, and progressive disease in 36% of patients. The median progression-free survival was 13.7 months, and median overall survival was not reached. PET/CT results showing a decrease in SUV max of the target lesion are indicative of a favorable objective response to Lu-PSMA therapy.
Click to Show/Hide
|
||||
| Experiment 412 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Progression-free survival (PFS) |
20 weeks
|
|||
| Patients Enrolled |
43 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | Every six to twelve weeks | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
A single center retrospective study reviewed 43 mCRPC patients with a median age of 71 (range 51-88) and 177Lu-PSMA-617 treatments every six to twelve weeks. A total of 112 cycles of RLT were conducted with a median of three cycles (range 1-6). Endpoints included PSA response, toxicity, median OS, and median PSA PFS. A PSA decline of greater than 90% was seen in 23% of patients, while a decline of greater than 50% was seen in 65% of patients. A median OS was 52 weeks, while a PSA PFS was found to be 20 weeks.
Click to Show/Hide
|
||||
| Experiment 413 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Progressive Disease (PD) |
27%
|
|||
| Patients Enrolled |
30 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 4 cycles | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
Another single-arm, single-center, phase 2 trial recruited thirty men with mCRPC and progressive disease after receiving standard treatments including taxane-based chemotherapy and second-generation anti-androgen treatment (abiraterone, enzalutamide, or both). They were administered four cycles of 177Lu-PSMA-617. The primary end points included PSA level, imaging response using bone scan, and PET/CT and quality of life. The PSA decline of greater than or equal to 50% was achieved in 57% of patients. Imaging response using PSMA PET showed a complete response in 10% of patients, a partial response in 30% of patients, and progressive disease in 27% of patients. Cognitive functioning, insomnia, and pain, which were measured using the EORTC-QLQ30 (European Organization for the Research and Treatment of Cancer Quality of Life Questionnaire) and BPI (brief pain inventory) scoring tools showed improvement during treatment compared to baseline, thus indicating improved quality of life.
Click to Show/Hide
|
||||
| Experiment 414 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Progressive Disease (PD) |
29%
|
|||
| Patients Enrolled |
14 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | Up to 3 cycles every six weeks | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
A prospective phase II pilot study enrolled fourteen patients with progressive and symptomatic mCRPC despite taxane and novel anti-androgen therapy to receive up to four cycles of 177Lu PSMA-617 every six weeks. Ten out of the 14 patients had a mean PSA reduction of 59%, with five patients having over a 50% reduction, and nine patients having over a 30% reduction in PSA levels. At baseline testing, the PSMA PET SUV predicted a reduction in PSA of more than 30%, with an SUV max value of 17 ± 9 compared to 44 ± 15 (p < 0.007), and a PSMA SUV mean of 6 ± 4 compared to 10 ± 4 (p < 0.04).
Click to Show/Hide
|
||||
| Experiment 415 Reporting the Activity Data of This PDC | [68] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Progressive Disease (PD) |
4%
|
|||
| Patients Enrolled |
51 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 2 cycles | ||||
| Administration Dosage | 12.9 GBq (range: 9.1-16.9) | ||||
| Evaluation Method | Molecular-imaging based response assessed by SUVpeak | ||||
| MOA of PDC |
68Ga-PSMA-11 PET-derived response assessment based on normalization of tumoral PSMA expression to normal liver tissue (TLR) may be an appropriate biomarker for monitoring 177Lu-PSMA-617 RLT in mCRPC patients and predicting survival outcome (PFS) of this treatment modality. Our study indicates the superiority of using liver-normalized tumor SUV values for molecular response assessment in this setting compared to the use of standard tumor SUV measurements, which are widely practiced at present. However, prospective studies with larger patient cohorts are needed to confirm these initial findings.
Click to Show/Hide
|
||||
| Description |
Thirty-one patients (61%) showed partial biochemical response (PRPSA), 18 patients (35%) stable disease (SDPSA), and two patients (4%) progressive disease (PDPSA). Using molecular-imaging based response assessed by SUVpeak, 37 patients (73%) showed partial response (PRSUV), 12 patients (23%) stable disease (SDSUV), and two patients (4%) progressive disease (PDSUV). Response assessment using TLR gave similar results, with PRTLR in 35 patients (69%), SDTLR in 13 patients (25%), and PDTLR in three patients (6%).
Click to Show/Hide
|
||||
| Experiment 416 Reporting the Activity Data of This PDC | [68] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Progressive Disease (PD) |
6%
|
|||
| Patients Enrolled |
51 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 2 cycles | ||||
| Administration Dosage | 12.9 GBq (range: 9.1-16.9) | ||||
| Evaluation Method | TLR gave similar results assay | ||||
| MOA of PDC |
68Ga-PSMA-11 PET-derived response assessment based on normalization of tumoral PSMA expression to normal liver tissue (TLR) may be an appropriate biomarker for monitoring 177Lu-PSMA-617 RLT in mCRPC patients and predicting survival outcome (PFS) of this treatment modality. Our study indicates the superiority of using liver-normalized tumor SUV values for molecular response assessment in this setting compared to the use of standard tumor SUV measurements, which are widely practiced at present. However, prospective studies with larger patient cohorts are needed to confirm these initial findings.
Click to Show/Hide
|
||||
| Description |
Thirty-one patients (61%) showed partial biochemical response (PRPSA), 18 patients (35%) stable disease (SDPSA), and two patients (4%) progressive disease (PDPSA). Using molecular-imaging based response assessed by SUVpeak, 37 patients (73%) showed partial response (PRSUV), 12 patients (23%) stable disease (SDSUV), and two patients (4%) progressive disease (PDSUV). Response assessment using TLR gave similar results, with PRTLR in 35 patients (69%), SDTLR in 13 patients (25%), and PDTLR in three patients (6%).
Click to Show/Hide
|
||||
| Experiment 417 Reporting the Activity Data of This PDC | [52] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Progressive Disease (PD) |
11%
|
|||
| Patients Enrolled |
19 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 5 (iqr: 3-6) cycles | ||||
| Administration Dosage | A cumulative activity of 32 ± 11 GBq | ||||
| Evaluation Method | 68Ga-PSMA-11 PET/CT assay | ||||
| MOA of PDC |
Intermittent 177Lu-PSMA-617 radioligand therapy in early responders with oligometastatic castration-resistant prostate cancer seems to not compromise survival outcome, despite long treatment-free intervals. The safety profile remained favorable, warranting further investigation of the concept of intermittent treatment in selected patients with a longer life-expectancy.
Click to Show/Hide
|
||||
| Description |
Four (21%) patients showed no response (PD) to the 177Lu-PSMA-RLT cycles after the first treatment break, and in two patients (11%), progression after the initial disease stabilization (SD) under subsequent cycles led to treatment discontinuation. Two patients (11%) completed the intended six cycles with a stable disease. In the remaining 11/19 (84%) patients, resuming 177Lu-PSMA-RLT resulted in a repeated PR. Altogether, 14/19 (74%) patients died by the time of this analysis. The median PFS was 27 (95% CI: 23-31) months and the OS was 45 (95% CI: 28-62) months.
Click to Show/Hide
|
||||
| Experiment 418 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Progressive Disease (PD) |
13%
|
|||
| Patients Enrolled |
36 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 2 cycles | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
A retrospective single center study looked at therapeutic outcomes of 177Lu-PSMA-617 in mCRPC based on post-treatment imaging findings. 36 patients (aged 67 ± 8.8 years) were included out of which 23 received 2 cycles of treatment. Eleven patients (47.8%) were considered responsive in the post-therapeutic scans by 177Lu-PSMA-617, two of which experienced complete response. Nine (39.1%) patients had stable disease while three (13%) experienced disease progression.
Click to Show/Hide
|
||||
| Experiment 419 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Progressive Disease (PD) |
19%
|
|||
| Patients Enrolled |
21 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | Every 8 weeks | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
Another real-world prospective cohort study included twenty-one treatments refractory mCRPC patients at Bushehr Department of Nuclear Medicine between December 2016 to December 2018 treated with 177Lu-PSMA-617 every 8 weeks. Patients had to have PSMA secreting lesions detected by PSMA imaging with 68Ga-PSMA PET or 177Lu/99Tc-PSMA before to undergoing treatment. The mean age of patients was 70.3 ± 9.6 (range 54-88) with a median of two cycles of treatment (range 1-4). The primary endpoint of the study was to assess biochemical response (BCR), which was defined as a drop in the PSA of more than 50. Additional secondary endpoints included response by ECOG and overall survival. A BCR was seen in 62% of patients. The estimated overall survival was seen to be 62.69 weeks (95% confidence interval: 42.06-83.33) with a median follow-up period of 9 months (range 1-25 months).
Click to Show/Hide
|
||||
| Experiment 420 Reporting the Activity Data of This PDC | [22] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Progressive Disease (PD) |
23%
|
|||
| Patients Enrolled |
90 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 1-7 cycles | ||||
| Administration Dosage | 3.7-8 GBq/cycle | ||||
| Evaluation Method | PET/CT assay | ||||
| MOA of PDC |
The PSMA molecule acts as a target for theranostics in detecting and treating prostatic lesions. This ultimately promotes the concept of precision and personalized medicine. Several published articles showed favorable outcomes of Lu-PSMA-PRLT in mCRPC patients, which quickly translated into routine clinical practices with real effectiveness, a low toxicity profile, and documentation of the risk-benefit of PRLT. Nevertheless, many questions related to PRLT remain unresolved such as the sequencing of PRLT with ARTA or taxane-based chemotherapy, re-challenge therapy, combined therapy, alpha therapy in mCRPC patients, and early treatment of PRLT in mHNPC patients. To solve these questions, several clinical trials are currently under way, and the results of these trials will be helpful in deciding treatment strategies for prostate cancer patients.
Click to Show/Hide
|
||||
| Description |
A favorable response rate (PSA and objective response) and safe profile of 177Lu-PSMA-617 were demonstrated in this study, leading to greater use of Lu-PSMA-PRLT in clinical practices. Similarly, Yadav et al. reported favorable outcomes of 177Lu-PSMA-617 in a prospective, single-arm, single-center study in 90 mCRPC patients.
|
||||
| Experiment 421 Reporting the Activity Data of This PDC | [48] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Progressive Disease (PD) |
23.40%
|
|||
| Patients Enrolled |
Patients with metastatic castration-resistant prostate cancer who underwent 68Ga-PSMA and FDG PET-CT scans.
|
||||
| Evaluation Method | 68Ga-PSMA/18F-FDG PET-CT assay | ||||
| Description |
In the period between 2016 and 2018, 58 patients were referred for [177Lu]-PSMA PRLT to the center, of which 51 patients underwent both [68Ga]-PSMA and FDG PET-CT scans and provisionally qualified for the analysis; out of these complete information of four patients was not available and hence were excluded. Thus, 47 patients were retrospectively recruited and categorized according to the proposed Pro-PET scoring scheme and were analyzed as discussed above. The cohort comprised of heavily pretreated patients with 2 (4.3%) underwent radical prostatectomy; surgical castration was performed in 45 (95.7%) patients; first-line hormonal therapy (with estrogen analogues, leutinizing hormone releasing hormone agonists and antagonists and antiandrogens) in 44 (93.6%) patients, second-line hormonal therapy (with CYP17 blockers and newer anti-androgens) in 34 (72.4%) patients; first-line chemotherapy (with docetaxel) in 33 (70.2%) patients, second-line chemotherapy (with cabazitaxel, oral metronomic chemotherapy, etc.) in 22 (46.8%) and radiotherapy in 26 (55.3%) patients.
Click to Show/Hide
|
||||
| Experiment 422 Reporting the Activity Data of This PDC | [22], [26] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Progressive Disease (PD) |
24.50%
|
|||
| Patients Enrolled |
175 metastatic castration-resistant prostate cancer (mCRPC) patient were included in this meta-analysis. 65 (37.2%) patients experienced partial remission, 67 had stable disease (38.3%), and 43 (24.5%) had progressive disease.
|
||||
| Administration Dosage | 3.7-8.7 GBq/cycle | ||||
| Evaluation Method | PET/CT assay | ||||
| MOA of PDC |
The PSMA molecule acts as a target for theranostics in detecting and treating prostatic lesions. This ultimately promotes the concept of precision and personalized medicine. Several published articles showed favorable outcomes of Lu-PSMA-PRLT in mCRPC patients, which quickly translated into routine clinical practices with real effectiveness, a low toxicity profile, and documentation of the risk-benefit of PRLT. Nevertheless, many questions related to PRLT remain unresolved such as the sequencing of PRLT with ARTA or taxane-based chemotherapy, re-challenge therapy, combined therapy, alpha therapy in mCRPC patients, and early treatment of PRLT in mHNPC patients. To solve these questions, several clinical trials are currently under way, and the results of these trials will be helpful in deciding treatment strategies for prostate cancer patients.
Click to Show/Hide
|
||||
| Description |
Yadav et al. provided a meta-analysis of 177Lu-PSMA-PRLT for treating mCRPC patients. They analyzed 16 articles (13 articles used 177Lu-PSMA-617, 2 articles used 177Lu-PSMA-I&T, and 1 article used both radioligands). The authors showed >50% PSA decline after 177Lu-PSMA-PRLT in 46% of patients. Anatomical imaging response as per the RECIST criteria was reported by eight studies, with a proportion of 37.2% of patients had PR, SD in 38.3% of patients and PD in 24.5% of patients, whereas molecular imaging response as per the PERCIST criteria demonstrated PR in 74 patients (44.3%), SD in 39 patients (23.4%), and PD in 54 patients (32.3%). Common clinical toxicities were grades 1-2, which included anemia (23%), leukopenia (14.2%), thrombocytopenia (15%), nephrotoxicity (9.5%), and xerostomia (14.5%). The authors observed significant heterogeneity in several studies while analyzing this meta-analysis. They concluded that 177Lu-PSMA-PRLT is a promising treatment modality in mCRPC patients who showed PD after standard care treatments.
Click to Show/Hide
|
||||
| Experiment 423 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Progressive Disease (PD) |
28%
|
|||
| Patients Enrolled |
56 patients with metastatic castration-resistant prostate cancer.
|
||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
Another prospective trial studied 56 patients with progressive mCRPC and rising PSA levels who then received 177Lu-PSMA. Clinical efficacy was assessed using the visual analogue scale for pain, PSA levels, median overall survival, and Gallium-68-labeled prostate-specific membrane antigen (68Ga-PSMA PET/CT) for objective response. There was a decline in PSA of greater than 80% in 23.2% of patients, a decline of greater than 50% in 58.9%, and a decline of greater than 30% in 66.1% of patients. Progressive disease was noted in 10.7% of patients with a rise in PSA level greater than 25%. 68Ga-PSMA PET/CT prior to PSMA radioligand therapy showed the median SUVmax of the target lesion to be 37.5, which decreased to 15.7 after PSMA RLT. Ga-PSMA PET/CT was used to measure response rates which included a partial remission in 56%, stable disease in 8%, and progressive disease in 36% of patients. The median progression-free survival was 13.7 months, and median overall survival was not reached. PET/CT results showing a decrease in SUV max of the target lesion are indicative of a favorable objective response to Lu-PSMA therapy.
Click to Show/Hide
|
||||
| Experiment 424 Reporting the Activity Data of This PDC | [54] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Progressive Disease (PD) |
30%
|
|||
| Patients Enrolled |
10 patients with metastatic castration-resistant prostate cancer and with visceral metastasis.
|
||||
| Administration Time | One cycle | ||||
| Administration Dosage | 4.88 GBq | ||||
| Evaluation Method | Prostate-specific antigen (PSA) response assessment assay | ||||
| MOA of PDC |
Lutetium-177-PSMA was a reasonable palliative treatment option with limited toxicity for these end-stage mCRPC patients with visceral metastasis with adequate PSA stabilization. A synergistic drug amalgamation may be an ideal way to boost the outcome in the future.
|
||||
| Description |
Liver (80%), lung (30%), adrenal (10%), and peritoneum (10%) were the sites of visceral metastasis in our study. On PSA response assessment, 10%, 60%, and 30% of the patients had partial response, stable disease, and progressive disease, respectively. Forty percent of the patients had improvement in the VAS, while 50% had improvement in the AQS score. Median PFS was 24 weeks in our study. A cut-off of 4.88GBq of 177Lu-PSMA was the best-predicted progression with 66.67% sensitivity and 100% specificity on ROC analysis. Thirty percent of the patients showed grade 3 anemia. No other significant toxicity was seen.
Click to Show/Hide
|
||||
| Experiment 425 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Progressive Disease (PD) |
36%
|
|||
| Patients Enrolled |
56 patients with metastatic castration-resistant prostate cancer.
|
||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
Another prospective trial studied 56 patients with progressive mCRPC and rising PSA levels who then received 177Lu-PSMA. Clinical efficacy was assessed using the visual analogue scale for pain, PSA levels, median overall survival, and Gallium-68-labeled prostate-specific membrane antigen (68Ga-PSMA PET/CT) for objective response. There was a decline in PSA of greater than 80% in 23.2% of patients, a decline of greater than 50% in 58.9%, and a decline of greater than 30% in 66.1% of patients. Progressive disease was noted in 10.7% of patients with a rise in PSA level greater than 25%. 68Ga-PSMA PET/CT prior to PSMA radioligand therapy showed the median SUVmax of the target lesion to be 37.5, which decreased to 15.7 after PSMA RLT. Ga-PSMA PET/CT was used to measure response rates which included a partial remission in 56%, stable disease in 8%, and progressive disease in 36% of patients. The median progression-free survival was 13.7 months, and median overall survival was not reached. PET/CT results showing a decrease in SUV max of the target lesion are indicative of a favorable objective response to Lu-PSMA therapy.
Click to Show/Hide
|
||||
| Experiment 426 Reporting the Activity Data of This PDC | [48] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Progressive Disease (PD) |
42.60%
|
|||
| Patients Enrolled |
Patients with metastatic castration-resistant prostate cancer who underwent 68Ga-PSMA and FDG PET-CT scans.
|
||||
| Evaluation Method | 68Ga-PSMA/18F-FDG PET-CT assay | ||||
| Description |
In the period between 2016 and 2018, 58 patients were referred for [177Lu]-PSMA PRLT to the center, of which 51 patients underwent both [68Ga]-PSMA and FDG PET-CT scans and provisionally qualified for the analysis; out of these complete information of four patients was not available and hence were excluded. Thus, 47 patients were retrospectively recruited and categorized according to the proposed Pro-PET scoring scheme and were analyzed as discussed above. The cohort comprised of heavily pretreated patients with 2 (4.3%) underwent radical prostatectomy; surgical castration was performed in 45 (95.7%) patients; first-line hormonal therapy (with estrogen analogues, leutinizing hormone releasing hormone agonists and antagonists and antiandrogens) in 44 (93.6%) patients, second-line hormonal therapy (with CYP17 blockers and newer anti-androgens) in 34 (72.4%) patients; first-line chemotherapy (with docetaxel) in 33 (70.2%) patients, second-line chemotherapy (with cabazitaxel, oral metronomic chemotherapy, etc.) in 22 (46.8%) and radiotherapy in 26 (55.3%) patients.
Click to Show/Hide
|
||||
| Experiment 427 Reporting the Activity Data of This PDC | [48] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Progressive Disease (PD) |
44.70%
|
|||
| Patients Enrolled |
Patients with metastatic castration-resistant prostate cancer who underwent 68Ga-PSMA and FDG PET-CT scans.
|
||||
| Evaluation Method | 68Ga-PSMA/18F-FDG PET-CT assay | ||||
| Description |
In the period between 2016 and 2018, 58 patients were referred for [177Lu]-PSMA PRLT to the center, of which 51 patients underwent both [68Ga]-PSMA and FDG PET-CT scans and provisionally qualified for the analysis; out of these complete information of four patients was not available and hence were excluded. Thus, 47 patients were retrospectively recruited and categorized according to the proposed Pro-PET scoring scheme and were analyzed as discussed above. The cohort comprised of heavily pretreated patients with 2 (4.3%) underwent radical prostatectomy; surgical castration was performed in 45 (95.7%) patients; first-line hormonal therapy (with estrogen analogues, leutinizing hormone releasing hormone agonists and antagonists and antiandrogens) in 44 (93.6%) patients, second-line hormonal therapy (with CYP17 blockers and newer anti-androgens) in 34 (72.4%) patients; first-line chemotherapy (with docetaxel) in 33 (70.2%) patients, second-line chemotherapy (with cabazitaxel, oral metronomic chemotherapy, etc.) in 22 (46.8%) and radiotherapy in 26 (55.3%) patients.
Click to Show/Hide
|
||||
| Experiment 428 Reporting the Activity Data of This PDC | [48] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Progressive Disease (PD) |
51.10%
|
|||
| Patients Enrolled |
Patients with metastatic castration-resistant prostate cancer who underwent 68Ga-PSMA and FDG PET-CT scans.
|
||||
| Evaluation Method | 68Ga-PSMA/18F-FDG PET-CT assay | ||||
| Description |
In the period between 2016 and 2018, 58 patients were referred for [177Lu]-PSMA PRLT to the center, of which 51 patients underwent both [68Ga]-PSMA and FDG PET-CT scans and provisionally qualified for the analysis; out of these complete information of four patients was not available and hence were excluded. Thus, 47 patients were retrospectively recruited and categorized according to the proposed Pro-PET scoring scheme and were analyzed as discussed above. The cohort comprised of heavily pretreated patients with 2 (4.3%) underwent radical prostatectomy; surgical castration was performed in 45 (95.7%) patients; first-line hormonal therapy (with estrogen analogues, leutinizing hormone releasing hormone agonists and antagonists and antiandrogens) in 44 (93.6%) patients, second-line hormonal therapy (with CYP17 blockers and newer anti-androgens) in 34 (72.4%) patients; first-line chemotherapy (with docetaxel) in 33 (70.2%) patients, second-line chemotherapy (with cabazitaxel, oral metronomic chemotherapy, etc.) in 22 (46.8%) and radiotherapy in 26 (55.3%) patients.
Click to Show/Hide
|
||||
| Experiment 429 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Progressive Disease (PD) |
57.10%
|
|||
| Patients Enrolled |
50 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | A median of 3 cycles | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
Fifty patients were studied prospectively with PSMA-avid prostate cancer metastases who underwent a median of three cycles (range 1-4) of 177Lu PSMA-617 therapy. Nine were deemed 177Lu PSMA-617 refractory prior to death with a total of twelve deaths in the study. A PSA decline was noted in 23 patients, with 11 patients having a PSA decline of ≥50% after the first cycle of treatment. 12 patients had a PSA decline of <50% ranging from 11.3 to 43.5%. The remaining 23 patients experienced a PSA increase after the first 177Lu PSMA-617 cycle (range 19.7-100%).
Click to Show/Hide
|
||||
| Experiment 430 Reporting the Activity Data of This PDC | [74] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | PSA decline |
9.86 ng/mL
|
|||
| Administration Time | 2 months after the t hird cycle of the therapy | ||||
| Administration Dosage | 5.92 GBq | ||||
| Description |
A 56-year-old man with metastatic castration-resistant prostate cancer underwent 3 cycles of radioligand therapy (RLT) with 177Lu-prostate-specific membrane antigen (PSMA). The patient showed a dramatic response, a drop in prostate-specific antigen level from 11 ng/mL at baseline to 1.14 ng/mL at 2 months after the third cycle of the therapy, along with reduced bone pain.
Click to Show/Hide
|
||||
| In Vivo Model | A 56-year-old man with metastatic castration-resistant prostate cancer. | ||||
| Experiment 431 Reporting the Activity Data of This PDC | [75] | ||||
| Indication | ATM-mutated metastatic castration resistant prostate cancer | ||||
| Efficacy Data | PSA decline |
17.8 ng/mL
|
|||
| Administration Time | 2 cycles doses at intervals of 12 weeks | ||||
| Administration Dosage | 6 GBq | ||||
| Evaluation Method | 68Ga-PSMA PET-CT assay | ||||
| Description |
He received 2 cycles of 6 GBq doses of 177Lu-PSMA-617 at intervals of 12 weeks along with daily 160 mg of oral enzalutamide. His PSA level declined from 20 ng/mL at baseline to 2.2 ng/mL (89% reduction from baseline) after completion of 2 cycles of 177Lu-PSMA-617 with concomitant oral enzalutamide.
|
||||
| In Vivo Model | A 68-year-old man diagnosed with adenocarcinoma prostate (Gleason score 5 + 5). | ||||
| Experiment 432 Reporting the Activity Data of This PDC | [10] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | PSA decline |
40%
|
|||
| Patients Enrolled |
90-year-old patient with advanced metastatic castration-resistant prostate cancer.
|
||||
| Description |
Prasad et al. observed a 40% PSA decline in a 90-y-old patient with advanced mCRPC who initiated 177Lu-PSMA-617 while receiving pembrolizumab for locally advanced squamous cell carcinoma.
|
||||
| Experiment 433 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | PSA decline |
46%
|
|||
| Patients Enrolled |
30 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Dosage | 180 mCi | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
A study sought to analyze the prognostic significance of monitoring PSA levels during 177Lu-PSMA-617 treatment. The study included thirty mCPRC patients who had baseline Ga-68 PSMA PET/CT prior to undergoing 177Lu-PSMA-617 treatment. Patients were treated with a fixed dose of 180 mCi of 177Lu-PSMA-617 every six to eight weeks. A total of 171 cycles of treatment were administered with a median of four cycles per patients (range 3-7). A PSA decline greater than 50% was seen in 33% of patients after one cycle of treatment and increased to 43% of patients at the conclusion of the last cycle of treatment. Of the 20 patients who did not have a 50% reduction in PSA levels after the first cycle, four of these patients eventually had a PSA decline of greater than 50% after the conclusion of the last cycle of treatment. The median OS was statistically significant in those who had a greater than 50% decline in PSA level 21 ± 10 (95% CI: 1.2-40.7) compared to those who did not 8.0 ± 2.6 (95% CI: 2.7-13.2) months (p = 0.012). Any PSA decline was seen in 50% of patients after just one cycle of treatment and remained stable at 46% of patients at the conclusion of treatment, but did not have a statistically significant impact on median OS; however it was significant for any PSA decline after the last cycle of treatment (13 ± 1, 95% CI: 10.9-15 months for responders versus 6.0 ± 1.9, 95% CI: 2.2-9.7 months for non-responders).
Click to Show/Hide
|
||||
| Experiment 434 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | PSA decline |
50%
|
|||
| Patients Enrolled |
30 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 1 cycles | ||||
| Administration Dosage | 180 mCi | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
A study sought to analyze the prognostic significance of monitoring PSA levels during 177Lu-PSMA-617 treatment. The study included thirty mCPRC patients who had baseline Ga-68 PSMA PET/CT prior to undergoing 177Lu-PSMA-617 treatment. Patients were treated with a fixed dose of 180 mCi of 177Lu-PSMA-617 every six to eight weeks. A total of 171 cycles of treatment were administered with a median of four cycles per patients (range 3-7). A PSA decline greater than 50% was seen in 33% of patients after one cycle of treatment and increased to 43% of patients at the conclusion of the last cycle of treatment. Of the 20 patients who did not have a 50% reduction in PSA levels after the first cycle, four of these patients eventually had a PSA decline of greater than 50% after the conclusion of the last cycle of treatment. The median OS was statistically significant in those who had a greater than 50% decline in PSA level 21 ± 10 (95% CI: 1.2-40.7) compared to those who did not 8.0 ± 2.6 (95% CI: 2.7-13.2) months (p = 0.012). Any PSA decline was seen in 50% of patients after just one cycle of treatment and remained stable at 46% of patients at the conclusion of treatment, but did not have a statistically significant impact on median OS; however it was significant for any PSA decline after the last cycle of treatment (13 ± 1, 95% CI: 10.9-15 months for responders versus 6.0 ± 1.9, 95% CI: 2.2-9.7 months for non-responders).
Click to Show/Hide
|
||||
| Experiment 435 Reporting the Activity Data of This PDC | [5] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | PSA decline |
51%
|
|||
| Patients Enrolled |
45 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 164 cycles of rnt, every 6-8 weeks | ||||
| Description |
Forty-five patients were treated with total of 164 cycles of RNT. Fifteen patients (33%) had PSA decline of ≥50%, 23 patients (51%) showed any PSA decline and 20 patients (44%) showed PSA increase of ≥25%. Median OS and PFS were 17,1 months and 7,4 months. Patients had any or ≥50% PSA response after the first cycle, lower initial ALP (<120U/L) had longer OS and PFS. Patients had normal Hb showed longer OS and patients had lower initial PSA (<51ng/mL) had longer PFS. Patients had PSA progression of ≥25% had shorter OS and PFS.
Click to Show/Hide
|
||||
| Experiment 436 Reporting the Activity Data of This PDC | [76] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | PSA decline |
58.50%
|
|||
| Description |
A 79-year-old man with a history of metastatic prostate cancer was initially treated with Eligard and switched to relugolix in 2021. The 2022 bone scan presented superscan and extensive osseous metastatic lesions; some had intense PSMA uptake on the initial PSMA PET scan without nodal or visceral metastatic lesions. We treated him with Pluvicto and relugolix. The intermediate PSMA scan demonstrated prominent bone marrow PSMA uptake. However, PSA decreased 58.5%. We hypothesized that the patient might have a bone flare. The final PSMA scan confirmed our hypothesis. Based on our knowledge, this is the first case of Pluvicto-induced bone flare.
Click to Show/Hide
|
||||
| In Vivo Model | A 79-year-old man with a history of metastatic prostate cancer. | ||||
| Experiment 437 Reporting the Activity Data of This PDC | [14] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | PSA decline |
59%
|
|||
| Patients Enrolled |
28 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 1 dose | ||||
| MOA of PDC |
Radiopharmaceuticals have been used in prostate cancer for decades with known efficacy in palliation of bone metastasis. The FDA approval of the most recent radiopharmaceutical, 177Lu-PSMA-617, shows a clear overall survival benefit compared to the best SOC. Current studies are ongoing to evaluate the effectiveness of 177Lu-PSMA-617 in earlier lines of therapy, such as after only 1 line of therapy with an ARPI as in the PSMAfore study, or in mCSPC in combination with ADT and an ARPI as in the PSMAddition study. Studies are also ongoing with 177Lu-PSMA-617 in combination with other treatments which may produce a synergistic effect. As described, there are many clinical trials ongoing that are modifying the 177Lu-PSMA-617 to possibly achieve improved results. Studies are also ongoing looking at swapping the 177Lu for another radioactive agent, such as 225Ac (an alpha emitter) which may have benefits over the beta-emitting 177Lu. Other studies are looking at J591, a monoclonal antibody to PSMA which has unique differences compared to small-molecule PSMA binders. Overall, PSMA-based radioligand therapy has been shown to be an effective and life-prolonging therapy and should be considered a treatment option for selected men with mCRPC. As described, there are many ongoing studies further evaluating PSMA radioligand therapy in Australia, South Africa, Europe, and the United States, representing a truly global effort to improve prostate cancer care.
Click to Show/Hide
|
||||
| Description |
A subsequent retrospective study, the first evaluating multiple administrations of 177Lu-PSMA-617, was reported by the same group. The authors reviewed 28 consecutive patients who received 50 infusions of 177Lu-PSMA-617 between 2014 and 2015. In their report, a PSA decline was noted in 59% and 75% of patients after 1 and 2 therapies, respectively, and a PSA decline of 50% or greater occurred in 32% and 50%, respectively. The estimated median survival was 29.4 weeks compared to 19.7 weeks in the historical best supportive care group which was statistically significant (HR 44; 95% CI 0.20-0.95; P=.031). Authors of the study also noted no significant changes in hematologic or renal parameters
Click to Show/Hide
|
||||
| Experiment 438 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | PSA decline |
59%
|
|||
| Patients Enrolled |
28 patients with metastatic castration-resistant prostate cancer.
|
||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
A retrospective analysis studied 28 patients with mCRPC who were treated with 177Lu-PSMA-617 [Citation47]. The estimated median survival was 29.4 weeks, significantly longer than survival in the supportive care group (HR, 0.44; 95% confidence interval, 0.20-0.95]; P = 0.031). Results of the study noted any PSA decline in 59% of patients after one cycle and 75% of patients after two cycles of treatment, while there was a noted PSA decline of 50% or greater in 32% of patients after one cycle of treatment and in 50% of patients after two cycles of treatment. Although this study found a 50% or greater PSA decline in majority of treated patients, 83% of patients reported a stable or improved quality of life after treatment.
Click to Show/Hide
|
||||
| Experiment 439 Reporting the Activity Data of This PDC | [22] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | PSA decline |
60%
|
|||
| Patients Enrolled |
145 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 1-4 cycles | ||||
| Administration Dosage | 2-8 GBq/cycle | ||||
| MOA of PDC |
The PSMA molecule acts as a target for theranostics in detecting and treating prostatic lesions. This ultimately promotes the concept of precision and personalized medicine. Several published articles showed favorable outcomes of Lu-PSMA-PRLT in mCRPC patients, which quickly translated into routine clinical practices with real effectiveness, a low toxicity profile, and documentation of the risk-benefit of PRLT. Nevertheless, many questions related to PRLT remain unresolved such as the sequencing of PRLT with ARTA or taxane-based chemotherapy, re-challenge therapy, combined therapy, alpha therapy in mCRPC patients, and early treatment of PRLT in mHNPC patients. To solve these questions, several clinical trials are currently under way, and the results of these trials will be helpful in deciding treatment strategies for prostate cancer patients.
Click to Show/Hide
|
||||
| Description |
The first major multi-center retrospective study on 177Lu-PSMA-617 was published by Rahbar et al., reporting 145 patients with mCRPC who progressed after second-line systemic therapies. The overall response rate in terms of serum PSA decline >50% was seen in 45% of patients after all 177Lu-PSMA-617 cycles. On imaging, 21 (45%) patients and 13 (28%) patients had PR and SD, respectively. There was grade 3-4 toxicity in 18 patients (13%), which included severe anemia, thrombocytopenia, and leukopenia. They found elevated alkaline phosphatase and visceral metastases as negative predictors of response to 177Lu-PSMA-617. A major drawback of this study was the variable cycles and doses of 177Lu-PSMA-617 given to patients
Click to Show/Hide
|
||||
| Experiment 440 Reporting the Activity Data of This PDC | [32] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | PSA decline |
62%
|
|||
| Patients Enrolled |
Metastatic castration-resistant prostate cancer patients.
|
||||
| Description |
One of the earliest experiences with 177Lu-PSMA-617 radioligand therapy (RLT) was described by Ahmadzadehfar et al. in 2015. Ten patients with mCRPC were recruited to undergo 177Lu-PSMA-617 RLT and received one cycle of therapy (dose 6 GBq). At eight-week follow-up, 70% (7/10) experienced PSA decline, and 50% (5/10) experienced >50% decline in PSA levels. After those initial encouraging results, in a follow-up study with an expanded cohort, 24 patients with progressive mCRPC underwent 177Lu-PSMA-617 RLT. After one cycle, 79.1% (19/24) showed a decline in PSA levels; 41.7% (10/24) showed >50% decline. Twenty-two out of the 24 patients were selected for a second cycle, and 68.2% (15/22) had a PSA decline, with 13 (59%) experiencing >50% decline. Since then, numerous retrospective studies with larger groups of patients have been published by the same group. In 2017, Ahmadzadehfar et al. reported a cohort of 52 patients who each received between three and six cycles of therapy (mean: 3.6 cycles, mean dose: 6 GBq). Dosing was administered in eight-week intervals and the median cumulative dose was 18.5 GBq. Of note, 80.8% (42/52) experienced a PSA decline eight weeks after the first cycle. Median overall survival was 60 weeks, with patients who had PSA responses having significantly longer survival compared to those who did not (68 vs. 33 weeks). In a cohort of 99 patients who received between one to four cycles of therapy (mean: 1.7 cycles) with 8-12 week intervals, 65.6% (45/99) had PSA response after the first cycle. In a cohort of 104 patients, described in 2018, 67.3% (70/104) experienced a PSA decline after one cycle of therapy. Patients underwent an average of 3.4 cycles of therapy, with eight-week intervals. The average dose was 6.1 GBq per cycle and 18.8 GBq cumulatively. The median overall survival was 56 weeks; again, those who responded had longer survival (62.9 vs. 47 weeks).
Click to Show/Hide
|
||||
| Experiment 441 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | PSA decline |
64%
|
|||
| Patients Enrolled |
82 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 1 dose | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
One study retrospectively analyzed 82 mCRPC patients who received a single dose of Lu-PSMA. Tolerability and response to treatment were assessed using hematologic parameters, renal scintigraphy, clinical data, and prostate-specific antigen (PSA) levels. A PSA decline from baseline was noted in 64% patients with 31% of patients having a greater than 50% decline, while 47% patients had stable disease with a 25-50% decrease in PSA levels. Only 25% of patients showed an increase in PSA levels indicating disease progression, and 7% of patients died due to extensive disease.
Click to Show/Hide
|
||||
| Experiment 442 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | PSA decline |
65%
|
|||
| Patients Enrolled |
56 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 1-4 cycles | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
Another retrospective study evaluated 56 mCPRC patients with a median age of 69.5 (range 55-84) who received one to four cycles of 177Lu-PSMA-617. Biochemical response was defined using Prostate Cancer Working Group Criteria 3 (PCWG3). A total of 139 cycles of treatment were performed with a decline of greater than 50% in 54% of patients and any PSA decline in 65% of patients. Estimated median overall survival was 16 months versus 14 months in the chemotherapy alone group. Longer OS was observed in patients with a PSA decline of >50%, a baseline ALP level <220 U/l, more than two cycles of treatment, and cumulative activity of greater than 15 GBq.
Click to Show/Hide
|
||||
| Experiment 443 Reporting the Activity Data of This PDC | [29] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | PSA decline |
66%
|
|||
| Patients Enrolled |
Patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | Total of 213 cycles; 3 cycles with every 8 weeks | ||||
| Administration Dosage | 6.016 ± 0.543 GBq | ||||
| Description |
A PSA decline ≥50% and some PSA decline occurred in 56% and 66% of the patients.
|
||||
| Experiment 444 Reporting the Activity Data of This PDC | [15] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | PSA decline |
67%
|
|||
| Patients Enrolled |
Patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 351 cycles | ||||
| Description |
Any PSA decline occurred in 70 (67%) and a PSA decline ≥50% in 34 (33%) of patients after the first cycle.
|
||||
| Experiment 445 Reporting the Activity Data of This PDC | [17] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | PSA decline |
69.30%
|
|||
| Patients Enrolled |
508patients with metastatic castration-resistant prostate cancer.
|
||||
| Description |
A total of 12 studies involving 508 cases of mCRPC were included in this analysis. After the first cycle of treatment, the pooled rate of PSA decline was 69.30% (95% CI: 65.40%73.30%), and that of >50% PSA decline was 35.90% (95% CI: 31.80%40.00%). No significant adverse events were reported in any of the studies.
|
||||
| Experiment 446 Reporting the Activity Data of This PDC | [14] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | PSA decline |
70%
|
|||
| Patients Enrolled |
10 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 8 weeks | ||||
| MOA of PDC |
Radiopharmaceuticals have been used in prostate cancer for decades with known efficacy in palliation of bone metastasis. The FDA approval of the most recent radiopharmaceutical, 177Lu-PSMA-617, shows a clear overall survival benefit compared to the best SOC. Current studies are ongoing to evaluate the effectiveness of 177Lu-PSMA-617 in earlier lines of therapy, such as after only 1 line of therapy with an ARPI as in the PSMAfore study, or in mCSPC in combination with ADT and an ARPI as in the PSMAddition study. Studies are also ongoing with 177Lu-PSMA-617 in combination with other treatments which may produce a synergistic effect. As described, there are many clinical trials ongoing that are modifying the 177Lu-PSMA-617 to possibly achieve improved results. Studies are also ongoing looking at swapping the 177Lu for another radioactive agent, such as 225Ac (an alpha emitter) which may have benefits over the beta-emitting 177Lu. Other studies are looking at J591, a monoclonal antibody to PSMA which has unique differences compared to small-molecule PSMA binders. Overall, PSMA-based radioligand therapy has been shown to be an effective and life-prolonging therapy and should be considered a treatment option for selected men with mCRPC. As described, there are many ongoing studies further evaluating PSMA radioligand therapy in Australia, South Africa, Europe, and the United States, representing a truly global effort to improve prostate cancer care.
Click to Show/Hide
|
||||
| Description |
Though the first experience with PSMA-targeted 177Lu dates to 2013 at Bad Burka, this experience was not reported until later. The first report on safety and efficacy came from investigators at University Hospital Bonn and University Hospital Muenster. The authors retrospectively evaluated the results of 10 consecutive patients with mCRPC who were treated with a single dose of 177Lu-DKFZ-617 (later called simply PSMA-617) PSMA between 2013 and 2014. They showed that after 8 weeks, 7 patients (70%) showed a PSA decline with 5 patients (50%) having more than a 50% decline in PSA. Grade 3 or higher hematotoxicity was seen in only one patient and there was no relevant nephrotoxicity or hepatotoxicity.
Click to Show/Hide
|
||||
| Experiment 447 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | PSA decline |
70%
|
|||
| Patients Enrolled |
30 patients with PSMA-positive prostate tumor.
|
||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
177Lu-PSMA-617 was offered to thirty patients with PSMA-positive prostate tumor. Treatment efficacy was retrospectively assessed by PSA levels with 70% of patients demonstrating a decrease in PSA levels. 18 patients were noted to have PSA decline greater than 25%, while 13 patients had a decline greater than 50%. Six of these patients were restaged using PSMA PET/CT (positron emission tomography/computed tomography), and all six patients had a response rate of more than 50% in SUVmax (maximum standardized uptake value) of the tumor.
Click to Show/Hide
|
||||
| Experiment 448 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | PSA decline |
70%
|
|||
| Patients Enrolled |
10 patients with metastatic castration-resistant prostate cancer.
|
||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
A small two center study was conducted in 2015, which followed ten mCRPC patients treated with 177Lu-PSMA-617. Response was evaluated by change in PSA. Eight weeks after therapy, seven out of the 10 study subjects, experienced a decline in PSA. Six out of ten patients had a decline more than 30%, while five patients had a decline of more than 50% in their PSA levels. Three patients showed an increase in PSA indicative of progression of disease. Post-treatment PSA levels declined significantly in this study, indicating positive treatment response.
Click to Show/Hide
|
||||
| Experiment 449 Reporting the Activity Data of This PDC | [22] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | PSA decline |
71.80%
|
|||
| Patients Enrolled |
416 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 3 cycles | ||||
| MOA of PDC |
The PSMA molecule acts as a target for theranostics in detecting and treating prostatic lesions. This ultimately promotes the concept of precision and personalized medicine. Several published articles showed favorable outcomes of Lu-PSMA-PRLT in mCRPC patients, which quickly translated into routine clinical practices with real effectiveness, a low toxicity profile, and documentation of the risk-benefit of PRLT. Nevertheless, many questions related to PRLT remain unresolved such as the sequencing of PRLT with ARTA or taxane-based chemotherapy, re-challenge therapy, combined therapy, alpha therapy in mCRPC patients, and early treatment of PRLT in mHNPC patients. To solve these questions, several clinical trials are currently under way, and the results of these trials will be helpful in deciding treatment strategies for prostate cancer patients.
Click to Show/Hide
|
||||
| Description |
Since initial retrospective studies had a limited number of patients and a heterogeneous population, the WARMTH (World Association of Radiopharmaceutical and Molecular Therapy) planned a multi-center retrospective study to evaluate response rate, OS, and the impact of prior therapies on OS in more than 300 mCRPC patients treated with 177Lu-PSMA-617. The study included 416 mCRPC patients who received a total of 1493 cycles of 177Lu-PSMA-617, with a median of 3 cycles per patient. Post-177Lu-PSMA-617, serum PSA decline was seen in 282 (71.8%) patients, of whom 163 (41.5%) showed a serum PSA decline of ≥50%, whereas 111 patients (28.2%) showed an increase in serum PSA levels. A median OS of 11.1 months (95% CI 9.7-12.5 months) was observed. Prior chemotherapy, the presence of bone and liver metastases, and poor ECOG status were significant adverse prognosticators for survival in both univariate and multivariate analyses. No imaging response evaluation and no determination of PFS after 177Lu-PSMA-617 were major limitations for this study.
Click to Show/Hide
|
||||
| Experiment 450 Reporting the Activity Data of This PDC | [33] | ||||
| Indication | ATM-mutated metastatic castration resistant prostate cancer | ||||
| Efficacy Data | PSA decline |
73%
|
|||
| Patients Enrolled |
121 metastatic castration-resistant prostate cancer patients.
|
||||
| Administration Dosage | Median administered cumulative activity: 20 GBq | ||||
| MOA of PDC |
177Lu-PSMA-617 RLT is an effective form of therapy in mCRPC patients and confirms the findings of the short-term studies. 177Lu-PSMA-617 prolongs the overall survival in mCRPC patients heavily pre-treated with chemotherapy, first and second-line anti-androgens, and androgen inhibitor therapies. The delayed toxicity is low and acceptable by most of these patients. Patients who were treated with various other mCRPC-approved compounds before 177Lu-PSMA-RLT were associated with a significantly shorter OS than that of the patients who received 177Lu-PSMA RLT at the earlier stages of mCRPC. An aggressive treatment approach, either sequential or in combination with second-generation anti-androgens, chemotherapies, or with investigational 225Ac-PSMA-617 alpha therapies, might prolong the survival of mCRPC patients in the future.
Click to Show/Hide
|
||||
| Description |
The median administered cumulative activity was 20 GBq (3.7-37 GBq). The median follow-up duration was 36 months (6-72 months). The estimated median PFS and OS were 12 months (mo) (95% CI: 10.3-13 mo) and 16 mo (95% CI: 13-17 mo), respectively. Any PSA decline and PSA decline >50% was achieved in 73% and 61% of the patients, respectively. Multivariate analysis revealed only failure to achieve >50% PSA decline as a significant factor associated with a poor PFS. Prognostic factors associated with reduced OS included, failure to experience >50% PSA decline, heavily pre-treated patient cohort who received >2 lines of prior treatment options, and patient sub-group treated with ≥2 lines of chemotherapy. Patients re-treated with additional treatment options after attaining 177Lu-PSMA refractory disease showed a remarkably prolonged OS. A significant clinical benefit was achieved post 177Lu-PSMA-617 RLT. The most common toxicities observed were fatigue (34.7%), followed by nausea (33%), and dry mouth (24.7%).
Click to Show/Hide
|
||||
| Experiment 451 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | PSA decline |
73%
|
|||
| Patients Enrolled |
52 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 3 cycles every eight weeks | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
An additional retrospective study of 52 mCRPC patients (mean age of 70, range 48-87 years) evaluated the PSA response of those treated with 177Lu-PSMA-617 after one to three cycles of radioligand therapy (RLT) every eight weeks. A total of 190 cycles of RLT (3-6 cycles per patient) were given and 80% of patients showed a decline after the first cycle with 44% of patients showing a PSA response of more than 50%. After the third cycle, 73% of patients showed any PSA decline. The median OS was 60 weeks for all patients and median OS was statistically longer for those who responded with decline in PSA after first cycle compared to those without (68 vs 33 weeks).
Click to Show/Hide
|
||||
| Experiment 452 Reporting the Activity Data of This PDC | [14] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | PSA decline |
75%
|
|||
| Patients Enrolled |
28 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 2 doses | ||||
| MOA of PDC |
Radiopharmaceuticals have been used in prostate cancer for decades with known efficacy in palliation of bone metastasis. The FDA approval of the most recent radiopharmaceutical, 177Lu-PSMA-617, shows a clear overall survival benefit compared to the best SOC. Current studies are ongoing to evaluate the effectiveness of 177Lu-PSMA-617 in earlier lines of therapy, such as after only 1 line of therapy with an ARPI as in the PSMAfore study, or in mCSPC in combination with ADT and an ARPI as in the PSMAddition study. Studies are also ongoing with 177Lu-PSMA-617 in combination with other treatments which may produce a synergistic effect. As described, there are many clinical trials ongoing that are modifying the 177Lu-PSMA-617 to possibly achieve improved results. Studies are also ongoing looking at swapping the 177Lu for another radioactive agent, such as 225Ac (an alpha emitter) which may have benefits over the beta-emitting 177Lu. Other studies are looking at J591, a monoclonal antibody to PSMA which has unique differences compared to small-molecule PSMA binders. Overall, PSMA-based radioligand therapy has been shown to be an effective and life-prolonging therapy and should be considered a treatment option for selected men with mCRPC. As described, there are many ongoing studies further evaluating PSMA radioligand therapy in Australia, South Africa, Europe, and the United States, representing a truly global effort to improve prostate cancer care.
Click to Show/Hide
|
||||
| Description |
A subsequent retrospective study, the first evaluating multiple administrations of 177Lu-PSMA-617, was reported by the same group. The authors reviewed 28 consecutive patients who received 50 infusions of 177Lu-PSMA-617 between 2014 and 2015. In their report, a PSA decline was noted in 59% and 75% of patients after 1 and 2 therapies, respectively, and a PSA decline of 50% or greater occurred in 32% and 50%, respectively. The estimated median survival was 29.4 weeks compared to 19.7 weeks in the historical best supportive care group which was statistically significant (HR 44; 95% CI 0.20-0.95; P=.031). Authors of the study also noted no significant changes in hematologic or renal parameters
Click to Show/Hide
|
||||
| Experiment 453 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | PSA decline |
75%
|
|||
| Patients Enrolled |
28 patients with metastatic castration-resistant prostate cancer.
|
||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
A retrospective analysis studied 28 patients with mCRPC who were treated with 177Lu-PSMA-617 [Citation47]. The estimated median survival was 29.4 weeks, significantly longer than survival in the supportive care group (HR, 0.44; 95% confidence interval, 0.20-0.95]; P = 0.031). Results of the study noted any PSA decline in 59% of patients after one cycle and 75% of patients after two cycles of treatment, while there was a noted PSA decline of 50% or greater in 32% of patients after one cycle of treatment and in 50% of patients after two cycles of treatment. Although this study found a 50% or greater PSA decline in majority of treated patients, 83% of patients reported a stable or improved quality of life after treatment.
Click to Show/Hide
|
||||
| Experiment 454 Reporting the Activity Data of This PDC | [22] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | PSA decline |
75-90%
|
|||
| Patients Enrolled |
30 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 3 cycles | ||||
| Administration Dosage | 3.8-6.7 GBq/cycle | ||||
| MOA of PDC |
The PSMA molecule acts as a target for theranostics in detecting and treating prostatic lesions. This ultimately promotes the concept of precision and personalized medicine. Several published articles showed favorable outcomes of Lu-PSMA-PRLT in mCRPC patients, which quickly translated into routine clinical practices with real effectiveness, a low toxicity profile, and documentation of the risk-benefit of PRLT. Nevertheless, many questions related to PRLT remain unresolved such as the sequencing of PRLT with ARTA or taxane-based chemotherapy, re-challenge therapy, combined therapy, alpha therapy in mCRPC patients, and early treatment of PRLT in mHNPC patients. To solve these questions, several clinical trials are currently under way, and the results of these trials will be helpful in deciding treatment strategies for prostate cancer patients.
Click to Show/Hide
|
||||
| Description |
Yordanova et al., evaluated the response rate and clinical toxicity of re-challenge 177Lu-PSMA-617 in progressive prostatic cancer patients who previously benefited from this therapy. In this retrospective study, a total of 30 patients were re-treated with a median of 3 (range 1-6) cycles of 177Lu-PSMA-617. They found that 75-90% of patients demonstrated favorable serum PSA responses following re-challenge cycles, with a median OS of 12 months after the first re-challenge cycle and without any life-threatening grade-4 adverse event. The authors concluded that the majority of patients benefited from re-challenging 177Lu-PSMA-617 with a longer OS in biochemically responsive patients. At present, data on re-challenge 177Lu-PSMA-617 is limited and requires a prospective randomized trial before a definitive conclusion.
Click to Show/Hide
|
||||
| Experiment 455 Reporting the Activity Data of This PDC | [77] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | PSA decline |
76%
|
|||
| Patients Enrolled |
30 patients with proven metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 5 cycles of treatment with 177lu-psma-617 prlt | ||||
| Administration Dosage | 4.94 ± 0.45 GBq/cycle | ||||
| Description |
After the first cycle of 177Lu-PSMA-617 therapy, 9 patients expired due to their progressive disease. Of the 21 patients, where prostate-specific antigen (PSA) data are available, 16 (76%) showed reduction in PSA levels.
|
||||
| Experiment 456 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | PSA decline |
80%
|
|||
| Patients Enrolled |
52 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 1 cycles | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
An additional retrospective study of 52 mCRPC patients (mean age of 70, range 48-87 years) evaluated the PSA response of those treated with 177Lu-PSMA-617 after one to three cycles of radioligand therapy (RLT) every eight weeks. A total of 190 cycles of RLT (3-6 cycles per patient) were given and 80% of patients showed a decline after the first cycle with 44% of patients showing a PSA response of more than 50%. After the third cycle, 73% of patients showed any PSA decline. The median OS was 60 weeks for all patients and median OS was statistically longer for those who responded with decline in PSA after first cycle compared to those without (68 vs 33 weeks).
Click to Show/Hide
|
||||
| Experiment 457 Reporting the Activity Data of This PDC | [78] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | PSA decline |
80.30%
|
|||
| Patients Enrolled |
61 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | T hree cycles at four weekly intervals | ||||
| Administration Dosage | Mean 7321 ± 592 MBq | ||||
| Description |
Forty-nine (80.3%) patients demonstrated a therapy response in terms of any PSA decline, while 21 (19.7%) patients showed increase or no changes in their PSA levels.
|
||||
| Experiment 458 Reporting the Activity Data of This PDC | [79] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | PSA decline |
90%
|
|||
| Administration Time | 3 cycles and an interval of 6-8 weeks | ||||
| Administration Dosage | 5.5 GBq/cycle | ||||
| MOA of PDC |
Although distant cutaneous metastasis is an uncommon presentation of prostate cancer, it remains an important diagnostic consideration as an advanced disease and a poor prognosis. Herein we present a rare case of prostate cancer patient whose multiple cutaneous metastases were treated with 177Lu-PSMA-617 radioligand treatment. To our knowledge, it is the first report in which a complete response was seen with 68Ga-PSMA PET/CT scan after 177Lu-PSMA-617 radioligand treatment.
Click to Show/Hide
|
||||
| Description |
A 70-year-old man with history of prostate cancer was referred to our department for 68Ga-PSMA PET/CT. He had been diagnosed with prostate adenocarcinoma 12 years earlier, with a Gleason score of 5 + 5 = 10. He had a complaint of skin nodules on the pubis and the left lower extremity swelling that had appeared for a few months. Physical examination revealed multiple indurated, erythematous, and infiltrating papulonodular lesions with the largest 3.5 2.3 cm over the pubis (A). The PSA level was 755 ng/mL. Increased 68Ga-PSMA uptakes were seen to correspond to most of the cutaneous lesions on pubis, with a mean SUVmax of 25. In addition, there were multiple pelvic and retroperitoneal lymph nodes showing increased PSMA uptake (SUVmax, 17) highly suggestive of lymph node metastasis (B) and increased PSMA uptakes in the cutaneous and subcutaneous tissues and edema in the left lower extremity (C). Given the patient history, skin nodules showing increased 68Ga-PSMA uptake were suspected to be metastatic lesions from prostate carcinoma as well. Histological evaluation and immunohistochemical staining with PSA, prostate-specific acid phosphatase (PSAP), cytokeratin 20 (CK20), and CDX2 were consistent with metastatic prostate adenocarcinoma to cutaneous tissue. 177Lu-PSMA radioligand treatment was planned because the lesions showed increased PSMA uptakes. After a total of 3 cycles 177Lu-PSMA-617 (with a mean activity of 5.5 GBq per cycle and an interval of 6-8 weeks), it was observed that the existing all skin lesions disappeared. Also 68Ga-PSMA PET/CT scan revealed that all lesions showing increased PSMA uptake disappeared (D). The PSA level has dropped to 75 ng/mL.
Click to Show/Hide
|
||||
| In Vivo Model | A 70-year-old man with history of prostate cancer. | ||||
| Experiment 459 Reporting the Activity Data of This PDC | [28] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | PSA decline |
91%
|
|||
| Patients Enrolled |
Patients with metastatic castration-resistant prostate cance, who had been treated with at least one next-generation antihormonal drug as well as chemotherapy.
|
||||
| Administration Time | 159 cycle | ||||
| Administration Dosage | Median dose 6.11 GBq | ||||
| Description |
A decline in prostate-specific antigen (PSA) of ≥50% occurred in 53%, and a decline in PSA of any amount in 91% of patients. The estimated median OS was 32 weeks.
|
||||
| Experiment 460 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | PSA decline |
91%
|
|||
| Patients Enrolled |
59 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | A median of 3 cycles | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
Another study retrospectively studied fifty-nine mCRPC patients after receiving at least one antihormonal drug as well as chemotherapy. These patients were treated with a median of three cycles of 177Lu-PSMA-61. The primary end point was overall survival, and secondary end point was decrease in PSA level. Follow-up data was available for forty-five patients with 91% showing a PSA decline. A decline in PSA levels of greater than or equal to 50% occurred in 53% of the patients. The median overall survival was 32 weeks. An initial alkaline phosphatase (ALP) level less than 220 U/L and a PSA decline after the first cycle were associated with a longer overall survival (56 vs. 28 weeks, p < 0.01, and 56 vs. 29 weeks, p = 0.04, respectively). Toxicity overview showed grade 3 leukopenia and thrombocytopenia in 3% patients and grade 3 anemia in 19%. No grade 3 or 4 nephrotoxicity or grade 4 blood toxicity was observed. This study showed a statistically significant decline in ALP levels after the first cycle of 177Lu-PSMA-617.
Click to Show/Hide
|
||||
| Experiment 461 Reporting the Activity Data of This PDC | [13] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | PSA decline rate |
58%
|
|||
| Patients Enrolled |
22 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | First treatment cycle | ||||
| Description |
After the first treatment cycle, only 58% of the patients (n = 19) showed a decrease in serum PSA, and only 32% showed a decrease of more than 50%. After all treatment cycles were completed, 65% of the patients responded with a PSA drop greater than 50%. An even higher group of 84% responded with a general decrease in PSA levels. The highest reduction of PSA levels was observed from 139.1 to 0.24 ug/L (99.83%). Before PSMA RLT treatment, the mean serum PSA level was 258.12 ug/L (range, 0.42-3305.00 ug/L) and after 2 to 9 treatment cycles, it decreased to 79.61 ug/L (range, 0.24-869.10 ug/L).
Click to Show/Hide
|
||||
| Experiment 462 Reporting the Activity Data of This PDC | [24] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | PSA decline rate |
60%
|
|||
| Patients Enrolled |
Patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 2-cycles of 177lu-psma-rlt | ||||
| Administration Dosage | 3.5-7.5 GBq | ||||
| MOA of PDC |
Entwickelt im Deutschen Krebsforschungszentrum in Heidelberg, ist PSMA-617 der weltweit weiterhin am hufigsten eingesetzte Ligand zur Behandlung von Patienten mit metastasiertem Prostatakarzinom. (Developed at the German Cancer Research Center in Heidelberg, PSMA-617 remains the most commonly used ligand worldwide for treating patients with metastatic prostate cancer.)
Click to Show/Hide
|
||||
| Description |
Im Median erhielten die Patienten 2 Zyklen der 177Lu-PSMA-RLT. Die Mehrheit der Patienten erhielt 3,5-7,5 GBq (im Median 6,0 GBq) Aktivitt pro Zyklus. ber den gesamten Beobachtungszeitraum zeigten 45 % der Patienten eine PSA50. Irgendein PSA-Abfall trat bei 60 % der Patienten auf. (The patients received a median of 2 cycles of 177Lu-PSMA-RLT. The majority of the patients received 3.5-7.5 GBq (a median of 6.0 GBq) of activity per cycle. Throughout the entire observation period, 45% of the patients exhibited a PSA50. Some decrease in PSA levels occurred in 60% of the patients.)
Click to Show/Hide
|
||||
| Half life period | 6.7 day | ||||
| Experiment 463 Reporting the Activity Data of This PDC | [13] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | PSA decline rate |
84%
|
|||
| Patients Enrolled |
22 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | All treatment cycles | ||||
| Description |
After the first treatment cycle, only 58% of the patients (n = 19) showed a decrease in serum PSA, and only 32% showed a decrease of more than 50%. After all treatment cycles were completed, 65% of the patients responded with a PSA drop greater than 50%. An even higher group of 84% responded with a general decrease in PSA levels. The highest reduction of PSA levels was observed from 139.1 to 0.24 ug/L (99.83%). Before PSMA RLT treatment, the mean serum PSA level was 258.12 ug/L (range, 0.42-3305.00 ug/L) and after 2 to 9 treatment cycles, it decreased to 79.61 ug/L (range, 0.24-869.10 ug/L).
Click to Show/Hide
|
||||
| Experiment 464 Reporting the Activity Data of This PDC | [75] | ||||
| Indication | ATM-mutated metastatic castration resistant prostate cancer | ||||
| Efficacy Data | PSA decline rate |
89%
|
|||
| Administration Time | 2 cycles doses at intervals of 12 weeks | ||||
| Administration Dosage | 6 GBq | ||||
| Evaluation Method | 68Ga-PSMA PET-CT assay | ||||
| Description |
He received 2 cycles of 6 GBq doses of 177Lu-PSMA-617 at intervals of 12 weeks along with daily 160 mg of oral enzalutamide. His PSA level declined from 20 ng/mL at baseline to 2.2 ng/mL (89% reduction from baseline) after completion of 2 cycles of 177Lu-PSMA-617 with concomitant oral enzalutamide.
|
||||
| In Vivo Model | A 68-year-old man diagnosed with adenocarcinoma prostate (Gleason score 5 + 5). | ||||
| Experiment 465 Reporting the Activity Data of This PDC | [80] | ||||
| Indication | Metastatic hormone-sensitive prostate cancer | ||||
| Efficacy Data | PSA decline rate |
99.80%
|
|||
| Administration Time | Two cycles at 8-weeks intervals | ||||
| Administration Dosage | 6.0 GBq/cycle | ||||
| MOA of PDC |
177Lu-PSMA-617 appeared to be a feasible, safe, and effective modality for patients with low-volume mHSPC. The excellent biochemical and radiological responses, as well as progression-free survival comparable to that with upfront docetaxel, as observed in our patient, underscore the potential utility of 177Lu-PSMA-617 in high-volume mHSPC.
Click to Show/Hide
|
||||
| Description |
He showed remarkable symptomatic improvement, with complete resolution of pain by 6 wk following the first cycle, and his ECOG performance score improved to zero. At 12 wk after the second cycle, his serum PSA had decreased from 100 ng/ml to 0.25 ng/ml (99.8% reduction from baseline) and repeat 68Ga-PSMA-11 PET/CT showed a near-complete molecular response with a marked reduction in the extent and tracer avidity of the lesions.
Click to Show/Hide
|
||||
| In Vivo Model | 68-year-old male with newly diagnosed high-volume metastatic hormone-sensitive prostate cancer. | ||||
| Experiment 466 Reporting the Activity Data of This PDC | [81] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | PSA decline rate |
100%
|
|||
| Description |
The -fetoprotein serum level increased from 248 to 578 kUI/L after the second treatment. We concluded that the prostatic disease exhibited a positive response to 177Lu PSMA-617, evidenced by a significant decrease in PSA serum levels (from 1.26 ng/mL to undetectable levels after the second treatment). However, there was no observable effect on HCC nodules, prompting the patients readmission for chemoembolization. Notably, there is a high PSMA expression in various solid tumors neovessels, among others HCC.
Click to Show/Hide
|
||||
| In Vivo Model | A 69-year-old man diagnosed with progressive bone metastatic castration-resistant prostate adenocarcinoma and concurrent alcoholic cirrhosis with multiple hepatocellular carcinoma (HCC). | ||||
| Experiment 467 Reporting the Activity Data of This PDC | [82] | ||||
| Indication | Adenocarcinoma prostate | ||||
| Efficacy Data | PSA level |
0.3 ng/mL
|
|||
| Administration Dosage | 10.36 GBq (280 mCi) | ||||
| Description |
Patient underwent 68Ga-labeled PSMA PET/CT scan after 8 weeks of PSMA-RLT, which revealed complete resolution of bilateral pelvic lymph nodes and PSMA-avid lesions in the prostate. Meanwhile, patients PSA levels have also dropped to 0.3 ng/mL.
|
||||
| In Vivo Model | 61-year-old man diagnosed with adenocarcinoma prostate. | ||||
| Experiment 468 Reporting the Activity Data of This PDC | [45] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | PSA progression |
15%
|
|||
| Patients Enrolled |
23 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 16 week | ||||
| Administration Dosage | 6 GBq (162.16 mCi) | ||||
| MOA of PDC |
This study shows that PSA changes in patients with mCRPC as early as four weeks after the first administration of PSMA-RLT are predictive of both long-term biochemical and PET imaging responses, as well as overall survival. At this early stage, a PSA decrease of at least 30% was found to be more suitable to detect future responders, as well as a longer overall survival compared to the threshold of 50% proposed by the PCWG for long-term biochemical evaluation. An early increase in PSA (+25%) is a strong predictor for biochemical progression and shorter overall survival. Larger prospective studies are warranted to validate these findings and provide criteria for the early assessment of PSMA-RLT, including even more lenient thresholds, as suggested by our explorative retrospective ROC analysis.
Click to Show/Hide
|
||||
| Description |
At w16, 16 patients (59%) achieved a biochemical response according to the PCWG3 criteria (mean %PSAw16 -77 ± 13). Four patients (15%) displayed PSA progression (mean %PSAw16 103 ± 62), and three patients were biochemically stable (mean %PSAw16 -19 ± 22). In all patients, the biochemical response status was confirmed in the PSA follow-up. %PSAw16 had no correlation to previous treatments or other relevant pretherapeutic parameters (p ≥ 0.15)
Click to Show/Hide
|
||||
| Experiment 469 Reporting the Activity Data of This PDC | [12] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | PSA progression rate |
51%
|
|||
| Patients Enrolled |
61 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | Median 4 (iqr: 2-6) cycles | ||||
| Administration Dosage | Median 800 (IQR: 470-1150) mCi | ||||
| MOA of PDC |
In conclusion, the current study was the first to demonstrate that pretreatment NLR, MLR, PLR and SII are powerful independent prognostic indices predicting survival in patients with mCRPC receiving 177Lu-PSMA-617 therapy. A large-scale prospective study is warranted to confirm the preliminary results obtained in this study.
|
||||
| Description |
Mean follow-up time was 53.2±24 months. While there were 61 patients at the baseline, 46 (75%) patients were able to complete the fourth cycle, and 18 (30%) patients were able to complete the eighth cycle. Median 4 (IQR: 2-6) cycles and 800 (IQR: 470-1150) mCi 177Lu-PSMA-617 were applied. During the 177Lu-PSMA-617 therapy period, androgen receptor signaling inhibitor was continued in 8 (13%) patients and chemotherapy was continued in 3 (5%) patients. According to the PCWG3 PSA response patterns, 18 (30%) patients had fitted into pattern 1 (PSA reduction of 50% or more from baseline and sustained), 12 (20%) patients into pattern 2 (PSA decrease of more than 50% followed by a modest rise), and 31 (51%) patients into pattern 3 (PSA progression of more than 25%). No significant difference was found between PSA patterns according to baseline inflammation indices (P values for NLR, dNLR, MLR, PLR, SII, PIV were.298,.105,.137,.774,.727,.944, respectively).
Click to Show/Hide
|
||||
| Experiment 470 Reporting the Activity Data of This PDC | [36] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Rate of adverse events |
52.70%
|
|||
| Patients Enrolled |
1192 patients with metastatic castration-resistant prostate cancer.
|
||||
| Description |
177Lu PSMA-617 has been shown to have a low, but significant, rate of adverse events (AE) in several clinical studies. In the phase III VISION study, 52.7% of patients experienced a grade 3 or higher AE, as compared to 38.0% of patients with similar events in the control group. Anemia was the most common grade ≥3 AE, observed in 12.9% of subjects
Click to Show/Hide
|
||||
| Experiment 471 Reporting the Activity Data of This PDC | [19] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Rate of ECOG decline |
47%
|
|||
| Patients Enrolled |
25 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | A median of four (iqr: 2-6) cycles every 6-8 weeks | ||||
| Administration Dosage | Mean of 7.7 ± 1.4 GBq/cycle | ||||
| MOA of PDC |
The response to radioligand therapy with 177Lu-PSMA-617 seems to be independent of the presence of early-onset prostate cancer (EOPC); however, the less favorable survival outcome observed in our study may indicate a more aggressive disease course. Expectedly, the safety of LuPSMA-RLT does not seem to be compromised in metastasized castration-resistant EOPC patients. Comparative studies on age at diagnosis of prostate cancer and the patients outcome after LuPSMA-RLT are needed.
Click to Show/Hide
|
||||
| Description |
Intra- or post-therapeutic toxicity was graded according to the CTCAE v5.0 criteria. Newly developing grade ≥ 3 anemia, leukopenia, and thrombocytopenia occurred in three (12%), one (4%), and three (12%) patients, respectively. One patient showed renal toxicity (grade ≥ 3) during follow-up. Pain palliation (>2 level VAS decline) was achieved in 9/14 (64%) and performance status improvement (ECOG level decline ≥ 1) in 8/17 (47%) of patients.
Click to Show/Hide
|
||||
| Experiment 472 Reporting the Activity Data of This PDC | [41] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Rate of intracranial hemorrhage |
0.20%
|
|||
| Patients Enrolled |
734 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 5 doses (range: 1 to 6) | ||||
| Administration Dosage | Median cumulative dose 37.5 GBq (range, 7.0 to 48.3) | ||||
| MOA of PDC |
On March 23, 2022, the FDA approved 177Lu-PSMA-617 for the treatment of adult patients with PSMA-positive mCRPC who have been treated with androgen receptor pathway inhibition and taxane-based chemotherapy. The approval was based on a meaningful advantage in overall survival supported by a delay in tumor progression and higher objective response rate. The decision took into account several important factors unique to this applications context. Metastatic castration-resistant prostate cancer (mCRPC) is a life-threatening condition that lacks curative treatment, creating an unmet need. This product provides a novel mechanism of action as the first radioligand therapeutic agent for mCRPC providing anti-tumor effects in both bone and non-bone sites and may provide an opportunity to be combined with other available therapies with different toxicity profiles across mechanistic classes. Finally, 177Lu-PSMA-617 offers a different safety profile than other available systemic therapies which was determined to be acceptable for the indicated patient population, expanding treatment options that can be individualized to a patients preferences and comorbidities.
Click to Show/Hide
|
||||
| Description |
Serious adverse reactions occurred in 36% of patients who received 177Lu-PSMA-617 plus BSoC. Fatal adverse reactions occurred in 2.8% of patients who received 177Lu-PSMA-617 plus BSoC, including sepsis (0.9%), pancytopenia (0.6%), hepatic failure (0.4%), intracranial hemorrhage (0.2%), subdural hematoma (0.2%), ischemic stroke (0.2%), COVID-19 (0.2%), and aspiration pneumonia (0.2%). The 2 fatal adverse reactions of intracranial hemorrhage and subdural hematoma occurred in patients who had concurrent treatment-related thrombocytopenia. The most common adverse reactions (≥ 20%) occurring at a higher incidence in patients who received 177Lu-PSMA-617 plus BSoC were fatigue, dry mouth, nausea, anemia, decreased appetite, and constipation. The most common laboratory abnormalities that worsened from baseline in ≥ 30% of patients who received 177Lu-PSMA-617 plus BSoC were decreased lymphocytes, decreased hemoglobin, decreased leukocytes, decreased platelets, decreased calcium, and decreased sodium.
Click to Show/Hide
|
||||
| Experiment 473 Reporting the Activity Data of This PDC | [41] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Rate of ischemic stroke |
0.20%
|
|||
| Patients Enrolled |
734 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 5 doses (range: 1 to 6) | ||||
| Administration Dosage | Median cumulative dose 37.5 GBq (range, 7.0 to 48.3) | ||||
| MOA of PDC |
On March 23, 2022, the FDA approved 177Lu-PSMA-617 for the treatment of adult patients with PSMA-positive mCRPC who have been treated with androgen receptor pathway inhibition and taxane-based chemotherapy. The approval was based on a meaningful advantage in overall survival supported by a delay in tumor progression and higher objective response rate. The decision took into account several important factors unique to this applications context. Metastatic castration-resistant prostate cancer (mCRPC) is a life-threatening condition that lacks curative treatment, creating an unmet need. This product provides a novel mechanism of action as the first radioligand therapeutic agent for mCRPC providing anti-tumor effects in both bone and non-bone sites and may provide an opportunity to be combined with other available therapies with different toxicity profiles across mechanistic classes. Finally, 177Lu-PSMA-617 offers a different safety profile than other available systemic therapies which was determined to be acceptable for the indicated patient population, expanding treatment options that can be individualized to a patients preferences and comorbidities.
Click to Show/Hide
|
||||
| Description |
Serious adverse reactions occurred in 36% of patients who received 177Lu-PSMA-617 plus BSoC. Fatal adverse reactions occurred in 2.8% of patients who received 177Lu-PSMA-617 plus BSoC, including sepsis (0.9%), pancytopenia (0.6%), hepatic failure (0.4%), intracranial hemorrhage (0.2%), subdural hematoma (0.2%), ischemic stroke (0.2%), COVID-19 (0.2%), and aspiration pneumonia (0.2%). The 2 fatal adverse reactions of intracranial hemorrhage and subdural hematoma occurred in patients who had concurrent treatment-related thrombocytopenia. The most common adverse reactions (≥ 20%) occurring at a higher incidence in patients who received 177Lu-PSMA-617 plus BSoC were fatigue, dry mouth, nausea, anemia, decreased appetite, and constipation. The most common laboratory abnormalities that worsened from baseline in ≥ 30% of patients who received 177Lu-PSMA-617 plus BSoC were decreased lymphocytes, decreased hemoglobin, decreased leukocytes, decreased platelets, decreased calcium, and decreased sodium.
Click to Show/Hide
|
||||
| Experiment 474 Reporting the Activity Data of This PDC | [83] | ||||
| Indication | ATM-mutated metastatic castration resistant prostate cancer | ||||
| Efficacy Data | Rate of PSA <0.2 ng/mL |
25%
|
|||
| Patients Enrolled |
140 patients wit high-volume metastatic hormone-naive prostate cancer.
|
||||
| Administration Time | 2 cycles | ||||
| Administration Dosage | 7.5 GBq | ||||
| Description |
The primary endpoint of this study is undetectable PSA (PSA ≤0.2 ng/mL) at 12 months after initiation of protocol therapy. In the CHAARTED study, 27% of all mHNPC patients treated with ADT+ docetaxel attained a PSA ≤0.2 ng/mL at 12 months. We have assumed that 25% of patients in the control arm (Arm B) will have PSA ≤0.2 ng/mL at 12 months. With 140 patients randomized 1:1 between the treatment arms, the study will have 85% power to reject the null hypothesis that the 12-month undetectable PSA rate is the same between the arms if the true 12-month undetectable PSA rate in the experimental arm (Arm A) is 50%.
Click to Show/Hide
|
||||
| Related Clinical Trial | |||||
| NCT Number | NCT04343885 | Clinical Status | Phase 2 | ||
| Clinical Description | This phase 2 randomised clinical trial will compare the effectiveness of Lu-PSMA therapy followed by docetaxel chemotherapy versus docetaxel chemotherapy on its own in patients with newly-diagnosed high-volume metastatic hormone-naive prostate cancer (mHNPC). | ||||
| Experiment 475 Reporting the Activity Data of This PDC | [78] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Rate of PSA increase |
19.70%
|
|||
| Patients Enrolled |
61 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | T hree cycles at four weekly intervals | ||||
| Administration Dosage | Mean 7321 ± 592 MBq | ||||
| Description |
Forty-nine (80.3%) patients demonstrated a therapy response in terms of any PSA decline, while 21 (19.7%) patients showed increase or no changes in their PSA levels.
|
||||
| Experiment 476 Reporting the Activity Data of This PDC | [77] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Reduction in liver lesion volume |
99%
|
|||
| Patients Enrolled |
30 patients with proven metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 5 cycles of treatment with 177lu-psma-617 prlt | ||||
| Administration Dosage | 4.94 ± 0.45 GBq/cycle | ||||
| Evaluation Method | 68Ga-PSMA-11 PET-CT assay | ||||
| Description |
The response of 177Lu-PSMA-617 therapy in one of the study patients, which was evaluated by comparing the 68Ga-PSMA-11 PET-CT recorded before each therapy cycle, and from this figure, it is evident that there is drastic reduction (99%) in liver lesion volume after four treatment cycles.
|
||||
| Experiment 477 Reporting the Activity Data of This PDC | [41] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Sepsis |
0.90%
|
|||
| Patients Enrolled |
734 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 5 doses (range: 1 to 6) | ||||
| Administration Dosage | Median cumulative dose 37.5 GBq (range, 7.0 to 48.3) | ||||
| MOA of PDC |
On March 23, 2022, the FDA approved 177Lu-PSMA-617 for the treatment of adult patients with PSMA-positive mCRPC who have been treated with androgen receptor pathway inhibition and taxane-based chemotherapy. The approval was based on a meaningful advantage in overall survival supported by a delay in tumor progression and higher objective response rate. The decision took into account several important factors unique to this applications context. Metastatic castration-resistant prostate cancer (mCRPC) is a life-threatening condition that lacks curative treatment, creating an unmet need. This product provides a novel mechanism of action as the first radioligand therapeutic agent for mCRPC providing anti-tumor effects in both bone and non-bone sites and may provide an opportunity to be combined with other available therapies with different toxicity profiles across mechanistic classes. Finally, 177Lu-PSMA-617 offers a different safety profile than other available systemic therapies which was determined to be acceptable for the indicated patient population, expanding treatment options that can be individualized to a patients preferences and comorbidities.
Click to Show/Hide
|
||||
| Description |
Serious adverse reactions occurred in 36% of patients who received 177Lu-PSMA-617 plus BSoC. Fatal adverse reactions occurred in 2.8% of patients who received 177Lu-PSMA-617 plus BSoC, including sepsis (0.9%), pancytopenia (0.6%), hepatic failure (0.4%), intracranial hemorrhage (0.2%), subdural hematoma (0.2%), ischemic stroke (0.2%), COVID-19 (0.2%), and aspiration pneumonia (0.2%). The 2 fatal adverse reactions of intracranial hemorrhage and subdural hematoma occurred in patients who had concurrent treatment-related thrombocytopenia. The most common adverse reactions (≥ 20%) occurring at a higher incidence in patients who received 177Lu-PSMA-617 plus BSoC were fatigue, dry mouth, nausea, anemia, decreased appetite, and constipation. The most common laboratory abnormalities that worsened from baseline in ≥ 30% of patients who received 177Lu-PSMA-617 plus BSoC were decreased lymphocytes, decreased hemoglobin, decreased leukocytes, decreased platelets, decreased calcium, and decreased sodium.
Click to Show/Hide
|
||||
| Experiment 478 Reporting the Activity Data of This PDC | [84] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Serum creatinine level |
0.8 mg/dL
|
|||
| Patients Enrolled |
Patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 5 cycles | ||||
| Administration Dosage | 4 GBq/cycle | ||||
| Description |
However, excellent response was noted and serum creatinine level of 0.8 mg/dL remained stable.
|
||||
| Experiment 479 Reporting the Activity Data of This PDC | [41] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Sodium decrease rate | ≥ 30% | |||
| Patients Enrolled |
734 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 5 doses (range: 1 to 6) | ||||
| Administration Dosage | Median cumulative dose 37.5 GBq (range, 7.0 to 48.3) | ||||
| MOA of PDC |
On March 23, 2022, the FDA approved 177Lu-PSMA-617 for the treatment of adult patients with PSMA-positive mCRPC who have been treated with androgen receptor pathway inhibition and taxane-based chemotherapy. The approval was based on a meaningful advantage in overall survival supported by a delay in tumor progression and higher objective response rate. The decision took into account several important factors unique to this applications context. Metastatic castration-resistant prostate cancer (mCRPC) is a life-threatening condition that lacks curative treatment, creating an unmet need. This product provides a novel mechanism of action as the first radioligand therapeutic agent for mCRPC providing anti-tumor effects in both bone and non-bone sites and may provide an opportunity to be combined with other available therapies with different toxicity profiles across mechanistic classes. Finally, 177Lu-PSMA-617 offers a different safety profile than other available systemic therapies which was determined to be acceptable for the indicated patient population, expanding treatment options that can be individualized to a patients preferences and comorbidities.
Click to Show/Hide
|
||||
| Description |
Serious adverse reactions occurred in 36% of patients who received 177Lu-PSMA-617 plus BSoC. Fatal adverse reactions occurred in 2.8% of patients who received 177Lu-PSMA-617 plus BSoC, including sepsis (0.9%), pancytopenia (0.6%), hepatic failure (0.4%), intracranial hemorrhage (0.2%), subdural hematoma (0.2%), ischemic stroke (0.2%), COVID-19 (0.2%), and aspiration pneumonia (0.2%). The 2 fatal adverse reactions of intracranial hemorrhage and subdural hematoma occurred in patients who had concurrent treatment-related thrombocytopenia. The most common adverse reactions (≥ 20%) occurring at a higher incidence in patients who received 177Lu-PSMA-617 plus BSoC were fatigue, dry mouth, nausea, anemia, decreased appetite, and constipation. The most common laboratory abnormalities that worsened from baseline in ≥ 30% of patients who received 177Lu-PSMA-617 plus BSoC were decreased lymphocytes, decreased hemoglobin, decreased leukocytes, decreased platelets, decreased calcium, and decreased sodium.
Click to Show/Hide
|
||||
| Experiment 480 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Stable disease (SD) |
14%
|
|||
| Patients Enrolled |
14 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | Up to 3 cycles every six weeks | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
A prospective phase II pilot study enrolled fourteen patients with progressive and symptomatic mCRPC despite taxane and novel anti-androgen therapy to receive up to four cycles of 177Lu PSMA-617 every six weeks. Ten out of the 14 patients had a mean PSA reduction of 59%, with five patients having over a 50% reduction, and nine patients having over a 30% reduction in PSA levels. At baseline testing, the PSMA PET SUV predicted a reduction in PSA of more than 30%, with an SUV max value of 17 ± 9 compared to 44 ± 15 (p < 0.007), and a PSMA SUV mean of 6 ± 4 compared to 10 ± 4 (p < 0.04).
Click to Show/Hide
|
||||
| Experiment 481 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Stable disease (SD) |
7.10%
|
|||
| Patients Enrolled |
50 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | A median of 3 cycles | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
Fifty patients were studied prospectively with PSMA-avid prostate cancer metastases who underwent a median of three cycles (range 1-4) of 177Lu PSMA-617 therapy. Nine were deemed 177Lu PSMA-617 refractory prior to death with a total of twelve deaths in the study. A PSA decline was noted in 23 patients, with 11 patients having a PSA decline of ≥50% after the first cycle of treatment. 12 patients had a PSA decline of <50% ranging from 11.3 to 43.5%. The remaining 23 patients experienced a PSA increase after the first 177Lu PSMA-617 cycle (range 19.7-100%).
Click to Show/Hide
|
||||
| Experiment 482 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Stable disease (SD) |
8%
|
|||
| Patients Enrolled |
56 patients with metastatic castration-resistant prostate cancer.
|
||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
Another prospective trial studied 56 patients with progressive mCRPC and rising PSA levels who then received 177Lu-PSMA. Clinical efficacy was assessed using the visual analogue scale for pain, PSA levels, median overall survival, and Gallium-68-labeled prostate-specific membrane antigen (68Ga-PSMA PET/CT) for objective response. There was a decline in PSA of greater than 80% in 23.2% of patients, a decline of greater than 50% in 58.9%, and a decline of greater than 30% in 66.1% of patients. Progressive disease was noted in 10.7% of patients with a rise in PSA level greater than 25%. 68Ga-PSMA PET/CT prior to PSMA radioligand therapy showed the median SUVmax of the target lesion to be 37.5, which decreased to 15.7 after PSMA RLT. Ga-PSMA PET/CT was used to measure response rates which included a partial remission in 56%, stable disease in 8%, and progressive disease in 36% of patients. The median progression-free survival was 13.7 months, and median overall survival was not reached. PET/CT results showing a decrease in SUV max of the target lesion are indicative of a favorable objective response to Lu-PSMA therapy.
Click to Show/Hide
|
||||
| Experiment 483 Reporting the Activity Data of This PDC | [48] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Stable disease (SD) |
10.60%
|
|||
| Patients Enrolled |
Patients with metastatic castration-resistant prostate cancer who underwent 68Ga-PSMA and FDG PET-CT scans.
|
||||
| Evaluation Method | 68Ga-PSMA/18F-FDG PET-CT assay | ||||
| Description |
In the period between 2016 and 2018, 58 patients were referred for [177Lu]-PSMA PRLT to the center, of which 51 patients underwent both [68Ga]-PSMA and FDG PET-CT scans and provisionally qualified for the analysis; out of these complete information of four patients was not available and hence were excluded. Thus, 47 patients were retrospectively recruited and categorized according to the proposed Pro-PET scoring scheme and were analyzed as discussed above. The cohort comprised of heavily pretreated patients with 2 (4.3%) underwent radical prostatectomy; surgical castration was performed in 45 (95.7%) patients; first-line hormonal therapy (with estrogen analogues, leutinizing hormone releasing hormone agonists and antagonists and antiandrogens) in 44 (93.6%) patients, second-line hormonal therapy (with CYP17 blockers and newer anti-androgens) in 34 (72.4%) patients; first-line chemotherapy (with docetaxel) in 33 (70.2%) patients, second-line chemotherapy (with cabazitaxel, oral metronomic chemotherapy, etc.) in 22 (46.8%) and radiotherapy in 26 (55.3%) patients.
Click to Show/Hide
|
||||
| Experiment 484 Reporting the Activity Data of This PDC | [52] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Stable disease (SD) |
11%
|
|||
| Patients Enrolled |
19 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 5 (iqr: 3-6) cycles | ||||
| Administration Dosage | A cumulative activity of 32 ± 11 GBq | ||||
| Evaluation Method | 68Ga-PSMA-11 PET/CT assay | ||||
| MOA of PDC |
Intermittent 177Lu-PSMA-617 radioligand therapy in early responders with oligometastatic castration-resistant prostate cancer seems to not compromise survival outcome, despite long treatment-free intervals. The safety profile remained favorable, warranting further investigation of the concept of intermittent treatment in selected patients with a longer life-expectancy.
Click to Show/Hide
|
||||
| Description |
Four (21%) patients showed no response (PD) to the 177Lu-PSMA-RLT cycles after the first treatment break, and in two patients (11%), progression after the initial disease stabilization (SD) under subsequent cycles led to treatment discontinuation. Two patients (11%) completed the intended six cycles with a stable disease. In the remaining 11/19 (84%) patients, resuming 177Lu-PSMA-RLT resulted in a repeated PR. Altogether, 14/19 (74%) patients died by the time of this analysis. The median PFS was 27 (95% CI: 23-31) months and the OS was 45 (95% CI: 28-62) months.
Click to Show/Hide
|
||||
| Experiment 485 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Stable disease (SD) |
19%
|
|||
| Patients Enrolled |
21 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | Every 8 weeks | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
Another real-world prospective cohort study included twenty-one treatments refractory mCRPC patients at Bushehr Department of Nuclear Medicine between December 2016 to December 2018 treated with 177Lu-PSMA-617 every 8 weeks. Patients had to have PSMA secreting lesions detected by PSMA imaging with 68Ga-PSMA PET or 177Lu/99Tc-PSMA before to undergoing treatment. The mean age of patients was 70.3 ± 9.6 (range 54-88) with a median of two cycles of treatment (range 1-4). The primary endpoint of the study was to assess biochemical response (BCR), which was defined as a drop in the PSA of more than 50. Additional secondary endpoints included response by ECOG and overall survival. A BCR was seen in 62% of patients. The estimated overall survival was seen to be 62.69 weeks (95% confidence interval: 42.06-83.33) with a median follow-up period of 9 months (range 1-25 months).
Click to Show/Hide
|
||||
| Experiment 486 Reporting the Activity Data of This PDC | [68] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Stable disease (SD) |
23%
|
|||
| Patients Enrolled |
51 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 2 cycles | ||||
| Administration Dosage | 12.9 GBq (range: 9.1-16.9) | ||||
| Evaluation Method | Molecular-imaging based response assessed by SUVpeak | ||||
| MOA of PDC |
68Ga-PSMA-11 PET-derived response assessment based on normalization of tumoral PSMA expression to normal liver tissue (TLR) may be an appropriate biomarker for monitoring 177Lu-PSMA-617 RLT in mCRPC patients and predicting survival outcome (PFS) of this treatment modality. Our study indicates the superiority of using liver-normalized tumor SUV values for molecular response assessment in this setting compared to the use of standard tumor SUV measurements, which are widely practiced at present. However, prospective studies with larger patient cohorts are needed to confirm these initial findings.
Click to Show/Hide
|
||||
| Description |
Thirty-one patients (61%) showed partial biochemical response (PRPSA), 18 patients (35%) stable disease (SDPSA), and two patients (4%) progressive disease (PDPSA). Using molecular-imaging based response assessed by SUVpeak, 37 patients (73%) showed partial response (PRSUV), 12 patients (23%) stable disease (SDSUV), and two patients (4%) progressive disease (PDSUV). Response assessment using TLR gave similar results, with PRTLR in 35 patients (69%), SDTLR in 13 patients (25%), and PDTLR in three patients (6%).
Click to Show/Hide
|
||||
| Experiment 487 Reporting the Activity Data of This PDC | [68] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Stable disease (SD) |
25%
|
|||
| Patients Enrolled |
51 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 2 cycles | ||||
| Administration Dosage | 12.9 GBq (range: 9.1-16.9) | ||||
| Evaluation Method | TLR gave similar results assay | ||||
| MOA of PDC |
68Ga-PSMA-11 PET-derived response assessment based on normalization of tumoral PSMA expression to normal liver tissue (TLR) may be an appropriate biomarker for monitoring 177Lu-PSMA-617 RLT in mCRPC patients and predicting survival outcome (PFS) of this treatment modality. Our study indicates the superiority of using liver-normalized tumor SUV values for molecular response assessment in this setting compared to the use of standard tumor SUV measurements, which are widely practiced at present. However, prospective studies with larger patient cohorts are needed to confirm these initial findings.
Click to Show/Hide
|
||||
| Description |
Thirty-one patients (61%) showed partial biochemical response (PRPSA), 18 patients (35%) stable disease (SDPSA), and two patients (4%) progressive disease (PDPSA). Using molecular-imaging based response assessed by SUVpeak, 37 patients (73%) showed partial response (PRSUV), 12 patients (23%) stable disease (SDSUV), and two patients (4%) progressive disease (PDSUV). Response assessment using TLR gave similar results, with PRTLR in 35 patients (69%), SDTLR in 13 patients (25%), and PDTLR in three patients (6%).
Click to Show/Hide
|
||||
| Experiment 488 Reporting the Activity Data of This PDC | [48] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Stable disease (SD) |
25.50%
|
|||
| Patients Enrolled |
Patients with metastatic castration-resistant prostate cancer who underwent 68Ga-PSMA and FDG PET-CT scans.
|
||||
| Evaluation Method | 68Ga-PSMA/18F-FDG PET-CT assay | ||||
| Description |
In the period between 2016 and 2018, 58 patients were referred for [177Lu]-PSMA PRLT to the center, of which 51 patients underwent both [68Ga]-PSMA and FDG PET-CT scans and provisionally qualified for the analysis; out of these complete information of four patients was not available and hence were excluded. Thus, 47 patients were retrospectively recruited and categorized according to the proposed Pro-PET scoring scheme and were analyzed as discussed above. The cohort comprised of heavily pretreated patients with 2 (4.3%) underwent radical prostatectomy; surgical castration was performed in 45 (95.7%) patients; first-line hormonal therapy (with estrogen analogues, leutinizing hormone releasing hormone agonists and antagonists and antiandrogens) in 44 (93.6%) patients, second-line hormonal therapy (with CYP17 blockers and newer anti-androgens) in 34 (72.4%) patients; first-line chemotherapy (with docetaxel) in 33 (70.2%) patients, second-line chemotherapy (with cabazitaxel, oral metronomic chemotherapy, etc.) in 22 (46.8%) and radiotherapy in 26 (55.3%) patients.
Click to Show/Hide
|
||||
| Experiment 489 Reporting the Activity Data of This PDC | [22] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Stable disease (SD) |
28%
|
|||
| Patients Enrolled |
145 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 1-4 cycles | ||||
| Administration Dosage | 2-8 GBq/cycle | ||||
| Evaluation Method | PET/CT assay | ||||
| MOA of PDC |
The PSMA molecule acts as a target for theranostics in detecting and treating prostatic lesions. This ultimately promotes the concept of precision and personalized medicine. Several published articles showed favorable outcomes of Lu-PSMA-PRLT in mCRPC patients, which quickly translated into routine clinical practices with real effectiveness, a low toxicity profile, and documentation of the risk-benefit of PRLT. Nevertheless, many questions related to PRLT remain unresolved such as the sequencing of PRLT with ARTA or taxane-based chemotherapy, re-challenge therapy, combined therapy, alpha therapy in mCRPC patients, and early treatment of PRLT in mHNPC patients. To solve these questions, several clinical trials are currently under way, and the results of these trials will be helpful in deciding treatment strategies for prostate cancer patients.
Click to Show/Hide
|
||||
| Description |
The first major multi-center retrospective study on 177Lu-PSMA-617 was published by Rahbar et al., reporting 145 patients with mCRPC who progressed after second-line systemic therapies. The overall response rate in terms of serum PSA decline >50% was seen in 45% of patients after all 177Lu-PSMA-617 cycles. On imaging, 21 (45%) patients and 13 (28%) patients had PR and SD, respectively. There was grade 3-4 toxicity in 18 patients (13%), which included severe anemia, thrombocytopenia, and leukopenia. They found elevated alkaline phosphatase and visceral metastases as negative predictors of response to 177Lu-PSMA-617. A major drawback of this study was the variable cycles and doses of 177Lu-PSMA-617 given to patients
Click to Show/Hide
|
||||
| Experiment 490 Reporting the Activity Data of This PDC | [48] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Stable disease (SD) |
31.90%
|
|||
| Patients Enrolled |
Patients with metastatic castration-resistant prostate cancer who underwent 68Ga-PSMA and FDG PET-CT scans.
|
||||
| Evaluation Method | 68Ga-PSMA/18F-FDG PET-CT assay | ||||
| Description |
In the period between 2016 and 2018, 58 patients were referred for [177Lu]-PSMA PRLT to the center, of which 51 patients underwent both [68Ga]-PSMA and FDG PET-CT scans and provisionally qualified for the analysis; out of these complete information of four patients was not available and hence were excluded. Thus, 47 patients were retrospectively recruited and categorized according to the proposed Pro-PET scoring scheme and were analyzed as discussed above. The cohort comprised of heavily pretreated patients with 2 (4.3%) underwent radical prostatectomy; surgical castration was performed in 45 (95.7%) patients; first-line hormonal therapy (with estrogen analogues, leutinizing hormone releasing hormone agonists and antagonists and antiandrogens) in 44 (93.6%) patients, second-line hormonal therapy (with CYP17 blockers and newer anti-androgens) in 34 (72.4%) patients; first-line chemotherapy (with docetaxel) in 33 (70.2%) patients, second-line chemotherapy (with cabazitaxel, oral metronomic chemotherapy, etc.) in 22 (46.8%) and radiotherapy in 26 (55.3%) patients.
Click to Show/Hide
|
||||
| Experiment 491 Reporting the Activity Data of This PDC | [68] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Stable disease (SD) |
35%
|
|||
| Patients Enrolled |
51 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 2 cycles | ||||
| Administration Dosage | 12.9 GBq (range: 9.1-16.9) | ||||
| MOA of PDC |
68Ga-PSMA-11 PET-derived response assessment based on normalization of tumoral PSMA expression to normal liver tissue (TLR) may be an appropriate biomarker for monitoring 177Lu-PSMA-617 RLT in mCRPC patients and predicting survival outcome (PFS) of this treatment modality. Our study indicates the superiority of using liver-normalized tumor SUV values for molecular response assessment in this setting compared to the use of standard tumor SUV measurements, which are widely practiced at present. However, prospective studies with larger patient cohorts are needed to confirm these initial findings.
Click to Show/Hide
|
||||
| Description |
Thirty-one patients (61%) showed partial biochemical response (PRPSA), 18 patients (35%) stable disease (SDPSA), and two patients (4%) progressive disease (PDPSA). Using molecular-imaging based response assessed by SUVpeak, 37 patients (73%) showed partial response (PRSUV), 12 patients (23%) stable disease (SDSUV), and two patients (4%) progressive disease (PDSUV). Response assessment using TLR gave similar results, with PRTLR in 35 patients (69%), SDTLR in 13 patients (25%), and PDTLR in three patients (6%).
Click to Show/Hide
|
||||
| Experiment 492 Reporting the Activity Data of This PDC | [22], [26] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Stable disease (SD) |
38.30%
|
|||
| Patients Enrolled |
175 metastatic castration-resistant prostate cancer (mCRPC) patient were included in this meta-analysis. 65 (37.2%) patients experienced partial remission, 67 had stable disease (38.3%), and 43 (24.5%) had progressive disease.
|
||||
| Administration Dosage | 3.7-8.7 GBq/cycle | ||||
| Evaluation Method | PET/CT assay | ||||
| MOA of PDC |
The PSMA molecule acts as a target for theranostics in detecting and treating prostatic lesions. This ultimately promotes the concept of precision and personalized medicine. Several published articles showed favorable outcomes of Lu-PSMA-PRLT in mCRPC patients, which quickly translated into routine clinical practices with real effectiveness, a low toxicity profile, and documentation of the risk-benefit of PRLT. Nevertheless, many questions related to PRLT remain unresolved such as the sequencing of PRLT with ARTA or taxane-based chemotherapy, re-challenge therapy, combined therapy, alpha therapy in mCRPC patients, and early treatment of PRLT in mHNPC patients. To solve these questions, several clinical trials are currently under way, and the results of these trials will be helpful in deciding treatment strategies for prostate cancer patients.
Click to Show/Hide
|
||||
| Description |
Yadav et al. provided a meta-analysis of 177Lu-PSMA-PRLT for treating mCRPC patients. They analyzed 16 articles (13 articles used 177Lu-PSMA-617, 2 articles used 177Lu-PSMA-I&T, and 1 article used both radioligands). The authors showed >50% PSA decline after 177Lu-PSMA-PRLT in 46% of patients. Anatomical imaging response as per the RECIST criteria was reported by eight studies, with a proportion of 37.2% of patients had PR, SD in 38.3% of patients and PD in 24.5% of patients, whereas molecular imaging response as per the PERCIST criteria demonstrated PR in 74 patients (44.3%), SD in 39 patients (23.4%), and PD in 54 patients (32.3%). Common clinical toxicities were grades 1-2, which included anemia (23%), leukopenia (14.2%), thrombocytopenia (15%), nephrotoxicity (9.5%), and xerostomia (14.5%). The authors observed significant heterogeneity in several studies while analyzing this meta-analysis. They concluded that 177Lu-PSMA-PRLT is a promising treatment modality in mCRPC patients who showed PD after standard care treatments.
Click to Show/Hide
|
||||
| Experiment 493 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Stable disease (SD) |
39.10%
|
|||
| Patients Enrolled |
36 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 2 cycles | ||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
A retrospective single center study looked at therapeutic outcomes of 177Lu-PSMA-617 in mCRPC based on post-treatment imaging findings. 36 patients (aged 67 ± 8.8 years) were included out of which 23 received 2 cycles of treatment. Eleven patients (47.8%) were considered responsive in the post-therapeutic scans by 177Lu-PSMA-617, two of which experienced complete response. Nine (39.1%) patients had stable disease while three (13%) experienced disease progression.
Click to Show/Hide
|
||||
| Experiment 494 Reporting the Activity Data of This PDC | [48] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Stable disease (SD) |
51.10%
|
|||
| Patients Enrolled |
Patients with metastatic castration-resistant prostate cancer who underwent 68Ga-PSMA and FDG PET-CT scans.
|
||||
| Evaluation Method | 68Ga-PSMA/18F-FDG PET-CT assay | ||||
| Description |
In the period between 2016 and 2018, 58 patients were referred for [177Lu]-PSMA PRLT to the center, of which 51 patients underwent both [68Ga]-PSMA and FDG PET-CT scans and provisionally qualified for the analysis; out of these complete information of four patients was not available and hence were excluded. Thus, 47 patients were retrospectively recruited and categorized according to the proposed Pro-PET scoring scheme and were analyzed as discussed above. The cohort comprised of heavily pretreated patients with 2 (4.3%) underwent radical prostatectomy; surgical castration was performed in 45 (95.7%) patients; first-line hormonal therapy (with estrogen analogues, leutinizing hormone releasing hormone agonists and antagonists and antiandrogens) in 44 (93.6%) patients, second-line hormonal therapy (with CYP17 blockers and newer anti-androgens) in 34 (72.4%) patients; first-line chemotherapy (with docetaxel) in 33 (70.2%) patients, second-line chemotherapy (with cabazitaxel, oral metronomic chemotherapy, etc.) in 22 (46.8%) and radiotherapy in 26 (55.3%) patients.
Click to Show/Hide
|
||||
| Experiment 495 Reporting the Activity Data of This PDC | [3] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Stable disease (SD) |
52%
|
|||
| Patients Enrolled |
56 patients with metastatic castration-resistant prostate cancer.
|
||||
| MOA of PDC |
177Lu-PSMA-617 has shown promising results in the treatment of men with mCRPC and is likely to play a significant role in the future of prostate cancer management. Repeatedly, this novel therapy has demonstrated a low toxicity profile and appears to be well tolerated in men with refractory metastatic disease. Both retrospective studies and prospective clinical trials have shown to be an effective option for patients with mCRPC following novel hormonal agents and chemotherapy. A limitation to this review is its retrospective nature, which makes it difficult to compare patient populations, dosing cycles, and dose intensities between studies. Amongst the studies, there is also inherent variation in measurement/biomarkers of response, PSMA imaging modalities used, retrospective vs. prospective designs, and small recruitment size. Nonetheless, this systematic review covers the landmark early studies that led to approval of 177Lu-PSMA-617 for mCRPC and highlights the promise of this novel prostate cancer treatment.
Click to Show/Hide
|
||||
| Description |
Another prospective trial studied 56 patients with progressive mCRPC and rising PSA levels who then received 177Lu-PSMA. Clinical efficacy was assessed using the visual analogue scale for pain, PSA levels, median overall survival, and Gallium-68-labeled prostate-specific membrane antigen (68Ga-PSMA PET/CT) for objective response. There was a decline in PSA of greater than 80% in 23.2% of patients, a decline of greater than 50% in 58.9%, and a decline of greater than 30% in 66.1% of patients. Progressive disease was noted in 10.7% of patients with a rise in PSA level greater than 25%. 68Ga-PSMA PET/CT prior to PSMA radioligand therapy showed the median SUVmax of the target lesion to be 37.5, which decreased to 15.7 after PSMA RLT. Ga-PSMA PET/CT was used to measure response rates which included a partial remission in 56%, stable disease in 8%, and progressive disease in 36% of patients. The median progression-free survival was 13.7 months, and median overall survival was not reached. PET/CT results showing a decrease in SUV max of the target lesion are indicative of a favorable objective response to Lu-PSMA therapy.
Click to Show/Hide
|
||||
| Experiment 496 Reporting the Activity Data of This PDC | [22] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Stable disease (SD) |
54%
|
|||
| Patients Enrolled |
90 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 1-7 cycles | ||||
| Administration Dosage | 3.7-8 GBq/cycle | ||||
| Evaluation Method | PET/CT assay | ||||
| MOA of PDC |
The PSMA molecule acts as a target for theranostics in detecting and treating prostatic lesions. This ultimately promotes the concept of precision and personalized medicine. Several published articles showed favorable outcomes of Lu-PSMA-PRLT in mCRPC patients, which quickly translated into routine clinical practices with real effectiveness, a low toxicity profile, and documentation of the risk-benefit of PRLT. Nevertheless, many questions related to PRLT remain unresolved such as the sequencing of PRLT with ARTA or taxane-based chemotherapy, re-challenge therapy, combined therapy, alpha therapy in mCRPC patients, and early treatment of PRLT in mHNPC patients. To solve these questions, several clinical trials are currently under way, and the results of these trials will be helpful in deciding treatment strategies for prostate cancer patients.
Click to Show/Hide
|
||||
| Description |
A favorable response rate (PSA and objective response) and safe profile of 177Lu-PSMA-617 were demonstrated in this study, leading to greater use of Lu-PSMA-PRLT in clinical practices. Similarly, Yadav et al. reported favorable outcomes of 177Lu-PSMA-617 in a prospective, single-arm, single-center study in 90 mCRPC patients.
|
||||
| Experiment 497 Reporting the Activity Data of This PDC | [54] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Stable disease (SD) |
60%
|
|||
| Patients Enrolled |
10 patients with metastatic castration-resistant prostate cancer and with visceral metastasis.
|
||||
| Administration Time | One cycle | ||||
| Administration Dosage | 4.88 GBq | ||||
| Evaluation Method | Prostate-specific antigen (PSA) response assessment assay | ||||
| MOA of PDC |
Lutetium-177-PSMA was a reasonable palliative treatment option with limited toxicity for these end-stage mCRPC patients with visceral metastasis with adequate PSA stabilization. A synergistic drug amalgamation may be an ideal way to boost the outcome in the future.
|
||||
| Description |
Liver (80%), lung (30%), adrenal (10%), and peritoneum (10%) were the sites of visceral metastasis in our study. On PSA response assessment, 10%, 60%, and 30% of the patients had partial response, stable disease, and progressive disease, respectively. Forty percent of the patients had improvement in the VAS, while 50% had improvement in the AQS score. Median PFS was 24 weeks in our study. A cut-off of 4.88GBq of 177Lu-PSMA was the best-predicted progression with 66.67% sensitivity and 100% specificity on ROC analysis. Thirty percent of the patients showed grade 3 anemia. No other significant toxicity was seen.
Click to Show/Hide
|
||||
| Experiment 498 Reporting the Activity Data of This PDC | [41] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Subdural hematoma |
0.20%
|
|||
| Patients Enrolled |
734 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 5 doses (range: 1 to 6) | ||||
| Administration Dosage | Median cumulative dose 37.5 GBq (range, 7.0 to 48.3) | ||||
| MOA of PDC |
On March 23, 2022, the FDA approved 177Lu-PSMA-617 for the treatment of adult patients with PSMA-positive mCRPC who have been treated with androgen receptor pathway inhibition and taxane-based chemotherapy. The approval was based on a meaningful advantage in overall survival supported by a delay in tumor progression and higher objective response rate. The decision took into account several important factors unique to this applications context. Metastatic castration-resistant prostate cancer (mCRPC) is a life-threatening condition that lacks curative treatment, creating an unmet need. This product provides a novel mechanism of action as the first radioligand therapeutic agent for mCRPC providing anti-tumor effects in both bone and non-bone sites and may provide an opportunity to be combined with other available therapies with different toxicity profiles across mechanistic classes. Finally, 177Lu-PSMA-617 offers a different safety profile than other available systemic therapies which was determined to be acceptable for the indicated patient population, expanding treatment options that can be individualized to a patients preferences and comorbidities.
Click to Show/Hide
|
||||
| Description |
Serious adverse reactions occurred in 36% of patients who received 177Lu-PSMA-617 plus BSoC. Fatal adverse reactions occurred in 2.8% of patients who received 177Lu-PSMA-617 plus BSoC, including sepsis (0.9%), pancytopenia (0.6%), hepatic failure (0.4%), intracranial hemorrhage (0.2%), subdural hematoma (0.2%), ischemic stroke (0.2%), COVID-19 (0.2%), and aspiration pneumonia (0.2%). The 2 fatal adverse reactions of intracranial hemorrhage and subdural hematoma occurred in patients who had concurrent treatment-related thrombocytopenia. The most common adverse reactions (≥ 20%) occurring at a higher incidence in patients who received 177Lu-PSMA-617 plus BSoC were fatigue, dry mouth, nausea, anemia, decreased appetite, and constipation. The most common laboratory abnormalities that worsened from baseline in ≥ 30% of patients who received 177Lu-PSMA-617 plus BSoC were decreased lymphocytes, decreased hemoglobin, decreased leukocytes, decreased platelets, decreased calcium, and decreased sodium.
Click to Show/Hide
|
||||
| Experiment 499 Reporting the Activity Data of This PDC | [45] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Survival rate |
19%
|
|||
| Patients Enrolled |
23 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 51 months | ||||
| Administration Dosage | 6 GBq (162.16 mCi) | ||||
| MOA of PDC |
This study shows that PSA changes in patients with mCRPC as early as four weeks after the first administration of PSMA-RLT are predictive of both long-term biochemical and PET imaging responses, as well as overall survival. At this early stage, a PSA decrease of at least 30% was found to be more suitable to detect future responders, as well as a longer overall survival compared to the threshold of 50% proposed by the PCWG for long-term biochemical evaluation. An early increase in PSA (+25%) is a strong predictor for biochemical progression and shorter overall survival. Larger prospective studies are warranted to validate these findings and provide criteria for the early assessment of PSMA-RLT, including even more lenient thresholds, as suggested by our explorative retrospective ROC analysis.
Click to Show/Hide
|
||||
| Description |
Patient follow-up was of over 51 months, with the median follow-up (reverse Kaplan-Meier estimator) being 39.1 months (95% CI 32.1-46.1). Median survival was 12.0 (95% CI 10.8-13.2) months, with five patients (19%) still alive at the last follow-up. There were no therapy-related deaths documented. At w16, 14 patients (52%) stated an improvement in pain status from the baseline of at least one tier/level, 11 of which were biochemical responders.
Click to Show/Hide
|
||||
| Experiment 500 Reporting the Activity Data of This PDC | [40] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Thrombocytopenia |
4.30%
|
|||
| Patients Enrolled |
14 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 140 patients receiving a total of 497 cycles | ||||
| Administration Dosage | 6.9 GBq/cycle | ||||
| MOA of PDC |
Hematologic adverse events after RLT have an acceptable overall incidence and are frequently reversible. High bone tumor burden, previous taxane-based chemotherapy and pretreatment grade 2 cytopenia may be considered as risk factors for developing clinically relevant myelosuppression, whereas cumulative RLT activity and previous 223Ra-dichloride treatment show no significant contribution to incidence rates.
Click to Show/Hide
|
||||
| Description |
Significant (grade ≥ 3) hematologic adverse events occurred in 13 (9.3%) patients, with anemia in 10 (7.1%), leukopenia in 5 (3.6%) and thrombocytopenia in 6 (4.3%). Hematotoxicity was reversible to grade ≤ 2 through a median follow-up of 8 (IQR 9) months in all but two patients who died from disease progression within less than 3 months after RLT.
Click to Show/Hide
|
||||
| Experiment 501 Reporting the Activity Data of This PDC | [14] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Thrombocytopenia |
8%
|
|||
| Patients Enrolled |
831 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | Every 6 weeks for 4-6 cycles | ||||
| MOA of PDC |
Radiopharmaceuticals have been used in prostate cancer for decades with known efficacy in palliation of bone metastasis. The FDA approval of the most recent radiopharmaceutical, 177Lu-PSMA-617, shows a clear overall survival benefit compared to the best SOC. Current studies are ongoing to evaluate the effectiveness of 177Lu-PSMA-617 in earlier lines of therapy, such as after only 1 line of therapy with an ARPI as in the PSMAfore study, or in mCSPC in combination with ADT and an ARPI as in the PSMAddition study. Studies are also ongoing with 177Lu-PSMA-617 in combination with other treatments which may produce a synergistic effect. As described, there are many clinical trials ongoing that are modifying the 177Lu-PSMA-617 to possibly achieve improved results. Studies are also ongoing looking at swapping the 177Lu for another radioactive agent, such as 225Ac (an alpha emitter) which may have benefits over the beta-emitting 177Lu. Other studies are looking at J591, a monoclonal antibody to PSMA which has unique differences compared to small-molecule PSMA binders. Overall, PSMA-based radioligand therapy has been shown to be an effective and life-prolonging therapy and should be considered a treatment option for selected men with mCRPC. As described, there are many ongoing studies further evaluating PSMA radioligand therapy in Australia, South Africa, Europe, and the United States, representing a truly global effort to improve prostate cancer care.
Click to Show/Hide
|
||||
| Description |
Toxicities of grade 3 or higher were experienced by 52.7% of patients. The most common all-grade toxicities with 177Lu-PSMA-617 were fatigue (43.1%), dry mouth (38.8%-0% grade 3 or higher), and nausea (35.3%). The most common grade 3 or higher toxicities included anemia (12.9%), thrombocytopenia (7.9%), and leucopenia (7.8%).
|
||||
| Experiment 502 Reporting the Activity Data of This PDC | [19] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Thrombocytopenia |
12%
|
|||
| Patients Enrolled |
25 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | A median of four (iqr: 2-6) cycles every 6-8 weeks | ||||
| Administration Dosage | Mean of 7.7 ± 1.4 GBq/cycle | ||||
| MOA of PDC |
The response to radioligand therapy with 177Lu-PSMA-617 seems to be independent of the presence of early-onset prostate cancer (EOPC); however, the less favorable survival outcome observed in our study may indicate a more aggressive disease course. Expectedly, the safety of LuPSMA-RLT does not seem to be compromised in metastasized castration-resistant EOPC patients. Comparative studies on age at diagnosis of prostate cancer and the patients outcome after LuPSMA-RLT are needed.
Click to Show/Hide
|
||||
| Description |
Intra- or post-therapeutic toxicity was graded according to the CTCAE v5.0 criteria. Newly developing grade ≥ 3 anemia, leukopenia, and thrombocytopenia occurred in three (12%), one (4%), and three (12%) patients, respectively. One patient showed renal toxicity (grade ≥ 3) during follow-up. Pain palliation (>2 level VAS decline) was achieved in 9/14 (64%) and performance status improvement (ECOG level decline ≥ 1) in 8/17 (47%) of patients.
Click to Show/Hide
|
||||
| Experiment 503 Reporting the Activity Data of This PDC | [42] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Thrombocytopenia |
18%
|
|||
| Patients Enrolled |
45 patients with progressive metastatic castration-resistant prostate cancer and diffuse bone marrow involvement.
|
||||
| Administration Time | 4 cycles | ||||
| Administration Dosage | 7.4 ± 1.4 GBq | ||||
| Evaluation Method | 68Ga-PSMA-11 PET/CT assay | ||||
| MOA of PDC |
Our findings suggest that repeated cycles of RLT with 177Lu-PSMA-617 can be carried out at an acceptable safety profile in mCRPC patients with diffuse bone marrow involvement. RLT may provide a suitable strategy for prolonged disease control with substantial clinical benefit. After a minimum of two cycles, treatment response translated into significantly longer median OS. Further studies should be carried out to investigate the role of individualized RLT concepts in this advanced stage setting.
Click to Show/Hide
|
||||
| Description |
Patients with PR on interim imaging after two cycles had a longer median OS compared to patients with stable or progressive disease (15.5 vs. 7.1 mo, p < 0.001). Previous taxane-based chemotherapy (HR 3.21, 95%CI 1.18-8.70, p = 0.02) and baseline LDH levels (HR 1.001, 95%CI 1.000-1.001, p = 0.04) were inversely associated with OS on a Cox-regression analysis. Grade ≥ 3 hematological decline was observed after 22/201 (11%) cycles with anemia, leukopenia and thrombocytopenia in 15/45 (33%), 6/45 (13%) and 8/45 (18%) patients, respectively.
Click to Show/Hide
|
||||
| Experiment 504 Reporting the Activity Data of This PDC | [14] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Thrombocytopenia |
18%
|
|||
| Patients Enrolled |
200 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | Every 6 weeks (up to 6 cycles) | ||||
| MOA of PDC |
Radiopharmaceuticals have been used in prostate cancer for decades with known efficacy in palliation of bone metastasis. The FDA approval of the most recent radiopharmaceutical, 177Lu-PSMA-617, shows a clear overall survival benefit compared to the best SOC. Current studies are ongoing to evaluate the effectiveness of 177Lu-PSMA-617 in earlier lines of therapy, such as after only 1 line of therapy with an ARPI as in the PSMAfore study, or in mCSPC in combination with ADT and an ARPI as in the PSMAddition study. Studies are also ongoing with 177Lu-PSMA-617 in combination with other treatments which may produce a synergistic effect. As described, there are many clinical trials ongoing that are modifying the 177Lu-PSMA-617 to possibly achieve improved results. Studies are also ongoing looking at swapping the 177Lu for another radioactive agent, such as 225Ac (an alpha emitter) which may have benefits over the beta-emitting 177Lu. Other studies are looking at J591, a monoclonal antibody to PSMA which has unique differences compared to small-molecule PSMA binders. Overall, PSMA-based radioligand therapy has been shown to be an effective and life-prolonging therapy and should be considered a treatment option for selected men with mCRPC. As described, there are many ongoing studies further evaluating PSMA radioligand therapy in Australia, South Africa, Europe, and the United States, representing a truly global effort to improve prostate cancer care.
Click to Show/Hide
|
||||
| Description |
Grade 3-4 AEs occurred in 32 (33%) of men who received 177Lu-PSMA-617 versus 45 (53%) of men in the cabazitaxel group. All-grade toxicities that were more common in the 177Lu-PSMA-617 were dry mouth (60% vs. 21%), dry eyes (30% vs. 4%), and thrombocytopenia (18% vs. 5%). All-grade toxicities that were more common with cabazitaxel were diarrhea (52% vs. 18%), neuropathy (26% vs. 10%), and dysgeusia (27% vs. 12%).
Click to Show/Hide
|
||||
| Experiment 505 Reporting the Activity Data of This PDC | [34] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Thrombocytopenia |
21%
|
|||
| Patients Enrolled |
99 patients with metastatic castration-resistant prostate cancer.
|
||||
| MOA of PDC |
At our center, patients who did not meet the TheraP PSMA imaging criteria or the VISION laboratory criteria benefited from 177Lu-PSMA-617 radioligand therapy.
|
||||
| Description |
Ninety-nine patients were included. Sixty patients achieved a PSA50. Seven of 18 (39%) patients who did not meet the TheraP PSMA imaging criteria achieved a PSA50. Nineteen of 31 (61%) patients who did not meet the VISION laboratory criteria achieved a PSA50. Sixty-three patients had a delay or stoppage in therapy, which was due to a good response in 19 patients and progressive disease in 14 patients. Of 10 patients with a good response who restarted treatment, 9 subsequently achieved a PSA50 on retreatment. The most common toxicities were anemia (33%) and thrombocytopenia (21%).
Click to Show/Hide
|
||||
| Experiment 506 Reporting the Activity Data of This PDC | [35] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Thrombocytopenia |
21.40%
|
|||
| Administration Time | Median of 4 (iqr: 2-7) cycles | ||||
| Administration Dosage | Mean cumulative activity of 30.7 ± 23.4 GBq | ||||
| MOA of PDC |
RLT with 177Lu-PSMA-617 can be effectively and safely initiated as early as 8 weeks after failure of 223Ra in patients with progressive bone-metastatic mCRPC refractory to 223Ra. Objective response can be achieved even in patients with more advanced disease and disseminated/diffuse bone metastases, albeit with increasing incidence of significant hematotoxicity.
Click to Show/Hide
|
||||
| Description |
Grade ≥ 3 hematological toxicity was observed in six patients after their last treatment cycle with anemia, leukopenia and thrombocytopenia in 5/28 (17.9%), 4/28 (14.3%) and 6/28 (21.4%) patients, respectively.
|
||||
| In Vivo Model | 28 men with progressive metastatic castration-resistant prostate cancer who median age 73 years, range 63-89 years). | ||||
| Experiment 507 Reporting the Activity Data of This PDC | [44] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Thrombopenia |
3%
|
|||
| Patients Enrolled |
64 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 2 cycles | ||||
| Administration Dosage | Cumulative mean activity of 11.5 (8.1-14.9) GBq | ||||
| MOA of PDC |
In general, the first two cycles of PSMA-RLT were well tolerated haematologically. Qualitative and quantitative bone marrow impairment appears closely associated with osseous tumour burden as only patients with advanced bone involvement and non-response to therapy exhibited high-grade haematological adverse events as well as a significant mean decline of haematological parameters. This implies that in patients with already advanced mCRPC, non-response to PSMA-RLT may be a major cause of bone marrow impairment during early treatment cycles.
Click to Show/Hide
|
||||
| Description |
In addition, lower grade thrombopenia and leukopenia were observed in 9 (14%) and 11 (17%) patients at baseline, respectively. During the observation period, severe (grade 3) anaemia, thrombopenia and leukopenia occurred in 5 (8%), 2 (3%) and 1 (2%) patients, all of whom suffered from disseminated or diffuse bone involvement according to promise criteria and none of whom experienced biochemical response over the course of therapy
Click to Show/Hide
|
||||
| Experiment 508 Reporting the Activity Data of This PDC | [13] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Tumor Growth Inhibition value (TGI) |
32.30%
|
|||
| Patients Enrolled |
22 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | All treatment cycles | ||||
| Evaluation Method | PET/CT assay | ||||
| Description |
Sixty-three TMVs were identified in the bone, lymph node, and liver tissue with an average reduction of 32.3%, 84.7%, and 72.9%, respectively. Absorbed doses per unit of administered activity for organs and lesions show good agreement with previous works (0.77, 0.71, and 0.27 mGy/MBq for parotid gland, kidneys, and liver as well as 4.38, 5.47, and 4.95 mGy/MBq for bone, lymph node, and liver malignancies, respectively).
Click to Show/Hide
|
||||
| Experiment 509 Reporting the Activity Data of This PDC | [13] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Tumor Growth Inhibition value (TGI) |
72.90%
|
|||
| Patients Enrolled |
22 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | All treatment cycles | ||||
| Evaluation Method | PET/CT assay | ||||
| Description |
Sixty-three TMVs were identified in the bone, lymph node, and liver tissue with an average reduction of 32.3%, 84.7%, and 72.9%, respectively. Absorbed doses per unit of administered activity for organs and lesions show good agreement with previous works (0.77, 0.71, and 0.27 mGy/MBq for parotid gland, kidneys, and liver as well as 4.38, 5.47, and 4.95 mGy/MBq for bone, lymph node, and liver malignancies, respectively).
Click to Show/Hide
|
||||
| Experiment 510 Reporting the Activity Data of This PDC | [13] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Tumor Growth Inhibition value (TGI) |
84.70%
|
|||
| Patients Enrolled |
22 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | All treatment cycles | ||||
| Evaluation Method | PET/CT assay | ||||
| Description |
Sixty-three TMVs were identified in the bone, lymph node, and liver tissue with an average reduction of 32.3%, 84.7%, and 72.9%, respectively. Absorbed doses per unit of administered activity for organs and lesions show good agreement with previous works (0.77, 0.71, and 0.27 mGy/MBq for parotid gland, kidneys, and liver as well as 4.38, 5.47, and 4.95 mGy/MBq for bone, lymph node, and liver malignancies, respectively).
Click to Show/Hide
|
||||
| Experiment 511 Reporting the Activity Data of This PDC | [15] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Visceral metastases |
32%
|
|||
| Patients Enrolled |
Patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 351 cycles | ||||
| Description |
A total of 51 patients (49%) died during the observation period. The majority of patients (97%) presented with bone metastases, 77% with lymph node metastases and 32% with visceral metastases.
|
||||
| Experiment 512 Reporting the Activity Data of This PDC | [54] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Visual relief rate |
40%
|
|||
| Patients Enrolled |
10 patients with metastatic castration-resistant prostate cancer and with visceral metastasis.
|
||||
| Administration Time | One cycle | ||||
| Administration Dosage | 4.88 GBq | ||||
| MOA of PDC |
Lutetium-177-PSMA was a reasonable palliative treatment option with limited toxicity for these end-stage mCRPC patients with visceral metastasis with adequate PSA stabilization. A synergistic drug amalgamation may be an ideal way to boost the outcome in the future.
|
||||
| Description |
Liver (80%), lung (30%), adrenal (10%), and peritoneum (10%) were the sites of visceral metastasis in our study. On PSA response assessment, 10%, 60%, and 30% of the patients had partial response, stable disease, and progressive disease, respectively. Forty percent of the patients had improvement in the VAS, while 50% had improvement in the AQS score. Median PFS was 24 weeks in our study. A cut-off of 4.88GBq of 177Lu-PSMA was the best-predicted progression with 66.67% sensitivity and 100% specificity on ROC analysis. Thirty percent of the patients showed grade 3 anemia. No other significant toxicity was seen.
Click to Show/Hide
|
||||
| Experiment 513 Reporting the Activity Data of This PDC | [14] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Xerophthalmia rate |
30%
|
|||
| Patients Enrolled |
200 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | Every 6 weeks (up to 6 cycles) | ||||
| MOA of PDC |
Radiopharmaceuticals have been used in prostate cancer for decades with known efficacy in palliation of bone metastasis. The FDA approval of the most recent radiopharmaceutical, 177Lu-PSMA-617, shows a clear overall survival benefit compared to the best SOC. Current studies are ongoing to evaluate the effectiveness of 177Lu-PSMA-617 in earlier lines of therapy, such as after only 1 line of therapy with an ARPI as in the PSMAfore study, or in mCSPC in combination with ADT and an ARPI as in the PSMAddition study. Studies are also ongoing with 177Lu-PSMA-617 in combination with other treatments which may produce a synergistic effect. As described, there are many clinical trials ongoing that are modifying the 177Lu-PSMA-617 to possibly achieve improved results. Studies are also ongoing looking at swapping the 177Lu for another radioactive agent, such as 225Ac (an alpha emitter) which may have benefits over the beta-emitting 177Lu. Other studies are looking at J591, a monoclonal antibody to PSMA which has unique differences compared to small-molecule PSMA binders. Overall, PSMA-based radioligand therapy has been shown to be an effective and life-prolonging therapy and should be considered a treatment option for selected men with mCRPC. As described, there are many ongoing studies further evaluating PSMA radioligand therapy in Australia, South Africa, Europe, and the United States, representing a truly global effort to improve prostate cancer care.
Click to Show/Hide
|
||||
| Description |
Grade 3-4 AEs occurred in 32 (33%) of men who received 177Lu-PSMA-617 versus 45 (53%) of men in the cabazitaxel group. All-grade toxicities that were more common in the 177Lu-PSMA-617 were dry mouth (60% vs. 21%), dry eyes (30% vs. 4%), and thrombocytopenia (18% vs. 5%). All-grade toxicities that were more common with cabazitaxel were diarrhea (52% vs. 18%), neuropathy (26% vs. 10%), and dysgeusia (27% vs. 12%).
Click to Show/Hide
|
||||
| Experiment 514 Reporting the Activity Data of This PDC | [14] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Xerostomia |
8%
|
|||
| Patients Enrolled |
145 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 1-4 cycles | ||||
| MOA of PDC |
Radiopharmaceuticals have been used in prostate cancer for decades with known efficacy in palliation of bone metastasis. The FDA approval of the most recent radiopharmaceutical, 177Lu-PSMA-617, shows a clear overall survival benefit compared to the best SOC. Current studies are ongoing to evaluate the effectiveness of 177Lu-PSMA-617 in earlier lines of therapy, such as after only 1 line of therapy with an ARPI as in the PSMAfore study, or in mCSPC in combination with ADT and an ARPI as in the PSMAddition study. Studies are also ongoing with 177Lu-PSMA-617 in combination with other treatments which may produce a synergistic effect. As described, there are many clinical trials ongoing that are modifying the 177Lu-PSMA-617 to possibly achieve improved results. Studies are also ongoing looking at swapping the 177Lu for another radioactive agent, such as 225Ac (an alpha emitter) which may have benefits over the beta-emitting 177Lu. Other studies are looking at J591, a monoclonal antibody to PSMA which has unique differences compared to small-molecule PSMA binders. Overall, PSMA-based radioligand therapy has been shown to be an effective and life-prolonging therapy and should be considered a treatment option for selected men with mCRPC. As described, there are many ongoing studies further evaluating PSMA radioligand therapy in Australia, South Africa, Europe, and the United States, representing a truly global effort to improve prostate cancer care.
Click to Show/Hide
|
||||
| Description |
A larger retrospective multicenter analysis of 145 patients treated with 248 therapy cycles of 177Lu-PSMA-617 at 12 nuclear medicine centers throughout Germany between 2014 and 2015 was conducted. Patients had received 1-4 therapy cycles of treatment. In their analysis, the biochemical response rate (defined as a 50% or greater drop in PSA) was 45% after all therapy cycles. Grade 3 or 4 hematotoxicity occurred in 18 patients (12%) and xerostomia occurred in 11 patients (8%).
Click to Show/Hide
|
||||
| Experiment 515 Reporting the Activity Data of This PDC | [7] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Xerostomia | > 30% | |||
| Administration Time | Every 6 weeks for up to six doses | ||||
| Administration Dosage | 7.4 GBq | ||||
| MOA of PDC |
After binding to the PSMA receptor, [177Lu]Lu-PSMA-617 is internalized into the PSMA positive cells, resulting in a long retention within these cells; the high energy electrons emitted during the decay can selectively induce tissue and DNA damage, leading to cell death.
|
||||
| Description |
As described above, most of the observed toxicities have been low grade, with xerostomia or dry mouth being the most common adverse reactions in >30% of patients.
|
||||
| Half life period | 41.1 ± 9.3 h | ||||
| Experiment 516 Reporting the Activity Data of This PDC | [41] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Xerostomia rate | ≥ 20% | |||
| Patients Enrolled |
734 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | 5 doses (range: 1 to 6) | ||||
| Administration Dosage | Median cumulative dose 37.5 GBq (range, 7.0 to 48.3) | ||||
| MOA of PDC |
On March 23, 2022, the FDA approved 177Lu-PSMA-617 for the treatment of adult patients with PSMA-positive mCRPC who have been treated with androgen receptor pathway inhibition and taxane-based chemotherapy. The approval was based on a meaningful advantage in overall survival supported by a delay in tumor progression and higher objective response rate. The decision took into account several important factors unique to this applications context. Metastatic castration-resistant prostate cancer (mCRPC) is a life-threatening condition that lacks curative treatment, creating an unmet need. This product provides a novel mechanism of action as the first radioligand therapeutic agent for mCRPC providing anti-tumor effects in both bone and non-bone sites and may provide an opportunity to be combined with other available therapies with different toxicity profiles across mechanistic classes. Finally, 177Lu-PSMA-617 offers a different safety profile than other available systemic therapies which was determined to be acceptable for the indicated patient population, expanding treatment options that can be individualized to a patients preferences and comorbidities.
Click to Show/Hide
|
||||
| Description |
Serious adverse reactions occurred in 36% of patients who received 177Lu-PSMA-617 plus BSoC. Fatal adverse reactions occurred in 2.8% of patients who received 177Lu-PSMA-617 plus BSoC, including sepsis (0.9%), pancytopenia (0.6%), hepatic failure (0.4%), intracranial hemorrhage (0.2%), subdural hematoma (0.2%), ischemic stroke (0.2%), COVID-19 (0.2%), and aspiration pneumonia (0.2%). The 2 fatal adverse reactions of intracranial hemorrhage and subdural hematoma occurred in patients who had concurrent treatment-related thrombocytopenia. The most common adverse reactions (≥ 20%) occurring at a higher incidence in patients who received 177Lu-PSMA-617 plus BSoC were fatigue, dry mouth, nausea, anemia, decreased appetite, and constipation. The most common laboratory abnormalities that worsened from baseline in ≥ 30% of patients who received 177Lu-PSMA-617 plus BSoC were decreased lymphocytes, decreased hemoglobin, decreased leukocytes, decreased platelets, decreased calcium, and decreased sodium.
Click to Show/Hide
|
||||
| Experiment 517 Reporting the Activity Data of This PDC | [33] | ||||
| Indication | ATM-mutated metastatic castration resistant prostate cancer | ||||
| Efficacy Data | Xerostomia rate |
24.70%
|
|||
| Patients Enrolled |
121 metastatic castration-resistant prostate cancer patients.
|
||||
| Administration Dosage | Median administered cumulative activity: 20 GBq | ||||
| MOA of PDC |
177Lu-PSMA-617 RLT is an effective form of therapy in mCRPC patients and confirms the findings of the short-term studies. 177Lu-PSMA-617 prolongs the overall survival in mCRPC patients heavily pre-treated with chemotherapy, first and second-line anti-androgens, and androgen inhibitor therapies. The delayed toxicity is low and acceptable by most of these patients. Patients who were treated with various other mCRPC-approved compounds before 177Lu-PSMA-RLT were associated with a significantly shorter OS than that of the patients who received 177Lu-PSMA RLT at the earlier stages of mCRPC. An aggressive treatment approach, either sequential or in combination with second-generation anti-androgens, chemotherapies, or with investigational 225Ac-PSMA-617 alpha therapies, might prolong the survival of mCRPC patients in the future.
Click to Show/Hide
|
||||
| Description |
The median administered cumulative activity was 20 GBq (3.7-37 GBq). The median follow-up duration was 36 months (6-72 months). The estimated median PFS and OS were 12 months (mo) (95% CI: 10.3-13 mo) and 16 mo (95% CI: 13-17 mo), respectively. Any PSA decline and PSA decline >50% was achieved in 73% and 61% of the patients, respectively. Multivariate analysis revealed only failure to achieve >50% PSA decline as a significant factor associated with a poor PFS. Prognostic factors associated with reduced OS included, failure to experience >50% PSA decline, heavily pre-treated patient cohort who received >2 lines of prior treatment options, and patient sub-group treated with ≥2 lines of chemotherapy. Patients re-treated with additional treatment options after attaining 177Lu-PSMA refractory disease showed a remarkably prolonged OS. A significant clinical benefit was achieved post 177Lu-PSMA-617 RLT. The most common toxicities observed were fatigue (34.7%), followed by nausea (33%), and dry mouth (24.7%).
Click to Show/Hide
|
||||
| Experiment 518 Reporting the Activity Data of This PDC | [14] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Xerostomia rate |
60%
|
|||
| Patients Enrolled |
200 patients with metastatic castration-resistant prostate cancer.
|
||||
| Administration Time | Every 6 weeks (up to 6 cycles) | ||||
| MOA of PDC |
Radiopharmaceuticals have been used in prostate cancer for decades with known efficacy in palliation of bone metastasis. The FDA approval of the most recent radiopharmaceutical, 177Lu-PSMA-617, shows a clear overall survival benefit compared to the best SOC. Current studies are ongoing to evaluate the effectiveness of 177Lu-PSMA-617 in earlier lines of therapy, such as after only 1 line of therapy with an ARPI as in the PSMAfore study, or in mCSPC in combination with ADT and an ARPI as in the PSMAddition study. Studies are also ongoing with 177Lu-PSMA-617 in combination with other treatments which may produce a synergistic effect. As described, there are many clinical trials ongoing that are modifying the 177Lu-PSMA-617 to possibly achieve improved results. Studies are also ongoing looking at swapping the 177Lu for another radioactive agent, such as 225Ac (an alpha emitter) which may have benefits over the beta-emitting 177Lu. Other studies are looking at J591, a monoclonal antibody to PSMA which has unique differences compared to small-molecule PSMA binders. Overall, PSMA-based radioligand therapy has been shown to be an effective and life-prolonging therapy and should be considered a treatment option for selected men with mCRPC. As described, there are many ongoing studies further evaluating PSMA radioligand therapy in Australia, South Africa, Europe, and the United States, representing a truly global effort to improve prostate cancer care.
Click to Show/Hide
|
||||
| Description |
Grade 3-4 AEs occurred in 32 (33%) of men who received 177Lu-PSMA-617 versus 45 (53%) of men in the cabazitaxel group. All-grade toxicities that were more common in the 177Lu-PSMA-617 were dry mouth (60% vs. 21%), dry eyes (30% vs. 4%), and thrombocytopenia (18% vs. 5%). All-grade toxicities that were more common with cabazitaxel were diarrhea (52% vs. 18%), neuropathy (26% vs. 10%), and dysgeusia (27% vs. 12%).
Click to Show/Hide
|
||||
Discovered Using Cell Line-derived Xenograft Model
| Experiment 1 Reporting the Activity Data of This PDC | [85] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Drug uptake dose |
7.5 ± 2.6%
|
|||
| Administration Dosage | 4.44-5.55 GBq | ||||
| Description |
Preclinical cell-binding studies of [177Lu]Lu-PSMA-617 revealed specific binding with LNCaP cells of 17.4% ± 2.4%. The uptake in LnCaP xenografted tumor (nude mice) was 7.5 ± 2.6% ID/g for ˜1.5-2.0 cm3 tumor volume at 24-h post-injection. Post-therapy (24 h) SPECT image of mCRPC patients with prior orchidectomy and various hormone therapy showed specific localization of [177Lu]Lu-PSMA-617 in the tumor region.
Click to Show/Hide
|
||||
| In Vivo Model | Nude mice LNCaP cells tumor xenograft model. | ||||
| In Vitro Model | Prostate carcinoma | LNCaP cell | CVCL_0395 | ||
| Experiment 2 Reporting the Activity Data of This PDC | [85] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Drug uptake dose |
17.4% ± 2.4%
|
|||
| Administration Dosage | 4.44-5.55 GBq | ||||
| Description |
Preclinical cell-binding studies of [177Lu]Lu-PSMA-617 revealed specific binding with LNCaP cells of 17.4% ± 2.4%. The uptake in LnCaP xenografted tumor (nude mice) was 7.5 ± 2.6% ID/g for ˜1.5-2.0 cm3 tumor volume at 24-h post-injection. Post-therapy (24 h) SPECT image of mCRPC patients with prior orchidectomy and various hormone therapy showed specific localization of [177Lu]Lu-PSMA-617 in the tumor region.
Click to Show/Hide
|
||||
| In Vivo Model | Nude mice LNCaP cells tumor xenograft model. | ||||
| In Vitro Model | Prostate carcinoma | LNCaP cell | CVCL_0395 | ||
Obtained from the Model Organism Data
| Experiment 1 Reporting the Activity Data of This PDC | [86] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Body mass decrease |
0.55 g
|
|||
| Administration Time | 4 days | ||||
| Administration Dosage | 120 MBq | ||||
| MOA of PDC |
In conclusion, the hematotoxicity resulting from the infusion of radioactivity doses up to 200 MBq in our mouse model is transient, and mice exhibit normalized blood values within a month with no other apparent adverse effects (e.g., deaths, bleeding, or sustained body mass loss). These activities in animal models may increase the relevance when studying renal toxicity in animal models and, hence, help improve therapeutic translation from animal models to the clinic.
Click to Show/Hide
|
||||
| Description |
Body mass was continuously monitored to assess health. Although mice receiving activity had an initial significant body mass loss (presented as gained/lost fraction from starting body mass), all mice had gained additional body mass at the end of the experiment. There was no significant difference in the body mass gains between groups (presented as gained mass relative to starting body mass).
Click to Show/Hide
|
||||
| In Vivo Model | BALB/cAnNRj mice. | ||||
| Experiment 2 Reporting the Activity Data of This PDC | [86] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Body mass decrease |
0.55 g
|
|||
| Administration Time | 4 days | ||||
| Administration Dosage | 200 MBq | ||||
| MOA of PDC |
In conclusion, the hematotoxicity resulting from the infusion of radioactivity doses up to 200 MBq in our mouse model is transient, and mice exhibit normalized blood values within a month with no other apparent adverse effects (e.g., deaths, bleeding, or sustained body mass loss). These activities in animal models may increase the relevance when studying renal toxicity in animal models and, hence, help improve therapeutic translation from animal models to the clinic.
Click to Show/Hide
|
||||
| Description |
Body mass was continuously monitored to assess health. Although mice receiving activity had an initial significant body mass loss (presented as gained/lost fraction from starting body mass), all mice had gained additional body mass at the end of the experiment. There was no significant difference in the body mass gains between groups (presented as gained mass relative to starting body mass).
Click to Show/Hide
|
||||
| In Vivo Model | BALB/cAnNRj mice. | ||||
| Experiment 3 Reporting the Activity Data of This PDC | [86] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Body mass decrease |
0.6 g
|
|||
| Administration Time | 4 days | ||||
| Administration Dosage | 160 MBq | ||||
| MOA of PDC |
In conclusion, the hematotoxicity resulting from the infusion of radioactivity doses up to 200 MBq in our mouse model is transient, and mice exhibit normalized blood values within a month with no other apparent adverse effects (e.g., deaths, bleeding, or sustained body mass loss). These activities in animal models may increase the relevance when studying renal toxicity in animal models and, hence, help improve therapeutic translation from animal models to the clinic.
Click to Show/Hide
|
||||
| Description |
Body mass was continuously monitored to assess health. Although mice receiving activity had an initial significant body mass loss (presented as gained/lost fraction from starting body mass), all mice had gained additional body mass at the end of the experiment. There was no significant difference in the body mass gains between groups (presented as gained mass relative to starting body mass).
Click to Show/Hide
|
||||
| In Vivo Model | BALB/cAnNRj mice. | ||||
| Experiment 4 Reporting the Activity Data of This PDC | [86] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Granulocyte count |
1.2x109/L
|
|||
| Administration Time | 13 days | ||||
| Administration Dosage | 120 MBq | ||||
| MOA of PDC |
In conclusion, the hematotoxicity resulting from the infusion of radioactivity doses up to 200 MBq in our mouse model is transient, and mice exhibit normalized blood values within a month with no other apparent adverse effects (e.g., deaths, bleeding, or sustained body mass loss). These activities in animal models may increase the relevance when studying renal toxicity in animal models and, hence, help improve therapeutic translation from animal models to the clinic.
Click to Show/Hide
|
||||
| Description |
After 17 days, the 160 MBq group still had lower WBC and lymphocytes, but the monocytes and granulocytes had recovered to a similar level as control animals. At 21, 25, and 32 days, there were no significant differences between control and animals receiving 177Lu-PSMA-617, suggesting no long-lasting hematotoxicity. Overall, there was no correlation between activity received and decrease in white blood cells at the different time points, not when correcting for body mass differences either.
Click to Show/Hide
|
||||
| In Vivo Model | BALB/cAnNRj mice. | ||||
| Experiment 5 Reporting the Activity Data of This PDC | [86] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Granulocyte count |
1.3x109/L
|
|||
| Administration Time | 13 days | ||||
| Administration Dosage | 200 MBq | ||||
| MOA of PDC |
In conclusion, the hematotoxicity resulting from the infusion of radioactivity doses up to 200 MBq in our mouse model is transient, and mice exhibit normalized blood values within a month with no other apparent adverse effects (e.g., deaths, bleeding, or sustained body mass loss). These activities in animal models may increase the relevance when studying renal toxicity in animal models and, hence, help improve therapeutic translation from animal models to the clinic.
Click to Show/Hide
|
||||
| Description |
After 17 days, the 160 MBq group still had lower WBC and lymphocytes, but the monocytes and granulocytes had recovered to a similar level as control animals. At 21, 25, and 32 days, there were no significant differences between control and animals receiving 177Lu-PSMA-617, suggesting no long-lasting hematotoxicity. Overall, there was no correlation between activity received and decrease in white blood cells at the different time points, not when correcting for body mass differences either.
Click to Show/Hide
|
||||
| In Vivo Model | BALB/cAnNRj mice. | ||||
| Experiment 6 Reporting the Activity Data of This PDC | [86] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Granulocyte count |
1.5x109/L
|
|||
| Administration Time | 13 days | ||||
| Administration Dosage | 160 MBq | ||||
| MOA of PDC |
In conclusion, the hematotoxicity resulting from the infusion of radioactivity doses up to 200 MBq in our mouse model is transient, and mice exhibit normalized blood values within a month with no other apparent adverse effects (e.g., deaths, bleeding, or sustained body mass loss). These activities in animal models may increase the relevance when studying renal toxicity in animal models and, hence, help improve therapeutic translation from animal models to the clinic.
Click to Show/Hide
|
||||
| Description |
After 17 days, the 160 MBq group still had lower WBC and lymphocytes, but the monocytes and granulocytes had recovered to a similar level as control animals. At 21, 25, and 32 days, there were no significant differences between control and animals receiving 177Lu-PSMA-617, suggesting no long-lasting hematotoxicity. Overall, there was no correlation between activity received and decrease in white blood cells at the different time points, not when correcting for body mass differences either.
Click to Show/Hide
|
||||
| In Vivo Model | BALB/cAnNRj mice. | ||||
| Experiment 7 Reporting the Activity Data of This PDC | [86] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Granulocyte count |
1.9x109/L
|
|||
| Administration Time | 13 days | ||||
| Administration Dosage | 160 MBq | ||||
| MOA of PDC |
In conclusion, the hematotoxicity resulting from the infusion of radioactivity doses up to 200 MBq in our mouse model is transient, and mice exhibit normalized blood values within a month with no other apparent adverse effects (e.g., deaths, bleeding, or sustained body mass loss). These activities in animal models may increase the relevance when studying renal toxicity in animal models and, hence, help improve therapeutic translation from animal models to the clinic.
Click to Show/Hide
|
||||
| Description |
After 17 days, the 160 MBq group still had lower WBC and lymphocytes, but the monocytes and granulocytes had recovered to a similar level as control animals. At 21, 25, and 32 days, there were no significant differences between control and animals receiving 177Lu-PSMA-617, suggesting no long-lasting hematotoxicity. Overall, there was no correlation between activity received and decrease in white blood cells at the different time points, not when correcting for body mass differences either.
Click to Show/Hide
|
||||
| In Vivo Model | BALB/cAnNRj mice. | ||||
| Experiment 8 Reporting the Activity Data of This PDC | [86] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Granulocyte count |
2.1x109/L
|
|||
| Administration Time | 13 days | ||||
| Administration Dosage | 200 MBq | ||||
| MOA of PDC |
In conclusion, the hematotoxicity resulting from the infusion of radioactivity doses up to 200 MBq in our mouse model is transient, and mice exhibit normalized blood values within a month with no other apparent adverse effects (e.g., deaths, bleeding, or sustained body mass loss). These activities in animal models may increase the relevance when studying renal toxicity in animal models and, hence, help improve therapeutic translation from animal models to the clinic.
Click to Show/Hide
|
||||
| Description |
After 17 days, the 160 MBq group still had lower WBC and lymphocytes, but the monocytes and granulocytes had recovered to a similar level as control animals. At 21, 25, and 32 days, there were no significant differences between control and animals receiving 177Lu-PSMA-617, suggesting no long-lasting hematotoxicity. Overall, there was no correlation between activity received and decrease in white blood cells at the different time points, not when correcting for body mass differences either.
Click to Show/Hide
|
||||
| In Vivo Model | BALB/cAnNRj mice. | ||||
| Experiment 9 Reporting the Activity Data of This PDC | [86] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Granulocyte count |
2.2x109/L
|
|||
| Administration Time | 13 days | ||||
| Administration Dosage | 120 MBq | ||||
| MOA of PDC |
In conclusion, the hematotoxicity resulting from the infusion of radioactivity doses up to 200 MBq in our mouse model is transient, and mice exhibit normalized blood values within a month with no other apparent adverse effects (e.g., deaths, bleeding, or sustained body mass loss). These activities in animal models may increase the relevance when studying renal toxicity in animal models and, hence, help improve therapeutic translation from animal models to the clinic.
Click to Show/Hide
|
||||
| Description |
After 17 days, the 160 MBq group still had lower WBC and lymphocytes, but the monocytes and granulocytes had recovered to a similar level as control animals. At 21, 25, and 32 days, there were no significant differences between control and animals receiving 177Lu-PSMA-617, suggesting no long-lasting hematotoxicity. Overall, there was no correlation between activity received and decrease in white blood cells at the different time points, not when correcting for body mass differences either.
Click to Show/Hide
|
||||
| In Vivo Model | BALB/cAnNRj mice. | ||||
| Experiment 10 Reporting the Activity Data of This PDC | [86] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Hematocrit decrease rate |
10%
|
|||
| Administration Time | 21 days | ||||
| Administration Dosage | 200 MBq | ||||
| MOA of PDC |
In conclusion, the hematotoxicity resulting from the infusion of radioactivity doses up to 200 MBq in our mouse model is transient, and mice exhibit normalized blood values within a month with no other apparent adverse effects (e.g., deaths, bleeding, or sustained body mass loss). These activities in animal models may increase the relevance when studying renal toxicity in animal models and, hence, help improve therapeutic translation from animal models to the clinic.
Click to Show/Hide
|
||||
| Description |
After 21 days, all groups showed a tendency toward a lower number of RBCs, although only significant in the 120 MBq group. However, when analyzing the blood at 25 days post injection, the number of RBCs and HCT were again significantly lower in the 160 MBq animals. After 32 days, all studied parameters involving RBCs were normalized and did not differ from control mice, with the only exception of MCV in the 200 MBq group. Similar to the RBCs, the spread, in general, was larger in the treated groups for MCV, HBG, and HCT than in the control group. Further, as with the WBC, the decrease in RBCs and HBG levels did not have a correlation to injected activity, and no significant differences between the 120, 160, and 200 MBq were seen at any time point.
Click to Show/Hide
|
||||
| In Vivo Model | BALB/cAnNRj mice. | ||||
| Experiment 11 Reporting the Activity Data of This PDC | [86] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Hematocrit decrease rate |
16%
|
|||
| Administration Time | 21 days | ||||
| Administration Dosage | 120 MBq | ||||
| MOA of PDC |
In conclusion, the hematotoxicity resulting from the infusion of radioactivity doses up to 200 MBq in our mouse model is transient, and mice exhibit normalized blood values within a month with no other apparent adverse effects (e.g., deaths, bleeding, or sustained body mass loss). These activities in animal models may increase the relevance when studying renal toxicity in animal models and, hence, help improve therapeutic translation from animal models to the clinic.
Click to Show/Hide
|
||||
| Description |
After 21 days, all groups showed a tendency toward a lower number of RBCs, although only significant in the 120 MBq group. However, when analyzing the blood at 25 days post injection, the number of RBCs and HCT were again significantly lower in the 160 MBq animals. After 32 days, all studied parameters involving RBCs were normalized and did not differ from control mice, with the only exception of MCV in the 200 MBq group. Similar to the RBCs, the spread, in general, was larger in the treated groups for MCV, HBG, and HCT than in the control group. Further, as with the WBC, the decrease in RBCs and HBG levels did not have a correlation to injected activity, and no significant differences between the 120, 160, and 200 MBq were seen at any time point.
Click to Show/Hide
|
||||
| In Vivo Model | BALB/cAnNRj mice. | ||||
| Experiment 12 Reporting the Activity Data of This PDC | [86] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Hematocrit decrease rate |
19%
|
|||
| Administration Time | 21 days | ||||
| Administration Dosage | 160 MBq | ||||
| MOA of PDC |
In conclusion, the hematotoxicity resulting from the infusion of radioactivity doses up to 200 MBq in our mouse model is transient, and mice exhibit normalized blood values within a month with no other apparent adverse effects (e.g., deaths, bleeding, or sustained body mass loss). These activities in animal models may increase the relevance when studying renal toxicity in animal models and, hence, help improve therapeutic translation from animal models to the clinic.
Click to Show/Hide
|
||||
| Description |
After 21 days, all groups showed a tendency toward a lower number of RBCs, although only significant in the 120 MBq group. However, when analyzing the blood at 25 days post injection, the number of RBCs and HCT were again significantly lower in the 160 MBq animals. After 32 days, all studied parameters involving RBCs were normalized and did not differ from control mice, with the only exception of MCV in the 200 MBq group. Similar to the RBCs, the spread, in general, was larger in the treated groups for MCV, HBG, and HCT than in the control group. Further, as with the WBC, the decrease in RBCs and HBG levels did not have a correlation to injected activity, and no significant differences between the 120, 160, and 200 MBq were seen at any time point.
Click to Show/Hide
|
||||
| In Vivo Model | BALB/cAnNRj mice. | ||||
| Experiment 13 Reporting the Activity Data of This PDC | [86] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Hematocrit decrease rate |
40%
|
|||
| Administration Time | 21 days | ||||
| Administration Dosage | 160 MBq | ||||
| MOA of PDC |
In conclusion, the hematotoxicity resulting from the infusion of radioactivity doses up to 200 MBq in our mouse model is transient, and mice exhibit normalized blood values within a month with no other apparent adverse effects (e.g., deaths, bleeding, or sustained body mass loss). These activities in animal models may increase the relevance when studying renal toxicity in animal models and, hence, help improve therapeutic translation from animal models to the clinic.
Click to Show/Hide
|
||||
| Description |
After 21 days, all groups showed a tendency toward a lower number of RBCs, although only significant in the 120 MBq group. However, when analyzing the blood at 25 days post injection, the number of RBCs and HCT were again significantly lower in the 160 MBq animals. After 32 days, all studied parameters involving RBCs were normalized and did not differ from control mice, with the only exception of MCV in the 200 MBq group. Similar to the RBCs, the spread, in general, was larger in the treated groups for MCV, HBG, and HCT than in the control group. Further, as with the WBC, the decrease in RBCs and HBG levels did not have a correlation to injected activity, and no significant differences between the 120, 160, and 200 MBq were seen at any time point.
Click to Show/Hide
|
||||
| In Vivo Model | BALB/cAnNRj mice. | ||||
| Experiment 14 Reporting the Activity Data of This PDC | [86] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Hematocrit decrease rate |
43%
|
|||
| Administration Time | 21 days | ||||
| Administration Dosage | 120 MBq | ||||
| MOA of PDC |
In conclusion, the hematotoxicity resulting from the infusion of radioactivity doses up to 200 MBq in our mouse model is transient, and mice exhibit normalized blood values within a month with no other apparent adverse effects (e.g., deaths, bleeding, or sustained body mass loss). These activities in animal models may increase the relevance when studying renal toxicity in animal models and, hence, help improve therapeutic translation from animal models to the clinic.
Click to Show/Hide
|
||||
| Description |
After 21 days, all groups showed a tendency toward a lower number of RBCs, although only significant in the 120 MBq group. However, when analyzing the blood at 25 days post injection, the number of RBCs and HCT were again significantly lower in the 160 MBq animals. After 32 days, all studied parameters involving RBCs were normalized and did not differ from control mice, with the only exception of MCV in the 200 MBq group. Similar to the RBCs, the spread, in general, was larger in the treated groups for MCV, HBG, and HCT than in the control group. Further, as with the WBC, the decrease in RBCs and HBG levels did not have a correlation to injected activity, and no significant differences between the 120, 160, and 200 MBq were seen at any time point.
Click to Show/Hide
|
||||
| In Vivo Model | BALB/cAnNRj mice. | ||||
| Experiment 15 Reporting the Activity Data of This PDC | [86] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Hematocrit decrease rate |
49%
|
|||
| Administration Time | 21 days | ||||
| Administration Dosage | 200 MBq | ||||
| MOA of PDC |
In conclusion, the hematotoxicity resulting from the infusion of radioactivity doses up to 200 MBq in our mouse model is transient, and mice exhibit normalized blood values within a month with no other apparent adverse effects (e.g., deaths, bleeding, or sustained body mass loss). These activities in animal models may increase the relevance when studying renal toxicity in animal models and, hence, help improve therapeutic translation from animal models to the clinic.
Click to Show/Hide
|
||||
| Description |
After 21 days, all groups showed a tendency toward a lower number of RBCs, although only significant in the 120 MBq group. However, when analyzing the blood at 25 days post injection, the number of RBCs and HCT were again significantly lower in the 160 MBq animals. After 32 days, all studied parameters involving RBCs were normalized and did not differ from control mice, with the only exception of MCV in the 200 MBq group. Similar to the RBCs, the spread, in general, was larger in the treated groups for MCV, HBG, and HCT than in the control group. Further, as with the WBC, the decrease in RBCs and HBG levels did not have a correlation to injected activity, and no significant differences between the 120, 160, and 200 MBq were seen at any time point.
Click to Show/Hide
|
||||
| In Vivo Model | BALB/cAnNRj mice. | ||||
| Experiment 16 Reporting the Activity Data of This PDC | [86] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Hemoglobin |
12 g/dL
|
|||
| Administration Time | 21 days | ||||
| Administration Dosage | 120 MBq | ||||
| MOA of PDC |
In conclusion, the hematotoxicity resulting from the infusion of radioactivity doses up to 200 MBq in our mouse model is transient, and mice exhibit normalized blood values within a month with no other apparent adverse effects (e.g., deaths, bleeding, or sustained body mass loss). These activities in animal models may increase the relevance when studying renal toxicity in animal models and, hence, help improve therapeutic translation from animal models to the clinic.
Click to Show/Hide
|
||||
| Description |
After 21 days, all groups showed a tendency toward a lower number of RBCs, although only significant in the 120 MBq group. However, when analyzing the blood at 25 days post injection, the number of RBCs and HCT were again significantly lower in the 160 MBq animals. After 32 days, all studied parameters involving RBCs were normalized and did not differ from control mice, with the only exception of MCV in the 200 MBq group. Similar to the RBCs, the spread, in general, was larger in the treated groups for MCV, HBG, and HCT than in the control group. Further, as with the WBC, the decrease in RBCs and HBG levels did not have a correlation to injected activity, and no significant differences between the 120, 160, and 200 MBq were seen at any time point.
Click to Show/Hide
|
||||
| In Vivo Model | BALB/cAnNRj mice. | ||||
| Experiment 17 Reporting the Activity Data of This PDC | [86] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Hemoglobin |
12 g/dL
|
|||
| Administration Time | 21 days | ||||
| Administration Dosage | 160 MBq | ||||
| MOA of PDC |
In conclusion, the hematotoxicity resulting from the infusion of radioactivity doses up to 200 MBq in our mouse model is transient, and mice exhibit normalized blood values within a month with no other apparent adverse effects (e.g., deaths, bleeding, or sustained body mass loss). These activities in animal models may increase the relevance when studying renal toxicity in animal models and, hence, help improve therapeutic translation from animal models to the clinic.
Click to Show/Hide
|
||||
| Description |
After 21 days, all groups showed a tendency toward a lower number of RBCs, although only significant in the 120 MBq group. However, when analyzing the blood at 25 days post injection, the number of RBCs and HCT were again significantly lower in the 160 MBq animals. After 32 days, all studied parameters involving RBCs were normalized and did not differ from control mice, with the only exception of MCV in the 200 MBq group. Similar to the RBCs, the spread, in general, was larger in the treated groups for MCV, HBG, and HCT than in the control group. Further, as with the WBC, the decrease in RBCs and HBG levels did not have a correlation to injected activity, and no significant differences between the 120, 160, and 200 MBq were seen at any time point.
Click to Show/Hide
|
||||
| In Vivo Model | BALB/cAnNRj mice. | ||||
| Experiment 18 Reporting the Activity Data of This PDC | [86] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Hemoglobin |
13.5 g/dL
|
|||
| Administration Time | 21 days | ||||
| Administration Dosage | 200 MBq | ||||
| MOA of PDC |
In conclusion, the hematotoxicity resulting from the infusion of radioactivity doses up to 200 MBq in our mouse model is transient, and mice exhibit normalized blood values within a month with no other apparent adverse effects (e.g., deaths, bleeding, or sustained body mass loss). These activities in animal models may increase the relevance when studying renal toxicity in animal models and, hence, help improve therapeutic translation from animal models to the clinic.
Click to Show/Hide
|
||||
| Description |
After 21 days, all groups showed a tendency toward a lower number of RBCs, although only significant in the 120 MBq group. However, when analyzing the blood at 25 days post injection, the number of RBCs and HCT were again significantly lower in the 160 MBq animals. After 32 days, all studied parameters involving RBCs were normalized and did not differ from control mice, with the only exception of MCV in the 200 MBq group. Similar to the RBCs, the spread, in general, was larger in the treated groups for MCV, HBG, and HCT than in the control group. Further, as with the WBC, the decrease in RBCs and HBG levels did not have a correlation to injected activity, and no significant differences between the 120, 160, and 200 MBq were seen at any time point.
Click to Show/Hide
|
||||
| In Vivo Model | BALB/cAnNRj mice. | ||||
| Experiment 19 Reporting the Activity Data of This PDC | [86] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Hemoglobin decrease |
2.5 g/dL
|
|||
| Administration Time | 21 days | ||||
| Administration Dosage | 200 MBq | ||||
| MOA of PDC |
In conclusion, the hematotoxicity resulting from the infusion of radioactivity doses up to 200 MBq in our mouse model is transient, and mice exhibit normalized blood values within a month with no other apparent adverse effects (e.g., deaths, bleeding, or sustained body mass loss). These activities in animal models may increase the relevance when studying renal toxicity in animal models and, hence, help improve therapeutic translation from animal models to the clinic.
Click to Show/Hide
|
||||
| Description |
After 21 days, all groups showed a tendency toward a lower number of RBCs, although only significant in the 120 MBq group. However, when analyzing the blood at 25 days post injection, the number of RBCs and HCT were again significantly lower in the 160 MBq animals. After 32 days, all studied parameters involving RBCs were normalized and did not differ from control mice, with the only exception of MCV in the 200 MBq group. Similar to the RBCs, the spread, in general, was larger in the treated groups for MCV, HBG, and HCT than in the control group. Further, as with the WBC, the decrease in RBCs and HBG levels did not have a correlation to injected activity, and no significant differences between the 120, 160, and 200 MBq were seen at any time point.
Click to Show/Hide
|
||||
| In Vivo Model | BALB/cAnNRj mice. | ||||
| Experiment 20 Reporting the Activity Data of This PDC | [86] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Hemoglobin decrease |
4 g/dL
|
|||
| Administration Time | 21 days | ||||
| Administration Dosage | 120 MBq | ||||
| MOA of PDC |
In conclusion, the hematotoxicity resulting from the infusion of radioactivity doses up to 200 MBq in our mouse model is transient, and mice exhibit normalized blood values within a month with no other apparent adverse effects (e.g., deaths, bleeding, or sustained body mass loss). These activities in animal models may increase the relevance when studying renal toxicity in animal models and, hence, help improve therapeutic translation from animal models to the clinic.
Click to Show/Hide
|
||||
| Description |
After 21 days, all groups showed a tendency toward a lower number of RBCs, although only significant in the 120 MBq group. However, when analyzing the blood at 25 days post injection, the number of RBCs and HCT were again significantly lower in the 160 MBq animals. After 32 days, all studied parameters involving RBCs were normalized and did not differ from control mice, with the only exception of MCV in the 200 MBq group. Similar to the RBCs, the spread, in general, was larger in the treated groups for MCV, HBG, and HCT than in the control group. Further, as with the WBC, the decrease in RBCs and HBG levels did not have a correlation to injected activity, and no significant differences between the 120, 160, and 200 MBq were seen at any time point.
Click to Show/Hide
|
||||
| In Vivo Model | BALB/cAnNRj mice. | ||||
| Experiment 21 Reporting the Activity Data of This PDC | [86] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Hemoglobin decrease |
4 g/dL
|
|||
| Administration Time | 21 days | ||||
| Administration Dosage | 160 MBq | ||||
| MOA of PDC |
In conclusion, the hematotoxicity resulting from the infusion of radioactivity doses up to 200 MBq in our mouse model is transient, and mice exhibit normalized blood values within a month with no other apparent adverse effects (e.g., deaths, bleeding, or sustained body mass loss). These activities in animal models may increase the relevance when studying renal toxicity in animal models and, hence, help improve therapeutic translation from animal models to the clinic.
Click to Show/Hide
|
||||
| Description |
After 21 days, all groups showed a tendency toward a lower number of RBCs, although only significant in the 120 MBq group. However, when analyzing the blood at 25 days post injection, the number of RBCs and HCT were again significantly lower in the 160 MBq animals. After 32 days, all studied parameters involving RBCs were normalized and did not differ from control mice, with the only exception of MCV in the 200 MBq group. Similar to the RBCs, the spread, in general, was larger in the treated groups for MCV, HBG, and HCT than in the control group. Further, as with the WBC, the decrease in RBCs and HBG levels did not have a correlation to injected activity, and no significant differences between the 120, 160, and 200 MBq were seen at any time point.
Click to Show/Hide
|
||||
| In Vivo Model | BALB/cAnNRj mice. | ||||
| Experiment 22 Reporting the Activity Data of This PDC | [86] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Lymphocyte count |
4x109/L
|
|||
| Administration Time | 13 days | ||||
| Administration Dosage | 160 MBq | ||||
| MOA of PDC |
In conclusion, the hematotoxicity resulting from the infusion of radioactivity doses up to 200 MBq in our mouse model is transient, and mice exhibit normalized blood values within a month with no other apparent adverse effects (e.g., deaths, bleeding, or sustained body mass loss). These activities in animal models may increase the relevance when studying renal toxicity in animal models and, hence, help improve therapeutic translation from animal models to the clinic.
Click to Show/Hide
|
||||
| Description |
After 17 days, the 160 MBq group still had lower WBC and lymphocytes, but the monocytes and granulocytes had recovered to a similar level as control animals. At 21, 25, and 32 days, there were no significant differences between control and animals receiving 177Lu-PSMA-617, suggesting no long-lasting hematotoxicity. Overall, there was no correlation between activity received and decrease in white blood cells at the different time points, not when correcting for body mass differences either.
Click to Show/Hide
|
||||
| In Vivo Model | BALB/cAnNRj mice. | ||||
| Experiment 23 Reporting the Activity Data of This PDC | [86] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Lymphocyte count |
4.5x109/L
|
|||
| Administration Time | 13 days | ||||
| Administration Dosage | 200 MBq | ||||
| MOA of PDC |
In conclusion, the hematotoxicity resulting from the infusion of radioactivity doses up to 200 MBq in our mouse model is transient, and mice exhibit normalized blood values within a month with no other apparent adverse effects (e.g., deaths, bleeding, or sustained body mass loss). These activities in animal models may increase the relevance when studying renal toxicity in animal models and, hence, help improve therapeutic translation from animal models to the clinic.
Click to Show/Hide
|
||||
| Description |
After 17 days, the 160 MBq group still had lower WBC and lymphocytes, but the monocytes and granulocytes had recovered to a similar level as control animals. At 21, 25, and 32 days, there were no significant differences between control and animals receiving 177Lu-PSMA-617, suggesting no long-lasting hematotoxicity. Overall, there was no correlation between activity received and decrease in white blood cells at the different time points, not when correcting for body mass differences either.
Click to Show/Hide
|
||||
| In Vivo Model | BALB/cAnNRj mice. | ||||
| Experiment 24 Reporting the Activity Data of This PDC | [86] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Lymphocyte count |
5.5x109/L
|
|||
| Administration Time | 13 days | ||||
| Administration Dosage | 120 MBq | ||||
| MOA of PDC |
In conclusion, the hematotoxicity resulting from the infusion of radioactivity doses up to 200 MBq in our mouse model is transient, and mice exhibit normalized blood values within a month with no other apparent adverse effects (e.g., deaths, bleeding, or sustained body mass loss). These activities in animal models may increase the relevance when studying renal toxicity in animal models and, hence, help improve therapeutic translation from animal models to the clinic.
Click to Show/Hide
|
||||
| Description |
After 17 days, the 160 MBq group still had lower WBC and lymphocytes, but the monocytes and granulocytes had recovered to a similar level as control animals. At 21, 25, and 32 days, there were no significant differences between control and animals receiving 177Lu-PSMA-617, suggesting no long-lasting hematotoxicity. Overall, there was no correlation between activity received and decrease in white blood cells at the different time points, not when correcting for body mass differences either.
Click to Show/Hide
|
||||
| In Vivo Model | BALB/cAnNRj mice. | ||||
| Experiment 25 Reporting the Activity Data of This PDC | [86] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Lymphocyte count |
6.5x109/L
|
|||
| Administration Time | 13 days | ||||
| Administration Dosage | 200 MBq | ||||
| MOA of PDC |
In conclusion, the hematotoxicity resulting from the infusion of radioactivity doses up to 200 MBq in our mouse model is transient, and mice exhibit normalized blood values within a month with no other apparent adverse effects (e.g., deaths, bleeding, or sustained body mass loss). These activities in animal models may increase the relevance when studying renal toxicity in animal models and, hence, help improve therapeutic translation from animal models to the clinic.
Click to Show/Hide
|
||||
| Description |
After 17 days, the 160 MBq group still had lower WBC and lymphocytes, but the monocytes and granulocytes had recovered to a similar level as control animals. At 21, 25, and 32 days, there were no significant differences between control and animals receiving 177Lu-PSMA-617, suggesting no long-lasting hematotoxicity. Overall, there was no correlation between activity received and decrease in white blood cells at the different time points, not when correcting for body mass differences either.
Click to Show/Hide
|
||||
| In Vivo Model | BALB/cAnNRj mice. | ||||
| Experiment 26 Reporting the Activity Data of This PDC | [86] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Lymphocyte count |
7x109/L
|
|||
| Administration Time | 13 days | ||||
| Administration Dosage | 160 MBq | ||||
| MOA of PDC |
In conclusion, the hematotoxicity resulting from the infusion of radioactivity doses up to 200 MBq in our mouse model is transient, and mice exhibit normalized blood values within a month with no other apparent adverse effects (e.g., deaths, bleeding, or sustained body mass loss). These activities in animal models may increase the relevance when studying renal toxicity in animal models and, hence, help improve therapeutic translation from animal models to the clinic.
Click to Show/Hide
|
||||
| Description |
After 17 days, the 160 MBq group still had lower WBC and lymphocytes, but the monocytes and granulocytes had recovered to a similar level as control animals. At 21, 25, and 32 days, there were no significant differences between control and animals receiving 177Lu-PSMA-617, suggesting no long-lasting hematotoxicity. Overall, there was no correlation between activity received and decrease in white blood cells at the different time points, not when correcting for body mass differences either.
Click to Show/Hide
|
||||
| In Vivo Model | BALB/cAnNRj mice. | ||||
| Experiment 27 Reporting the Activity Data of This PDC | [86] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Mean cell volume |
0.3x1012/L
|
|||
| Administration Time | 13 days | ||||
| Administration Dosage | 160 MBq | ||||
| MOA of PDC |
In conclusion, the hematotoxicity resulting from the infusion of radioactivity doses up to 200 MBq in our mouse model is transient, and mice exhibit normalized blood values within a month with no other apparent adverse effects (e.g., deaths, bleeding, or sustained body mass loss). These activities in animal models may increase the relevance when studying renal toxicity in animal models and, hence, help improve therapeutic translation from animal models to the clinic.
Click to Show/Hide
|
||||
| Description |
After 21 days, all groups showed a tendency toward a lower number of RBCs, although only significant in the 120 MBq group. However, when analyzing the blood at 25 days post injection, the number of RBCs and HCT were again significantly lower in the 160 MBq animals. After 32 days, all studied parameters involving RBCs were normalized and did not differ from control mice, with the only exception of MCV in the 200 MBq group. Similar to the RBCs, the spread, in general, was larger in the treated groups for MCV, HBG, and HCT than in the control group. Further, as with the WBC, the decrease in RBCs and HBG levels did not have a correlation to injected activity, and no significant differences between the 120, 160, and 200 MBq were seen at any time point.
Click to Show/Hide
|
||||
| In Vivo Model | BALB/cAnNRj mice. | ||||
| Experiment 28 Reporting the Activity Data of This PDC | [86] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Mean cell volume |
1x1012/L
|
|||
| Administration Time | 13 days | ||||
| Administration Dosage | 120 MBq | ||||
| MOA of PDC |
In conclusion, the hematotoxicity resulting from the infusion of radioactivity doses up to 200 MBq in our mouse model is transient, and mice exhibit normalized blood values within a month with no other apparent adverse effects (e.g., deaths, bleeding, or sustained body mass loss). These activities in animal models may increase the relevance when studying renal toxicity in animal models and, hence, help improve therapeutic translation from animal models to the clinic.
Click to Show/Hide
|
||||
| Description |
After 21 days, all groups showed a tendency toward a lower number of RBCs, although only significant in the 120 MBq group. However, when analyzing the blood at 25 days post injection, the number of RBCs and HCT were again significantly lower in the 160 MBq animals. After 32 days, all studied parameters involving RBCs were normalized and did not differ from control mice, with the only exception of MCV in the 200 MBq group. Similar to the RBCs, the spread, in general, was larger in the treated groups for MCV, HBG, and HCT than in the control group. Further, as with the WBC, the decrease in RBCs and HBG levels did not have a correlation to injected activity, and no significant differences between the 120, 160, and 200 MBq were seen at any time point.
Click to Show/Hide
|
||||
| In Vivo Model | BALB/cAnNRj mice. | ||||
| Experiment 29 Reporting the Activity Data of This PDC | [86] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Mean cell volume |
1.5x1012/L
|
|||
| Administration Time | 17 days | ||||
| Administration Dosage | 160 MBq | ||||
| MOA of PDC |
In conclusion, the hematotoxicity resulting from the infusion of radioactivity doses up to 200 MBq in our mouse model is transient, and mice exhibit normalized blood values within a month with no other apparent adverse effects (e.g., deaths, bleeding, or sustained body mass loss). These activities in animal models may increase the relevance when studying renal toxicity in animal models and, hence, help improve therapeutic translation from animal models to the clinic.
Click to Show/Hide
|
||||
| Description |
After 21 days, all groups showed a tendency toward a lower number of RBCs, although only significant in the 120 MBq group. However, when analyzing the blood at 25 days post injection, the number of RBCs and HCT were again significantly lower in the 160 MBq animals. After 32 days, all studied parameters involving RBCs were normalized and did not differ from control mice, with the only exception of MCV in the 200 MBq group. Similar to the RBCs, the spread, in general, was larger in the treated groups for MCV, HBG, and HCT than in the control group. Further, as with the WBC, the decrease in RBCs and HBG levels did not have a correlation to injected activity, and no significant differences between the 120, 160, and 200 MBq were seen at any time point.
Click to Show/Hide
|
||||
| In Vivo Model | BALB/cAnNRj mice. | ||||
| Experiment 30 Reporting the Activity Data of This PDC | [86] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Mean cell volume |
55.5x1012/L
|
|||
| Administration Time | 13 days | ||||
| Administration Dosage | 200 MBq | ||||
| MOA of PDC |
In conclusion, the hematotoxicity resulting from the infusion of radioactivity doses up to 200 MBq in our mouse model is transient, and mice exhibit normalized blood values within a month with no other apparent adverse effects (e.g., deaths, bleeding, or sustained body mass loss). These activities in animal models may increase the relevance when studying renal toxicity in animal models and, hence, help improve therapeutic translation from animal models to the clinic.
Click to Show/Hide
|
||||
| Description |
After 21 days, all groups showed a tendency toward a lower number of RBCs, although only significant in the 120 MBq group. However, when analyzing the blood at 25 days post injection, the number of RBCs and HCT were again significantly lower in the 160 MBq animals. After 32 days, all studied parameters involving RBCs were normalized and did not differ from control mice, with the only exception of MCV in the 200 MBq group. Similar to the RBCs, the spread, in general, was larger in the treated groups for MCV, HBG, and HCT than in the control group. Further, as with the WBC, the decrease in RBCs and HBG levels did not have a correlation to injected activity, and no significant differences between the 120, 160, and 200 MBq were seen at any time point.
Click to Show/Hide
|
||||
| In Vivo Model | BALB/cAnNRj mice. | ||||
| Experiment 31 Reporting the Activity Data of This PDC | [86] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Mean cell volume |
55.8x1012/L
|
|||
| Administration Time | 13 days | ||||
| Administration Dosage | 160 MBq | ||||
| MOA of PDC |
In conclusion, the hematotoxicity resulting from the infusion of radioactivity doses up to 200 MBq in our mouse model is transient, and mice exhibit normalized blood values within a month with no other apparent adverse effects (e.g., deaths, bleeding, or sustained body mass loss). These activities in animal models may increase the relevance when studying renal toxicity in animal models and, hence, help improve therapeutic translation from animal models to the clinic.
Click to Show/Hide
|
||||
| Description |
After 21 days, all groups showed a tendency toward a lower number of RBCs, although only significant in the 120 MBq group. However, when analyzing the blood at 25 days post injection, the number of RBCs and HCT were again significantly lower in the 160 MBq animals. After 32 days, all studied parameters involving RBCs were normalized and did not differ from control mice, with the only exception of MCV in the 200 MBq group. Similar to the RBCs, the spread, in general, was larger in the treated groups for MCV, HBG, and HCT than in the control group. Further, as with the WBC, the decrease in RBCs and HBG levels did not have a correlation to injected activity, and no significant differences between the 120, 160, and 200 MBq were seen at any time point.
Click to Show/Hide
|
||||
| In Vivo Model | BALB/cAnNRj mice. | ||||
| Experiment 32 Reporting the Activity Data of This PDC | [86] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Mean cell volume |
56.5x1012/L
|
|||
| Administration Time | 13 days | ||||
| Administration Dosage | 120 MBq | ||||
| MOA of PDC |
In conclusion, the hematotoxicity resulting from the infusion of radioactivity doses up to 200 MBq in our mouse model is transient, and mice exhibit normalized blood values within a month with no other apparent adverse effects (e.g., deaths, bleeding, or sustained body mass loss). These activities in animal models may increase the relevance when studying renal toxicity in animal models and, hence, help improve therapeutic translation from animal models to the clinic.
Click to Show/Hide
|
||||
| Description |
After 21 days, all groups showed a tendency toward a lower number of RBCs, although only significant in the 120 MBq group. However, when analyzing the blood at 25 days post injection, the number of RBCs and HCT were again significantly lower in the 160 MBq animals. After 32 days, all studied parameters involving RBCs were normalized and did not differ from control mice, with the only exception of MCV in the 200 MBq group. Similar to the RBCs, the spread, in general, was larger in the treated groups for MCV, HBG, and HCT than in the control group. Further, as with the WBC, the decrease in RBCs and HBG levels did not have a correlation to injected activity, and no significant differences between the 120, 160, and 200 MBq were seen at any time point.
Click to Show/Hide
|
||||
| In Vivo Model | BALB/cAnNRj mice. | ||||
| Experiment 33 Reporting the Activity Data of This PDC | [86] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Mean cell volume |
57x1012/L
|
|||
| Administration Time | 17 days | ||||
| Administration Dosage | 160 MBq | ||||
| MOA of PDC |
In conclusion, the hematotoxicity resulting from the infusion of radioactivity doses up to 200 MBq in our mouse model is transient, and mice exhibit normalized blood values within a month with no other apparent adverse effects (e.g., deaths, bleeding, or sustained body mass loss). These activities in animal models may increase the relevance when studying renal toxicity in animal models and, hence, help improve therapeutic translation from animal models to the clinic.
Click to Show/Hide
|
||||
| Description |
After 21 days, all groups showed a tendency toward a lower number of RBCs, although only significant in the 120 MBq group. However, when analyzing the blood at 25 days post injection, the number of RBCs and HCT were again significantly lower in the 160 MBq animals. After 32 days, all studied parameters involving RBCs were normalized and did not differ from control mice, with the only exception of MCV in the 200 MBq group. Similar to the RBCs, the spread, in general, was larger in the treated groups for MCV, HBG, and HCT than in the control group. Further, as with the WBC, the decrease in RBCs and HBG levels did not have a correlation to injected activity, and no significant differences between the 120, 160, and 200 MBq were seen at any time point.
Click to Show/Hide
|
||||
| In Vivo Model | BALB/cAnNRj mice. | ||||
| Experiment 34 Reporting the Activity Data of This PDC | [86] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Monocyte count |
0.2x109/L
|
|||
| Administration Time | 13 days | ||||
| Administration Dosage | 120 MBq | ||||
| MOA of PDC |
In conclusion, the hematotoxicity resulting from the infusion of radioactivity doses up to 200 MBq in our mouse model is transient, and mice exhibit normalized blood values within a month with no other apparent adverse effects (e.g., deaths, bleeding, or sustained body mass loss). These activities in animal models may increase the relevance when studying renal toxicity in animal models and, hence, help improve therapeutic translation from animal models to the clinic.
Click to Show/Hide
|
||||
| Description |
After 17 days, the 160 MBq group still had lower WBC and lymphocytes, but the monocytes and granulocytes had recovered to a similar level as control animals. At 21, 25, and 32 days, there were no significant differences between control and animals receiving 177Lu-PSMA-617, suggesting no long-lasting hematotoxicity. Overall, there was no correlation between activity received and decrease in white blood cells at the different time points, not when correcting for body mass differences either.
Click to Show/Hide
|
||||
| In Vivo Model | BALB/cAnNRj mice. | ||||
| Experiment 35 Reporting the Activity Data of This PDC | [86] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Monocyte count |
0.3x109/L
|
|||
| Administration Time | 13 days | ||||
| Administration Dosage | 200 MBq | ||||
| MOA of PDC |
In conclusion, the hematotoxicity resulting from the infusion of radioactivity doses up to 200 MBq in our mouse model is transient, and mice exhibit normalized blood values within a month with no other apparent adverse effects (e.g., deaths, bleeding, or sustained body mass loss). These activities in animal models may increase the relevance when studying renal toxicity in animal models and, hence, help improve therapeutic translation from animal models to the clinic.
Click to Show/Hide
|
||||
| Description |
After 17 days, the 160 MBq group still had lower WBC and lymphocytes, but the monocytes and granulocytes had recovered to a similar level as control animals. At 21, 25, and 32 days, there were no significant differences between control and animals receiving 177Lu-PSMA-617, suggesting no long-lasting hematotoxicity. Overall, there was no correlation between activity received and decrease in white blood cells at the different time points, not when correcting for body mass differences either.
Click to Show/Hide
|
||||
| In Vivo Model | BALB/cAnNRj mice. | ||||
| Experiment 36 Reporting the Activity Data of This PDC | [86] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Monocyte count |
0.35x109/L
|
|||
| Administration Time | 13 days | ||||
| Administration Dosage | 160 MBq | ||||
| MOA of PDC |
In conclusion, the hematotoxicity resulting from the infusion of radioactivity doses up to 200 MBq in our mouse model is transient, and mice exhibit normalized blood values within a month with no other apparent adverse effects (e.g., deaths, bleeding, or sustained body mass loss). These activities in animal models may increase the relevance when studying renal toxicity in animal models and, hence, help improve therapeutic translation from animal models to the clinic.
Click to Show/Hide
|
||||
| Description |
After 17 days, the 160 MBq group still had lower WBC and lymphocytes, but the monocytes and granulocytes had recovered to a similar level as control animals. At 21, 25, and 32 days, there were no significant differences between control and animals receiving 177Lu-PSMA-617, suggesting no long-lasting hematotoxicity. Overall, there was no correlation between activity received and decrease in white blood cells at the different time points, not when correcting for body mass differences either.
Click to Show/Hide
|
||||
| In Vivo Model | BALB/cAnNRj mice. | ||||
| Experiment 37 Reporting the Activity Data of This PDC | [86] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Monocyte count |
0.45x109/L
|
|||
| Administration Time | 13 days | ||||
| Administration Dosage | 160 MBq | ||||
| MOA of PDC |
In conclusion, the hematotoxicity resulting from the infusion of radioactivity doses up to 200 MBq in our mouse model is transient, and mice exhibit normalized blood values within a month with no other apparent adverse effects (e.g., deaths, bleeding, or sustained body mass loss). These activities in animal models may increase the relevance when studying renal toxicity in animal models and, hence, help improve therapeutic translation from animal models to the clinic.
Click to Show/Hide
|
||||
| Description |
After 17 days, the 160 MBq group still had lower WBC and lymphocytes, but the monocytes and granulocytes had recovered to a similar level as control animals. At 21, 25, and 32 days, there were no significant differences between control and animals receiving 177Lu-PSMA-617, suggesting no long-lasting hematotoxicity. Overall, there was no correlation between activity received and decrease in white blood cells at the different time points, not when correcting for body mass differences either.
Click to Show/Hide
|
||||
| In Vivo Model | BALB/cAnNRj mice. | ||||
| Experiment 38 Reporting the Activity Data of This PDC | [86] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Monocyte count |
0.5x109/L
|
|||
| Administration Time | 13 days | ||||
| Administration Dosage | 200 MBq | ||||
| MOA of PDC |
In conclusion, the hematotoxicity resulting from the infusion of radioactivity doses up to 200 MBq in our mouse model is transient, and mice exhibit normalized blood values within a month with no other apparent adverse effects (e.g., deaths, bleeding, or sustained body mass loss). These activities in animal models may increase the relevance when studying renal toxicity in animal models and, hence, help improve therapeutic translation from animal models to the clinic.
Click to Show/Hide
|
||||
| Description |
After 17 days, the 160 MBq group still had lower WBC and lymphocytes, but the monocytes and granulocytes had recovered to a similar level as control animals. At 21, 25, and 32 days, there were no significant differences between control and animals receiving 177Lu-PSMA-617, suggesting no long-lasting hematotoxicity. Overall, there was no correlation between activity received and decrease in white blood cells at the different time points, not when correcting for body mass differences either.
Click to Show/Hide
|
||||
| In Vivo Model | BALB/cAnNRj mice. | ||||
| Experiment 39 Reporting the Activity Data of This PDC | [86] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Monocyte count |
0.6x109/L
|
|||
| Administration Time | 13 days | ||||
| Administration Dosage | 120 MBq | ||||
| MOA of PDC |
In conclusion, the hematotoxicity resulting from the infusion of radioactivity doses up to 200 MBq in our mouse model is transient, and mice exhibit normalized blood values within a month with no other apparent adverse effects (e.g., deaths, bleeding, or sustained body mass loss). These activities in animal models may increase the relevance when studying renal toxicity in animal models and, hence, help improve therapeutic translation from animal models to the clinic.
Click to Show/Hide
|
||||
| Description |
After 17 days, the 160 MBq group still had lower WBC and lymphocytes, but the monocytes and granulocytes had recovered to a similar level as control animals. At 21, 25, and 32 days, there were no significant differences between control and animals receiving 177Lu-PSMA-617, suggesting no long-lasting hematotoxicity. Overall, there was no correlation between activity received and decrease in white blood cells at the different time points, not when correcting for body mass differences either.
Click to Show/Hide
|
||||
| In Vivo Model | BALB/cAnNRj mice. | ||||
| Experiment 40 Reporting the Activity Data of This PDC | [86] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Platelet count |
50x109/L
|
|||
| Administration Time | 4 days | ||||
| Administration Dosage | 200 MBq | ||||
| MOA of PDC |
In conclusion, the hematotoxicity resulting from the infusion of radioactivity doses up to 200 MBq in our mouse model is transient, and mice exhibit normalized blood values within a month with no other apparent adverse effects (e.g., deaths, bleeding, or sustained body mass loss). These activities in animal models may increase the relevance when studying renal toxicity in animal models and, hence, help improve therapeutic translation from animal models to the clinic.
Click to Show/Hide
|
||||
| Description |
After 17 days, a significant drop in platelet levels could be seen in the 160 MBq group, which remained significantly lower compared to the control group after 21 days. This was also seen for the 120 MBq group, but not in the 200 MBq group, although there was a large spread in the latter group. The reduction in platelet count was still significant after 25 days in the 160 MBq group. At the last time point, 32 days, animals that had received activity had a large interval in the number of platelets, but at the group level, there was no difference compared to the control group.
Click to Show/Hide
|
||||
| In Vivo Model | BALB/cAnNRj mice. | ||||
| Experiment 41 Reporting the Activity Data of This PDC | [86] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Platelet count |
75x109/L
|
|||
| Administration Time | 21 days | ||||
| Administration Dosage | 160 MBq | ||||
| MOA of PDC |
In conclusion, the hematotoxicity resulting from the infusion of radioactivity doses up to 200 MBq in our mouse model is transient, and mice exhibit normalized blood values within a month with no other apparent adverse effects (e.g., deaths, bleeding, or sustained body mass loss). These activities in animal models may increase the relevance when studying renal toxicity in animal models and, hence, help improve therapeutic translation from animal models to the clinic.
Click to Show/Hide
|
||||
| Description |
After 17 days, a significant drop in platelet levels could be seen in the 160 MBq group, which remained significantly lower compared to the control group after 21 days. This was also seen for the 120 MBq group, but not in the 200 MBq group, although there was a large spread in the latter group. The reduction in platelet count was still significant after 25 days in the 160 MBq group. At the last time point, 32 days, animals that had received activity had a large interval in the number of platelets, but at the group level, there was no difference compared to the control group.
Click to Show/Hide
|
||||
| In Vivo Model | BALB/cAnNRj mice. | ||||
| Experiment 42 Reporting the Activity Data of This PDC | [86] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Platelet count |
120x109/L
|
|||
| Administration Time | 21 days | ||||
| Administration Dosage | 120 MBq | ||||
| MOA of PDC |
In conclusion, the hematotoxicity resulting from the infusion of radioactivity doses up to 200 MBq in our mouse model is transient, and mice exhibit normalized blood values within a month with no other apparent adverse effects (e.g., deaths, bleeding, or sustained body mass loss). These activities in animal models may increase the relevance when studying renal toxicity in animal models and, hence, help improve therapeutic translation from animal models to the clinic.
Click to Show/Hide
|
||||
| Description |
After 17 days, a significant drop in platelet levels could be seen in the 160 MBq group, which remained significantly lower compared to the control group after 21 days. This was also seen for the 120 MBq group, but not in the 200 MBq group, although there was a large spread in the latter group. The reduction in platelet count was still significant after 25 days in the 160 MBq group. At the last time point, 32 days, animals that had received activity had a large interval in the number of platelets, but at the group level, there was no difference compared to the control group.
Click to Show/Hide
|
||||
| In Vivo Model | BALB/cAnNRj mice. | ||||
| Experiment 43 Reporting the Activity Data of This PDC | [86] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Platelet count |
180x109/L
|
|||
| Administration Time | 21 days | ||||
| Administration Dosage | 120 MBq | ||||
| MOA of PDC |
In conclusion, the hematotoxicity resulting from the infusion of radioactivity doses up to 200 MBq in our mouse model is transient, and mice exhibit normalized blood values within a month with no other apparent adverse effects (e.g., deaths, bleeding, or sustained body mass loss). These activities in animal models may increase the relevance when studying renal toxicity in animal models and, hence, help improve therapeutic translation from animal models to the clinic.
Click to Show/Hide
|
||||
| Description |
After 17 days, a significant drop in platelet levels could be seen in the 160 MBq group, which remained significantly lower compared to the control group after 21 days. This was also seen for the 120 MBq group, but not in the 200 MBq group, although there was a large spread in the latter group. The reduction in platelet count was still significant after 25 days in the 160 MBq group. At the last time point, 32 days, animals that had received activity had a large interval in the number of platelets, but at the group level, there was no difference compared to the control group.
Click to Show/Hide
|
||||
| In Vivo Model | BALB/cAnNRj mice. | ||||
| Experiment 44 Reporting the Activity Data of This PDC | [86] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Platelet count |
225x109/L
|
|||
| Administration Time | 21 days | ||||
| Administration Dosage | 160 MBq | ||||
| MOA of PDC |
In conclusion, the hematotoxicity resulting from the infusion of radioactivity doses up to 200 MBq in our mouse model is transient, and mice exhibit normalized blood values within a month with no other apparent adverse effects (e.g., deaths, bleeding, or sustained body mass loss). These activities in animal models may increase the relevance when studying renal toxicity in animal models and, hence, help improve therapeutic translation from animal models to the clinic.
Click to Show/Hide
|
||||
| Description |
After 17 days, a significant drop in platelet levels could be seen in the 160 MBq group, which remained significantly lower compared to the control group after 21 days. This was also seen for the 120 MBq group, but not in the 200 MBq group, although there was a large spread in the latter group. The reduction in platelet count was still significant after 25 days in the 160 MBq group. At the last time point, 32 days, animals that had received activity had a large interval in the number of platelets, but at the group level, there was no difference compared to the control group.
Click to Show/Hide
|
||||
| In Vivo Model | BALB/cAnNRj mice. | ||||
| Experiment 45 Reporting the Activity Data of This PDC | [86] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Platelet count |
250x109/L
|
|||
| Administration Time | 21 days | ||||
| Administration Dosage | 200 MBq | ||||
| MOA of PDC |
In conclusion, the hematotoxicity resulting from the infusion of radioactivity doses up to 200 MBq in our mouse model is transient, and mice exhibit normalized blood values within a month with no other apparent adverse effects (e.g., deaths, bleeding, or sustained body mass loss). These activities in animal models may increase the relevance when studying renal toxicity in animal models and, hence, help improve therapeutic translation from animal models to the clinic.
Click to Show/Hide
|
||||
| Description |
After 17 days, a significant drop in platelet levels could be seen in the 160 MBq group, which remained significantly lower compared to the control group after 21 days. This was also seen for the 120 MBq group, but not in the 200 MBq group, although there was a large spread in the latter group. The reduction in platelet count was still significant after 25 days in the 160 MBq group. At the last time point, 32 days, animals that had received activity had a large interval in the number of platelets, but at the group level, there was no difference compared to the control group.
Click to Show/Hide
|
||||
| In Vivo Model | BALB/cAnNRj mice. | ||||
| Experiment 46 Reporting the Activity Data of This PDC | [86] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Red blood cells count |
2x1012/L
|
|||
| Administration Time | 13 days | ||||
| Administration Dosage | 160 MBq | ||||
| MOA of PDC |
In conclusion, the hematotoxicity resulting from the infusion of radioactivity doses up to 200 MBq in our mouse model is transient, and mice exhibit normalized blood values within a month with no other apparent adverse effects (e.g., deaths, bleeding, or sustained body mass loss). These activities in animal models may increase the relevance when studying renal toxicity in animal models and, hence, help improve therapeutic translation from animal models to the clinic.
Click to Show/Hide
|
||||
| Description |
After 21 days, all groups showed a tendency toward a lower number of RBCs, although only significant in the 120 MBq group. However, when analyzing the blood at 25 days post injection, the number of RBCs and HCT were again significantly lower in the 160 MBq animals. After 32 days, all studied parameters involving RBCs were normalized and did not differ from control mice, with the only exception of MCV in the 200 MBq group. Similar to the RBCs, the spread, in general, was larger in the treated groups for MCV, HBG, and HCT than in the control group. Further, as with the WBC, the decrease in RBCs and HBG levels did not have a correlation to injected activity, and no significant differences between the 120, 160, and 200 MBq were seen at any time point.
Click to Show/Hide
|
||||
| In Vivo Model | BALB/cAnNRj mice. | ||||
| Experiment 47 Reporting the Activity Data of This PDC | [86] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Red blood cells count |
2.5x1012/L
|
|||
| Administration Time | 13 days | ||||
| Administration Dosage | 200 MBq | ||||
| MOA of PDC |
In conclusion, the hematotoxicity resulting from the infusion of radioactivity doses up to 200 MBq in our mouse model is transient, and mice exhibit normalized blood values within a month with no other apparent adverse effects (e.g., deaths, bleeding, or sustained body mass loss). These activities in animal models may increase the relevance when studying renal toxicity in animal models and, hence, help improve therapeutic translation from animal models to the clinic.
Click to Show/Hide
|
||||
| Description |
After 21 days, all groups showed a tendency toward a lower number of RBCs, although only significant in the 120 MBq group. However, when analyzing the blood at 25 days post injection, the number of RBCs and HCT were again significantly lower in the 160 MBq animals. After 32 days, all studied parameters involving RBCs were normalized and did not differ from control mice, with the only exception of MCV in the 200 MBq group. Similar to the RBCs, the spread, in general, was larger in the treated groups for MCV, HBG, and HCT than in the control group. Further, as with the WBC, the decrease in RBCs and HBG levels did not have a correlation to injected activity, and no significant differences between the 120, 160, and 200 MBq were seen at any time point.
Click to Show/Hide
|
||||
| In Vivo Model | BALB/cAnNRj mice. | ||||
| Experiment 48 Reporting the Activity Data of This PDC | [86] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Red blood cells count |
3x1012/L
|
|||
| Administration Time | 13 days | ||||
| Administration Dosage | 120 MBq | ||||
| MOA of PDC |
In conclusion, the hematotoxicity resulting from the infusion of radioactivity doses up to 200 MBq in our mouse model is transient, and mice exhibit normalized blood values within a month with no other apparent adverse effects (e.g., deaths, bleeding, or sustained body mass loss). These activities in animal models may increase the relevance when studying renal toxicity in animal models and, hence, help improve therapeutic translation from animal models to the clinic.
Click to Show/Hide
|
||||
| Description |
After 21 days, all groups showed a tendency toward a lower number of RBCs, although only significant in the 120 MBq group. However, when analyzing the blood at 25 days post injection, the number of RBCs and HCT were again significantly lower in the 160 MBq animals. After 32 days, all studied parameters involving RBCs were normalized and did not differ from control mice, with the only exception of MCV in the 200 MBq group. Similar to the RBCs, the spread, in general, was larger in the treated groups for MCV, HBG, and HCT than in the control group. Further, as with the WBC, the decrease in RBCs and HBG levels did not have a correlation to injected activity, and no significant differences between the 120, 160, and 200 MBq were seen at any time point.
Click to Show/Hide
|
||||
| In Vivo Model | BALB/cAnNRj mice. | ||||
| Experiment 49 Reporting the Activity Data of This PDC | [86] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Red blood cells count |
8x1012/L
|
|||
| Administration Time | 13 days | ||||
| Administration Dosage | 120 MBq | ||||
| MOA of PDC |
In conclusion, the hematotoxicity resulting from the infusion of radioactivity doses up to 200 MBq in our mouse model is transient, and mice exhibit normalized blood values within a month with no other apparent adverse effects (e.g., deaths, bleeding, or sustained body mass loss). These activities in animal models may increase the relevance when studying renal toxicity in animal models and, hence, help improve therapeutic translation from animal models to the clinic.
Click to Show/Hide
|
||||
| Description |
After 21 days, all groups showed a tendency toward a lower number of RBCs, although only significant in the 120 MBq group. However, when analyzing the blood at 25 days post injection, the number of RBCs and HCT were again significantly lower in the 160 MBq animals. After 32 days, all studied parameters involving RBCs were normalized and did not differ from control mice, with the only exception of MCV in the 200 MBq group. Similar to the RBCs, the spread, in general, was larger in the treated groups for MCV, HBG, and HCT than in the control group. Further, as with the WBC, the decrease in RBCs and HBG levels did not have a correlation to injected activity, and no significant differences between the 120, 160, and 200 MBq were seen at any time point.
Click to Show/Hide
|
||||
| In Vivo Model | BALB/cAnNRj mice. | ||||
| Experiment 50 Reporting the Activity Data of This PDC | [86] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Red blood cells count |
8.5x1012/L
|
|||
| Administration Time | 13 days | ||||
| Administration Dosage | 200 MBq | ||||
| MOA of PDC |
In conclusion, the hematotoxicity resulting from the infusion of radioactivity doses up to 200 MBq in our mouse model is transient, and mice exhibit normalized blood values within a month with no other apparent adverse effects (e.g., deaths, bleeding, or sustained body mass loss). These activities in animal models may increase the relevance when studying renal toxicity in animal models and, hence, help improve therapeutic translation from animal models to the clinic.
Click to Show/Hide
|
||||
| Description |
After 21 days, all groups showed a tendency toward a lower number of RBCs, although only significant in the 120 MBq group. However, when analyzing the blood at 25 days post injection, the number of RBCs and HCT were again significantly lower in the 160 MBq animals. After 32 days, all studied parameters involving RBCs were normalized and did not differ from control mice, with the only exception of MCV in the 200 MBq group. Similar to the RBCs, the spread, in general, was larger in the treated groups for MCV, HBG, and HCT than in the control group. Further, as with the WBC, the decrease in RBCs and HBG levels did not have a correlation to injected activity, and no significant differences between the 120, 160, and 200 MBq were seen at any time point.
Click to Show/Hide
|
||||
| In Vivo Model | BALB/cAnNRj mice. | ||||
| Experiment 51 Reporting the Activity Data of This PDC | [86] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Red blood cells count |
9x1012/L
|
|||
| Administration Time | 13 days | ||||
| Administration Dosage | 160 MBq | ||||
| MOA of PDC |
In conclusion, the hematotoxicity resulting from the infusion of radioactivity doses up to 200 MBq in our mouse model is transient, and mice exhibit normalized blood values within a month with no other apparent adverse effects (e.g., deaths, bleeding, or sustained body mass loss). These activities in animal models may increase the relevance when studying renal toxicity in animal models and, hence, help improve therapeutic translation from animal models to the clinic.
Click to Show/Hide
|
||||
| Description |
After 21 days, all groups showed a tendency toward a lower number of RBCs, although only significant in the 120 MBq group. However, when analyzing the blood at 25 days post injection, the number of RBCs and HCT were again significantly lower in the 160 MBq animals. After 32 days, all studied parameters involving RBCs were normalized and did not differ from control mice, with the only exception of MCV in the 200 MBq group. Similar to the RBCs, the spread, in general, was larger in the treated groups for MCV, HBG, and HCT than in the control group. Further, as with the WBC, the decrease in RBCs and HBG levels did not have a correlation to injected activity, and no significant differences between the 120, 160, and 200 MBq were seen at any time point.
Click to Show/Hide
|
||||
| In Vivo Model | BALB/cAnNRj mice. | ||||
| Experiment 52 Reporting the Activity Data of This PDC | [86] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | White blood cells count |
6x109/L
|
|||
| Administration Time | 13 days | ||||
| Administration Dosage | 160 MBq | ||||
| MOA of PDC |
In conclusion, the hematotoxicity resulting from the infusion of radioactivity doses up to 200 MBq in our mouse model is transient, and mice exhibit normalized blood values within a month with no other apparent adverse effects (e.g., deaths, bleeding, or sustained body mass loss). These activities in animal models may increase the relevance when studying renal toxicity in animal models and, hence, help improve therapeutic translation from animal models to the clinic.
Click to Show/Hide
|
||||
| Description |
There were no significant differences in blood values in control animals at the different time points during the experiment; hence, data for all control animals (a mean from the different time points of each individual animal) are presented at all timepoints. Already after 4 days post injection of 160 MBq 177Lu-PSMA-617, there was a significant lowering of WBC, notably in lymphocytes but not in monocytes and granulocytes. The drop in WBC was significant in all groups receiving activity, 120, 160, and 200 MBq, after 13 days, where monocytes and granulocytes, in addition to lymphocytes (with an exception for 120 MBq), also were significantly lower than the control group.
Click to Show/Hide
|
||||
| In Vivo Model | BALB/cAnNRj mice. | ||||
| Experiment 53 Reporting the Activity Data of This PDC | [86] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | White blood cells count |
6x109/L
|
|||
| Administration Time | 13 days | ||||
| Administration Dosage | 120 MBq | ||||
| MOA of PDC |
In conclusion, the hematotoxicity resulting from the infusion of radioactivity doses up to 200 MBq in our mouse model is transient, and mice exhibit normalized blood values within a month with no other apparent adverse effects (e.g., deaths, bleeding, or sustained body mass loss). These activities in animal models may increase the relevance when studying renal toxicity in animal models and, hence, help improve therapeutic translation from animal models to the clinic.
Click to Show/Hide
|
||||
| Description |
There were no significant differences in blood values in control animals at the different time points during the experiment; hence, data for all control animals (a mean from the different time points of each individual animal) are presented at all timepoints. Already after 4 days post injection of 160 MBq 177Lu-PSMA-617, there was a significant lowering of WBC, notably in lymphocytes but not in monocytes and granulocytes. The drop in WBC was significant in all groups receiving activity, 120, 160, and 200 MBq, after 13 days, where monocytes and granulocytes, in addition to lymphocytes (with an exception for 120 MBq), also were significantly lower than the control group.
Click to Show/Hide
|
||||
| In Vivo Model | BALB/cAnNRj mice. | ||||
| Experiment 54 Reporting the Activity Data of This PDC | [86] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | White blood cells count |
7x109/L
|
|||
| Administration Time | 13 days | ||||
| Administration Dosage | 200 MBq | ||||
| MOA of PDC |
In conclusion, the hematotoxicity resulting from the infusion of radioactivity doses up to 200 MBq in our mouse model is transient, and mice exhibit normalized blood values within a month with no other apparent adverse effects (e.g., deaths, bleeding, or sustained body mass loss). These activities in animal models may increase the relevance when studying renal toxicity in animal models and, hence, help improve therapeutic translation from animal models to the clinic.
Click to Show/Hide
|
||||
| Description |
There were no significant differences in blood values in control animals at the different time points during the experiment; hence, data for all control animals (a mean from the different time points of each individual animal) are presented at all timepoints. Already after 4 days post injection of 160 MBq 177Lu-PSMA-617, there was a significant lowering of WBC, notably in lymphocytes but not in monocytes and granulocytes. The drop in WBC was significant in all groups receiving activity, 120, 160, and 200 MBq, after 13 days, where monocytes and granulocytes, in addition to lymphocytes (with an exception for 120 MBq), also were significantly lower than the control group.
Click to Show/Hide
|
||||
| In Vivo Model | BALB/cAnNRj mice. | ||||
| Experiment 55 Reporting the Activity Data of This PDC | [86] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | White blood cells count |
8x109/L
|
|||
| Administration Time | 13 days | ||||
| Administration Dosage | 120 MBq | ||||
| MOA of PDC |
In conclusion, the hematotoxicity resulting from the infusion of radioactivity doses up to 200 MBq in our mouse model is transient, and mice exhibit normalized blood values within a month with no other apparent adverse effects (e.g., deaths, bleeding, or sustained body mass loss). These activities in animal models may increase the relevance when studying renal toxicity in animal models and, hence, help improve therapeutic translation from animal models to the clinic.
Click to Show/Hide
|
||||
| Description |
There were no significant differences in blood values in control animals at the different time points during the experiment; hence, data for all control animals (a mean from the different time points of each individual animal) are presented at all timepoints. Already after 4 days post injection of 160 MBq 177Lu-PSMA-617, there was a significant lowering of WBC, notably in lymphocytes but not in monocytes and granulocytes. The drop in WBC was significant in all groups receiving activity, 120, 160, and 200 MBq, after 13 days, where monocytes and granulocytes, in addition to lymphocytes (with an exception for 120 MBq), also were significantly lower than the control group.
Click to Show/Hide
|
||||
| In Vivo Model | BALB/cAnNRj mice. | ||||
| Experiment 56 Reporting the Activity Data of This PDC | [86] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | White blood cells count |
8x109/L
|
|||
| Administration Time | 13 days | ||||
| Administration Dosage | 160 MBq | ||||
| MOA of PDC |
In conclusion, the hematotoxicity resulting from the infusion of radioactivity doses up to 200 MBq in our mouse model is transient, and mice exhibit normalized blood values within a month with no other apparent adverse effects (e.g., deaths, bleeding, or sustained body mass loss). These activities in animal models may increase the relevance when studying renal toxicity in animal models and, hence, help improve therapeutic translation from animal models to the clinic.
Click to Show/Hide
|
||||
| Description |
There were no significant differences in blood values in control animals at the different time points during the experiment; hence, data for all control animals (a mean from the different time points of each individual animal) are presented at all timepoints. Already after 4 days post injection of 160 MBq 177Lu-PSMA-617, there was a significant lowering of WBC, notably in lymphocytes but not in monocytes and granulocytes. The drop in WBC was significant in all groups receiving activity, 120, 160, and 200 MBq, after 13 days, where monocytes and granulocytes, in addition to lymphocytes (with an exception for 120 MBq), also were significantly lower than the control group.
Click to Show/Hide
|
||||
| In Vivo Model | BALB/cAnNRj mice. | ||||
Revealed Based on the Cell Line Data
| Experiment 1 Reporting the Activity Data of This PDC | [87] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Cell blocking rate |
0.10%
|
|||
| Administration Time | 2 h | ||||
| Administration Dosage | 10 MBq/nmol (3.75 nM) | ||||
| Evaluation Method | ICP-MS or γ-counting assay | ||||
| MOA of PDC |
This study addresses the question whether inductively coupled plasma mass spectrometry (ICP-MS) can be used as a method for the in vitro and in vivo characterization of non-radioactive metal conjugates to predict the properties of analogous radiopharmaceuticals. In a proof-of-concept study, the prostate-specific membrane antigen (PSMA)-targeting [175Lu]Lu-PSMA-617 and [159Tb]Tb-PSMA-617 were compared with their respective radiolabeled analogues, [177Lu]Lu-PSMA-617 (PLUVICTO, Novartis) and [161Tb]Tb-PSMA-617. ICP-MS and conventional γ-counting of the cell samples revealed almost identical results (<6% absolute difference between the two technologies) for the in vitro uptake and internalization of the (radio)metal conjugates, irrespective of the employed methodology. In vivo, an equal uptake in PSMA-positive PC-3 PIP tumor xenografts was determined 1 h after the injection of [175Lu]Lu-/[177Lu]Lu-PSMA-617 (41 ± 6% ID/g and 44 ± 12% IA/g, respectively) and [159Tb]Tb-/[161Tb]Tb-PSMA-617 (44 ± 5% ID/g and 44 ± 5% IA/g, respectively). It was further revealed that it is crucial to use the same ratios of the (radio)metal-labeled and unlabeled ligands for both methodologies to obtain equal data in organs in which receptor saturation was reached such as the kidneys (12 ± 2% ID/g vs 10 ± 1% IA/g, 1 h after injection). The data of this study demonstrate that the use of high-sensitivity ICP-MS allows reliable and predictive quantification of compounds labeled with stable metal isotopes in cell and tissue samples obtained in preclinical studies. It can, hence, be employed as a valid alternative to the state-of-the-art γ-counting methodology to detect radioactive ligands.
Click to Show/Hide
|
||||
| Description |
In LNCaP cells, the uptake of [175Lu]Lu-PSMA-617 determined by ICP-MS was 13 ± 2% (after 2 h) and 18 ± 2% (after 4 h). γ-Counting revealed the uptake of [177Lu]Lu-PSMA-617 in LNCaP cells of 11 ± 1% (after 2 h) and 14 ± 1% (after 4 h). For [159Tb]Tb-PSMA-617, analysis by ICP-MS revealed the uptake in LNCaP cells of 12 ± 1% (after 2 h) and 13 ± 1% (after 4 h). For the radioligand [161Tb]Tb-PSMA-617, the uptake in LNCaP cells determined by γ-counting was 7.8 ± 0.8% (after 2 h) and 9.7 ± 0.2% (after 4 h).
Click to Show/Hide
|
||||
| In Vitro Model | Prostate carcinoma | LNCaP cell | CVCL_0395 | ||
| Experiment 2 Reporting the Activity Data of This PDC | [87] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Cell blocking rate |
0.20%
|
|||
| Administration Time | 4 h | ||||
| Administration Dosage | 10 MBq/nmol (3.75 nM) | ||||
| Evaluation Method | ICP-MS or γ-counting assay | ||||
| MOA of PDC |
This study addresses the question whether inductively coupled plasma mass spectrometry (ICP-MS) can be used as a method for the in vitro and in vivo characterization of non-radioactive metal conjugates to predict the properties of analogous radiopharmaceuticals. In a proof-of-concept study, the prostate-specific membrane antigen (PSMA)-targeting [175Lu]Lu-PSMA-617 and [159Tb]Tb-PSMA-617 were compared with their respective radiolabeled analogues, [177Lu]Lu-PSMA-617 (PLUVICTO, Novartis) and [161Tb]Tb-PSMA-617. ICP-MS and conventional γ-counting of the cell samples revealed almost identical results (<6% absolute difference between the two technologies) for the in vitro uptake and internalization of the (radio)metal conjugates, irrespective of the employed methodology. In vivo, an equal uptake in PSMA-positive PC-3 PIP tumor xenografts was determined 1 h after the injection of [175Lu]Lu-/[177Lu]Lu-PSMA-617 (41 ± 6% ID/g and 44 ± 12% IA/g, respectively) and [159Tb]Tb-/[161Tb]Tb-PSMA-617 (44 ± 5% ID/g and 44 ± 5% IA/g, respectively). It was further revealed that it is crucial to use the same ratios of the (radio)metal-labeled and unlabeled ligands for both methodologies to obtain equal data in organs in which receptor saturation was reached such as the kidneys (12 ± 2% ID/g vs 10 ± 1% IA/g, 1 h after injection). The data of this study demonstrate that the use of high-sensitivity ICP-MS allows reliable and predictive quantification of compounds labeled with stable metal isotopes in cell and tissue samples obtained in preclinical studies. It can, hence, be employed as a valid alternative to the state-of-the-art γ-counting methodology to detect radioactive ligands.
Click to Show/Hide
|
||||
| Description |
In LNCaP cells, the uptake of [175Lu]Lu-PSMA-617 determined by ICP-MS was 13 ± 2% (after 2 h) and 18 ± 2% (after 4 h). γ-Counting revealed the uptake of [177Lu]Lu-PSMA-617 in LNCaP cells of 11 ± 1% (after 2 h) and 14 ± 1% (after 4 h). For [159Tb]Tb-PSMA-617, analysis by ICP-MS revealed the uptake in LNCaP cells of 12 ± 1% (after 2 h) and 13 ± 1% (after 4 h). For the radioligand [161Tb]Tb-PSMA-617, the uptake in LNCaP cells determined by γ-counting was 7.8 ± 0.8% (after 2 h) and 9.7 ± 0.2% (after 4 h).
Click to Show/Hide
|
||||
| In Vitro Model | Prostate carcinoma | LNCaP cell | CVCL_0395 | ||
| Experiment 3 Reporting the Activity Data of This PDC | [87] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Cell internalization rate |
6.4 ± 0.6 %
|
|||
| Administration Time | 2 h | ||||
| Administration Dosage | 10 MBq/nmol (3.75 nM) | ||||
| Evaluation Method | ICP-MS or γ-counting assay | ||||
| MOA of PDC |
This study addresses the question whether inductively coupled plasma mass spectrometry (ICP-MS) can be used as a method for the in vitro and in vivo characterization of non-radioactive metal conjugates to predict the properties of analogous radiopharmaceuticals. In a proof-of-concept study, the prostate-specific membrane antigen (PSMA)-targeting [175Lu]Lu-PSMA-617 and [159Tb]Tb-PSMA-617 were compared with their respective radiolabeled analogues, [177Lu]Lu-PSMA-617 (PLUVICTO, Novartis) and [161Tb]Tb-PSMA-617. ICP-MS and conventional γ-counting of the cell samples revealed almost identical results (<6% absolute difference between the two technologies) for the in vitro uptake and internalization of the (radio)metal conjugates, irrespective of the employed methodology. In vivo, an equal uptake in PSMA-positive PC-3 PIP tumor xenografts was determined 1 h after the injection of [175Lu]Lu-/[177Lu]Lu-PSMA-617 (41 ± 6% ID/g and 44 ± 12% IA/g, respectively) and [159Tb]Tb-/[161Tb]Tb-PSMA-617 (44 ± 5% ID/g and 44 ± 5% IA/g, respectively). It was further revealed that it is crucial to use the same ratios of the (radio)metal-labeled and unlabeled ligands for both methodologies to obtain equal data in organs in which receptor saturation was reached such as the kidneys (12 ± 2% ID/g vs 10 ± 1% IA/g, 1 h after injection). The data of this study demonstrate that the use of high-sensitivity ICP-MS allows reliable and predictive quantification of compounds labeled with stable metal isotopes in cell and tissue samples obtained in preclinical studies. It can, hence, be employed as a valid alternative to the state-of-the-art γ-counting methodology to detect radioactive ligands.
Click to Show/Hide
|
||||
| Description |
In LNCaP cells, the uptake of [175Lu]Lu-PSMA-617 determined by ICP-MS was 13 ± 2% (after 2 h) and 18 ± 2% (after 4 h). γ-Counting revealed the uptake of [177Lu]Lu-PSMA-617 in LNCaP cells of 11 ± 1% (after 2 h) and 14 ± 1% (after 4 h). For [159Tb]Tb-PSMA-617, analysis by ICP-MS revealed the uptake in LNCaP cells of 12 ± 1% (after 2 h) and 13 ± 1% (after 4 h). For the radioligand [161Tb]Tb-PSMA-617, the uptake in LNCaP cells determined by γ-counting was 7.8 ± 0.8% (after 2 h) and 9.7 ± 0.2% (after 4 h).
Click to Show/Hide
|
||||
| In Vitro Model | Prostate carcinoma | LNCaP cell | CVCL_0395 | ||
| Experiment 4 Reporting the Activity Data of This PDC | [87] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Cell internalization rate |
10 ± 2 %
|
|||
| Administration Time | 4 h | ||||
| Administration Dosage | 10 MBq/nmol (3.75 nM) | ||||
| Evaluation Method | ICP-MS or γ-counting assay | ||||
| MOA of PDC |
This study addresses the question whether inductively coupled plasma mass spectrometry (ICP-MS) can be used as a method for the in vitro and in vivo characterization of non-radioactive metal conjugates to predict the properties of analogous radiopharmaceuticals. In a proof-of-concept study, the prostate-specific membrane antigen (PSMA)-targeting [175Lu]Lu-PSMA-617 and [159Tb]Tb-PSMA-617 were compared with their respective radiolabeled analogues, [177Lu]Lu-PSMA-617 (PLUVICTO, Novartis) and [161Tb]Tb-PSMA-617. ICP-MS and conventional γ-counting of the cell samples revealed almost identical results (<6% absolute difference between the two technologies) for the in vitro uptake and internalization of the (radio)metal conjugates, irrespective of the employed methodology. In vivo, an equal uptake in PSMA-positive PC-3 PIP tumor xenografts was determined 1 h after the injection of [175Lu]Lu-/[177Lu]Lu-PSMA-617 (41 ± 6% ID/g and 44 ± 12% IA/g, respectively) and [159Tb]Tb-/[161Tb]Tb-PSMA-617 (44 ± 5% ID/g and 44 ± 5% IA/g, respectively). It was further revealed that it is crucial to use the same ratios of the (radio)metal-labeled and unlabeled ligands for both methodologies to obtain equal data in organs in which receptor saturation was reached such as the kidneys (12 ± 2% ID/g vs 10 ± 1% IA/g, 1 h after injection). The data of this study demonstrate that the use of high-sensitivity ICP-MS allows reliable and predictive quantification of compounds labeled with stable metal isotopes in cell and tissue samples obtained in preclinical studies. It can, hence, be employed as a valid alternative to the state-of-the-art γ-counting methodology to detect radioactive ligands.
Click to Show/Hide
|
||||
| Description |
In LNCaP cells, the uptake of [175Lu]Lu-PSMA-617 determined by ICP-MS was 13 ± 2% (after 2 h) and 18 ± 2% (after 4 h). γ-Counting revealed the uptake of [177Lu]Lu-PSMA-617 in LNCaP cells of 11 ± 1% (after 2 h) and 14 ± 1% (after 4 h). For [159Tb]Tb-PSMA-617, analysis by ICP-MS revealed the uptake in LNCaP cells of 12 ± 1% (after 2 h) and 13 ± 1% (after 4 h). For the radioligand [161Tb]Tb-PSMA-617, the uptake in LNCaP cells determined by γ-counting was 7.8 ± 0.8% (after 2 h) and 9.7 ± 0.2% (after 4 h).
Click to Show/Hide
|
||||
| In Vitro Model | Prostate carcinoma | LNCaP cell | CVCL_0395 | ||
| Experiment 5 Reporting the Activity Data of This PDC | [87] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Cell internalization rate |
15 ± 1 %
|
|||
| Administration Time | 2 h | ||||
| Administration Dosage | 10 MBq/nmol (3.75 nM) | ||||
| Evaluation Method | ICP-MS or γ-counting assay | ||||
| MOA of PDC |
This study addresses the question whether inductively coupled plasma mass spectrometry (ICP-MS) can be used as a method for the in vitro and in vivo characterization of non-radioactive metal conjugates to predict the properties of analogous radiopharmaceuticals. In a proof-of-concept study, the prostate-specific membrane antigen (PSMA)-targeting [175Lu]Lu-PSMA-617 and [159Tb]Tb-PSMA-617 were compared with their respective radiolabeled analogues, [177Lu]Lu-PSMA-617 (PLUVICTO, Novartis) and [161Tb]Tb-PSMA-617. ICP-MS and conventional γ-counting of the cell samples revealed almost identical results (<6% absolute difference between the two technologies) for the in vitro uptake and internalization of the (radio)metal conjugates, irrespective of the employed methodology. In vivo, an equal uptake in PSMA-positive PC-3 PIP tumor xenografts was determined 1 h after the injection of [175Lu]Lu-/[177Lu]Lu-PSMA-617 (41 ± 6% ID/g and 44 ± 12% IA/g, respectively) and [159Tb]Tb-/[161Tb]Tb-PSMA-617 (44 ± 5% ID/g and 44 ± 5% IA/g, respectively). It was further revealed that it is crucial to use the same ratios of the (radio)metal-labeled and unlabeled ligands for both methodologies to obtain equal data in organs in which receptor saturation was reached such as the kidneys (12 ± 2% ID/g vs 10 ± 1% IA/g, 1 h after injection). The data of this study demonstrate that the use of high-sensitivity ICP-MS allows reliable and predictive quantification of compounds labeled with stable metal isotopes in cell and tissue samples obtained in preclinical studies. It can, hence, be employed as a valid alternative to the state-of-the-art γ-counting methodology to detect radioactive ligands.
Click to Show/Hide
|
||||
| Description |
The uptake of [175Lu]Lu-PSMA-617 in PC-3 PIP tumor cells determined by ICP-MS was 57 ± 5% (after 2 h) and 69 ± 6% (after 4 h), whereas it was 55 ± 2% (after 2 h) and 68 ± 5% (after 4 h) as determined by γ-counting for [177Lu]Lu-PSMA-617. For [159Tb]Tb-PSMA-617, the uptake in PC-3 PIP tumor cells determined by ICP-MS was 51 ± 4% (after 2 h) and 60 ± 5% (after 4 h), whereas for [161Tb]Tb-PSMA-617, it was 47 ± 3% (after 2 h) and 54 ± 6% (after 4 h) as determined by γ-counting.
Click to Show/Hide
|
||||
| In Vitro Model | Prostate carcinoma | PSMA-positive PC-3 PIP cell | CVCL_0035 | ||
| Experiment 6 Reporting the Activity Data of This PDC | [87] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Cell internalization rate |
20 ± 3 %
|
|||
| Administration Time | 4 h | ||||
| Administration Dosage | 10 MBq/nmol (3.75 nM) | ||||
| Evaluation Method | ICP-MS or γ-counting assay | ||||
| MOA of PDC |
This study addresses the question whether inductively coupled plasma mass spectrometry (ICP-MS) can be used as a method for the in vitro and in vivo characterization of non-radioactive metal conjugates to predict the properties of analogous radiopharmaceuticals. In a proof-of-concept study, the prostate-specific membrane antigen (PSMA)-targeting [175Lu]Lu-PSMA-617 and [159Tb]Tb-PSMA-617 were compared with their respective radiolabeled analogues, [177Lu]Lu-PSMA-617 (PLUVICTO, Novartis) and [161Tb]Tb-PSMA-617. ICP-MS and conventional γ-counting of the cell samples revealed almost identical results (<6% absolute difference between the two technologies) for the in vitro uptake and internalization of the (radio)metal conjugates, irrespective of the employed methodology. In vivo, an equal uptake in PSMA-positive PC-3 PIP tumor xenografts was determined 1 h after the injection of [175Lu]Lu-/[177Lu]Lu-PSMA-617 (41 ± 6% ID/g and 44 ± 12% IA/g, respectively) and [159Tb]Tb-/[161Tb]Tb-PSMA-617 (44 ± 5% ID/g and 44 ± 5% IA/g, respectively). It was further revealed that it is crucial to use the same ratios of the (radio)metal-labeled and unlabeled ligands for both methodologies to obtain equal data in organs in which receptor saturation was reached such as the kidneys (12 ± 2% ID/g vs 10 ± 1% IA/g, 1 h after injection). The data of this study demonstrate that the use of high-sensitivity ICP-MS allows reliable and predictive quantification of compounds labeled with stable metal isotopes in cell and tissue samples obtained in preclinical studies. It can, hence, be employed as a valid alternative to the state-of-the-art γ-counting methodology to detect radioactive ligands.
Click to Show/Hide
|
||||
| Description |
The uptake of [175Lu]Lu-PSMA-617 in PC-3 PIP tumor cells determined by ICP-MS was 57 ± 5% (after 2 h) and 69 ± 6% (after 4 h), whereas it was 55 ± 2% (after 2 h) and 68 ± 5% (after 4 h) as determined by γ-counting for [177Lu]Lu-PSMA-617. For [159Tb]Tb-PSMA-617, the uptake in PC-3 PIP tumor cells determined by ICP-MS was 51 ± 4% (after 2 h) and 60 ± 5% (after 4 h), whereas for [161Tb]Tb-PSMA-617, it was 47 ± 3% (after 2 h) and 54 ± 6% (after 4 h) as determined by γ-counting.
Click to Show/Hide
|
||||
| In Vitro Model | Prostate carcinoma | PSMA-positive PC-3 PIP cell | CVCL_0035 | ||
| Experiment 7 Reporting the Activity Data of This PDC | [87] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Cell uptake rate | < 0.10% | |||
| Administration Time | 4 h | ||||
| Administration Dosage | 10 MBq/nmol (3.75 nM) | ||||
| Evaluation Method | ICP-MS or γ-counting assay | ||||
| MOA of PDC |
This study addresses the question whether inductively coupled plasma mass spectrometry (ICP-MS) can be used as a method for the in vitro and in vivo characterization of non-radioactive metal conjugates to predict the properties of analogous radiopharmaceuticals. In a proof-of-concept study, the prostate-specific membrane antigen (PSMA)-targeting [175Lu]Lu-PSMA-617 and [159Tb]Tb-PSMA-617 were compared with their respective radiolabeled analogues, [177Lu]Lu-PSMA-617 (PLUVICTO, Novartis) and [161Tb]Tb-PSMA-617. ICP-MS and conventional γ-counting of the cell samples revealed almost identical results (<6% absolute difference between the two technologies) for the in vitro uptake and internalization of the (radio)metal conjugates, irrespective of the employed methodology. In vivo, an equal uptake in PSMA-positive PC-3 PIP tumor xenografts was determined 1 h after the injection of [175Lu]Lu-/[177Lu]Lu-PSMA-617 (41 ± 6% ID/g and 44 ± 12% IA/g, respectively) and [159Tb]Tb-/[161Tb]Tb-PSMA-617 (44 ± 5% ID/g and 44 ± 5% IA/g, respectively). It was further revealed that it is crucial to use the same ratios of the (radio)metal-labeled and unlabeled ligands for both methodologies to obtain equal data in organs in which receptor saturation was reached such as the kidneys (12 ± 2% ID/g vs 10 ± 1% IA/g, 1 h after injection). The data of this study demonstrate that the use of high-sensitivity ICP-MS allows reliable and predictive quantification of compounds labeled with stable metal isotopes in cell and tissue samples obtained in preclinical studies. It can, hence, be employed as a valid alternative to the state-of-the-art γ-counting methodology to detect radioactive ligands.
Click to Show/Hide
|
||||
| Description |
The uptake of [175Lu]Lu-PSMA-617 in PC-3 PIP tumor cells determined by ICP-MS was 57 ± 5% (after 2 h) and 69 ± 6% (after 4 h), whereas it was 55 ± 2% (after 2 h) and 68 ± 5% (after 4 h) as determined by γ-counting for [177Lu]Lu-PSMA-617. For [159Tb]Tb-PSMA-617, the uptake in PC-3 PIP tumor cells determined by ICP-MS was 51 ± 4% (after 2 h) and 60 ± 5% (after 4 h), whereas for [161Tb]Tb-PSMA-617, it was 47 ± 3% (after 2 h) and 54 ± 6% (after 4 h) as determined by γ-counting.
Click to Show/Hide
|
||||
| In Vitro Model | Prostate carcinoma | PSMA-negative PC-3 flu cell | CVCL_0035 | ||
| Experiment 8 Reporting the Activity Data of This PDC | [88] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Cell uptake rate |
3.50%
|
|||
| Administration Time | 5 min | ||||
| Administration Dosage | 37 kBq | ||||
| Evaluation Method | Gamma counter assay | ||||
| MOA of PDC |
Prostate-specific membrane antigen (PSMA) is an excellent target for imaging and radionuclide therapy of prostate cancer. Recently, [177Lu]Lu-PSMA-617 (Pluvicto) was approved by the FDA for radionuclide therapy. To develop hetero-bivalent agents targeting both PSMA and bone metastasis, [177Lu]Lu-P17-079 ([177Lu]Lu-1) and [177Lu]Lu-P17-081 ([177Lu]Lu-2) were prepared. In vivo biodistribution studies of [177Lu]Lu-PSMA-617, [177Lu]Lu-1, and [177Lu]Lu-2 in mice bearing PC3-PIP (PSMA positive) tumor showed high uptake in PSMA-positive tumor (14.5, 14.7, and 11.3% ID/g at 1 h, respectively) and distinctively different bone uptakes (0.52, 6.52, and 5.82% ID/g at 1 h, respectively). PET imaging using [68Ga]Ga-P17-079 ([68Ga]Ga-1) in the same mouse model displayed excellent images confirming the expected dual-targeting to PSMA-positive tumor and bone. Results suggest that [177Lu]Lu-P17-079 ([177Lu]Lu-1) is a promising candidate for further development as a hetero-bivalent radionuclide therapy agent targeting both PSMA expression and bone metastases for the treatment of prostate cancer.
Click to Show/Hide
|
||||
| Description |
As expected, the PSMA-targeting hetero-bivalent agents, [177Lu]Lu-1 and [177Lu]Lu-2, displayed excellent cell uptake in PC3-PIP PSMA-positive cells. Furthermore, [177Lu]Lu-1 displayed a higher uptake (about 2 times higher, p < 0.05) as that of [177Lu]Lu-2. The higher uptake in PSMA-positive cells suggested that [177Lu]Lu-1 may more readily penetrate the cell membrane and may be more localized in the PSMA-positive tumor cells. The uptake was specifically inhibited by blocking study (in the presence of 1 uM cold PSMA-617). Both agents did not show any significant cell uptakes in PSMA-negative cells (PC3 cells). Cell uptake kinetics of [177Lu]Lu-1 and [177Lu]Lu-2 showed very rapid uptakes in PC3-PIP PSMA-positive cells (5, 15, 30, 60, and 120 min, respectively). As a positive control, [177Lu]Lu-PSMA-617 also showed excellent cell uptake under a similar condition. It is noted that [177Lu]Lu-2 showed a very similar uptake kinetics as that of [177Lu]Lu-PSMA-617, while [177Lu]Lu-1 displayed a significantly higher and faster uptake. Apparently, a small change in the chemical structure of the location of the bisphosphonate group between [177Lu]Lu-1 and [177Lu]Lu-2 may have contributed to this observation. No obvious reason could be contributed to the superior cell uptake of [177Lu]Lu-1. This distinctive difference in in vitro cell uptake may also be responsible for variations of PSMA-positive tumor uptakes in vivo.
Click to Show/Hide
|
||||
| In Vitro Model | Prostate carcinoma | PC3-PIP PSMA-positive cell | CVCL_0035 | ||
| Experiment 9 Reporting the Activity Data of This PDC | [88] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Cell uptake rate |
5.50%
|
|||
| Administration Time | 15 min | ||||
| Administration Dosage | 37 kBq | ||||
| Evaluation Method | Gamma counter assay | ||||
| MOA of PDC |
Prostate-specific membrane antigen (PSMA) is an excellent target for imaging and radionuclide therapy of prostate cancer. Recently, [177Lu]Lu-PSMA-617 (Pluvicto) was approved by the FDA for radionuclide therapy. To develop hetero-bivalent agents targeting both PSMA and bone metastasis, [177Lu]Lu-P17-079 ([177Lu]Lu-1) and [177Lu]Lu-P17-081 ([177Lu]Lu-2) were prepared. In vivo biodistribution studies of [177Lu]Lu-PSMA-617, [177Lu]Lu-1, and [177Lu]Lu-2 in mice bearing PC3-PIP (PSMA positive) tumor showed high uptake in PSMA-positive tumor (14.5, 14.7, and 11.3% ID/g at 1 h, respectively) and distinctively different bone uptakes (0.52, 6.52, and 5.82% ID/g at 1 h, respectively). PET imaging using [68Ga]Ga-P17-079 ([68Ga]Ga-1) in the same mouse model displayed excellent images confirming the expected dual-targeting to PSMA-positive tumor and bone. Results suggest that [177Lu]Lu-P17-079 ([177Lu]Lu-1) is a promising candidate for further development as a hetero-bivalent radionuclide therapy agent targeting both PSMA expression and bone metastases for the treatment of prostate cancer.
Click to Show/Hide
|
||||
| Description |
As expected, the PSMA-targeting hetero-bivalent agents, [177Lu]Lu-1 and [177Lu]Lu-2, displayed excellent cell uptake in PC3-PIP PSMA-positive cells. Furthermore, [177Lu]Lu-1 displayed a higher uptake (about 2 times higher, p < 0.05) as that of [177Lu]Lu-2. The higher uptake in PSMA-positive cells suggested that [177Lu]Lu-1 may more readily penetrate the cell membrane and may be more localized in the PSMA-positive tumor cells. The uptake was specifically inhibited by blocking study (in the presence of 1 uM cold PSMA-617). Both agents did not show any significant cell uptakes in PSMA-negative cells (PC3 cells). Cell uptake kinetics of [177Lu]Lu-1 and [177Lu]Lu-2 showed very rapid uptakes in PC3-PIP PSMA-positive cells (5, 15, 30, 60, and 120 min, respectively). As a positive control, [177Lu]Lu-PSMA-617 also showed excellent cell uptake under a similar condition. It is noted that [177Lu]Lu-2 showed a very similar uptake kinetics as that of [177Lu]Lu-PSMA-617, while [177Lu]Lu-1 displayed a significantly higher and faster uptake. Apparently, a small change in the chemical structure of the location of the bisphosphonate group between [177Lu]Lu-1 and [177Lu]Lu-2 may have contributed to this observation. No obvious reason could be contributed to the superior cell uptake of [177Lu]Lu-1. This distinctive difference in in vitro cell uptake may also be responsible for variations of PSMA-positive tumor uptakes in vivo.
Click to Show/Hide
|
||||
| In Vitro Model | Prostate carcinoma | PC3-PIP PSMA-positive cell | CVCL_0035 | ||
| Experiment 10 Reporting the Activity Data of This PDC | [88] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Cell uptake rate |
6%
|
|||
| Administration Time | 30 min | ||||
| Administration Dosage | 37 kBq | ||||
| Evaluation Method | Gamma counter assay | ||||
| MOA of PDC |
Prostate-specific membrane antigen (PSMA) is an excellent target for imaging and radionuclide therapy of prostate cancer. Recently, [177Lu]Lu-PSMA-617 (Pluvicto) was approved by the FDA for radionuclide therapy. To develop hetero-bivalent agents targeting both PSMA and bone metastasis, [177Lu]Lu-P17-079 ([177Lu]Lu-1) and [177Lu]Lu-P17-081 ([177Lu]Lu-2) were prepared. In vivo biodistribution studies of [177Lu]Lu-PSMA-617, [177Lu]Lu-1, and [177Lu]Lu-2 in mice bearing PC3-PIP (PSMA positive) tumor showed high uptake in PSMA-positive tumor (14.5, 14.7, and 11.3% ID/g at 1 h, respectively) and distinctively different bone uptakes (0.52, 6.52, and 5.82% ID/g at 1 h, respectively). PET imaging using [68Ga]Ga-P17-079 ([68Ga]Ga-1) in the same mouse model displayed excellent images confirming the expected dual-targeting to PSMA-positive tumor and bone. Results suggest that [177Lu]Lu-P17-079 ([177Lu]Lu-1) is a promising candidate for further development as a hetero-bivalent radionuclide therapy agent targeting both PSMA expression and bone metastases for the treatment of prostate cancer.
Click to Show/Hide
|
||||
| Description |
As expected, the PSMA-targeting hetero-bivalent agents, [177Lu]Lu-1 and [177Lu]Lu-2, displayed excellent cell uptake in PC3-PIP PSMA-positive cells. Furthermore, [177Lu]Lu-1 displayed a higher uptake (about 2 times higher, p < 0.05) as that of [177Lu]Lu-2. The higher uptake in PSMA-positive cells suggested that [177Lu]Lu-1 may more readily penetrate the cell membrane and may be more localized in the PSMA-positive tumor cells. The uptake was specifically inhibited by blocking study (in the presence of 1 uM cold PSMA-617). Both agents did not show any significant cell uptakes in PSMA-negative cells (PC3 cells). Cell uptake kinetics of [177Lu]Lu-1 and [177Lu]Lu-2 showed very rapid uptakes in PC3-PIP PSMA-positive cells (5, 15, 30, 60, and 120 min, respectively). As a positive control, [177Lu]Lu-PSMA-617 also showed excellent cell uptake under a similar condition. It is noted that [177Lu]Lu-2 showed a very similar uptake kinetics as that of [177Lu]Lu-PSMA-617, while [177Lu]Lu-1 displayed a significantly higher and faster uptake. Apparently, a small change in the chemical structure of the location of the bisphosphonate group between [177Lu]Lu-1 and [177Lu]Lu-2 may have contributed to this observation. No obvious reason could be contributed to the superior cell uptake of [177Lu]Lu-1. This distinctive difference in in vitro cell uptake may also be responsible for variations of PSMA-positive tumor uptakes in vivo.
Click to Show/Hide
|
||||
| In Vitro Model | Prostate carcinoma | PC3-PIP PSMA-positive cell | CVCL_0035 | ||
| Experiment 11 Reporting the Activity Data of This PDC | [88] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Cell uptake rate |
7%
|
|||
| Administration Time | 60 min | ||||
| Administration Dosage | 37 kBq | ||||
| Evaluation Method | Gamma counter assay | ||||
| MOA of PDC |
Prostate-specific membrane antigen (PSMA) is an excellent target for imaging and radionuclide therapy of prostate cancer. Recently, [177Lu]Lu-PSMA-617 (Pluvicto) was approved by the FDA for radionuclide therapy. To develop hetero-bivalent agents targeting both PSMA and bone metastasis, [177Lu]Lu-P17-079 ([177Lu]Lu-1) and [177Lu]Lu-P17-081 ([177Lu]Lu-2) were prepared. In vivo biodistribution studies of [177Lu]Lu-PSMA-617, [177Lu]Lu-1, and [177Lu]Lu-2 in mice bearing PC3-PIP (PSMA positive) tumor showed high uptake in PSMA-positive tumor (14.5, 14.7, and 11.3% ID/g at 1 h, respectively) and distinctively different bone uptakes (0.52, 6.52, and 5.82% ID/g at 1 h, respectively). PET imaging using [68Ga]Ga-P17-079 ([68Ga]Ga-1) in the same mouse model displayed excellent images confirming the expected dual-targeting to PSMA-positive tumor and bone. Results suggest that [177Lu]Lu-P17-079 ([177Lu]Lu-1) is a promising candidate for further development as a hetero-bivalent radionuclide therapy agent targeting both PSMA expression and bone metastases for the treatment of prostate cancer.
Click to Show/Hide
|
||||
| Description |
As expected, the PSMA-targeting hetero-bivalent agents, [177Lu]Lu-1 and [177Lu]Lu-2, displayed excellent cell uptake in PC3-PIP PSMA-positive cells. Furthermore, [177Lu]Lu-1 displayed a higher uptake (about 2 times higher, p < 0.05) as that of [177Lu]Lu-2. The higher uptake in PSMA-positive cells suggested that [177Lu]Lu-1 may more readily penetrate the cell membrane and may be more localized in the PSMA-positive tumor cells. The uptake was specifically inhibited by blocking study (in the presence of 1 uM cold PSMA-617). Both agents did not show any significant cell uptakes in PSMA-negative cells (PC3 cells). Cell uptake kinetics of [177Lu]Lu-1 and [177Lu]Lu-2 showed very rapid uptakes in PC3-PIP PSMA-positive cells (5, 15, 30, 60, and 120 min, respectively). As a positive control, [177Lu]Lu-PSMA-617 also showed excellent cell uptake under a similar condition. It is noted that [177Lu]Lu-2 showed a very similar uptake kinetics as that of [177Lu]Lu-PSMA-617, while [177Lu]Lu-1 displayed a significantly higher and faster uptake. Apparently, a small change in the chemical structure of the location of the bisphosphonate group between [177Lu]Lu-1 and [177Lu]Lu-2 may have contributed to this observation. No obvious reason could be contributed to the superior cell uptake of [177Lu]Lu-1. This distinctive difference in in vitro cell uptake may also be responsible for variations of PSMA-positive tumor uptakes in vivo.
Click to Show/Hide
|
||||
| In Vitro Model | Prostate carcinoma | PC3-PIP PSMA-positive cell | CVCL_0035 | ||
| Experiment 12 Reporting the Activity Data of This PDC | [88] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Cell uptake rate |
9%
|
|||
| Administration Time | 120 min | ||||
| Administration Dosage | 37 kBq | ||||
| Evaluation Method | Gamma counter assay | ||||
| MOA of PDC |
Prostate-specific membrane antigen (PSMA) is an excellent target for imaging and radionuclide therapy of prostate cancer. Recently, [177Lu]Lu-PSMA-617 (Pluvicto) was approved by the FDA for radionuclide therapy. To develop hetero-bivalent agents targeting both PSMA and bone metastasis, [177Lu]Lu-P17-079 ([177Lu]Lu-1) and [177Lu]Lu-P17-081 ([177Lu]Lu-2) were prepared. In vivo biodistribution studies of [177Lu]Lu-PSMA-617, [177Lu]Lu-1, and [177Lu]Lu-2 in mice bearing PC3-PIP (PSMA positive) tumor showed high uptake in PSMA-positive tumor (14.5, 14.7, and 11.3% ID/g at 1 h, respectively) and distinctively different bone uptakes (0.52, 6.52, and 5.82% ID/g at 1 h, respectively). PET imaging using [68Ga]Ga-P17-079 ([68Ga]Ga-1) in the same mouse model displayed excellent images confirming the expected dual-targeting to PSMA-positive tumor and bone. Results suggest that [177Lu]Lu-P17-079 ([177Lu]Lu-1) is a promising candidate for further development as a hetero-bivalent radionuclide therapy agent targeting both PSMA expression and bone metastases for the treatment of prostate cancer.
Click to Show/Hide
|
||||
| Description |
As expected, the PSMA-targeting hetero-bivalent agents, [177Lu]Lu-1 and [177Lu]Lu-2, displayed excellent cell uptake in PC3-PIP PSMA-positive cells. Furthermore, [177Lu]Lu-1 displayed a higher uptake (about 2 times higher, p < 0.05) as that of [177Lu]Lu-2. The higher uptake in PSMA-positive cells suggested that [177Lu]Lu-1 may more readily penetrate the cell membrane and may be more localized in the PSMA-positive tumor cells. The uptake was specifically inhibited by blocking study (in the presence of 1 uM cold PSMA-617). Both agents did not show any significant cell uptakes in PSMA-negative cells (PC3 cells). Cell uptake kinetics of [177Lu]Lu-1 and [177Lu]Lu-2 showed very rapid uptakes in PC3-PIP PSMA-positive cells (5, 15, 30, 60, and 120 min, respectively). As a positive control, [177Lu]Lu-PSMA-617 also showed excellent cell uptake under a similar condition. It is noted that [177Lu]Lu-2 showed a very similar uptake kinetics as that of [177Lu]Lu-PSMA-617, while [177Lu]Lu-1 displayed a significantly higher and faster uptake. Apparently, a small change in the chemical structure of the location of the bisphosphonate group between [177Lu]Lu-1 and [177Lu]Lu-2 may have contributed to this observation. No obvious reason could be contributed to the superior cell uptake of [177Lu]Lu-1. This distinctive difference in in vitro cell uptake may also be responsible for variations of PSMA-positive tumor uptakes in vivo.
Click to Show/Hide
|
||||
| In Vitro Model | Prostate carcinoma | PC3-PIP PSMA-positive cell | CVCL_0035 | ||
| Experiment 13 Reporting the Activity Data of This PDC | [87] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Cell uptake rate |
11 ± 1 %
|
|||
| Administration Time | 2 h | ||||
| Administration Dosage | 10 MBq/nmol (3.75 nM) | ||||
| Evaluation Method | ICP-MS or γ-counting assay | ||||
| MOA of PDC |
This study addresses the question whether inductively coupled plasma mass spectrometry (ICP-MS) can be used as a method for the in vitro and in vivo characterization of non-radioactive metal conjugates to predict the properties of analogous radiopharmaceuticals. In a proof-of-concept study, the prostate-specific membrane antigen (PSMA)-targeting [175Lu]Lu-PSMA-617 and [159Tb]Tb-PSMA-617 were compared with their respective radiolabeled analogues, [177Lu]Lu-PSMA-617 (PLUVICTO, Novartis) and [161Tb]Tb-PSMA-617. ICP-MS and conventional γ-counting of the cell samples revealed almost identical results (<6% absolute difference between the two technologies) for the in vitro uptake and internalization of the (radio)metal conjugates, irrespective of the employed methodology. In vivo, an equal uptake in PSMA-positive PC-3 PIP tumor xenografts was determined 1 h after the injection of [175Lu]Lu-/[177Lu]Lu-PSMA-617 (41 ± 6% ID/g and 44 ± 12% IA/g, respectively) and [159Tb]Tb-/[161Tb]Tb-PSMA-617 (44 ± 5% ID/g and 44 ± 5% IA/g, respectively). It was further revealed that it is crucial to use the same ratios of the (radio)metal-labeled and unlabeled ligands for both methodologies to obtain equal data in organs in which receptor saturation was reached such as the kidneys (12 ± 2% ID/g vs 10 ± 1% IA/g, 1 h after injection). The data of this study demonstrate that the use of high-sensitivity ICP-MS allows reliable and predictive quantification of compounds labeled with stable metal isotopes in cell and tissue samples obtained in preclinical studies. It can, hence, be employed as a valid alternative to the state-of-the-art γ-counting methodology to detect radioactive ligands.
Click to Show/Hide
|
||||
| Description |
In LNCaP cells, the uptake of [175Lu]Lu-PSMA-617 determined by ICP-MS was 13 ± 2% (after 2 h) and 18 ± 2% (after 4 h). γ-Counting revealed the uptake of [177Lu]Lu-PSMA-617 in LNCaP cells of 11 ± 1% (after 2 h) and 14 ± 1% (after 4 h). For [159Tb]Tb-PSMA-617, analysis by ICP-MS revealed the uptake in LNCaP cells of 12 ± 1% (after 2 h) and 13 ± 1% (after 4 h). For the radioligand [161Tb]Tb-PSMA-617, the uptake in LNCaP cells determined by γ-counting was 7.8 ± 0.8% (after 2 h) and 9.7 ± 0.2% (after 4 h).
Click to Show/Hide
|
||||
| In Vitro Model | Prostate carcinoma | LNCaP cell | CVCL_0395 | ||
| Experiment 14 Reporting the Activity Data of This PDC | [87] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Cell uptake rate |
14 ± 1 %
|
|||
| Administration Time | 4 h | ||||
| Administration Dosage | 10 MBq/nmol (3.75 nM) | ||||
| Evaluation Method | ICP-MS or γ-counting assay | ||||
| MOA of PDC |
This study addresses the question whether inductively coupled plasma mass spectrometry (ICP-MS) can be used as a method for the in vitro and in vivo characterization of non-radioactive metal conjugates to predict the properties of analogous radiopharmaceuticals. In a proof-of-concept study, the prostate-specific membrane antigen (PSMA)-targeting [175Lu]Lu-PSMA-617 and [159Tb]Tb-PSMA-617 were compared with their respective radiolabeled analogues, [177Lu]Lu-PSMA-617 (PLUVICTO, Novartis) and [161Tb]Tb-PSMA-617. ICP-MS and conventional γ-counting of the cell samples revealed almost identical results (<6% absolute difference between the two technologies) for the in vitro uptake and internalization of the (radio)metal conjugates, irrespective of the employed methodology. In vivo, an equal uptake in PSMA-positive PC-3 PIP tumor xenografts was determined 1 h after the injection of [175Lu]Lu-/[177Lu]Lu-PSMA-617 (41 ± 6% ID/g and 44 ± 12% IA/g, respectively) and [159Tb]Tb-/[161Tb]Tb-PSMA-617 (44 ± 5% ID/g and 44 ± 5% IA/g, respectively). It was further revealed that it is crucial to use the same ratios of the (radio)metal-labeled and unlabeled ligands for both methodologies to obtain equal data in organs in which receptor saturation was reached such as the kidneys (12 ± 2% ID/g vs 10 ± 1% IA/g, 1 h after injection). The data of this study demonstrate that the use of high-sensitivity ICP-MS allows reliable and predictive quantification of compounds labeled with stable metal isotopes in cell and tissue samples obtained in preclinical studies. It can, hence, be employed as a valid alternative to the state-of-the-art γ-counting methodology to detect radioactive ligands.
Click to Show/Hide
|
||||
| Description |
In LNCaP cells, the uptake of [175Lu]Lu-PSMA-617 determined by ICP-MS was 13 ± 2% (after 2 h) and 18 ± 2% (after 4 h). γ-Counting revealed the uptake of [177Lu]Lu-PSMA-617 in LNCaP cells of 11 ± 1% (after 2 h) and 14 ± 1% (after 4 h). For [159Tb]Tb-PSMA-617, analysis by ICP-MS revealed the uptake in LNCaP cells of 12 ± 1% (after 2 h) and 13 ± 1% (after 4 h). For the radioligand [161Tb]Tb-PSMA-617, the uptake in LNCaP cells determined by γ-counting was 7.8 ± 0.8% (after 2 h) and 9.7 ± 0.2% (after 4 h).
Click to Show/Hide
|
||||
| In Vitro Model | Prostate carcinoma | LNCaP cell | CVCL_0395 | ||
| Experiment 15 Reporting the Activity Data of This PDC | [87] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Cell uptake rate |
55 ± 2 %
|
|||
| Administration Time | 2 h | ||||
| Administration Dosage | 10 MBq/nmol (3.75 nM) | ||||
| Evaluation Method | ICP-MS or γ-counting assay | ||||
| MOA of PDC |
This study addresses the question whether inductively coupled plasma mass spectrometry (ICP-MS) can be used as a method for the in vitro and in vivo characterization of non-radioactive metal conjugates to predict the properties of analogous radiopharmaceuticals. In a proof-of-concept study, the prostate-specific membrane antigen (PSMA)-targeting [175Lu]Lu-PSMA-617 and [159Tb]Tb-PSMA-617 were compared with their respective radiolabeled analogues, [177Lu]Lu-PSMA-617 (PLUVICTO, Novartis) and [161Tb]Tb-PSMA-617. ICP-MS and conventional γ-counting of the cell samples revealed almost identical results (<6% absolute difference between the two technologies) for the in vitro uptake and internalization of the (radio)metal conjugates, irrespective of the employed methodology. In vivo, an equal uptake in PSMA-positive PC-3 PIP tumor xenografts was determined 1 h after the injection of [175Lu]Lu-/[177Lu]Lu-PSMA-617 (41 ± 6% ID/g and 44 ± 12% IA/g, respectively) and [159Tb]Tb-/[161Tb]Tb-PSMA-617 (44 ± 5% ID/g and 44 ± 5% IA/g, respectively). It was further revealed that it is crucial to use the same ratios of the (radio)metal-labeled and unlabeled ligands for both methodologies to obtain equal data in organs in which receptor saturation was reached such as the kidneys (12 ± 2% ID/g vs 10 ± 1% IA/g, 1 h after injection). The data of this study demonstrate that the use of high-sensitivity ICP-MS allows reliable and predictive quantification of compounds labeled with stable metal isotopes in cell and tissue samples obtained in preclinical studies. It can, hence, be employed as a valid alternative to the state-of-the-art γ-counting methodology to detect radioactive ligands.
Click to Show/Hide
|
||||
| Description |
The uptake of [175Lu]Lu-PSMA-617 in PC-3 PIP tumor cells determined by ICP-MS was 57 ± 5% (after 2 h) and 69 ± 6% (after 4 h), whereas it was 55 ± 2% (after 2 h) and 68 ± 5% (after 4 h) as determined by γ-counting for [177Lu]Lu-PSMA-617. For [159Tb]Tb-PSMA-617, the uptake in PC-3 PIP tumor cells determined by ICP-MS was 51 ± 4% (after 2 h) and 60 ± 5% (after 4 h), whereas for [161Tb]Tb-PSMA-617, it was 47 ± 3% (after 2 h) and 54 ± 6% (after 4 h) as determined by γ-counting.
Click to Show/Hide
|
||||
| In Vitro Model | Prostate carcinoma | PSMA-positive PC-3 PIP cell | CVCL_0035 | ||
| Experiment 16 Reporting the Activity Data of This PDC | [87] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Cell uptake rate |
68 ± 5 %
|
|||
| Administration Time | 4 h | ||||
| Administration Dosage | 10 MBq/nmol (3.75 nM) | ||||
| Evaluation Method | ICP-MS or γ-counting assay | ||||
| MOA of PDC |
This study addresses the question whether inductively coupled plasma mass spectrometry (ICP-MS) can be used as a method for the in vitro and in vivo characterization of non-radioactive metal conjugates to predict the properties of analogous radiopharmaceuticals. In a proof-of-concept study, the prostate-specific membrane antigen (PSMA)-targeting [175Lu]Lu-PSMA-617 and [159Tb]Tb-PSMA-617 were compared with their respective radiolabeled analogues, [177Lu]Lu-PSMA-617 (PLUVICTO, Novartis) and [161Tb]Tb-PSMA-617. ICP-MS and conventional γ-counting of the cell samples revealed almost identical results (<6% absolute difference between the two technologies) for the in vitro uptake and internalization of the (radio)metal conjugates, irrespective of the employed methodology. In vivo, an equal uptake in PSMA-positive PC-3 PIP tumor xenografts was determined 1 h after the injection of [175Lu]Lu-/[177Lu]Lu-PSMA-617 (41 ± 6% ID/g and 44 ± 12% IA/g, respectively) and [159Tb]Tb-/[161Tb]Tb-PSMA-617 (44 ± 5% ID/g and 44 ± 5% IA/g, respectively). It was further revealed that it is crucial to use the same ratios of the (radio)metal-labeled and unlabeled ligands for both methodologies to obtain equal data in organs in which receptor saturation was reached such as the kidneys (12 ± 2% ID/g vs 10 ± 1% IA/g, 1 h after injection). The data of this study demonstrate that the use of high-sensitivity ICP-MS allows reliable and predictive quantification of compounds labeled with stable metal isotopes in cell and tissue samples obtained in preclinical studies. It can, hence, be employed as a valid alternative to the state-of-the-art γ-counting methodology to detect radioactive ligands.
Click to Show/Hide
|
||||
| Description |
The uptake of [175Lu]Lu-PSMA-617 in PC-3 PIP tumor cells determined by ICP-MS was 57 ± 5% (after 2 h) and 69 ± 6% (after 4 h), whereas it was 55 ± 2% (after 2 h) and 68 ± 5% (after 4 h) as determined by γ-counting for [177Lu]Lu-PSMA-617. For [159Tb]Tb-PSMA-617, the uptake in PC-3 PIP tumor cells determined by ICP-MS was 51 ± 4% (after 2 h) and 60 ± 5% (after 4 h), whereas for [161Tb]Tb-PSMA-617, it was 47 ± 3% (after 2 h) and 54 ± 6% (after 4 h) as determined by γ-counting.
Click to Show/Hide
|
||||
| In Vitro Model | Prostate carcinoma | PSMA-positive PC-3 PIP cell | CVCL_0035 | ||
| Experiment 17 Reporting the Activity Data of This PDC | [89] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Drug uptake dose |
31 cpm/µg
|
|||
| Administration Time | 30 min | ||||
| Administration Dosage | 177Lu-PSMA-617 0.44 nM, 2 MBq/4 ml/dish; PSMA-617 (10 nM) | ||||
| MOA of PDC |
Our results indicate that PSMA-617 inhibits proliferation of PCa cells and potentiates the cell death-promoting effects of 177Lu-PSMA-617. These findings require further confirmation in vitro and in vivo experiments to study the exact molecular mechanisms associated with the growth-inhibitory effects of PSMA-617 observed in PCa cells in order to test the potential of the simultaneous treatment with PSMA-617 and 177Lu-PSMA-617 for the translation in a clinical trial.
Click to Show/Hide
|
||||
| Description |
Both 177Lu-PSMA-617 and its non-radioactive precursor, PSMA-617, bind to the PSMA on the cell membrane. Therefore, PSMA-617 could compete with the 177Lu-PSMA-617- binding to LNCaP cells and, consequently may reduce its cytotoxic effects. However, PSMA-617 concentrations up to 100 nM did not impair the 177Lu-PSMA-617 uptake into the LNCaP cells (n = 9). Effects of PSMA-617 (10, 50 and 100 nM) (solid columns) on the uptake of 177Lu-PSMA-617 into LNCaP cells. Empty column, cells treated with vehicle. Results are expressed as the means ± SD. No significant differences among the groups were found (one-way ANOVA).
Click to Show/Hide
|
||||
| In Vitro Model | Prostate carcinoma | LNCaP cell | CVCL_0395 | ||
| Experiment 18 Reporting the Activity Data of This PDC | [89] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Drug uptake dose |
37.2 cpm/µg
|
|||
| Administration Time | 30 min | ||||
| Administration Dosage | 177Lu-PSMA-617 0.44 nM, 2 MBq/4 ml/dish; PSMA-617 (10 nM) | ||||
| MOA of PDC |
Our results indicate that PSMA-617 inhibits proliferation of PCa cells and potentiates the cell death-promoting effects of 177Lu-PSMA-617. These findings require further confirmation in vitro and in vivo experiments to study the exact molecular mechanisms associated with the growth-inhibitory effects of PSMA-617 observed in PCa cells in order to test the potential of the simultaneous treatment with PSMA-617 and 177Lu-PSMA-617 for the translation in a clinical trial.
Click to Show/Hide
|
||||
| Description |
Both 177Lu-PSMA-617 and its non-radioactive precursor, PSMA-617, bind to the PSMA on the cell membrane. Therefore, PSMA-617 could compete with the 177Lu-PSMA-617- binding to LNCaP cells and, consequently may reduce its cytotoxic effects. However, PSMA-617 concentrations up to 100 nM did not impair the 177Lu-PSMA-617 uptake into the LNCaP cells (n = 9). Effects of PSMA-617 (10, 50 and 100 nM) (solid columns) on the uptake of 177Lu-PSMA-617 into LNCaP cells. Empty column, cells treated with vehicle. Results are expressed as the means ± SD. No significant differences among the groups were found (one-way ANOVA).
Click to Show/Hide
|
||||
| In Vitro Model | Prostate carcinoma | LNCaP cell | CVCL_0395 | ||
| Experiment 19 Reporting the Activity Data of This PDC | [89] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Drug uptake dose |
38 cpm/µg
|
|||
| Administration Time | 30 min | ||||
| Administration Dosage | 177Lu-PSMA-617 0.44 nM, 2 MBq/4 ml/dish; PSMA-617 (10 nM) | ||||
| MOA of PDC |
Our results indicate that PSMA-617 inhibits proliferation of PCa cells and potentiates the cell death-promoting effects of 177Lu-PSMA-617. These findings require further confirmation in vitro and in vivo experiments to study the exact molecular mechanisms associated with the growth-inhibitory effects of PSMA-617 observed in PCa cells in order to test the potential of the simultaneous treatment with PSMA-617 and 177Lu-PSMA-617 for the translation in a clinical trial.
Click to Show/Hide
|
||||
| Description |
Both 177Lu-PSMA-617 and its non-radioactive precursor, PSMA-617, bind to the PSMA on the cell membrane. Therefore, PSMA-617 could compete with the 177Lu-PSMA-617- binding to LNCaP cells and, consequently may reduce its cytotoxic effects. However, PSMA-617 concentrations up to 100 nM did not impair the 177Lu-PSMA-617 uptake into the LNCaP cells (n = 9). Effects of PSMA-617 (10, 50 and 100 nM) (solid columns) on the uptake of 177Lu-PSMA-617 into LNCaP cells. Empty column, cells treated with vehicle. Results are expressed as the means ± SD. No significant differences among the groups were found (one-way ANOVA).
Click to Show/Hide
|
||||
| In Vitro Model | Prostate carcinoma | LNCaP cell | CVCL_0395 | ||
| Experiment 20 Reporting the Activity Data of This PDC | [90] | ||||
| Indication | Metastatic castration-resistant prostate cancer | ||||
| Efficacy Data | Half Maximal Inhibitory Concentration (IC50) |
11.1 ± 0.8 nM
|
|||
| Administration Time | 1 h | ||||
| Evaluation Method | Gamma counter assay | ||||
| MOA of PDC |
Prostate-specific membrane antigen (PSMA) is a promising target for the diagnosis and radionuclide therapy of prostate cancer. This study reports conversion of a previously reported 68Ga-imaging agent, [68Ga]Ga-P16-093, to a Lu-177 radionuclide therapeutic agent. Substitution of the HBED-CC metal chelating group with DOTA(GA)2 led to P17-087 (4) and P17-088 (7). Both agents showed excellent PSMA binding affinity (IC50 = 10-30 nM) comparable to that of recently FDA-approved [177Lu]Lu-PSMA-617 (Pluvicto). Biodistribution studies in PSMA expressing tumor bearing mice showed that [177Lu]Lu-4 exhibited very high tumor uptake and a fast blood clearance similar to those of [177Lu]Lu-PSMA-617. Conversely, [177Lu]Lu-7, containing an albumin binder, extended its blood half-life and exhibited significantly higher uptake and longer tumor residence time than [177Lu]Lu-4 and [177Lu]Lu-PSMA-617. The switch from chelator HBED-CC to DOTA(GA)2 and the switch from the imaging isotope gallium-68 to the therapeutic isotope lutetium-177 have successfully transformed a PSMA-targeting agent from diagnosis to promising radionuclide therapeutic agents.
Click to Show/Hide
|
||||
| Description |
The PSMA binding affinities were determined by a competitive binding assay using PSMA-overexpressing LNCaP human prostate carcinoma cell homogenates and a known high affinity 125I-labeled PSMA ligand, [125I]MIP-1095, as the radioligand. The IC50 values for the metal-free PSMA-inhibiting compounds and metal complexes are summarized in Table 1. PSMA-617 and P16-093 were included in this study as reference compounds. The PSMA affinities of 4 and 7 as well as their natLu-labeled complexes were comparable to those of the reference compounds and displayed excellent binding affinities (IC50 = 28.7, 15.4, 18.7, and 20.2 nM, respectively). The addition of the p-iodophenylbutanoyl group in compound 7 did not change the PSMA binding affinity because of the small molecular size and remote position from the PSMA binding site.
Click to Show/Hide
|
||||
| In Vitro Model | Prostate carcinoma | LNCaP cell | CVCL_0395 | ||
References